
Imaging Follow-Up of MSU Crystal Depletion

Abstract
1. Introduction
2. The Imaging Features of Gout
2.1. Ultrasonography
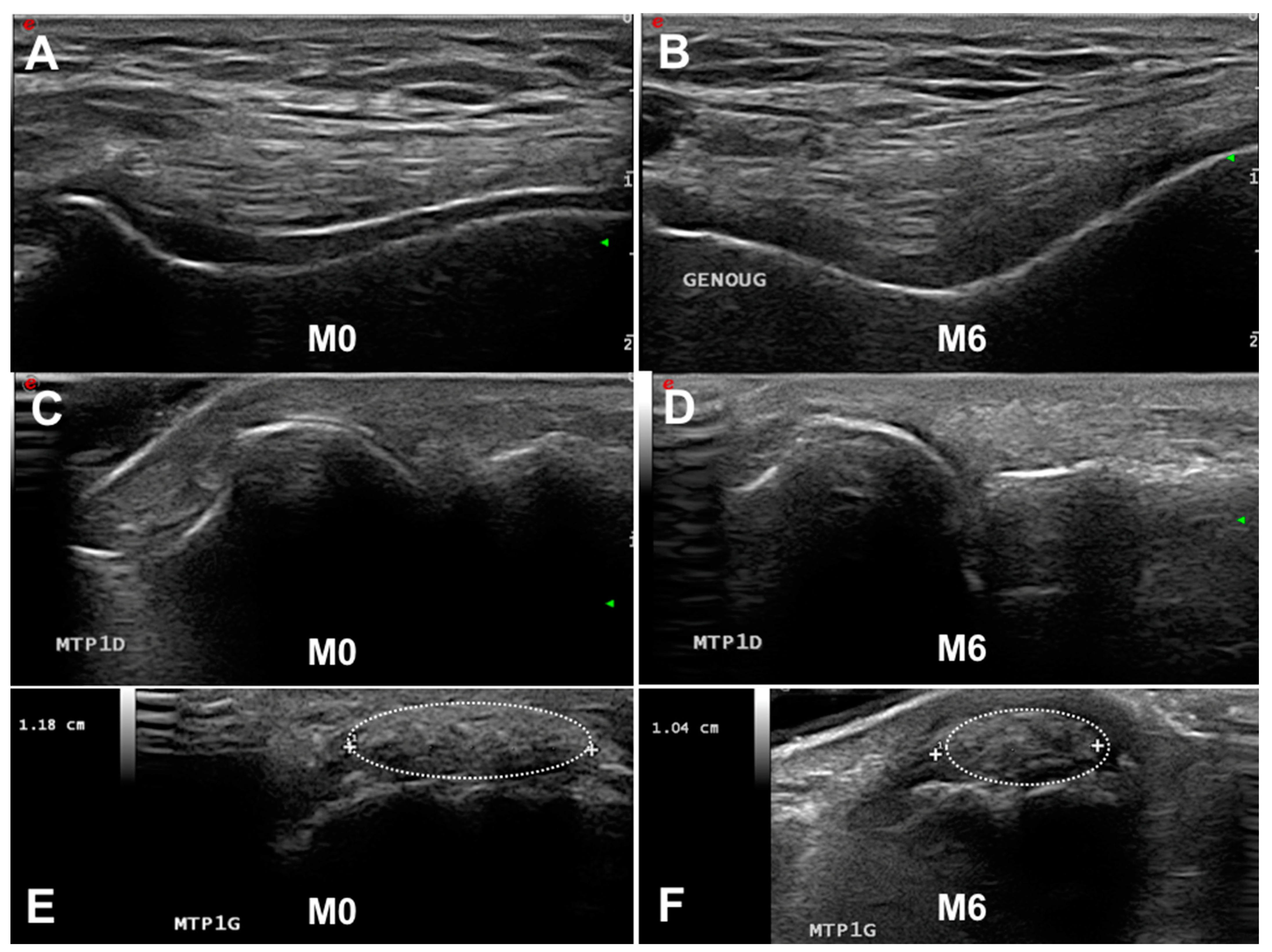
- Double contour sign: “abnormal hyperechoic band over the superficial margin of the anechoic cartilage, independent of the angle of insonation and which may be irregular, continuous, or intermittent and can distinguished from the cartilage interface sign” (Figure 1A,C). The DC sign must be searched preferentially at the first metatarsophalangeal joints (MTP1s), the trochleal cartilage of knees (suprapatellar plane in maximal flexion) and the talar cartilage.
