Abstract
Technological advancements driving smart healthcare transformation need new models and solutions for emerging technology challenges. The objective of this review paper is to introduce the concept of smart healthcare, identify its main characteristics, highlight the key drivers of its adoption (“Technological Advancements, Digital Citizen Societies, Shifting Models of Patient Care, Healthcare Workforce Shortages, Rising Costs of Healthcare Delivery, and Impacts of COVID-19”), and present the primary challenges associated with its implementation (“Reduced Human Interaction and Patient Monitoring, Data Accuracy and Reliability, Data Security and Privacy, Interoperability and System Performance, Ethical Concerns and Trust in AI, High Financial Costs”). The paper is written in simplified language to enable a wide range of healthcare stakeholders—particularly healthcare professionals with limited technical backgrounds—to develop a foundational understanding of smart healthcare. This knowledge can foster greater engagement in efforts to transform healthcare systems into smarter, more efficient models. Furthermore, the findings of this review may support future research efforts, especially those aimed at developing models or frameworks that facilitate the practical integration of smart healthcare beyond theoretical concepts, by offering a synthesized framework for SHC.
1. Introduction
In recent decades, modern society has experienced tremendous progress in areas such as community development, medicine, and technology. These swift innovations have played a significant role in enhancing the quality of life across the globe. As digital technologies continue to evolve, their integration into infrastructure, services, and industries has accelerated, with healthcare being one of the most pivotal sectors embracing this transformation [1]. Healthcare, which addresses the physical, mental, and social well-being of individuals, has always been fundamental to public welfare. With increasing expectations for healthcare to be effective, accessible, and efficient, it is essential that healthcare systems evolve in step with technological advances [2].
The traditional, reactive, hospital-centered model is shifting toward a more proactive, personalized, and preventive approach. Within this shift, the concept of smart healthcare (SHC) has emerged as a powerful and innovative solution [3]. For a better understanding of SHC, especially among non-technical healthcare professionals (HCPs), Table 1 illustrates some simplified explanations for the main SHC terminologies pertinent to this paper.

Table 1.
Key concepts in smart healthcare.
SHC employs cutting-edge digital technologies—such as AI, the IoT, big data analytics, and cloud computing—to improve the delivery, accessibility, and quality of healthcare services [24]. These tools help reduce costs, enhance efficiency, and produce better patient outcomes. Innovations like telemedicine and virtual care are especially helpful for individuals who face challenges traveling to healthcare facilities, such as those with disabilities [25]. Traditional systems are increasingly unable to meet these evolving, service-oriented demands [26].
The origins of SHC can be traced back to the late 1980s [27], when the focus was on reducing human error and operational expenses through automation and sensor-based systems [28]. Over time, the concept has expanded to emphasize enhanced patient experience, operational efficiency, and the use of digital technologies throughout the healthcare continuum. Today’s SHC systems leverage information and communication technologies (ICTs) to offer efficient, personalized, and connected care services [29].
While SHC impacts can be the most potent in tertiary settings, they are not confined to hospitals alone, and extend across the whole health delivery continuum, including general practices, clinics, private healthcare settings, and even residential and wearable devices. SHC benefits from technologies that enhance patient monitoring, streamline communication, and enable individualized treatment. Wearable devices, for example, can provide real-time data on heart rate and blood glucose, helping clinicians make timely, informed decisions. This emphasis on prevention rather than treatment reduces strain on healthcare facilities and improves patient outcomes.
Implementing SHC goes beyond adopting digital tools—it calls for rethinking models of care, operational workflows, infrastructure, and patient engagement strategies. This transition is redefining public expectations by promoting accessibility, personalization, and operational efficiency [29]. AI technologies have already shown great promise in diagnosing complex diseases like cancer with high accuracy [30]. Meanwhile, global digital connectivity enables real-time collaboration, data exchange, and continuous care across geographic boundaries [31].
