Green Spaces, Land Cover, Street Trees and Hypertension in the Megacity of São Paulo

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Hypertension Definition
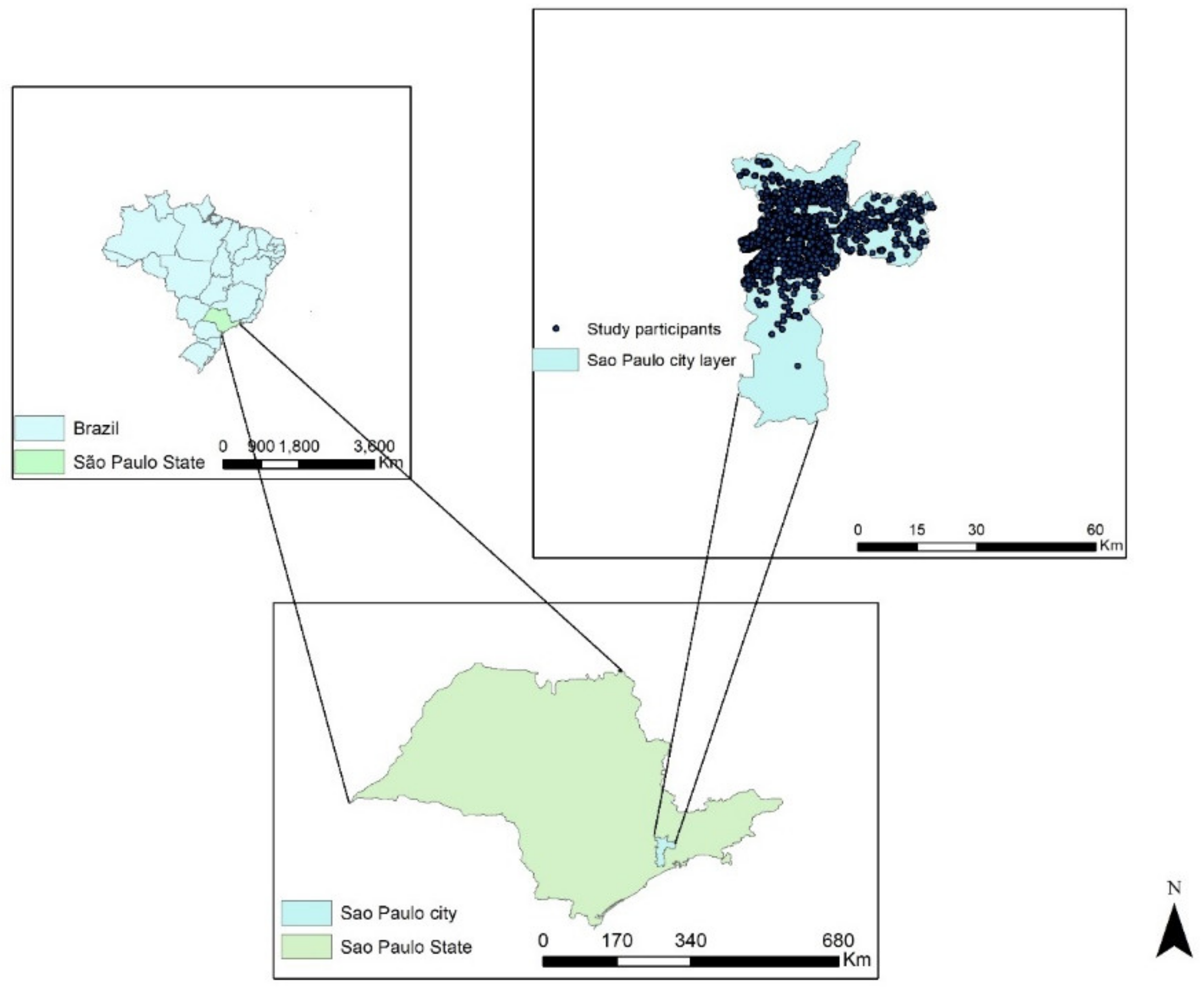
2.3. Study Area
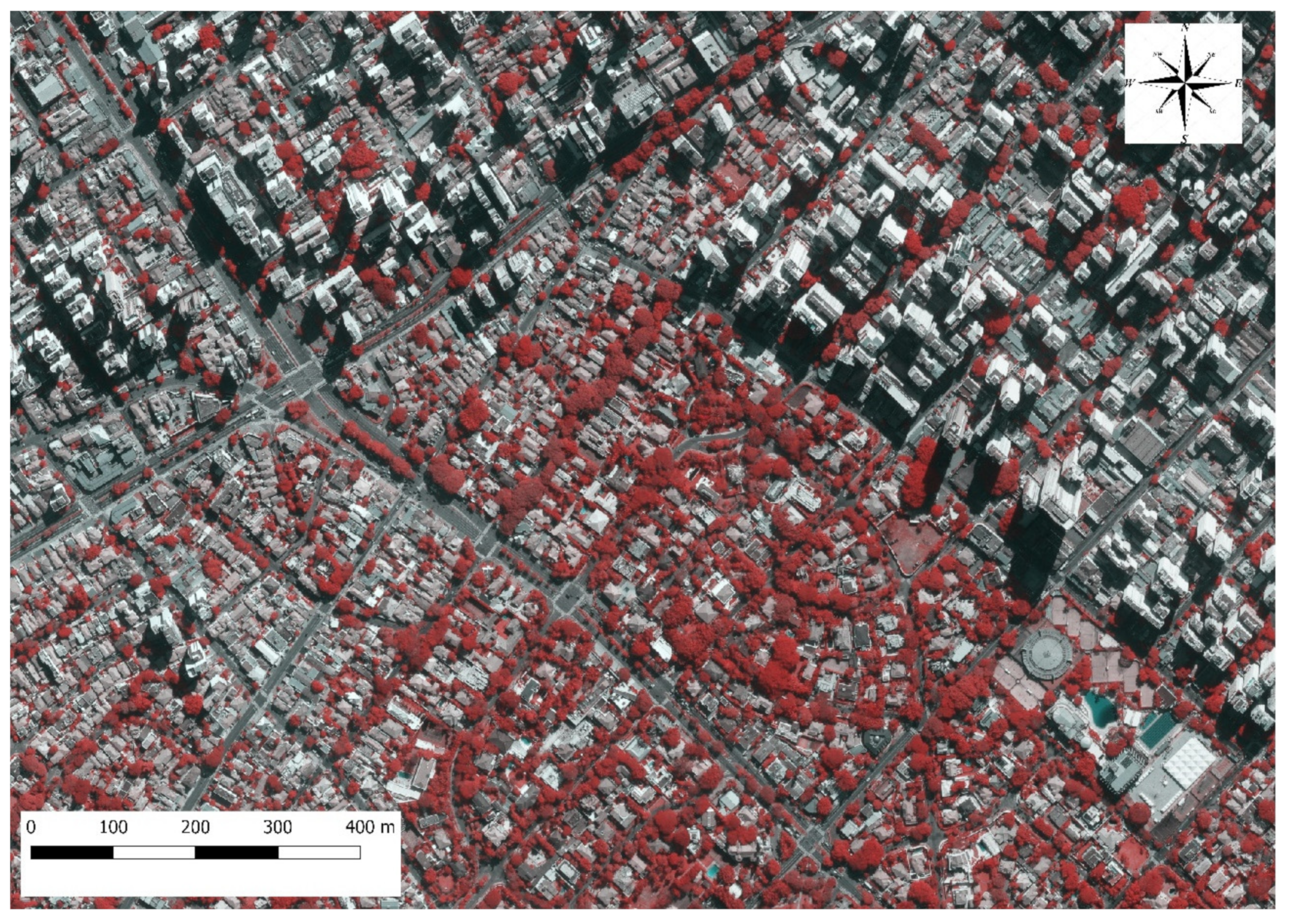
2.4. Street Trees Map
