
The Tasmanian Emergency Care Outcomes Registry (TECOR) Protocol




Abstract
1. Introduction
1.1. The Nature and Safety of Emergency Medicine and Emergency Departments
1.2. Routinely Collected Data in Australia
1.3. Clinical Quality Registries
1.4. Emergency Care Clinical Quality Registries
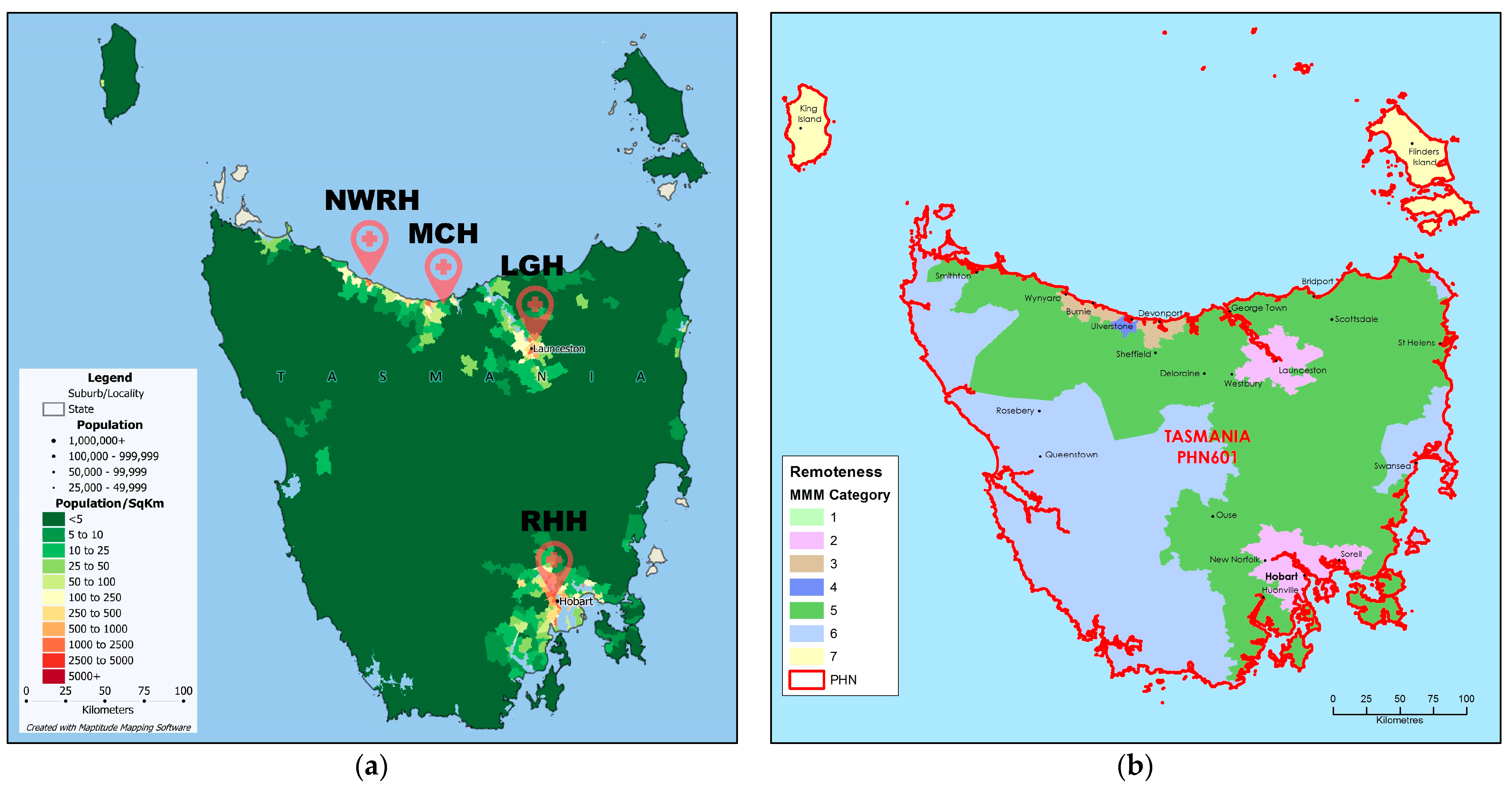
1.5. Australian and Tasmanian Emergency Care
1.6. Establishing the TECOR
2. Study Objectives
3. Materials and Methods
3.1. CQR Categorisation
3.2. Selection of Hospitals
3.3. Patient Eligibility
3.3.1. Inclusion Criteria
3.3.2. Exclusion Criteria
3.4. Data Collection
3.5. Follow-Up
3.6. Data Management and Security
3.7. Statistical Analysis
4. Reporting
5. Discussion
5.1. Future Studies: Nested Trials
5.2. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Australasian College for Emergency Medicine. About. Available online: https://acem.org.au/Content-Sources/About (accessed on 27 March 2024).