- Tophus: “a circumscribed, inhomogenous, hyperechoic and/or hypoechoic aggregation (which may or may not generate a posterior acoustic shadow)” (Figure 1E,F). The main locations for detecting US tophus are the MTP1s and quadricipital and patellar tendons.
- Aggregates: “bright hyperechoic, isolated spots too small to fulfil the tophus definition and characterized by maintaining their high degree of reflectivity when the insonation angle is changed”.
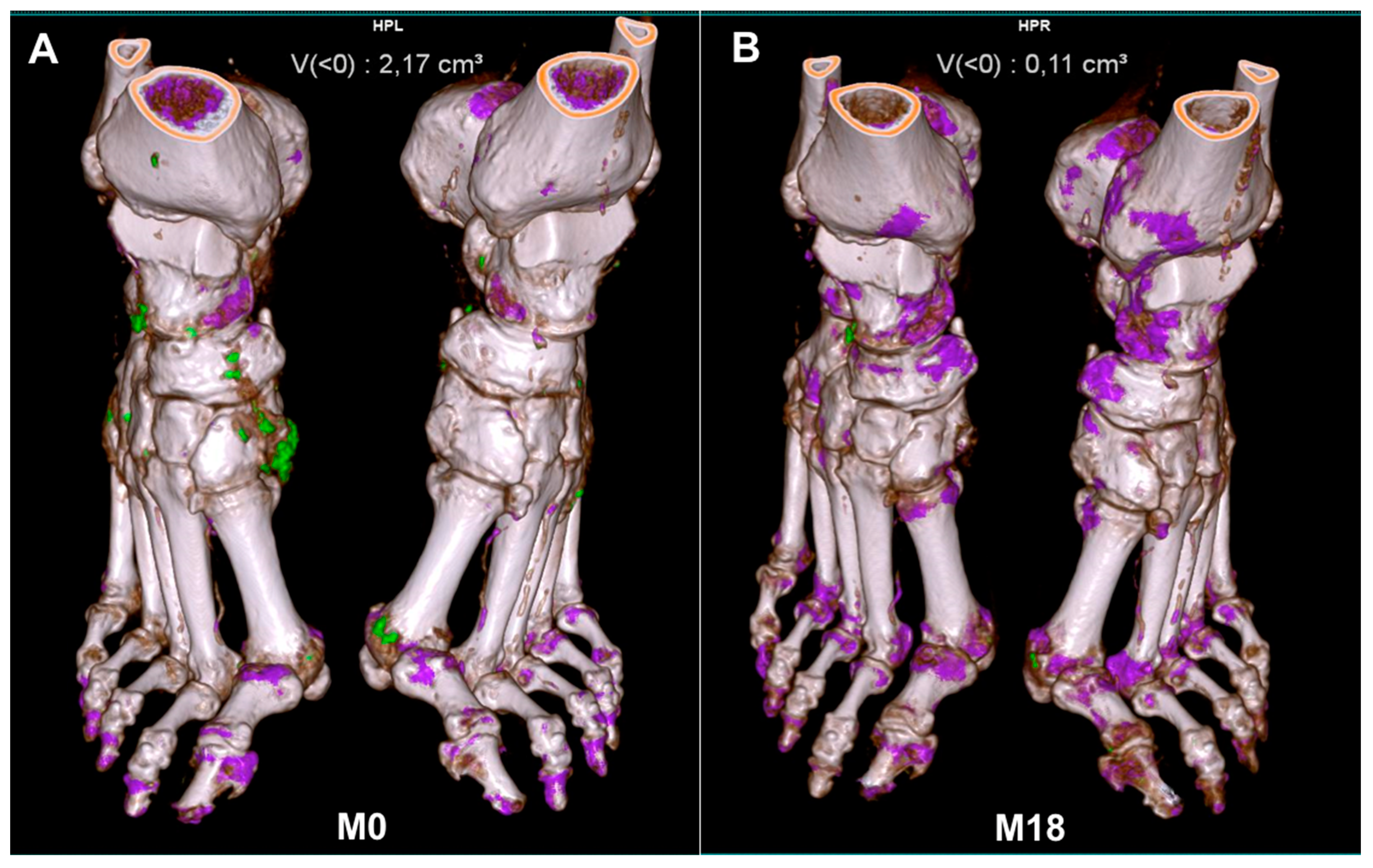
2.2. Dual-Energy CT
3. Scoring Imaging Features of Gout
3.1. Ultrasonography
3.1.1. Scoring
3.1.2. Which Joint to Analyze
3.2. Dual-Energy CT
3.2.1. Scoring
3.2.2. Which Joint to Analyze
4. The Ability of Imaging to Visualize the Dissolution of MSU Crystal Deposition
4.1. Ultrasonography
4.2. DECT
5. The Impact of Imaging on Relapse
5.1. Ultrasonography
5.2. Dual-Energy CT
6. Perspectives
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Richette, P.; Bardin, T. Gout. Lancet 2009, 375, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Bursill, D.; Taylor, W.J.; Terkeltaub, R.; Abhishek, A.; So, A.K.; Vargas-Santos, A.B.; Gaffo, A.L.; Rosenthal, A.; Tausche, A.-K.; Reginato, A.; et al. Gout, Hyperuricaemia and Crystal-Associated Disease Network (G-CAN) consensus statement regarding labels and definitions of disease states of gout. Ann. Rheum. Dis. 2019, 78, 1592–1600. [Google Scholar] [CrossRef] [PubMed]
- Chandratre, P.; Roddy, E.; Clarson, L.; Richardson, J.; Hider, S.L.; Mallen, C.D. Health-related quality of life in gout: A systematic review. Rheumatology 2013, 52, 2031–2040. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.; Belcher, J.; Nicholls, E.; Chandratre, P.; Blagojevic-Bucknall, M.; Hider, S.; A Lawton, S.; Mallen, C.D.; Muller, S.; Rome, K.; et al. Factors associated with change in health-related quality of life in people with gout: A 3-year prospective cohort study in primary care. Rheumatology 2022, 62, 2748–2756. [Google Scholar] [CrossRef]
- Kiadaliri, A.A.; Englund, M. Temporal trends and regional disparity in rheumatoid arthritis and gout hospitalizations in Sweden, 1998–2015. Clin. Rheumatol. 2018, 37, 825–830. [Google Scholar] [CrossRef]
- Lim, S.Y.; Lu, N.; Oza, A.; Fisher, M.; Rai, S.K.; Menendez, M.E.; Choi, H.K. Trends in Gout and Rheumatoid Arthritis Hospitalizations in the United States, 1993-2011. JAMA 2016, 315, 2345–2347. [Google Scholar] [CrossRef]
- Andrés, M.; Bernal, J.A.; Sivera, F.; Quilis, N.; Carmona, L.; Vela, P.; Pascual, E. Cardiovascular risk of patients with gout seen at rheumatology clinics following a structured assessment. Ann. Rheum. Dis. 2017, 76, 1263–1268. [Google Scholar] [CrossRef]
- Marty-Ané, A.; Norberciak, L.; Andrès, M.; Houvenagel, E.; Ducoulombier, V.; Legrand, J.; Budzik, J.-F.; Pascart, T. Crystal deposition measured with dual-energy computed tomography: Association with mortality and cardiovascular risks in gout. Rheumatology 2021, 60, 4855–4860. [Google Scholar] [CrossRef]