2.5. Land Cover Classification
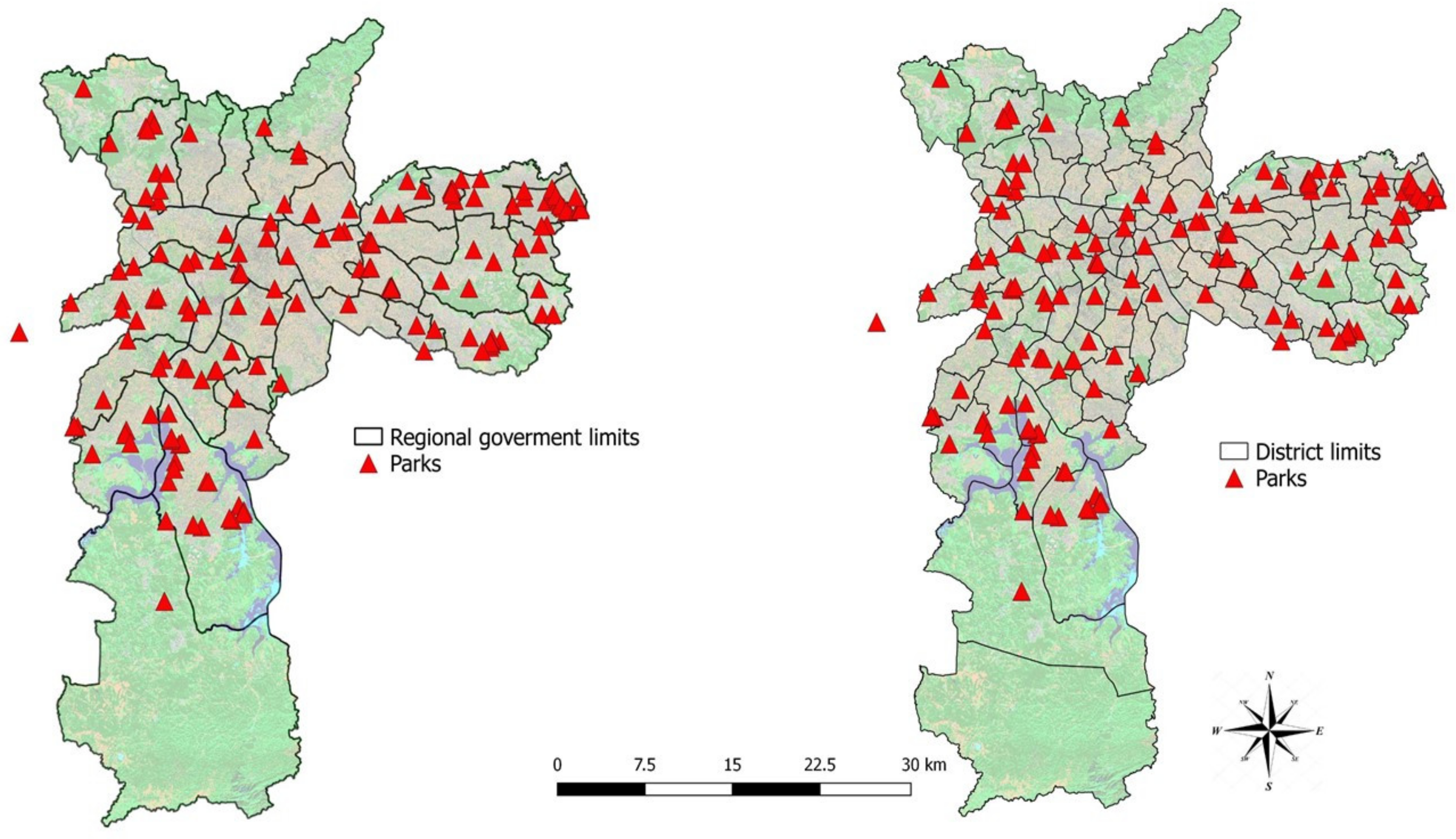
2.6. Urban Parks
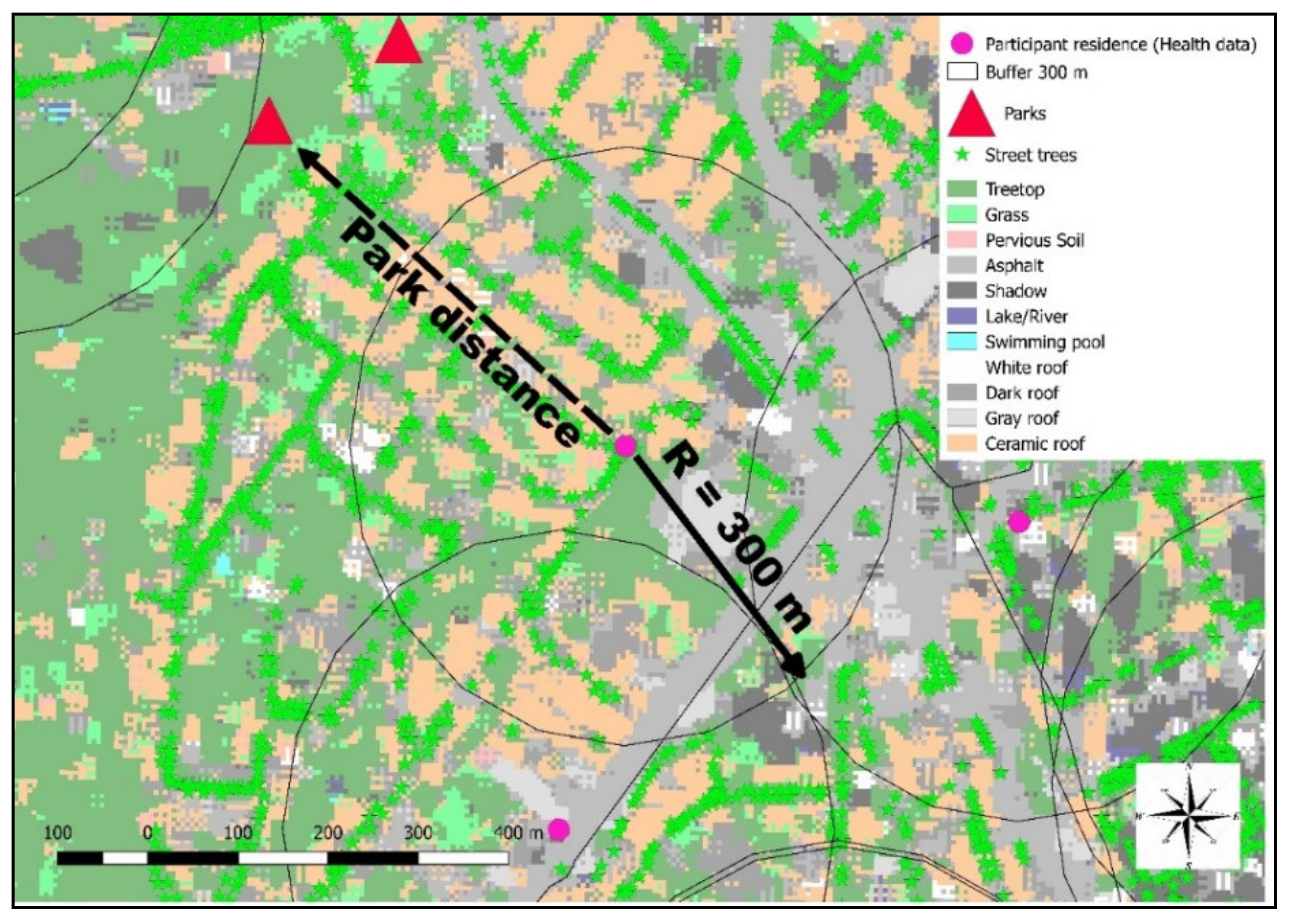
2.7. Land Cover Exposure Assessment
2.8. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McMichael, A.J. The urban environment and health in a world of increasing globalization: Issues for developing countries. Bull. World Health Organ. 2000, 78, 1117–1126. [Google Scholar] [PubMed]
- IBGE. Conheça Cidades e Estados do Brasil. Available online: www.cidades.ibge.gov.br (accessed on 25 September 2019).
