
Year in Review: Gout Clinical Research

Abstract
:1. Introduction
2. Conference Sections
2.1. Evaluation of Supported Self-Management in Gout (GoutSMART): A Randomized Controlled Feasibility Trial [1]
2.2. Association between Serum Urate and Flares in People with Gout and Evidence for Surrogate Status: A Secondary Analysis of Two Randomized Controlled Trials [6]
2.3. Association between Gout Flare and Subsequent Cardiovascular Events among Patients with Gout [13]
2.4. Allopurinol Initiation and All-Cause Mortality among Patients with Gout and Concurrent Chronic Kidney Disease [20]
2.5. Association of Sodium-Glucose Transport Protein 2 Inhibitor Use for Type 2 Diabetes and Incidence of Gout in Taiwan [25]
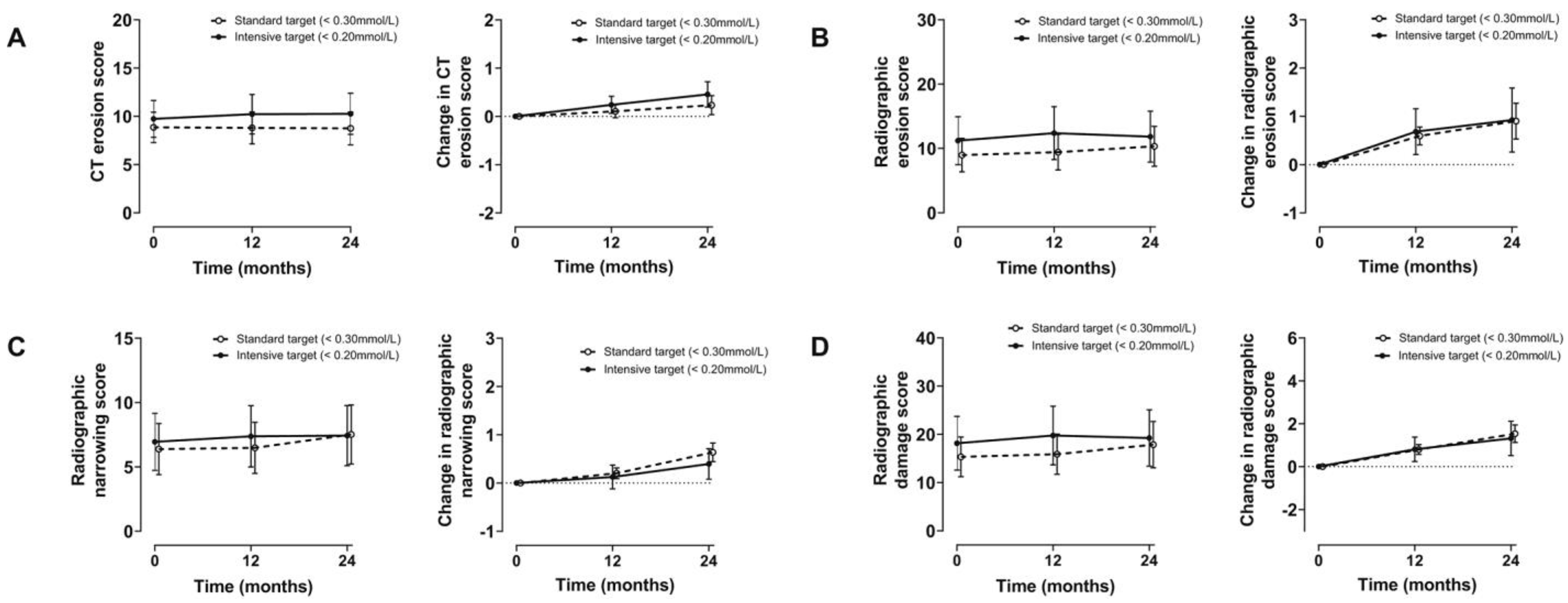
2.6. Intensive Serum Urate Lowering with Oral Urate-Lowering Therapy for Erosive Gout: A Randomized Double-Blind Controlled Trial [27]
2.7. Comparison of Rates of Lower Extremity Amputation in Patients with and without Gout in the US Department of Veterans Affairs Health System [38]
2.8. Gout and the Risk of COVID-19 Diagnosis and Death in the UK Biobank: A Population-Based Study [44]
3. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Riches, P.L.; Alexander, D.; Hauser, B.; Kuske, B.; Krause, A. Evaluation of supported self-management in gout (GoutSMART): A randomised controlled feasibility trial. Lancet Rheumatol. 2022, 4, e320–e328. [Google Scholar] [CrossRef]
- Kuo, C.-F.; Grainge, M.J.; Mallen, C.; Zhang, W.; Doherty, M. Rising burden of gout in the UK but continuing suboptimal management: A nationwide population study. Ann. Rheum. Dis. 2014, 74, 661–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doherty, M.; Jenkins, W.; Richardson, H.; Sarmanova, A.; Abhishek, A.; Ashton, D.; Barclay, C.; Doherty, S.; Duley, L.; Hatton, R.; et al. Efficacy and cost-effectiveness of nurse-led care involving education and engagement of patients and a treat-to-target urate-lowering strategy versus usual care for gout: A randomised controlled trial. Lancet 2018, 392, 1403–1412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paraskos, J.; Berke, Z.; Cook, J.; Miner, J.N.; Braddock, M.; Platt, A.; Hughes, G. An analytical comparison between point-of-care uric acid testing meters. Expert Rev. Mol. Diagn. 2016, 16, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Hammersley, V.; Parker, R.; Paterson, M.; Hanley, J.; Pinnock, H.; Padfield, P.; Stoddart, A.; Park, H.G.; Sheikh, A.; McKinstry, B. Telemonitoring at scale for hypertension in primary care: An implementation study. PLoS Med. 2020, 17, e1003124. [Google Scholar] [CrossRef]
- Stamp, L.K.; Frampton, C.; Morillon, M.B.; Taylor, W.J.; Dalbeth, N.; Singh, J.; Doherty, M.; Zhang, W.; Richardson, H.; Sarmanova, A.; et al. Association between serum urate and flares in people with gout and evidence for surrogate status: A secondary analysis of two randomised controlled trials. Lancet Rheumatol. 2021, 4, e53–e60. [Google Scholar] [CrossRef]