The integration of eHealth, mHealth, IoT, and AI is building a healthcare ecosystem where constant monitoring, tailored treatments, and real-time data analysis are becoming standard. This digital transformation not only improves care delivery but also increases public confidence in healthcare systems, ultimately contributing to healthier societies worldwide [32]. This study contributes to addressing the “research gap” comprising the need for more research on the rapidly developing SHC landscape; it does not seek to offer a new conceptual model, but to offer an updated review of recent evidence. Table 2 provides a summary of definitions from recent literature to help frame the concept of SHC. Based on these definitions, the current study adopts the following operational definition:
Table 2.
Definitions of smart healthcare.
“Smart healthcare is the integration of advanced technologies like the IoT, AI, and mobile internet into healthcare systems to improve patient care, monitoring, and treatment. It involves using intelligent sensors, wearable devices, and data analysis platforms to collect and process information autonomously, enabling continuous monitoring and informed decision-making.”
2. Materials and Methods
The research methodology for this review is based on a narrative approach, which enables a comprehensive and flexible synthesis of literature. This method, complemented with content analysis [36], is well-suited to capturing the evolution of SHC, identifying its key drivers, defining characteristics, and associated challenges—while also maintaining accessibility for a broad audience, including HCPs with limited technical backgrounds [37]. As illustrated in Figure 1, the review process followed a structured, step-by-step approach.
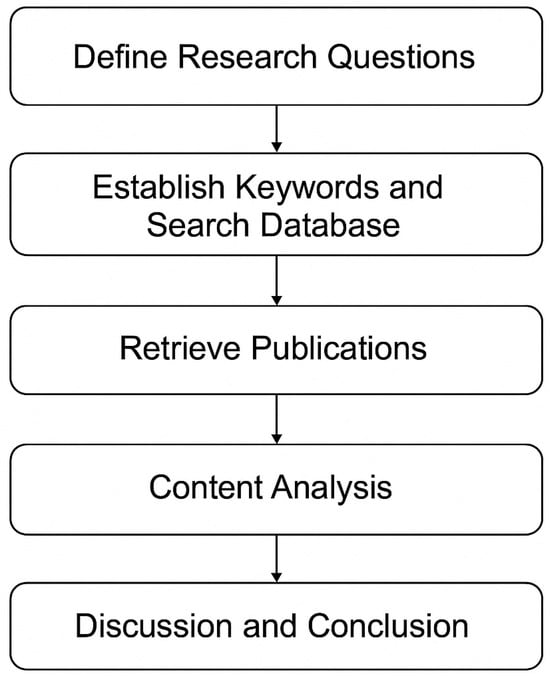
Figure 1.
Review protocol.
The research process began by formulating three guiding research questions:
- What is the concept of SHC?
- What are the main drivers and characteristics of SHC?
- What challenges are associated with its implementation?
Based on these questions, relevant keywords—such as “SHC” and “SHC challenges” were used to search the Google Scholar database. Publications were selected based on relevance, credibility, and recency, with a focus on works published between 2015 and 2025, to include the most up-to-date research. This resulted in 63 articles in total, comprising 49 journal articles (≈78%), 5 conference papers (≈8%), and 9 gray-literature items (≈14%), as shown in Figure 2. A qualitative content analysis approach was employed to extract and code relevant information from the selected literature [36]. Thematic synthesis facilitated the organization of data into the paper’s core sections: the concept, drivers, characteristics, and challenges of SHC. Finally, the findings were presented in a clear, structured format that aligns with these themes, and the paper concludes with a discussion of key insights and their implications for healthcare stakeholders and future research.
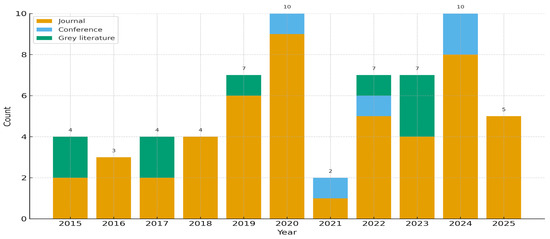
Figure 2.