- Millennium Ecosystem Assessment Board. Ecosystems and Human Well-Being: Wetlands and Water Synthesis; Island Press: Washington, DC, USA, 2005; ISBN 978-1-59726-040-4. [Google Scholar]
- Nieuwenhuijsen, M.J.; Khreis, H.; Triguero-Mas, M.; Gascon, M.; Dadvand, P. Fifty shades of green: Pathway to healthy urban living. Epidemiology 2017, 28, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Triguero-Mas, M.; Martínez, D.; Dadvand, P.; Rojas-Rueda, D.; Plasència, A.; Nieuwenhuijsen, M.J. Residential green spaces and mortality: A systematic review. Environ. Int. 2016, 86, 60–67. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Hart, J.E.; Banay, R.F.; Laden, F. Exposure to greenness and mortality in a nationwide prospective cohort study of women. Environ. Health Perspect. 2016, 124, 1344–1352. [Google Scholar] [CrossRef] [PubMed]
- Nowak, D.J.; Dwyer, J.F. Understanding the Benefits and Costs of Urban Forest Ecosystems; Springer: Dordrecht, The Netherlands, 2007; ISBN 978-1-4020-4288-1. [Google Scholar]
- Fang, C.-F.; Ling, D.-L. Guidance for noise reduction provided by tree belts. Landsc. Urban Plan. 2005, 71, 29–34. [Google Scholar] [CrossRef]
- Oliveira, S.; Andrade, H.; Vaz, T. The cooling effect of green spaces as a contribution to the mitigation of urban heat: A case study in Lisbon. Build. Environ. 2011, 46, 2186–2194. [Google Scholar] [CrossRef]
- Solecki, W.D.; Rosenzweig, C.; Parshall, L.; Pope, G.; Clark, M.; Cox, J.; Wiencke, M. Mitigation of the heat island effect in urban New Jersey. Glob. Environ. Chang. Part. B Environ. Hazards 2005, 6, 39–49. [Google Scholar] [CrossRef]
- Ngom, R.; Gosselin, P.; Blais, C.; Rochette, L. Type and proximity of green spaces are important for preventing cardiovascular morbidity and diabetes—A cross-sectional study for Quebec, Canada. Int. J. Environ. Res. Public Health 2016, 13, 423. [Google Scholar] [CrossRef]
- Araya, R.; Montgomery, A.; Rojas, G.; Fritsch, R.; Solis, J.; Signorelli, A.; Lewis, G. Common mental disorders and the built environment in Santiago, Chile. Br. J. Psychiatr. 2007, 190, 394–401. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Mitchell, R.; Hartig, T. The association between green space and mental health varies across the lifecourse. A longitudinal study. J. Epidemiol. Community Health 2014, 68, 578–583. [Google Scholar] [CrossRef]
- Van den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [PubMed]
- Senetra, A.; Krzywnicka, I.; Mielke, M. An analysis of the spatial distribution, influence and quality of urban green space—A case study of the Polish city of Tczew. Bull. Geogr. Socio Econ. Ser. 2018, 42, 129–149. [Google Scholar] [CrossRef]
- Wilker, E.H.; Wu, C.-D.; McNeely, E.; Mostofsky, E.; Spengler, J.; Wellenius, G.A.; Mittleman, M.A. Green space and mortality following ischemic stroke. Environ. Res. 2014, 133, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.-S.; Lung, S.-C.C. Can green structure reduce the mortality of cardiovascular diseases? Sci. Total Environ. 2016, 566–567, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Dzhambov, A.M.; Markevych, I.; Lercher, P. Greenspace seems protective of both high and low blood pressure among residents of an Alpine valley. Environ. Int. 2018, 121, 443–452. [Google Scholar] [CrossRef]
- Yeager, R.A.; Smith, T.R.; Bhatnagar, A. Green environments and cardiovascular health. Trends Cardiovasc. Med. 2019, in press. [Google Scholar] [CrossRef]
- Pereira, G.; Foster, S.; Martin, K.; Christian, H.; Boruff, B.J.; Knuiman, M.; Giles-Corti, B. The association between neighborhood greenness and cardiovascular disease: An observational study. BMC Public Health 2012, 12, 466. [Google Scholar] [CrossRef]
- Lanki, T.; Siponen, T.; Ojala, A.; Korpela, K.; Pennanen, A.; Tiittanen, P.; Tsunetsugu, Y.; Kagawa, T.; Tyrväinen, L. Acute effects of visits to urban green environments on cardiovascular physiology in women: A field experiment. Environ. Res. 2017, 159, 176–185. [Google Scholar] [CrossRef]
- Kardan, O.; Gozdyra, P.; Misic, B.; Moola, F.; Palmer, L.J.; Paus, T.; Berman, M.G. Neighborhood greenspace and health in a large urban center. Sci. Rep. 2015, 5, 11610. [Google Scholar] [CrossRef]