- Pascart, T.; Latourte, A.; Flipo, R.-M.; Chalès, G.; Coblentz-Baumann, L.; Cohen-Solal, A.; Ea, H.-K.; Grichy, J.; Letavernier, E.; Lioté, F.; et al. 2020 recommendations from the French Society of Rheumatology for the management of gout: Urate-lowering therapy. Jt. Bone Spine 2020, 87, 395–404. [Google Scholar] [CrossRef]
- Richette, P.; Doherty, M.; Pascual, E.; Barskova, V.; Becce, F.; Castañeda-Sanabria, J.; Coyfish, M.; Guillo, S.; Jansen, T.L.; Janssens, H.; et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann. Rheum. Dis. 2016, 76, 29–42. [Google Scholar] [CrossRef]
- FitzGerald, J.D.; Dalbeth, N.; Mikuls, T.; Brignardello-Petersen, R.; Guyatt, G.; Abeles, A.M.; Gelber, A.C.; Harrold, L.R.; Khanna, D.; King, C.; et al. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Care Res. 2020, 72, 744–760. [Google Scholar] [CrossRef] [PubMed]
- Goossens, J.; Lancrenon, S.; Lanz, S.; Ea, H.-K.; Lambert, C.; Guggenbuhl, P.; Saraux, A.; Delva, C.; Sahbane, S.; Lioté, F. GOSPEL 3: Management of gout by primary-care physicians and office-based rheumatologists in France in the early 21st century – comparison with 2006 EULAR Recommendations. Jt. Bone Spine 2017, 84, 447–453. [Google Scholar] [CrossRef]
- Richette, P.; Doherty, M.; Pascual, E.; Barskova, V.; Becce, F.; Castaneda, J.; Coyfish, M.; Guillo, S.; Jansen, T.; Janssens, H.; et al. 2018 updated European League Against Rheumatism evidence-based recommendations for the diagnosis of gout. Ann. Rheum. Dis. 2019, 79, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Ottaviani, S.; Bardin, T.; Richette, P. Usefulness of ultrasonography for gout. Jt. Bone Spine 2012, 79, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Filippucci, E.; Gutierrez, M.; Georgescu, D.; Salaffi, F.; Grassi, W. Hyaline cartilage involvement in patients with gout and calcium pyrophosphate deposition disease. An ultrasound study. Osteoarthr. Cartil. 2009, 17, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Ottaviani, S.; Allard, A.; Bardin, T.; Richette, P. Ultrasonography findings in early gout. Clin. Exp. Rheumatol. 2011, 29, 816–821. [Google Scholar] [PubMed]
- Ottaviani, S.; Richette, P.; Allard, A.; Ora, J.; Bardin, T. Ultrasonography in gout: A case-control study. Clin. Exp. Rheumatol. 2012, 30, 499–504. [Google Scholar]
- Thiele, R.G.; Schlesinger, N. Diagnosis of gout by ultrasound. Rheumatology 2007, 46, 1116–1121. [Google Scholar] [CrossRef]
- A Wright, S.; Filippucci, E.; McVeigh, C.; Grey, A.; McCarron, M.; Grassi, W.; Wright, G.D.; Taggart, A.J. High-resolution ultrasonography of the first metatarsal phalangeal joint in gout: A controlled study. Ann. Rheum. Dis. 2007, 66, 859–864. [Google Scholar] [CrossRef]
- Ogdie, A.; Taylor, W.J.; Neogi, T.; Fransen, J.; Jansen, T.L.; Schumacher, H.R.; Louthrenoo, W.; Vazquez-Mellado, J.; Eliseev, M.; McCarthy, G.; et al. Performance of Ultrasound in the Diagnosis of Gout in a Multicenter Study: Comparison With Monosodium Urate Monohydrate Crystal Analysis as the Gold Standard. Arthritis Rheumatol. 2016, 69, 429–438. [Google Scholar] [CrossRef]