- Australasian College for Emergency Medicine. Policy on Standard Terminology. Available online: https://acem.org.au/getmedia/e5cf7ac4-dae5-4193-be9a-6746b0d85009/Policy_on_Standard_Terminology (accessed on 27 March 2024).
- Trzeciak, S.; Rivers, E.P. Emergency department overcrowding in the United States: An emerging threat to patient safety and public health. Emerg. Med. J. 2003, 20, 402–405. [Google Scholar] [CrossRef]
- Schneider, S.M.; Gardner, A.F.; Weiss, L.D.; Wood, J.P.; Ybarra, M.; Beck, D.M.; Stauffer, A.R.; Wilkerson, D.; Brabson, T.; Jennings, A.; et al. The future of emergency medicine. J. Emerg. Nurs. 2010, 36, 330–335. [Google Scholar] [CrossRef]
- Ramlakhan, S.; Qayyum, H.; Burke, D.; Brown, R. The safety of emergency medicine. Emerg. Med. J. 2016, 33, 293–299. [Google Scholar] [CrossRef]
- Al-Qahtani, M.F.; Khubrani, F.Y. Exploring Potential Association Between Emergency Department Crowding Status and Patients’ Length of Stay at a University Hospital in Saudi Arabia. Open Access Emerg. Med. 2021, 13, 257–263. [Google Scholar] [CrossRef]
- Pines, J.M.; Garson, C.; Baxt, W.G.; Rhodes, K.V.; Shofer, F.S.; Hollander, J.E. ED crowding is associated with variable perceptions of care compromise. Acad. Emerg. Med. 2007, 14, 1176–1181. [Google Scholar] [CrossRef]
- Asaro, P.V.; Lewis, L.M.; Boxerman, S.B. Emergency Department Overcrowding: Analysis of the Factors of Renege Rate. Acad. Emerg. Med. 2007, 14, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Bentley, J.A.; Thakore, S.; Morrison, W.; Wang, W. Emergency Department redirection to primary care: A prospective evaluation of practice. Scott. Med. J. 2017, 62, 2–10. [Google Scholar] [CrossRef]
- Weiss, S.J.; Derlet, R.; Arndahl, J.; Ernst, A.A.; Richards, J.; Fernández-Frankelton, M.; Schwab, R.; Stair, T.O.; Vicellio, P.; Levy, D.; et al. Estimating the Degree of Emergency Department Overcrowding in Academic Medical Centers: Results of the National ED Overcrowding Study (NEDOCS). Acad. Emerg. Med. 2004, 11, 38–50. [Google Scholar] [CrossRef]
- Weiss, S.J.; Rogers, D.B.; Maas, F.; Ernst, A.A.; Nick, T.G. Evaluating community ED crowding: The Community ED Overcrowding Scale study. Am. J. Emerg. Med. 2014, 32, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Sprivulis, P.C.; Da Silva, J.-A.; Jacobs, I.G.; Frazer, A.R.L.; Jelinek, G.A. The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments. Med. J. Aus. 2006, 184, 616. [Google Scholar] [CrossRef] [PubMed]
- Guttmann, A.; Schull, M.J.; Vermeulen, M.J.; Stukel, T.A. Association between waiting times and short term mortality and hospital admission after departure from emergency department: Population based cohort study from Ontario, Canada. BMJ 2011, 342, d2983. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. About Our Data. Available online: https://www.aihw.gov.au/about-our-data (accessed on 27 March 2024).