- Abelt, K.; McLafferty, S. Green streets: Urban green and birth outcomes. Int. J. Environ. Res. Public Health 2017, 14, 771. [Google Scholar] [CrossRef]
- Lovasi, G.S.; Quinn, J.W.; Neckerman, K.M.; Perzanowski, M.S.; Rundle, A. Children living in areas with more street trees have lower prevalence of asthma. J. Epidemiol. Community Health 2008, 62, 647–649. [Google Scholar] [CrossRef] [PubMed]
- Mowafi, M.; Khadr, Z.; Bennett, G.; Hill, A.; Kawachi, I.; Subramanian, S.V. Is access to neighborhood green space associated with BMI among Egyptians? A multilevel study of Cairo neighborhoods. Health Place 2012, 18, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Yu, Y.; Xia, W.; Masri, S.; Sami, M.; Hu, Z.; Yu, Z.; Wu, J. Cardiovascular diseases in middle aged and older adults in China: The joint effects and mediation of different types of physical exercise and neighborhood greenness and walkability. Environ. Res. 2018, 167, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Chor, D.; Pinho Ribeiro, A.L.; Sá Carvalho, M.; Duncan, B.B.; Andrade Lotufo, P.; Araújo Nobre, A.; de Aquino, E.M.L.L.; Schmidt, M.I.; Griep, R.H.; Molina, M.D.C.B.; et al. Prevalence, awareness, treatment and influence of socioeconomic variables on control of high blood pressure: Results of the ELSA-Brasil study. PLoS ONE 2015, 10, e0127382. [Google Scholar] [CrossRef]
- Aquino, E.M.L.; Barreto, S.M.; Bensenor, I.M.; Carvalho, M.S.; Chor, D.; Duncan, B.B.; Lotufo, P.A.; Mill, J.G.; Molina, M.D.C.; Mota, E.L.A.; et al. Brazilian longitudinal study of adult health (ELSA-Brasil): Objectives and design. Am. J. Epidemiol. 2012, 175, 315–324. [Google Scholar] [CrossRef]
- Schmidt, M.I.; Hoffmann, J.F.; de Fátima Sander Diniz, M.; Lotufo, P.A.; Griep, R.H.; Bensenor, I.M.; Mill, J.G.; Barreto, S.M.; Aquino, E.M.L.; Duncan, B.B. High prevalence of diabetes and intermediate hyperglycemia—The Brazilian longitudinal study of adult health (ELSA-Brasil). Diabetol. Metab. Syndr. 2014, 6, 123. [Google Scholar] [CrossRef]
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report; US Department of Health and Human Services: Washington, DC, USA, 2008. [Google Scholar]
- Machado, L.B.M.; Silva, B.L.S.; Garcia, A.P.; Oliveira, R.A.M.; Barreto, S.M.; Fonseca, M.; de Jesus, M.; Lotufo, P.A.; Bensenor, I.M.; Santos, I.S. Ideal cardiovascular health score at the ELSA-Brasil baseline and its association with sociodemographic characteristics. Int. J. Cardiol. 2018, 254, 333–337. [Google Scholar] [CrossRef]
- Mill, J.G.; da Silva, A.B.T.; Baldo, M.P.; Molina, M.C.B.; Rodrigues, S.L. Correlation between sodium and potassium excretion in 24- and 12-h urine samples. Braz. J. Med. Biol. Res. 2012, 45, 799–805. [Google Scholar] [CrossRef]
- Bensenor, I.M.; Griep, R.H.; Pinto, K.A.; de Faria, C.P.; Felisbino-Mendes, M.; Caetano, E.I.; da Silva Albuquerque, L.; Schmidt, M.I.; Bensenor, I.M.; Griep, R.H.; et al. Rotinas de organização de exames e entrevistas no centro de investigação ELSA-Brasil. Revista de Saúde Pública 2013, 47, 37–47. [Google Scholar] [CrossRef]
- Schmidt, M.I.; Griep, R.H.; Passos, V.M.; Luft, V.C.; Goulart, A.C.; de Souza Menezes, G.M.; Molina, M.D.C.B.; Vigo, A.; Nunes, M.A. Strategies and development of quality assurance and control in the ELSA-Brasil. Revista de Saude Publica 2013, 47. [Google Scholar] [CrossRef]
- IBGE População. Available online: https://cidades.ibge.gov.br/brasil/sp/sao-paulo/panorama (accessed on 3 January 2020).
- Silva, L.S.E. A Cidade e a Floresta: O impacto da Expansão Urbana Sobre Áreas Vegetadas na Região Metropolitana de São Paulo (RMSP). Ph.D. Thesis, University of São Paulo, São Paulo, Brazil, August 2013. [Google Scholar]
- Amato-Lourenço, L.F.; Moreira, T.C.L.; de Arantes, B.L.; da Silva Filho, D.F.; Mauad, T. Metrópoles, cobertura vegetal, áreas verdes e saúde. Estudos Avançados 2016, 30, 113–130. [Google Scholar]
- De Miranda, R.M.; de Fatima Andrade, M.; Fornaro, A.; Astolfo, R.; de Andre, P.A.; Saldiva, P. Urban air pollution: A representative survey of PM2.5 mass concentrations in six Brazilian cities. Air Qual. Atmos. Health 2012, 5, 63–77. [Google Scholar] [CrossRef] [PubMed]
- São Paulo City Government. Sistema de Consulta do Mapa Digital da Cidade de São Paulo. Available online: http://geosampa.prefeitura.sp.gov.br/ (accessed on 4 August 2018).