- Filippou, G.; Miguel-Perez, M.; Coronel, L.; Sirotti, S.; Pacini, G.; Scanu, A.; Bong, D.; Möller, I.; EULAR Study Group on Anatomy for the Image. The ultrasonographic pseudo-double contour sign in calcium pyrophosphate deposition disease: An anatomic explanation and how to distinguish it from gout. Arthritis Rheumatol. 2023, 75, 639–640. [Google Scholar] [CrossRef] [PubMed]
- Cipolletta, E.; Abhishek, A.; Di Matteo, A.; Grassi, W.; Filippucci, E. Dynamic assessment of the double contour sign by ultrasonography helps to distinguish between gout and calcium pyrophosphate deposition disease. RMD Open 2023, 9, e002940. [Google Scholar] [CrossRef] [PubMed]
- Terslev, L.; Gutierrez, M.; Schmidt, W.A.; Keen, H.I.; Filippucci, E.; Kane, D.; Thiele, R.; Kaeley, G.; Balint, P.; Mandl, P.; et al. Ultrasound as an Outcome Measure in Gout. A Validation Process by the OMERACT Ultrasound Working Group. J. Rheumatol. 2015, 42, 2177–2181. [Google Scholar] [CrossRef] [PubMed]
- Terslev, L.; Gutierrez, M.; Christensen, R.; Balint, P.V.; Bruyn, G.A.; Sedie, A.D.; Filippucci, E.; Garrido, J.; Hammer, H.B.; Iagnocco, A.; et al. Assessing Elementary Lesions in Gout by Ultrasound: Results of an OMERACT Patient-based Agreement and Reliability Exercise. J. Rheumatol. 2015, 42, 2149–2154. [Google Scholar] [CrossRef]
- Christiansen, S.N.; Filippou, G.; Scirè, C.A.; Balint, P.V.; Bruyn, G.A.; Dalbeth, N.; Dejaco, C.; Sedie, A.D.; Filippucci, E.; Hammer, H.B.; et al. Consensus-based semi-quantitative ultrasound scoring system for gout lesions: Results of an OMERACT Delphi process and web-reliability exercise. Semin. Arthritis Rheum. 2021, 51, 644–649. [Google Scholar] [CrossRef]
- Filippou, G.; Pascart, T.; Iagnocco, A. Utility of Ultrasound and Dual Energy CT in Crystal Disease Diagnosis and Management. Curr. Rheumatol. Rep. 2020, 22, 1–8. [Google Scholar] [CrossRef]
- Neogi, T.; A Jansen, T.L.T.; Dalbeth, N.; Fransen, J.; Schumacher, H.R.; Berendsen, D.; Brown, M.; Choi, H.; Edwards, N.L.; Janssens, H.J.E.M.; et al. 2015 Gout classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2015, 74, 1789–1798. [Google Scholar] [CrossRef]
- Bongartz, T.; Glazebrook, K.N.; Kavros, S.J.; Murthy, N.S.; Merry, S.P.; Franz, W.B., 3rd; Michet, C.J.; Veetil, B.M.; Davis, J.M., 3rd; Mason, T.G., 2nd; et al. Dual-energy CT for the diagnosis of gout: An accuracy and diagnostic yield study. Ann. Rheum. Dis. 2015, 74, 1072–1077. [Google Scholar] [CrossRef]
- A Singh, J.; Budzik, J.-F.; Becce, F.; Pascart, T. Dual-energy computed tomography vs ultrasound, alone or combined, for the diagnosis of gout: A prospective study of accuracy. Rheumatology 2021, 60, 4861–4867. [Google Scholar] [CrossRef]
- Bardin, T.; Tran, K.M.; Nguyen, Q.D.; Sarfati, M.; Richette, P.; Vo, N.T.; Bousson, V.; Correas, J.-M. Renal medulla in severe gout: Typical findings on ultrasonography and dual-energy CT study in two patients. Ann. Rheum. Dis. 2018, 78, 433–434. [Google Scholar] [CrossRef]
- Christiansen, S.N.; Østergaard, M.; Slot, O.; Keen, H.; Bruyn, G.A.W.; D’Agostino, M.A.; Terslev, L. Assessing the sensitivity to change of the OMERACT ultrasound structural gout lesions during urate-lowering therapy. RMD Open 2020, 6, e001144. [Google Scholar] [CrossRef] [PubMed]