- FitzGerald, J.D.; Dalbeth, N.; Mikuls, T.; Brignardello-Petersen, R.; Guyatt, G.; Abeles, A.M.; Neogi, T. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Care Res. 2020, 72, 744–760. [Google Scholar] [CrossRef]
- Richette, P.; Doherty, M.; Pascual, E.; Barskova, V.; Becce, F.; Castañeda-Sanabria, J.; Bardin, T. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann. Rheum. Dis. 2017, 76, 29–42. [Google Scholar] [CrossRef] [Green Version]
- Schumacher, H.R.; Taylor, W.; Edwards, L.; Grainger, R.; Schlesinger, N.; Dalbeth, N.; Sivera, F.; Singh, J.; Evans, R.; Waltrip, R.W.; et al. Outcome Domains for Studies of Acute and Chronic Gout. J. Rheumatol. 2009, 36, 2342–2345. [Google Scholar] [CrossRef]
- Qaseem, A.; Harris, R.P.; Forciea, M.A.; Denberg, T.D.; Barry, M.J.; Boyd, C.; Clinical Guidelines Committee of the American College of Physicians. Management of Acute and Recurrent Gout: A Clinical Practice Guideline from the American College of Physicians. Ann. Intern. Med. 2017, 166, 58–68. [Google Scholar] [CrossRef] [Green Version]
- Stamp, L.K.; Chapman, P.T.; Barclay, M.; Horne, A.; Frampton, C.; Tan, P.; Drake, J.; Dalbeth, N. Allopurinol dose escalation to achieve serum urate below 6 mg/dL: An open-label extension study. Ann. Rheum. Dis. 2017, 76, 2065–2070. [Google Scholar] [CrossRef]
- Stamp, L.K.; Chapman, P.T.; Barclay, M.L.; Horne, A.; Frampton, C.; Tan, P.; Drake, J.; Dalbeth, N. A randomised controlled trial of the efficacy and safety of allopurinol dose escalation to achieve target serum urate in people with gout. Ann. Rheum. Dis. 2017, 76, 1522–1528. [Google Scholar] [CrossRef]
- Cipolletta, E.; Tata, L.J.; Nakafero, G.; Avery, A.J.; Mamas, M.A.; Abhishek, A. Association Between Gout Flare and Subsequent Cardiovascular Events among Patients with Gout. JAMA 2022, 328, 440–450. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Willerson, J.T.; Ridker, P.M. Inflammation as a cardiovascular risk factor. Circulation 2004, 109 (Suppl. 1), Ii2–Ii10. [Google Scholar] [CrossRef] [Green Version]
- De Vera, M.A.; Rahman, M.M.; Bhole, V.; Kopec, J.A.; Choi, H.K. Independent impact of gout on the risk of acute myocardial infarction among elderly women: A population-based study. Ann. Rheum. Dis. 2010, 69, 1162–1164. [Google Scholar] [CrossRef]
- Choi, H.K.; Curhan, G. Independent Impact of Gout on Mortality and Risk for Coronary Heart Disease. Circulation 2007, 116, 894–900. [Google Scholar] [CrossRef] [Green Version]
- Kuo, C.-F.; Yu, K.-H.; See, L.-C.; Chou, I.-J.; Ko, Y.-S.; Chang, H.-C.; Chiou, M.-J.; Luo, S.-F. Risk of myocardial infarction among patients with gout: A nationwide population-based study. Rheumatology 2012, 52, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, E.; Baker, J.F.; Furst, D.E.; Schumacher, H.R. Gout and the risk of acute myocardial infarction. Arthritis Rheumatol. 2006, 54, 2688–2696. [Google Scholar] [CrossRef]