- Rodriguez-Galiano, V.F.; Ghimire, B.; Rogan, J.; Chica-Olmo, M.; Rigol-Sanchez, J.P. An assessment of the effectiveness of a random forest classifier for land-cover classification. ISPRS J. Photogramm. Remote Sens. 2012, 67, 93–104. [Google Scholar] [CrossRef]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Gislason, P.O.; Benediktsson, J.A.; Sveinsson, J.R. Random forests for land cover classification. Pattern Recognit. Lett. 2006, 27, 294–300. [Google Scholar] [CrossRef]
- Jackson, R.D.; Huete, A.R. Interpreting vegetation indices. Prev. Vet. Med. 1991, 11, 185–200. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. An application of hierarchical kappa-type statistics in the assessment of majority agreement among multiple observers. Biometrics 1977, 33, 363–374. [Google Scholar] [CrossRef]
- World Health Organization. Urban Green Spaces and Health. A Review of Evidence; WHO: Copenhagen, Denmark, 2016. [Google Scholar]
- São Paulo City Government. Conheça um Pouco mais das Secretaria Municipal das Prefeituras Regionais da Cidade de São Paulo. Available online: http://www.prefeitura.sp.gov.br/cidade/secretarias/regionais/subprefeituras/index.php?p=8978 (accessed on 6 December 2018).
- Marguti, O.B.; Aurélio, C.M.; Favarão, C.B. Territórios em números: Insumos para políticas públicas a partir da análise do IDHM e do IVS de UHDs e regiões metropolitanas brasileiras, livro 2; IPEA: Brasília, Brazil, 2017; p. 224. [Google Scholar]
- Reid, C.; Clougherty, J.; Shmool, J.; Kubzansky, L. Is All urban green space the same? A comparison of the health benefits of trees and grass in New York City. Int. J. Environ. Res. Public Health 2017, 14, 1411. [Google Scholar] [CrossRef]
- Brook, R.D.M.; Rajagopalan, S.; Pope, C.A.I.; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.M.; Mittleman, M.A.M.; et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef]
- Maher, B.A.; Ahmed, I.A.M.; Davison, B.; Karloukovski, V.; Clarke, R. Impact of roadside tree lines on indoor concentrations of traffic-derived particulate matter. Environ. Sci. Technol. 2013, 47, 13737–13744. [Google Scholar] [CrossRef]
- Erbas, B.; Jazayeri, M.; Lambert, K.A.; Katelaris, C.H.; Prendergast, L.A.; Tham, R.; Parrodi, M.J.; Davies, J.; Newbigin, E.; Abramson, M.J. Outdoor pollen is a trigger of child and adolescent asthma emergency department presentations: A systematic review and meta-analysis. Allergy 2018, 73, 1632–1641. [Google Scholar] [CrossRef] [PubMed]
- Lambert, K.A.; Lodge, C.; Lowe, A.J.; Prendergast, L.A.; Thomas, P.S.; Bennett, C.M.; Abramson, M.J.; Dharmage, S.C.; Erbas, B. Pollen exposure at birth and adolescent lung function, and modification by residential greenness. Allergy 2019, 74. [Google Scholar] [CrossRef] [PubMed]
- Silveira, C.; Tchepel, O. Multiscale analysis of satellite-derived vegetation parameters for biogenic VOC emission modeling. In Proceedings of the First International Conference on Remote Sensing and Geoinformation of the Environment, Paphos, Cyprus, 8–10 April 2013. [Google Scholar]
- Brazienė, A.; Venclovienė, J.; Tamošiūnas, A.; Dėdelė, A.; Lukšienė, D.; Radišauskas, R. The influence of proximity to city parks and major roads on the development of arterial hypertension. Scand. J. Public Health 2018, 46, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Treff, C.; Benseñor, I.M.; Lotufo, P.A. Leisure-time and commuting physical activity and high blood pressure: The Brazilian longitudinal study of adult health (ELSA-Brasil). J. Hum. Hypertens. 2017, 31, 278–283. [Google Scholar] [CrossRef]
- Donovan, G.H. Including public-health benefits of trees in urban-forestry decision making. Urban For. Urban Green. 2017, 22, 120–123. [Google Scholar] [CrossRef]
- Cohen, D.A.; McKenzie, T.L.; Sehgal, A.; Williamson, S.; Golinelli, D.; Lurie, N. Contribution of public parks to physical activity. Am. J. Public Health 2007, 97, 509–514. [Google Scholar] [CrossRef]