- Hammer, H.B.; Karoliussen, L.; Terslev, L.; A Haavardsholm, E.; Kvien, T.K.; Uhlig, T. Ultrasound shows rapid reduction of crystal depositions during a treat-to-target approach in gout patients: 12-month results from the NOR-Gout study. Ann. Rheum. Dis. 2020, 79, 1500–1505. [Google Scholar] [CrossRef] [PubMed]
- Di Matteo, A.; Filippucci, E.; Cipolletta, E.; Ausili, M.; Martire, V.; Di Carlo, M.; Salaffi, F.; Grassi, W. The popliteal groove region: A new target for the detection of monosodium urate crystal deposits in patients with gout. An ultrasound study. Jt. Bone Spine 2018, 86, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Di Matteo, A.; Filippucci, E.; Cipolletta, E.; Musca, A.; Di Donato, E.; Martire, V.; Jesus, D.; Salaffi, F.; Grassi, W. Ultrasound and clinical features of hip involvement in patients with gout. Jt. Bone Spine 2019, 86, 633–636. [Google Scholar] [CrossRef] [PubMed]
- Ebstein, E.; Forien, M.; Norkuviene, E.; Richette, P.; Mouterde, G.; Daien, C.; Ea, H.-K.; Brière, C.; Lioté, F.; Petraitis, M.; et al. Ultrasound evaluation in follow-up of urate-lowering therapy in gout: The USEFUL study. Rheumatology 2018, 58, 410–417. [Google Scholar] [CrossRef]
- Ottaviani, S.; Gill, G.; Aubrun, A.; Palazzo, E.; Meyer, O.; Dieudé, P. Ultrasound in gout: A useful tool for following urate-lowering therapy. Jt. Bone Spine 2015, 82, 42–44. [Google Scholar] [CrossRef]
- Perez-Ruiz, F.; Martin, I.; Canteli, B. Ultrasonographic measurement of tophi as an outcome measure for chronic gout. J. Rheumatol. 2007, 34, 1888–1893. [Google Scholar]
- Naredo, E.; Uson, J.; Jimenez-Palop, M.; Martinez, A.; Vicente, E.; Brito, E.; Rodríguez, A.; Cornejo, F.J.; Castañeda, S.; Martínez, M.J.; et al. Ultrasound-detected musculoskeletal urate crystal deposition: Which joints and what findings should be assessed for diagnosing gout? Ann. Rheum. Dis. 2014, 73, 1522–1528. [Google Scholar] [CrossRef]
- Cipolletta, E.; Filippucci, E.; Abhishek, A.; Di Battista, J.; Smerilli, G.; Di Carlo, M.; Silveri, F.; De Angelis, R.; Salaffi, F.; Grassi, W.; et al. In patients with acute mono/oligoarthritis, a targeted ultrasound scanning protocol shows great accuracy for the diagnosis of gout and CPPD. Rheumatology 2022, 62, 1493–1500. [Google Scholar] [CrossRef]
- Peiteado, D.; Villalba, A.; Martín-Mola, E.; Balsa, A.; De Miguel, E. Ultrasound sensitivity to changes in gout: A longitudinal study after two years of treatment. Clin. Exp. Rheumatol. 2017, 35, 746–751. [Google Scholar]
- Bayat, S.; Aati, O.; Rech, J.; Sapsford, M.; Cavallaro, A.; Lell, M.; Araujo, E.; Petsch, C.; Stamp, L.K.; Schett, G.; et al. Development of a Dual-Energy Computed Tomography Scoring System for Measurement of Urate Deposition in Gout. Arthritis Care Res. 2015, 68, 769–775. [Google Scholar] [CrossRef]