Distribution of included studies.
3. Results
3.1. SHC Conceptualization
The concept of SHC has evolved from traditional healthcare models into a fully integrated, technology-driven system designed to enhance patient care and accessibility. Unlike conventional hospitals that rely heavily on in-person interactions and paper-based systems, SHC extends its reach beyond the physical boundaries of hospitals and clinics—into homes, workplaces, and community spaces—ensuring that patients and HCPs can stay connected, regardless of location or time (and time zone) [26]. Through the integration of sensors, interactive technologies, and advanced communication systems, smart hospitals enable continuous health monitoring, support daily living, and improve patient safety by facilitating rapid access to social, medical, and emergency services.
This innovation in healthcare delivery offers wide-ranging medical, social, and economic benefits. Patients can receive real-time assistance and care, while HCPs gain the ability to share data with specialists around the world, enhancing diagnosis and treatment quality. Moreover, researchers benefit from access to global datasets, allowing them to study disease patterns, evaluate treatments, and accelerate pharmaceutical development [29]. SHC technologies also contribute to improved patient outcomes and system efficiency through several key features. These include automated home monitoring services, which help reduce hospital and hospice occupancy, leading to lower overall healthcare costs. Additionally, they enable personalized healthcare services tailored to individual needs and support predictive analysis for the early detection of diseases [38].
Figure 3 illustrates an SHC ecosystem where people, places, and tools connect to improve care [4]. At the top, a patient with sensors uses wearable devices (for example, a smart watch) that collect health readings at home and send them securely to care teams—this is part of the Internet of Things and the Internet of Medical Things [6,10,23]. Care can be delivered remotely through telemedicine (video/phone consultations) and broader telehealth services, such as online monitoring and virtual clinics [9,14]. Many day-to-day services can be delivered through eHealth portals and mobile health apps, helping people to book, track, and follow care plans [11,12].
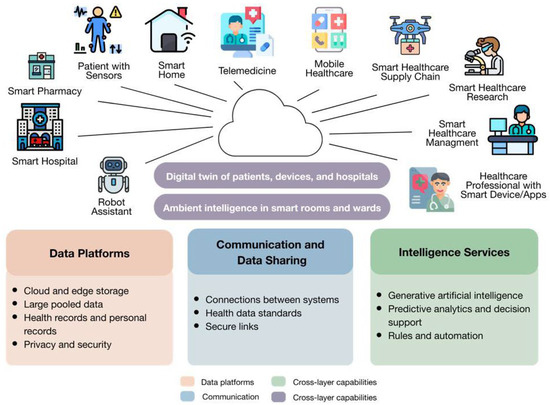
Figure 3.
An illustration of an SHC ecosystem.
For instance, a smart pharmacy can dispense medicines and coordinate refills, while smart hospitals and smart ambulances can share information so staff are prepared before the patient arrives. A drone represents the SHC supply chain, moving samples or medicines quickly when needed. Healthcare staff with smart devices and managers coordinate care, and SHC research teams analyze what works, using ethically governed data (i.e., with appropriate data protection and security) [19,20].
The central cloud stands for shared platforms powered by cloud computing, whereby data are available when and where they are needed [8]. These platforms pool information from many sources and support big data analytics to find patterns that can guide action [7]. The “intelligence” layer turns data into help at the point of care: artificial intelligence and clinical decision support systems can summarize notes, flag risks, and suggest next steps. In terms of imaging, smart radiomics helps read scans more precisely [5,13,15]. Continuous home follow-up appears as remote patient monitoring [17]. Because people’s skills and comfort with technology vary, the figure also acknowledges the role of digital citizens (i.e., people who are more familiar with digital tools), reminding us to support everyone fairly and according to their needs [18].