- Wei, J.; Choi, H.K.; Neogi, T.; Dalbeth, N.; Terkeltaub, R.; Stamp, L.K.; Zhang, Y. Allopurinol Initiation and All-Cause Mortality among Patients with Gout and Concurrent Chronic Kidney Disease: A Population-Based Cohort Study. Ann. Intern. Med. 2022, 175, 461–470. [Google Scholar] [CrossRef]
- Zhu, Y.; Pandya, B.J.; Choi, H.K. Comorbidities of gout and hyperuricemia in the US general population: NHANES 2007–2008. Am. J. Med. 2012, 125, 679–687.e1. [Google Scholar] [CrossRef] [PubMed]
- Bevis, M.; Blagojevic-Bucknall, M.; Mallen, C.; Hider, S.; Roddy, E. Comorbidity clusters in people with gout: An observational cohort study with linked medical record review. Rheumatology 2018, 57, 1358–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badve, S.V.; Pascoe, E.M.; Tiku, A.; Boudville, N.; Brown, F.G.; Cass, A.; Clarke, P.; Dalbeth, N.; Day, R.O.; de Zoysa, J.R.; et al. Effects of Allopurinol on the Progression of Chronic Kidney Disease. N. Engl. J. Med. 2020, 382, 2504–2513. [Google Scholar] [CrossRef] [PubMed]
- Doria, A.; Galecki, A.T.; Spino, C.; Pop-Busui, R.; Cherney, D.Z.; Lingvay, I.; Parsa, A.; Rossing, P.; Sigal, R.J.; Afkarian, M.; et al. Serum Urate Lowering with Allopurinol and Kidney Function in Type 1 Diabetes. N. Engl. J. Med. 2020, 382, 2493–2503. [Google Scholar] [CrossRef]
- Chung, M.-C.; Hung, P.-H.; Hsiao, P.-J.; Wu, L.-Y.; Chang, C.-H.; Wu, M.-J.; Shieh, J.-J.; Chung, C.-J. Association of Sodium-Glucose Transport Protein 2 Inhibitor Use for Type 2 Diabetes and Incidence of Gout in Taiwan. JAMA Netw. Open 2021, 4, e2135353. [Google Scholar] [CrossRef]
- Van Bommel, E.J.M.; Muskiet, M.H.A.; Tonneijck, L.; Kramer, M.H.H.; Nieuwdorp, M.; van Raalte, D.H. SGLT2 Inhibition in the Diabetic Kidney—From Mechanisms to Clinical Outcome. Clin. J. Am. Soc. Nephrol. 2017, 12, 700–710. [Google Scholar] [CrossRef] [Green Version]
- Dalbeth, N.; Doyle, A.J.; Billington, K.; Gamble, G.D.; Tan, P.; Latto, K.; Ram, T.P.; Narang, R.; Murdoch, R.; Bursill, D.; et al. Intensive Serum Urate Lowering with Oral Urate-Lowering Therapy for Erosive Gout: A Randomized Double-Blind Controlled Trial. Arthritis Rheumatol. 2022, 74, 1059–1069. [Google Scholar] [CrossRef]
- Dalbeth, N.; Clark, B.; McQueen, F.; Doyle, A.; Taylor, W. Validation of a radiographic damage index in chronic gout. Arthritis Rheumatol. 2007, 57, 1067–1073. [Google Scholar] [CrossRef]
- Stewart, S.; Aati, O.; Horne, A.; Doyle, A.J.; Dalbeth, N. Radiographic damage scores predict grip strength in patients with tophaceous gout. Rheumatology 2019, 59, 1440–1442. [Google Scholar] [CrossRef]
- Stewart, S.; Rome, K.; Eason, A.; House, M.E.; Horne, A.; Doyle, A.J.; Knight, J.; Taylor, W.J.; Dalbeth, N. Predictors of activity limitation in people with gout: A prospective study. Clin. Rheumatol. 2018, 37, 2213–2219. [Google Scholar] [CrossRef]