- Australian Institute of Health and Welfare. Emergency Department Care. Available online: https://www.aihw.gov.au/reports-data/myhospitals/sectors/emergency-department-care (accessed on 27 March 2024).
- Australian Institute of Health and Welfare. Emergency Department Care Activity. Available online: https://www.aihw.gov.au/reports-data/myhospitals/intersection/activity/ed (accessed on 27 March 2024).
- Evans, S.M.; Scott, I.A.; Johnson, N.P.; Cameron, P.A.; McNeil, J.J. Development of clinical-quality registries in Australia: The way forward. Med. J. Aust. 2011, 194, 360–363. [Google Scholar] [CrossRef] [PubMed]
- International Classifications in Australia. Australian Institute of Health and Welfare. Available online: https://www.aihw.gov.au/about-us/international-collaboration/australian-collaborating-centre-for-who/international-classifications-in-australia (accessed on 27 March 2024).
- Emergency Department ICD-10-AM Principal Diagnosis Short List. IHACPA. Available online: https://www.ihacpa.gov.au/health-care/classification/emergency-care/emergency-department-icd-10-am-principal-diagnosis-short-list (accessed on 27 March 2024).
- Australian Commission on Safety and Quality in Health Care. Framework for Australian Clinical Quality Registries. Available online: https://www.safetyandquality.gov.au/sites/default/files/migrated/Framework-for-Australian-Clinical-Quality-Registries.pdf (accessed on 27 March 2024).
- Larsson, S.; Lawyer, P.; Garellick, G.; Lindahl, B.; Lundström, M. Use of 13 disease registries in 5 countries demonstrates the potential to use outcome data to improve health care’s value. Health Aff. 2012, 31, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Ahern, S.; Evans, S.; Hopper, I.; Zalcberg, J. Towards a strategy for clinical quality registries in Australia. Aust. Health Rev. 2019, 43, 284–287. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.E.; Ramsay, N.; Mitchell, R.; McDougall, C.; Harris, I.A.; Hallen, J.; Ward, N.; Hurring, S.; Harvey, L.A.; Armstrong, E.; et al. Improving hip fracture care: A five-year review of the early contributors to the Australian and New Zealand Hip Fracture Registry. Australas. J. Ageing 2024, 43, 31–42. [Google Scholar] [CrossRef]
- Fitzgerald, M.C.; Curtis, K.; Cameron, P.A.; Ford, J.E.; Howard, T.S.; Crozier, J.A.; Fitzgerald, A.; Gruen, R.L.; Pollard, C. The Australian Trauma Registry. ANZ J. Surg. 2019, 89, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Cadilhac, D.A.; Andrew, N.E.; Lannin, N.A.; Middleton, S.; Levi, C.R.; Dewey, H.M.; Grabsch, B.; Faux, S.; Hill, K.; Grimley, R.; et al. Quality of Acute Care and Long-Term Quality of Life and Survival. Stroke 2017, 48, 1026–1032. [Google Scholar] [CrossRef]
- Zehtabchi, S.; Nishijima, D.K.; McKay, M.P.; Mann, N.C. Trauma registries: History, logistics, limitations, and contributions to emergency medicine research. Acad. Emerg. Med. 2011, 18, 637–643. [Google Scholar] [CrossRef]
- Australian Commission on Safety and Quality in Health Care. Australian Register of Clinical Registries. Available online: https://www.safetyandquality.gov.au/publications-and-resources/australian-register-clinical-registries (accessed on 27 March 2024).