- Dalbeth, N.; Billington, K.; Doyle, A.; Frampton, C.; Tan, P.; Aati, O.; Allan, J.; Drake, J.; Horne, A.; Stamp, L.K. Effects of Allopurinol Dose Escalation on Bone Erosion and Urate Volume in Gout: A Dual-Energy Computed Tomography Imaging Study Within a Randomized, Controlled Trial. Arthritis Rheumatol. 2019, 71, 1739–1746. [Google Scholar] [CrossRef] [PubMed]
- Pascart, T.; Grandjean, A.; Norberciak, L.; Ducoulombier, V.; Motte, M.; Luraschi, H.; Vandecandelaere, M.; Godart, C.; Houvenagel, E.; Namane, N.; et al. Ultrasonography and dual-energy computed tomography provide different quantification of urate burden in gout: Results from a cross-sectional study. Arthritis Res. Ther. 2017, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Thiele, R.G.; Schlesinger, N. Ultrasonography shows disappearance of monosodium urate crystal deposition on hyaline cartilage after sustained normouricemia is achieved. Rheumatol. Int. 2009, 30, 495–503. [Google Scholar] [CrossRef]
- Uhlig, T.; Eskild, T.; Karoliussen, L.F.; Sexton, J.; Kvien, T.K.; A Haavardsholm, E.; Dalbeth, N.; Hammer, H.B. Two-year reduction of dual-energy CT urate depositions during a treat-to-target strategy in gout in the NOR-Gout longitudinal study. Rheumatology 2021, 61, SI81–SI85. [Google Scholar] [CrossRef] [PubMed]
- Rajan, A.; Aati, O.; Kalluru, R.; Gamble, G.D.; Horne, A.; Doyle, A.J.; McQueen, F.M.; Dalbeth, N. Lack of change in urate deposition by dual-energy computed tomography among clinically stable patients with long-standing tophaceous gout: A prospective longitudinal study. Arthritis Res. Ther. 2013, 15, R160. [Google Scholar] [CrossRef] [PubMed]
- Araujo, E.G.; Bayat, S.; Petsch, C.; Englbrecht, M.; Faustini, F.; Kleyer, A.; Hueber, A.J.; Cavallaro, A.; Lell, M.; Dalbeth, N.; et al. Tophus resolution with pegloticase: A prospective dual-energy CT study. RMD Open 2015, 1, e000075. [Google Scholar] [CrossRef]
- Ellmann, H.; Bayat, S.; Araujo, E.; Manger, B.; Kleyer, A.; Cavallaro, A.; Lell, M.; Schenker, H.; Simon, D.; Tascilar, K.; et al. Effects of Conventional Uric Acid-Lowering Therapy on Monosodium Urate Crystal Deposits. Arthritis Rheumatol. 2020, 72, 150–156. [Google Scholar] [CrossRef]
- Sun, Y.; Chen, H.; Zhang, Z.; Ma, L.; Zhou, J.; Zhou, Y.; Ding, Y.; Jin, X.; Jiang, L. Dual-energy computed tomography for monitoring the effect of urate-lowering therapy in gouty arthritis. Int. J. Rheum. Dis. 2015, 18, 880–885. [Google Scholar] [CrossRef]
- Laurent, V.; Jauffret, C.; Pacaud, A.; Ducoulombier, V.; Legrand, J.; Verdun, S.; Norberciak, L.; Budzik, J.-F.; Pascart, T. Factors influencing the kinetics of MSU crystal depletion measured with dual-energy CT in patients with gout. RMD Open 2023, 9, e003725. [Google Scholar] [CrossRef]
- Dalbeth, N.; Becce, F.; Botson, J.K.; Zhao, L.; Kumar, A. Dual-energy CT assessment of rapid monosodium urate depletion and bone erosion remodelling during pegloticase plus methotrexate co-therapy. Rheumatology 2022, 61, 4898–4904. [Google Scholar] [CrossRef]
- Cipolletta, E.; Abhishek, A.; Di Battista, J.; Grassi, W.; Filippucci, E. Ultrasonography in the prediction of gout flares: A 12-month prospective observational study. Rheumatology 2022, 62, 1108–1116. [Google Scholar] [CrossRef] [PubMed]