- Dalbeth, N.; Aati, O.; Kalluru, R.; Gamble, G.D.; Horne, A.; Doyle, A.J.; McQueen, F.M. Relationship between structural joint damage and urate deposition in gout: A plain radiography and dual-energy CT study. Ann. Rheum. Dis. 2014, 74, 1030–1036. [Google Scholar] [CrossRef]
- Towiwat, P.; Doyle, A.J.; Gamble, G.D.; Tan, P.; Aati, O.; Horne, A.; Dalbeth, N. Urate crystal deposition and bone erosion in gout: ‘Inside-out’ or ‘outside-in’? A dual-energy computed tomography study. Arthritis Res. Ther. 2016, 18, 208. [Google Scholar] [CrossRef] [Green Version]
- Chhana, A.; Callon, K.E.; Pool, B.; Naot, D.; Watson, M.; Gamble, G.D.; McQueen, F.M.; Cornish, J.; Dalbeth, N. Monosodium urate monohydrate crystals inhibit osteoblast viability and function: Implications for development of bone erosion in gout. Ann. Rheum. Dis. 2011, 70, 1684–1691. [Google Scholar] [CrossRef]
- Chhana, A.; Pool, B.; Callon, K.E.; Tay, M.L.; Musson, D.; Naot, D.; McCarthy, G.; McGlashan, S.; Cornish, J.; Dalbeth, N. Monosodium urate crystals reduce osteocyte viability and indirectly promote a shift in osteocyte function towards a proinflammatory and proresorptive state. Thromb. Haemost. 2018, 20, 208. [Google Scholar] [CrossRef] [Green Version]
- Dalbeth, N.; Billington, K.; Doyle, A.; Frampton, C.; Tan, P.; Aati, O.; Allan, J.; Drake, J.; Horne, A.; Stamp, L.K. Effects of Allopurinol Dose Escalation on Bone Erosion and Urate Volume in Gout: A Dual-Energy Computed Tomography Imaging Study within a Randomized, Controlled Trial. Arthritis Rheumatol. 2019, 71, 1739–1746. [Google Scholar] [CrossRef]
- Sundy, J.S.; Baraf, H.S.; Yood, R.A.; Edwards, N.L.; Gutierrez-Urena, S.R.; Treadwell, E.L.; Becker, M.A. Efficacy and tolerability of pegloticase for the treatment of chronic gout in patients refractory to conventional treatment: Two randomized controlled trials. Jama 2011, 306, 711–720. [Google Scholar]
- Dalbeth, N.; Doyle, A.J.; McQueen, F.M.; Sundy, J.; Baraf, H.S.B. Exploratory study of radiographic change in patients with tophaceous gout treated with intensive urate-lowering therapy. Arthritis Care Res. 2013, 66, 82–85. [Google Scholar] [CrossRef]
- Mikuls, T.R.; Soto, Q.; Petro, A.; Helget, L.; Roul, P.; Sayles, H.; Cope, B.; Neogi, T.; LaMoreaux, B.; O’Dell, J.R.; et al. Comparison of Rates of Lower Extremity Amputation in Patients with and without Gout in the US Department of Veterans Affairs Health System. JAMA Netw. Open 2022, 5, e2142347. [Google Scholar] [CrossRef]
- Mikuls, T.R.; Farrar, J.T.; Bilker, W.B.; Fernandes, S.; Schumacher, H.R., Jr.; Saag, K.G. Gout epidemiology: Results from the UK General Practice Research Database, 1990–1999. Ann. Rheum. Dis. 2005, 64, 267–272. [Google Scholar] [CrossRef]