- Secombe, P.; Millar, J.; Litton, E.; Chavan, S.; Hensman, T.; Hart, G.K.; Slater, A.; Herkes, R.; Huckson, S.; Pilcher, D.V. Thirty years of ANZICS CORE: A clinical quality success story. Crit. Care Resusc. 2023, 25, 43–46. [Google Scholar] [CrossRef]
- Webb, S.A.; Pettilä, V.; Seppelt, I.; Bellomo, R.; Bailey, M.; Cooper, D.J.; Cretikos, M.; Davies, A.R.; Finfer, S.; Harrigan, P.W.; et al. Critical care services and 2009 H1N1 influenza in Australia and New Zealand. N. Engl. J. Med. 2009, 361, 1925–1934. [Google Scholar] [CrossRef]
- Reilly, J.R.; Deng, C.; Brown, W.A.; Brown, D.; Gabbe, B.J.; Hodgson, C.L.; Myles, P.S. Towards a national perioperative outcomes registry: A survey of perioperative electronic medical record utilisation to support quality assurance and research at Australian and New Zealand College of Anaesthetists Clinical Trials Network hospitals in Australia. Anaesth. Intens. Care 2022, 50, 189–196. [Google Scholar] [CrossRef]
- Smith, J.L.; Soderstrom, J.; Dawson, A.; Alfred, S.; Greene, S.; Isoardi, K.; McCutcheon, D.; Oosthuizen, F.; Ezard, N.; Burcham, J.; et al. The Emerging Drugs Network of Australia: A toxicosurveillance system of illicit and emerging drugs in the emergency department. Emerg. Med. Australas. 2022, 34, 58–64. [Google Scholar] [CrossRef]
- Alkhouri, H.; Vassiliadis, J.; Murray, M.; Mackenzie, J.; Tzannes, A.; McCarthy, S.; Fogg, T. Emergency airway management in Australian and New Zealand emergency departments: A multicentre descriptive study of 3710 emergency intubations. Emerg. Med. Australas. 2017, 29, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Cadilhac, D.A.; Lannin, N.A.; Anderson, C.S.; Levi, C.R.; Faux, S.; Price, C.; Middleton, S.; Lim, J.; Thrift, A.G.; Donnan, G.A. Protocol and Pilot Data for Establishing the Australian Stroke Clinical Registry. Int. J. Stroke 2010, 5, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Ekegren, C.L.; Edwards, E.R.; Page, R.; Hau, R.; de Steiger, R.; Bucknill, A.; Liew, S.; Oppy, A.; Gabbe, B.J. Twelve-month mortality and functional outcomes in hip fracture patients under 65 years of age. Injury 2016, 47, 2182–2188. [Google Scholar] [CrossRef]
- Taylor, A.; Kinsman, J.; Hawk, K.; D’Onofrio, G.; Malicki, C.; Malcom, B.; Goyal, P.; Venkatesh, A.K. Development and testing of data infrastructure in the American College of Emergency Physicians’ Clinical Emergency Data Registry for opioid-related research. J. Am. Coll. Emerg. Physicians Open 2022, 3, e12816. [Google Scholar] [CrossRef] [PubMed]
- Epstein, S.K.; Griffey, R.T.; Lin, M.P.; Augustine, J.J.; Goyal, P.; Venkatesh, A.K. Development of a qualified clinical data registry for emergency medicine. J. Am. Coll. Emerg. Physicians Open 2021, 2, e12547. [Google Scholar] [CrossRef] [PubMed]
- Brammen, D.; Greiner, F.; Kulla, M.; Otto, R.; Schirrmeister, W.; Thun, S.; Drösler, S.E.; Pollmanns, J.; Semler, S.C.; Lefering, R.; et al. AKTIN—The German Emergency Department Data Registry—Real-time data from emergency medicine: Implementation and first results from 15 emergency departments with focus on Federal Joint Committee’s guidelines on acuity assessment. Med. Klin. Intensivmed. Notfmed. 2022, 117, 24–33. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Clinical Registry. Available online: https://www.who.int/publications/m/item/who-clinical-registry (accessed on 27 March 2024).
- White, M.; O’Reilly, G.M.; Mitchell, R.D.; Noonan, M.; Hiller, R.; Mitra, B.; Paton, A.; Pristupa, K.; Luckhoff, C.; Smit, V.; et al. Informing the Alfred Registry for Emergency Care Project: An analysis of presenting complaint documentation in an emergency department. Emerg. Med. Australas. 2022, 34, 620–622. [Google Scholar] [CrossRef] [PubMed]
- Kloot, K.; Baker, T.R. Building a research-ready database of rural emergency presentations: The RAHDaR pilot study. Emerg. Med. Australas. 2019, 31, 126–128. [Google Scholar] [CrossRef]
- South Western Emergency Research Institute. Comprehensive Emergency Dataset for Research, innovation and Collaboration (CEDRIC). Available online: https://sweri.com.au/cedric/ (accessed on 27 March 2024).