- Bjork, J.; Albin, M.; Grahn, P.; Jacobsson, H.; Ardo, J.; Wadbro, J.; Ostergren, P.-O.; Skarback, E. Recreational values of the natural environment in relation to neighbourhood satisfaction, physical activity, obesity and wellbeing. J. Epidemiol. Community Health 2008, 62, e2. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Broomhall, M.H.; Knuiman, M.; Collins, C.; Douglas, K.; Ng, K.; Lange, A.; Donovan, R.J. Increasing walking: How important is distance to, attractiveness, and size of public open space? Am. J. Prev. Med. 2005, 28, 169–176. [Google Scholar] [CrossRef]
- Nielsen, T.S.; Hansen, K.B. Do green areas affect health? Results from a Danish survey on the use of green areas and health indicators. Health Place 2007, 13, 839–850. [Google Scholar] [CrossRef]
- Akpinar, A. How is quality of urban green spaces associated with physical activity and health? Urban. For. Urban. Green. 2016, 16, 76–83. [Google Scholar] [CrossRef]
- Ward Thompson, C.; Roe, J.; Aspinall, P.; Mitchell, R.; Clow, A.; Miller, D. More green space is linked to less stress in deprived communities: Evidence from salivary cortisol patterns. Landsc. Urban. Plan. 2012, 105, 221–229. [Google Scholar] [CrossRef]
- Tamosiunas, A.; Grazuleviciene, R.; Luksiene, D.; Dedele, A.; Reklaitiene, R.; Baceviciene, M.; Vencloviene, J.; Bernotiene, G.; Radisauskas, R.; Malinauskiene, V.; et al. Accessibility and use of urban green spaces, and cardiovascular health: Findings from a Kaunas cohort study. Environ. Health 2014, 13, 20. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Huxley, R.; Li, L.; Anna, V.; Xie, G.; Yao, C.; Woodward, M.; Li, X.; Chalmers, J.; Gao, R. Prevalence, awareness, treatment, and control of hypertension in China: Data from the China national nutrition and health survey 2002. Circulation 2008, 118, 2679–2686. [Google Scholar] [CrossRef]
- Lin, H.-C.; Lin, Y.-J.; Liu, T.-C.; Chen, C.-S.; Chiu, W.-T. Urbanization and stroke prevalence in Taiwan: Analysis of a nationwide survey. J. Urban Health 2007, 84, 604–614. [Google Scholar] [CrossRef] [PubMed]
- Vieira, J.; Matos, P.; Mexia, T.; Silva, P.; Lopes, N.; Freitas, C.; Correia, O.; Santos-Reis, M.; Branquinho, C.; Pinho, P. Green spaces are not all the same for the provision of air purification and climate regulation services: The case of urban parks. Environ. Res. 2018, 160, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Agyemang, C.; Hooijdonk, C.V.; Wendel-Vos, W.; Lindeman, E.; Stronks, K.; Droomers, M. The association of neighbourhood psychosocial stressors and self-rated health in Amsterdam, the Netherlands. J. Epidemiol. Community Health 2007, 61, 1042–1049. [Google Scholar] [CrossRef]
- Dadvand, P.; Sunyer, J.; Basagana, X.; Ballester, F.; Lertxundi, A.; Fernandez-Somoano, A.; Estarlich, M.; Garcia-Esteban, R.; Mendez, M.A.; Nieuwenhuijsen, M.J. Surrounding greenness and pregnancy outcomes in four Spanish birth cohorts. Environ. Health Perspect. 2012, 120, 1481–1487. [Google Scholar] [CrossRef]
- Hystad, P.; Davies, H.W.; Frank, L.; Van Loon, J.; Gehring, U.; Tamburic, L.; Brauer, M. Residential greenness and birth outcomes: Evaluating the influence of spatially correlated built-environment factors. Environ. Health Perspect. 2014, 122, 1095–1102. [Google Scholar] [CrossRef]
- James, P.; Banay, R.F.; Hart, J.E.; Laden, F. A review of the health benefits of greenness. Curr. Epidemiol. Rep. 2015, 2, 131–142. [Google Scholar] [CrossRef]
- Maas, J.; Verheij, R.A.; Groenewegen, P.P.; De Vries, S.; Spreeuwenberg, P. Green space, urbanity, and health: How strong is the relation? J. Epidemiol. Community Health 2006, 60, 587–592. [Google Scholar] [CrossRef]
- Donovan, G.H.; Butry, D.T.; Michael, Y.L.; Prestemon, J.P.; Liebhold, A.M.; Gatziolis, D.; Mao, M.Y. The relationship between trees and human health: Evidence from the spread of the emerald ash borer. Am. J. Prev. Med. 2013, 44, 139–145. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Socioeconomic Variables | Groups | Results |
|---|---|---|
| Gender | Man | 44.0% |
| Woman | 56.0% | |
| Age (years) | Mean | 52.3 |
| Range | 35–74 | |
| SD * | ±9.2 | |
| Educational level | Lower than high school | 12.4% |