- Cai, M.; Xie, Y.; Bowe, B.; Gibson, A.K.; Zayed, M.A.; Li, T.; Al-Aly, Z. Temporal Trends in Incidence Rates of Lower Extremity Amputation and Associated Risk Factors among Patients Using Veterans Health Administration Services from 2008 to 2018. JAMA Netw. Open 2021, 4, e2033953. [Google Scholar] [CrossRef]
- Sariyilmaz, K.; Eren, I.; Ozkunt, O.; Sungur, M.; Kilicoglu, O.I.; Dikici, F. Bilateral First-Ray Amputation of the Foot Due to Severe Tophaceous Gout Complicated by Infection and Discharged Sinus (A Case Report). J. Am. Podiatr. Med. Assoc. 2018, 108, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.H.; Luo, S.F.; Liou, L.B.; Wu, Y.J.; Tsai, W.P.; Chen, J.Y.; Ho, H.H. Concomitant septic and gouty arthritis—An analysis of 30 cases. Rheumatology 2003, 42, 1062–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, C.; Xue, C.; Yang, B.; Wang, W.; Xu, Y.; Huang, F.; Wang, Y. Amputation of the first metatarsophalangeal joint due to a giant gouty tophi: A case report. Medicine 2017, 96, e8441. [Google Scholar] [CrossRef] [PubMed]
- Topless, R.K.; Gaffo, A.; Stamp, L.K.; Robinson, P.C.; Dalbeth, N.; Merriman, T.R. Gout and the risk of COVID-19 diagnosis and death in the UK Biobank: A population-based study. Lancet Rheumatol. 2022, 4, e274–e281. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Serum Urate Responder | Serum Urate Non-Responder | OR (95% CI) or Mean Difference between Groups (95% CI) | p Value | |
|---|---|---|---|---|
| Unadjusted | ||||
| Nottingham | n = 290 | n = 227 | ||
| Participants with gout flare | 75 (26%) | 148 (65%) | 0.19 (0.13 to 0.27) | <0.0001 |
| Number of gout flares | 0.63 (0.05) | 2.41 (0.10) | −1.78 (−2.0 to −1.55) | <0.0001 |
| New Zealand | n = 53 | n = 18 | ||
| Participants with gout flare | 16 (30%) | 8 (44%) | 0.54 (0.18 to 1.62) | 0.27 |
| Number of gout flares | 0.81 (0.12) | 1.0 (0.24) | −0.19 (−0.71 to 0.33) | 0.48 |
| Combined | n = 343 | n = 245 | ||
| Participants with gout flare | 91 (27%) | 156 (64%) | 0.20 (0.15 to 0.29) | <0.0001 |
| Number of gout flares | 0.66 (0.04) | 2.31 (0.10) | −1.64 (−1.85 to −1.44) | <0.0001 |
| Adjusted * | ||||
| Nottingham | n = 290 | n = 227 | ||
| Participants with gout flare | 75 (26%) | 148 (65%) | 0.18 (0.10 to 0.32) | <0.0001 |
| Number of gout flares | 0.55 (0.05) | 2.17 (0.16) | −1.62 (−1.97 to −1.28) | <0.0001 |
| New Zealand | n = 53 | n = 18 | ||
| Participants with gout flare | 16 (30%) | 8 (44%) | 0.53 (0.17 to 1.61) | 0.26 |
| Number of gout flares | 0.86 (0.13) | 1.06 (0.25) | −0.20 (−0.76 to 0.35) | 0.47 |
| Combined | n = 343 | n = 245 | ||
| Participants with gout flare | 91 (27%) | 156 (64%) | 0.22 (0.13 to 0.37) | <0.0001 |
| Number of gout flares | 0.61 (0.05) | 1.94 (0.14) | −1.33 (−1.64 to −1.03) | <0.0001 |
| Adjusted ** | ||||
| Nottingham | n = 290 | n = 227 | ||
| Participants with gout flare | 76 (26%) | 148 (65%) | 0.24 (0.12 to 0.47) | <0.0001 |