- Australian Bureau of Statistics. National, State and Territory Population. Available online: https://www.abs.gov.au/statistics/people/population/national-state-and-territory-population/sep-2023 (accessed on 27 March 2024).
- Angeles, M.R.; Crosland, P.; Hensher, M. Challenges for Medicare and universal health care in Australia since 2000. Med. J. Aust. 2023, 218, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Whitson, R. Hospital Overcrowding, Wait Times Worst in Tasmania, Territories. ABC News. Available online: https://www.abc.net.au/news/2018-07-11/tasmanian-emergency-department-wait-times-worst-in-country/9972062 (accessed on 27 March 2024).
- Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS) Edition 3. ABS. Available online: https://www.abs.gov.au/statistics/standards/australian-statistical-geography-standard-asgs-edition-3/jul2021-jun2026/remoteness-structure/remoteness-areas (accessed on 20 March 2024).
- Department of Health and Aged Care. Modified Monash Model. Available online: https://www.health.gov.au/topics/rural-health-workforce/classifications/mmm?language=und&utm_source=health.gov.au&utm_medium=callout-auto-custom&utm_campaign=digital_transformation#what-is-the-mmm-used-for. (accessed on 20 March 2024).
- Caliper. Tasmania Population Density by Locality Maptitude Map. Available online: https://www.caliper.com/pdfs/tasmania-population-density-by-locality-maptitude-map.pdf (accessed on 14 February 2024).
- Australian Government Department of Health and Aged Care. Tasmania Primary Health Network (PHN) Map—Modified Monash Model (MMM) Remoteness Area. Available online: https://www.health.gov.au/resources/publications/tasmania-primary-health-network-phn-map-modified-monash-model-mmm-remoteness-area?language=en (accessed on 27 March 2024).
- O’Reilly, G.M.; Mitchell, R.D.; Rajiv, P.; Wu, J.; Brennecke, H.; Brichko, L.; Noonan, M.P.; Hiller, R.; Mitra, B.; Luckhoff, C.; et al. Epidemiology and clinical features of emergency department patients with suspected COVID-19: Initial results from the COVID-19 Emergency Department Quality Improvement Project (COVED-1). Emerg. Med. Australas. 2020, 32, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Australian Commission on Safety and Quality in Health Care. Legislation and Regulation Relating to Clinical Quality Registries; Australian Comission on Safet and Quality in Health Care: Sydney, Australia, 2020. [Google Scholar]
- Department of Health Victoria. Victorian Emergency Minimum Dataset (VEMD) Manual 2023–2024. Available online: https://www.health.vic.gov.au/publications/victorian-emergency-minimum-dataset-vemd-manual-2023-2024 (accessed on 14 February 2024).
- O’Reilly, G.M.; Mitchell, R.D.; Mitra, B.; Noonan, M.P.; Hiller, R.; Brichko, L.; Luckhoff, C.; Paton, A.; Smit, V.; Cameron, P.A. Informing emergency care for all patients: The Registry for Emergency Care (REC) Project protocol. Emerg. Med. Australas. 2020, 32, 687–691. [Google Scholar] [CrossRef] [PubMed]
- State of Tasmania. Disposal Schedule for Functional Records of Health Administration (DADA2525); Office of the State Archivist: Hobart, Australia, 2023. [Google Scholar]
- Australian Commission on Safety and Quality in Health Care. Clinical Outcome Feedback Loop; Australian Commission on Safety and Quality in Health Care: Sydney, Australia, 2022. [Google Scholar]
- Viviani, L.; Zolin, A.; Mehta, A.; Olesen, H.V. The European Cystic Fibrosis Society Patient Registry: Valuable lessons learned on how to sustain a disease registry. Orphanet J. Rare Dis. 2014, 9, 81. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Minimum Dataset | Additional Data |
|---|---|