For this to work safely, systems must interoperate so they can “talk to” each other, using common rules, while cybersecurity protects personal data [19,20]. RFID tags can track equipment and patients to improve safety and flow [21]. Finally, ambient intelligence can be provided, whereby rooms and wards can be monitored to sense needs and respond to critical changes (as described below), helping teams to act sooner and more smoothly, reducing adverse care outcomes and optimizing resource deployment [22]. Together, these elements create a loop where information flows, insights are created, and better decisions return to patients and professionals.
One notable example of SHC presented by Sarkar et al. [38] is an AMI system, which integrates the IoMT with intelligent computing to create adaptive, context-aware healthcare environments. As shown in Figure 4, AMI can significantly enhance healthcare delivery in multiple ways. It enables remote monitoring of patients’ vital signs, medication routines, and overall health status, allowing HCPs to respond promptly to sudden changes or emergencies. Through telehealth functions, AMI facilitates virtual consultations and remote diagnostics, ensuring that patients in remote or underserved areas have access to medical care. In smart hospital settings, AMI contributes to efficient resource management by automating routine tasks and optimizing environmental conditions such as lighting and temperature, while also reducing infection risks through continuous monitoring of patient interactions.
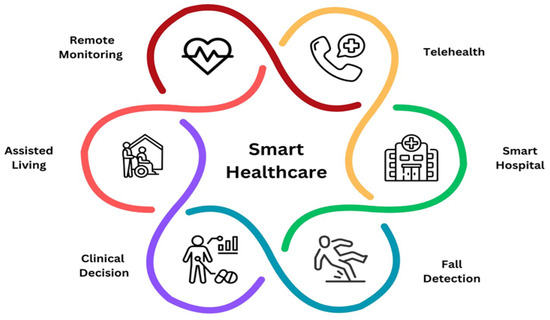
Figure 4.
SHC example: based on AMI in healthcare [38].
For fall detection, AMI uses real-time sensors to identify incidents and automatically notify caregivers or emergency responders, which is especially valuable for elderly individuals living independently. In clinical decision-making, AMI systems analyze data from wearables, electronic health records, and medical devices to support physicians with timely insights for diagnosis and treatment planning. Finally, in assisted living, AMI empowers elderly and disabled individuals to live independently by monitoring their activities, detecting emergencies, and providing support—while preserving their privacy and autonomy, thus promoting service user satisfaction.
However, implementing SHC systems requires high standards of data privacy and security, seamless data interoperability, and advanced network infrastructures [28]. When successfully deployed, these systems reduce medical errors, lower operational costs, and alleviate the burden on HCPs, creating a more efficient and responsive environment [28].
There are various examples of successes in deploying SHC systems worldwide. In Singapore, a high-income setting, national digital platforms and a shared patient record support joined-up, prevention-focused care [39]. In India, a low-/middle-income country, the eSanjeevani telemedicine program has expanded access at a national scale, especially in rural communities [40]. The brief comparison below shows different paths to success and complementary lessons.
Singapore has built a joined-up digital health system that puts prevention first and lets providers share a single view of the patient record via national platforms (e.g., Healthier SG and NEHR) [41,42,43]. Early evaluations report shorter hospital stays and fewer bed-days after Healthier SG roll-out in a large tertiary hospital [44]. However, while telehealth is growing, policy must keep seniors included and provide for digital “immigrants.” Surveys show that many older adults are still unsure about telehealth options and benefits [45]. Overall, Singapore’s strengths are integration, governance, and prevention, with the main challenges being onboarding every clinic and digital inclusion for less tech-confident groups [41,45].
India’s eSanjeevani is a national telemedicine service that delivers remote consultations at a massive scale, especially benefiting rural and remote communities [46]. Studies show good diagnostic agreement between teleconsultations and in-person care in rural Gujarat, supporting safe use when designed well [47]. Mixed-methods and clinician-use studies highlight strong access gains but also connectivity gaps, variable quality across regions, language/digital-skills barriers, and limited integration with shared records [48,49]. Recent qualitative work from Rajasthan describes eSanjeevani’s next phase (v2.0), adding point-of-care diagnostics, which is promising, but it will need training and outcome tracking to show impact beyond volume [49]. In short, India’s strengths are reach and equity at scale; the priorities now are last-mile enablement and deeper interoperability [46].