| Number of gout flares | 0.65 (0.06) | 2.52 (0.22) | −1.88 (−2.34 to −1.41) | <0.0001 |
| New Zealand | n = 53 | n = 18 | ||
| Participants with gout flare | 16 (30%) | 8 (44%) | 0.53 (0.17 to 1.62) | 0.26 |
| Number of gout flares | 0.81 (0.13) | 0.99 (0.24) | −0.18 (−0.70 to 0.34) | 0.50 |
| Combined | n = 343 | n = 245 | ||
| Participants with gout flare | 91 (27%) | 156 (64%) | 0.29 (0.17 to 0.51) | <0.0001 |
| Number of gout flares | 0.69 (0.06) | 2.09 (0.17) | −1.41 (−1.77 to −1.04) | <0.0001 |
| Diagnosis of COVID-19 | COVID-19-Related Death in COVID-19 Cohort | COVID-19-Related Death in Entire Cohort | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Unadjusted | ||||||
| Combined | 1.49 (1.39–1.60) | <0.0001 | 2.97 (2.45–3.62) | <0.0001 | 3.93 (3.28–4.70) | <0.0001 |
| Men | 1.34 (1.24–1.45) | <0.0001 | 1.99 (1.58–2.50) | <0.0001 | 2.43 (1.97–3.00) | <0.0001 |
| Women | 1.96 (1.67–2.30) | <0.0001 | 5.74 (3.86–8.53) | <0.0001 | 9.37 (6.58–13.35) | <0.0001 |
| Model 1 * | ||||||
| Combined | 1.41 (1.31–1.51) | <0.0001 | 1.44 (1.16–1.78) | 0.00091 | 1.76 (1.46–2.12) | <0.0001 |
| Men | 1.27 (1.17–1.38) | <0.0001 | 1.25 (0.98–1.60) | 0.073 | 1.47 (1.19–1.83) | 0.00044 |
| Women | 1.91 (1.62–2.24) | <0.0001 | 2.34 (1.51–3.62) | 0.00013 | 3.49 (2.41–5.04) | <0.0001 |
| Model 2 ** | ||||||
| Combined | 1.20 (1.11–1.29) | <0.0001 | 1.20 (0.96–1.51) | 0.11 | 1.29 (1.06–1.56) | 0.013 |
| Men | 1.12 (1.03–1.22) | 0.0066 | 1.11 (0.85–1.44) | 0.44 | 1.16 (0.93–1.45) | 0.20 |
| Women | 1.44 (1.22–1.70) | <0.0001 | 1.65 (1.04–2.64) | 0.035 | 1.98 (1.34–2.94) | 0.00062 |
| Study | Main Finding | Strengths | Limitations |
|---|---|---|---|
| Evaluation of supported self-management in gout (GoutSMART): a randomized controlled feasibility trial | More patients in a supported self-management group achieved a serum urate goal of less than 5 mg/dL at 24 weeks compared to patients in a usual care group. | Innovative approach to gout management. | Feasibility study with a small sample size. |
| Association between serum urate and flares in people with gout and evidence for surrogate status: a secondary analysis of two randomized controlled trials | Fewer serum urate responders had a gout flare compared to non-responders between 12 and 24 months. | Validates serum urate as a surrogate for a patient-centered outcome: acute flares. | Unable to account for the use of ULT other than allopurinol, subset by sex, or analyze the influence of foods and alcohol as triggers for flares. |
| Association between gout flare and subsequent cardiovascular events among patients with gout | Patients with cardiovascular events had significantly higher odds of having had a gout flare in the previous 0 to 60 days compared to patients without cardiovascular events. | Findings were robust to sensitivity analyses. Derived from a large database representative of the general population. Care in the ascertainment of predictors and outcomes. | Data is only available for events captured in electronic health records. Unable to consider the severity of flares. |