| High school | 34.1% | |
| College or above | 41.9% | |
| Income | Low income—<USD1245 | 25.0% |
| High income—≥USD3320 | 32.0% | |
| Medium income—USD1245–3319 | 41.9% | |
| Race | White | 62.1% |
| Mixed | 18.8% | |
| Black | 11.3% | |
| Other | 6.3% |
| Risk Factor Variables | Groups | Results |
|---|---|---|
| Smoking habits | Current smoker | 16.06% |
| Past smoker | 30.84% | |
| Never smoked | 53.10% | |
| Body mass index (BMI) | Mean | 27.10 |
| SD | ±4.85 | |
| Physical activity | Ideal | 26.07% |
| Intermediate | 12.08% | |
| Poor | 61.85% | |
| Excessive drink | No | 94.55% |
| Yes | 5.45% | |
| Hypertension | No | 67.47% |
| Yes | 32.53% | |
| Diabetes | No | 76.67% |
| Yes | 20.33% | |
| Dyslipidemia | No | 42.05% |
| Yes | 57.95% | |
| Salt consumption (g) According to sodium excretion | <3 g | 2.01% |
| 3–5.9 g | 14.86% | |
| 6–8.9 g | 25.23% | |
| 9–11.9 g | 22.16% | |
| 12–14.9 g | 16.11% | |
| 15–17.9 g | 8.75% | |
| >18 g | 10.88% |
| Variable | Crude | Model 1 Adjusted | Model 2 Adjusted |
|---|---|---|---|
| OR (CI) | OR (CI) | OR (CI) | |
| Street trees (300 m buffer) | 1.037 (0.984 to 1.092) | 1.068 (1.010 to 1.131) * | 1.059 (0.996 to 1.126) ” |
| Street trees (distric) | 0.980 (0.937 to 1.024) | 0.988 (0.940 to 1.038) | 0.988 (0.937 to 1.043) |
| Street trees (government) | 0.922 (0.875 to 1.024) ** | 0.929 (0.878 to 0.984) * | 0.937 (0.881 to 0.996) * |
| Green space (300 m buffer) | 0.998 (0.922 to 1.004) | 0.998 (0.992 to 1.004) | 0.999 (0.992 to 1.006) |
| Green space(distric) | 0.993 (0.987 to 1.000) ” | 0.992 (0.984 to 0.999) | 0.993 (0.985 to 1.001) ” |
| Green space (government) | 0.991 (0.981 to 1.002) | 0.992 (0.980 to 1.003) | 0.991 (0.978 to 1.003) |
| Tree canopy (300 m buffer) | 0.998 (0.991 to 1.005) | 0.998 (0.991 to 1.005) | 1.000 (0.992 to 1.008) |
| Tree canopy (distric) | 0.990 (0.981 to 0.999) * | 0.988 (0.978 to 0.997) * | 0.990 (0.980 to 1.000) ” |
| Grass (300 m buffer) | 0.994 (0.976 to 1.014) | 0.993 (0.972 to 1.014) | 0.993 (0.971 to 1.015) |
| Grass (distric) | 1.000 (0.977 to 1.022) | 0.994 (0.970 to 1.018) | 0.992 (0.967 to 1.019) |
| Roofs (300 m buffer) | 1.005 (0.999 to 1.011) ” | 1.004 (0.997 to 1.011) | 1.004 (0.997 to 1.011) |
| Roofs (distric) | 1.010 (1.001 to 1.081) * | 1.012 (1.003 to 1.021) ** | 1.011 (1.002 to 1.021) * |
| Parks less than 1 km | 0.921 (0.826 to 1.027) | 0.902 (0.801 to 1.015) | 0.876 (0.769 to 0.998) * |
| 1 park within 1 km | 0.940 (0.797 to 1.108) | 0.943 (0.789 to 1.126) | 0.930 (0.766 to 1.127) |
| 2 parks within 1 km | 0828 (0.641 to 1.069) | 0.763 (0.577 to 1.009) ” | 0.724 (0.532 to 0.986) * |
| 3 parks within 1 km | 1.002 (0.090 to 1.077 | 1.021 (0.952 to 5.061) | 0.000 (0.000 to 0.000) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreira, T.C.L.; Polizel, J.L.; Santos, I.d.S.; Silva Filho, D.F.; Bensenor, I.; Lotufo, P.A.; Mauad, T. Green Spaces, Land Cover, Street Trees and Hypertension in the Megacity of São Paulo. Int. J. Environ. Res. Public Health 2020, 17, 725. https://doi.org/10.3390/ijerph17030725
Moreira TCL, Polizel JL, Santos IdS, Silva Filho DF, Bensenor I, Lotufo PA, Mauad T. Green Spaces, Land Cover, Street Trees and Hypertension in the Megacity of São Paulo. International Journal of Environmental Research and Public Health. 2020; 17(3):725. https://doi.org/10.3390/ijerph17030725
Chicago/Turabian StyleMoreira, Tiana C. L., Jefferson L. Polizel, Itamar de Souza Santos, Demóstenes F. Silva Filho, Isabela Bensenor, Paulo A. Lotufo, and Thais Mauad. 2020. "Green Spaces, Land Cover, Street Trees and Hypertension in the Megacity of São Paulo" International Journal of Environmental Research and Public Health 17, no. 3: 725. https://doi.org/10.3390/ijerph17030725
APA StyleMoreira, T. C. L., Polizel, J. L., Santos, I. d. S., Silva Filho, D. F., Bensenor, I., Lotufo, P. A., & Mauad, T. (2020). Green Spaces, Land Cover, Street Trees and Hypertension in the Megacity of São Paulo. International Journal of Environmental Research and Public Health, 17(3), 725. https://doi.org/10.3390/ijerph17030725