Table 3 provides a summary comparison of the cases of Singapore and India as high- and lower-middle-income countries (respectively) that have successfully applied SMC projects.
Table 3.
Comparison between SMC projects in Singapore and India.
3.2. SHC Characteristics
3.2.1. Overview
One notable feature of SHC is its adoption of cutting-edge technologies such as AI, robotic surgery systems, and mixed reality. These innovations are revolutionizing how diseases are diagnosed and treated by making medical procedures more accurate and efficient. AI has significantly enhanced CDSS, with impressive results in identifying diseases like hepatitis, lung cancer, and skin cancer [29]. In diagnostic areas like pathology and imaging, AI often outperforms human practitioners by recognizing complex patterns in large volumes of data. A well-known example is IBM Watson, which processes extensive clinical datasets to deliver accurate diagnostic recommendations, particularly in managing chronic illnesses like cancer and diabetes [29]. AI is also improving precision in treatments, such as through smart radiomics in tumor radiotherapy and robotic-assisted surgeries [15].
Another defining characteristic of SHC is the use of mHealth services. These involve mobile technologies such as smartphones, tablets, and wearable devices to support health monitoring and care delivery. A central aspect of this is personal health records, which empower individuals to monitor their health independently by collecting data from various healthcare institutions and tracking indicators like weight, physical activity, and blood sugar levels. A study from Stanford University revealed that 81% of users wearing smartwatches or fitness trackers detected early signs of COVID-19 up to nine days before conventional symptoms appeared [39]. With growing demand for mobile access to health information, tools such as the NHS mobile app in the UK allow users to view electronic medical records, manage prescriptions, book appointments, and access treatment summaries [50].
Telehealth is a third key element of SHC. Enabled by information and communication technologies, telehealth allows for the remote delivery of medical services. Applications include tele-ICUs, virtual consultations, and collaborative care platforms. Tools such as chatbots and wearable sensors can facilitate synchronous or asynchronous communication without requiring in-person contact [51]. In the United States, telehealth platforms provide medical consultations to individuals in remote areas with limited access to in-person care. Patients can interact with diverse HCPs—such as health coaches—through mobile devices, receiving treatment plans, medical advice, and support. Telehealth also supports critical care communication between clinicians and patients in intensive care units using video and audio technologies [52]. At Johns Hopkins Hospital, for example, the implementation of a tele-ICU program led to shorter ICU stays and better clinical outcomes, cutting the cost per case by 24.6% [53].
A fourth feature of SHC is its focus on prevention and real-time observation. Traditional methods of risk assessment often rely on collecting patient data manually, which may delay information sharing between facilities. In contrast, SHC enables centralized, cloud-based data storage, making records accessible from any location and reducing the need for physical visits. Wearable technologies can continuously upload health metrics to cloud platforms or mobile applications, allowing clinicians to monitor patient conditions in real time [29].
The fifth characteristic involves enhancing pharmaceutical research. Drug development typically involves multiple manual steps—such as screening, discovery, and clinical trials—which can introduce errors and delays. SHC systems help overcome these limitations by digitally recording every step of the process, ensuring data integrity and improving transparency. These systems also assist with high-speed calculations and validation of research findings [29].
In essence, SHC represents a major evolution in how care is delivered and managed. Through technologies like AI, mobile health tools, and telehealth, it provides real-time monitoring and communication, ensuring that HCPs can respond quickly—regardless of geographical location or patient limitations (e.g., people with disabilities who have more difficulty in accessing traditional clinical settings and resources). This integrated approach not only enhances treatment outcomes through individualized care but also supports scientific research by offering access to extensive data for analysis and discovery. As SHC continues to advance, it is expected to significantly improve drug development and disease prevention, making care more responsive and cost-effective.