- Ebstein, E.; Forien, M.; Norkuviene, E.; Richette, P.; Mouterde, G.; Daien, C.; Ea, H.-K.; Brière, C.; Lioté, F.; Petraitis, M.; et al. UltraSound evaluation in follow-up of urate-lowering therapy in gout phase 2 (USEFUL-2): Duration of flare prophylaxis. Jt. Bone Spine 2020, 87, 647–651. [Google Scholar] [CrossRef] [PubMed]
- Cipolletta, E.; Di Battista, J.; Di Carlo, M.; Di Matteo, A.; Salaffi, F.; Grassi, W.; Filippucci, E. Sonographic estimation of monosodium urate burden predicts the fulfillment of the 2016 remission criteria for gout: A 12-month study. Arthritis Res. Ther. 2021, 23, 185. [Google Scholar] [CrossRef] [PubMed]
- Pascart, T.; Grandjean, A.; Capon, B.; Legrand, J.; Namane, N.; Ducoulombier, V.; Motte, M.; Vandecandelaere, M.; Luraschi, H.; Godart, C.; et al. Monosodium urate burden assessed with dual-energy computed tomography predicts the risk of flares in gout: A 12-month observational study: MSU burden and risk of gout flare. Arthritis Res. Ther. 2018, 20, 210. [Google Scholar] [CrossRef]
- Hammer, H.B.; Karoliussen, L.F.; Eskild, T.; Sexton, J.; Terslev, L.; Haavardsholm, E.A.; Uhlig, T. OP0296 CRYSTAL DEPOSITIONS ASSESSED BY ULTRASOUND AND DECT DECREASE DURING TREATMENT AND PREDICTS REDUCED NUMBERS OF FLARES; TWO-YEARS RESULTS FROM THE NOR-GOUT TREAT-TO-TARGET STUDY. In Proceedings of the EULAR 2023 European Congress of Rheumatology, Milan, Italy, 31 May–3 June 2023; pp. 192–193. [Google Scholar]
- Dale, J.; Stirling, A.; Zhang, R.; Purves, D.; Foley, J.; Sambrook, M.; Conaghan, P.G.; van der Heijde, D.; McConnachie, A.; McInnes, I.B.; et al. Targeting ultrasound remission in early rheumatoid arthritis: The results of the TaSER study, a randomised clinical trial. Ann. Rheum. Dis. 2016, 75, 1043–1050. [Google Scholar] [CrossRef]
- A Haavardsholm, E.; Aga, A.-B.; Olsen, I.C.; Lillegraven, S.; Hammer, H.B.; Uhlig, T.; Fremstad, H.; Madland, T.M.; Lexberg, S.; Haukeland, H.; et al. Ultrasound in management of rheumatoid arthritis: ARCTIC randomised controlled strategy trial. BMJ 2016, 354, i4205. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| References | No. of Patients | Follow-Up | Analyzed US Features of Gout | Scoring System | Location | Results | Correlation with Urate Serum Level |
|---|---|---|---|---|---|---|---|
| [37] | 22 | 12 months | Tophus | Tophus size | Knee, ankle | ↓ Tophus size | Yes |
| [18] | 5 | 7–18 months | DC sign | Binary | MCP2, Knee | Disappearance of DC sign (80% patients) | Yes |
| MTP1 | |||||||
| [36] | 16 | 6 months | DC sign | Binary | Knee, MTP1 | Disappearance of DC sign (75% patients) | Yes |
| Tophus | Index tophus size | Knee, MTP1 | ↓ Tophus size (75% patients) | Yes | |||
| [40] | 23 | 24 months | DC sign | Binary | Knee, MTP1 | ↓ Number of DC signs | Yes |
| Tophus | Binary | Knee, MTP1, patellar tendon | ↓ Number of tophus (except patellar tendon) | No | |||
| [35] | 79 | 6 months | DC sign | Binary | Knee, MTP1 | ↓ Number of DC signs | Yes |
| Tophus | Index tophus size | Knee, MTP1 | ↓ Tophus size | M3: No M6: Yes | |||