| Age at presentation 1,2,3 Sex 1,2,3 Australian Postcode 1,2,3 Geographic remoteness, remoteness classification 1,2 Country of birth 1,2,3 Indigenous status 1,2,3 Hospital 1,2,3 Mode of arrival 1,2,3 Date of presentation 1,2,3 Time of presentation 1,2,3 Date of triage 1,2,3 Time of triage 1,2,3 ED end date 1,2,3 ED end time 1,2,3 Service episode length (total min) 1,2,3 Type of visit 1,2,3 Triage category 1,2,3 Date seen by medical officer 1,2,3 Time seen by medical officer 1,2,3 Emergency Department wait time 1,2 Disposition 1,2,3 ED stay—urgency-related group major diagnostic block 1,2 ED stay—principal diagnosis 1,2,3 ED stay—diagnosis classification type 1,2,3 ED stay—physical departure date 1,2,3 ED stay—physical departure time 1,2,3 Patient—compensable status 1,2,3 ED stay—additional diagnosis, code 1,2,3 Episode of admitted patient care—admission date 1,2 Episode of admitted patient care—admission time 1,2 Safety event(s) URN 1,3 Emergency Attendance ID 1,3 ED triage/presenting complaint 1,3 Admission time, date 1,2 | Episode of admitted patient care—length of stay in intensive care unit, total hours 1,2 Episode of admitted patient care—separation date 1,2 Episode of care—source of funding, patient funding source code 1,2 Episode of admitted patient care—separation mode 1,2 Episode of admitted patient care—number of days of hospital-in-the-home care 1,2 Episode of care—principal diagnosis, code 1,2,5 Episode of care—secondary diagnosis and beyond, code 1,2,5 Episode of admitted patient care—admission urgency status 1,2 Referred by 1,3 Referred to, position, specialty 1 Referred to time, date 1 Consultation, position, specialty 1 Consultation time, date 1 Bed request time, date 1 Bed available time, date Departure Status 1,3 Clinical observations 4 Pathology testing and blood products requests time, date and type 4 Pathology testing results and blood products given time and date 4 Imaging testing requests time, date and type 4 Imaging testing results time and date 4 Discharge method 1,3 Procedures performed 4 Medications prescribed including route and dose 4 Medical progress notes 1,4 Nursing progress notes 1 Goals of Care prior to arrival 1,4 Goals of Care at admission 1,4 Goals of Care at discharge 1,4 Hospital Capacity 2 Emergency Department Capacity 1 |
| Observational Trial | Trial Description |
|---|---|
| PROCSED 1 | A quality improvement database on the current clinical practice of procedural sedation in the ED in order to improve the quality of care |
| EDNA 2 | The Emerging Drugs Network of Australia (EDNA) brings together emergency physicians, toxicologists and forensic laboratories to establish a standardised ED toxicosurveillance system in Australia [31] |
| ANZEDAR 2 | A binational airway registry prospectively capturing intubations and factors associated with first attempt success [32] |
| MET Call Database 1 | A quality improvement database on the MET calls in the ED to identify challenges to improved patient care |
| AuSCR 2 | The Australian Stroke Clinical Registry aims to provide national, prospective, systematic data on processes and outcomes for stroke [33] |
| ANZHFR 2 | A clinical quality registry that collects data about older people admitted to hospital with a broken hip in Australia and New Zealand [34] |
| ANZTR 2 | Focuses on monitoring trauma care, from the time of incident to discharge from definitive care, in order to reflect and act upon emerging trends and demands on the trauma system across Australia and New Zealand [24] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, V.; Barrington, G.; Page, S. The Tasmanian Emergency Care Outcomes Registry (TECOR) Protocol. Emerg. Care Med. 2024, 1, 153-164. https://doi.org/10.3390/ecm1020017
Tran V, Barrington G, Page S. The Tasmanian Emergency Care Outcomes Registry (TECOR) Protocol. Emergency Care and Medicine. 2024; 1(2):153-164. https://doi.org/10.3390/ecm1020017
Chicago/Turabian StyleTran, Viet, Giles Barrington, and Simone Page. 2024. "The Tasmanian Emergency Care Outcomes Registry (TECOR) Protocol" Emergency Care and Medicine 1, no. 2: 153-164. https://doi.org/10.3390/ecm1020017
APA StyleTran, V., Barrington, G., & Page, S. (2024). The Tasmanian Emergency Care Outcomes Registry (TECOR) Protocol. Emergency Care and Medicine, 1(2), 153-164. https://doi.org/10.3390/ecm1020017