| Allopurinol initiation and all-cause mortality among patients with gout and concurrent chronic kidney disease | Mortality was lower in people that initiated allopurinol when compared to those who did not. | Large study. Robust results, with the same direction of effect for the evaluated associations. | Observational study using an existing database, hence with risk for residual confounding. |
| Association of Sodium-Glucose Transport Protein 2 Inhibitor Use for Type 2 Diabetes and Incidence of Gout in Taiwan | Individuals with type 2 diabetes receiving SLGT2 inhibitors had a lower risk of gout compared to those receiving DPP4 inhibitors. | Large size. Novel gout treatment target. | Short follow-up period. Lack of serum urate results. |
| Intensive serum urate lowering with oral urate-lowering therapy for erosive gout: a randomized, double-blind controlled trial | A radiographic bone erosion score worsened in individuals with an intensive serum urate control goal of less than 3.3 mg/dL and those with a goal of less than 5 mg/dL. There was no difference between the two. | First randomized controlled study to compare serum urate target goals. | Unable to obtain and maintain the serum urate goals. |
| Comparison of rates of lower extremity amputation in patients with and without gout in the US Department of Veterans Affairs health system | Individuals with gout had a higher rate of lower extremity amputations than people without gout. | Use of a patient-centered outcome. Large sample size. | Observational study. |
| Gout and the risk of COVID-19 diagnosis and death in the UK Biobank: a population-based study | Gout is a risk factor for COVID-19 diagnosis and COVID-19-related death in women, independent of metabolic comorbidities. | First study to evaluate the association of gout with COVID-19 by sex stratification. Large sample size. | Unable to account for the severity of gout, medication adherence, and the role of vaccination. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urquiaga, M.; Gaffo, A.L. Year in Review: Gout Clinical Research. Gout Urate Cryst. Depos. Dis. 2023, 1, 37-48. https://doi.org/10.3390/gucdd1010005
Urquiaga M, Gaffo AL. Year in Review: Gout Clinical Research. Gout, Urate, and Crystal Deposition Disease. 2023; 1(1):37-48. https://doi.org/10.3390/gucdd1010005
Chicago/Turabian StyleUrquiaga, Mariana, and Angelo L. Gaffo. 2023. "Year in Review: Gout Clinical Research" Gout, Urate, and Crystal Deposition Disease 1, no. 1: 37-48. https://doi.org/10.3390/gucdd1010005
APA StyleUrquiaga, M., & Gaffo, A. L. (2023). Year in Review: Gout Clinical Research. Gout, Urate, and Crystal Deposition Disease, 1(1), 37-48. https://doi.org/10.3390/gucdd1010005