| [32] | 209 | 12 months | DC sign | Semi-quantitative (0–3) | Wrist, knee, MTP1, MCP2 | ↓ DC sum score (4.3–1.3) | Yes |
| Tophus | Wrist, knee, MTP1, MCP2 Achilles, triceps tendons | ↓ Tophus sum score (6.5–3.8) | No | ||||
| Aggregates | Wrist, knee, MTP1, MCP2 | ↓ Aggregates sum score (9.3–6.7) | No | ||||
| [31] | 50 | 6 months | DC sign | Binary | 28 joints and 26 tendons: MCP1-5, wrist, elbow, MTP1-5, tibiotalar, knee, tendons (triceps, quadriceps, patellar, Achilles, finger extensors, peroneus, tibial posterior) | ↓ DC sum score (3.2–1.3) | Yes |
| Tophus | Binary | ↓ Tophus sum score (2.7–1.8) | No | ||||
| Aggregates | Binary | ↓ Aggregates sum score (6.1–5.0) | No | ||||
| Erosion | Binary | No decrease in erosion score | No |
| References | No. of Patients | Follow-Up | ULT-Naïve at Baseline | Scoring System | Location of DECT Analysis | Results | Correlation with Urate Serum Variation |
|---|---|---|---|---|---|---|---|
| [46] | 73 | 12 months | No | Tophus volume | Feet | ↓ Volume of 0.01 cm3 | No |
| [47] | 10 | 13.3 weeks | Yes (switch to pegloticase) | Tophus volume | Feet (n = 10) Hands (n = 2) | ↓ Volume of 74% | Yes |
| [48] | 83 | 18 months | Yes | Tophus volume | Feet | ↓ Volume (0.33–0.2 cm3) | Yes |
| DECT urate score | ↓ Score (4.2–2.5) | Yes | |||||
| [49] | 44 | 6–24 months | Yes | Number of crystals < or >3 mm | Feet | ↓ Number of crystals | Yes |
| Maximal tophus volume | ↓ Maximal volume (3.5–2.7 cm3) | Yes | |||||
| [42] | 87 | 24 months | Yes | Index tophus volume | Feet | ↓ Volume | Yes |
| [45] | 187 | 24 months | Yes | DECT urate score | feet | ↓ Score (4.6–1.5) | Yes |
| Ultrasonography | DECT | |
|---|---|---|
| Advantages | Availability Cost Feasibility in clinical practice Possible whole-body assessment No irradiation Good sensibility to changes Associated with changes in serum urate level | Good sensibility to change Associated with changes in serum urate level Direct quantification of urate volume Able to analyze bone erosion Able to analyze spine |
| Limitations | Operator-dependent Some sites are not accessible (e.g., spine) False positive results: pseudo-DC sign Semi-quantitative measure of urate deposition | Availability Cost Feasibility in clinical practice Irradiation One analyzed site False positive results (e.g., nail artefact) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ottaviani, S. Imaging Follow-Up of MSU Crystal Depletion. Gout Urate Cryst. Depos. Dis. 2024, 2, 34-44. https://doi.org/10.3390/gucdd2010003
Ottaviani S. Imaging Follow-Up of MSU Crystal Depletion. Gout, Urate, and Crystal Deposition Disease. 2024; 2(1):34-44. https://doi.org/10.3390/gucdd2010003
Chicago/Turabian StyleOttaviani, Sébastien. 2024. "Imaging Follow-Up of MSU Crystal Depletion" Gout, Urate, and Crystal Deposition Disease 2, no. 1: 34-44. https://doi.org/10.3390/gucdd2010003
APA StyleOttaviani, S. (2024). Imaging Follow-Up of MSU Crystal Depletion. Gout, Urate, and Crystal Deposition Disease, 2(1), 34-44. https://doi.org/10.3390/gucdd2010003