Ultimately, SHC aims to optimize patient comfort and safety (i.e., quality of care and client satisfaction) while easing the burden on HCPs. By addressing the varied needs of both patients and professionals, it paves the way for a more connected, adaptable, and inclusive healthcare ecosystem—one where quality care is available anytime, anywhere, leading to better health outcomes and an improved quality of life worldwide. The key characteristics of smart hospitals based on the reviewed literature are summarized in Table 4.
Table 4.
Key characteristics of smart hospitals [54].
3.2.2. Bridging Drivers and Characteristics
To avoid conflating motivations with features, it helps to distinguish drivers from characteristics. Drivers explain why SHC adoption occurs—e.g., advances in AI/IoT and analytics, demographic change, workforce and cost pressures, interoperability requirements, and pandemic shocks [5,6,7,20,52]. Characteristics describe how SHC manifests in practice—for example, telemedicine, mobile health, wearables/remote monitoring, clinical decision support, radiomics, and shared/cloud data platforms used in clinical workflows [9,10,11,12,13,15,17]. To provide a better understanding, Table 5 demonstrates comparison examples between drivers and characteristics of SHC.
Table 5.
Drivers vs. characteristics of SHC.
3.2.3. Mini Cases: From Generic Challenges to Actionable Lessons
Case 1—AI in oncology (IBM Watson as a cautionary tale): Early oncology decision-support exemplified potential alongside limited explainability and variable local fit, highlighting the need for transparent rationale, local validation, and human oversight. Ethical anchors include autonomy (clinician judgment), beneficence (patient good), and documented accountability; operational controls include explanation summaries, bias/fairness evaluation across subgroups, and audit trails before routine use [5,13].
Case 2—Telemedicine equity during COVID-19: Pandemic-era telehealth sustained access but revealed digital divides (connectivity, devices, skills, language), leading to uneven benefits across populations [52]. Practical responses include low-bandwidth options, assisted/mediated visits, multilingual support, and monitoring of outcome gaps—not just visit counts. Privacy and consent safeguards aligned with GDPR/HIPAA principles and interoperable data flows help ensure remote encounters are captured in longitudinal records [20,52].
Governance note (cross-cutting): Translating ethics into concrete mechanisms entails model documentation and bias audits (fairness), rationale exposure (explainability), human-in-the-loop checkpoints (accountability), privacy/security impact assessments, and conformance testing for interoperability [5,13,20].
3.3. SHC Drivers
SHC systems have grown significantly in popularity due to their efficiency, user-friendliness, and ability to enhance patient care. As global advancements in technology and medicine continue, the adoption of SHC is expected to accelerate further. As shown in Figure 5, several major factors are driving this trend: rapid technological progress, the rise of digitally native populations, evolving patient care needs, shortages in the healthcare workforce, the rising cost of healthcare services, and the global impact of the COVID-19 pandemic.
Figure 5.
Key drivers of SHC adoption and use.
A significant driver behind the growing adoption of SHC is the rapid advancement of technologies such as the IoT, AI, and sophisticated data analytics. As digital-native populations (particularly “Generation Z”) continue to grow, there is an increasing demand for healthcare systems that are more integrated with modern technologies. Rising healthcare costs have also compelled institutions to seek more cost-effective methods of delivering quality care. SHC not only promises to enhance service delivery but also offers solutions to operational challenges and cost inefficiencies. Additionally, global healthcare workforce shortages underline the need for systems that maximize existing resources and support staff effectively.
The COVID-19 pandemic further underscored the necessity for adaptable and resilient healthcare systems. It accelerated the integration of SHC technologies to handle increased patient loads and maintain care continuity during lockdowns. This global crisis exposed the vulnerabilities of traditional healthcare systems and emphasized the critical role that technology plays in patient care. Consequently, many countries are now viewing SHC as a viable long-term solution to enhance patient outcomes and system responsiveness.
The following sections explore the primary factors propelling the shift toward SHC. Collectively, these drivers demonstrate the growing necessity and appeal of SHC. From economic pressures and evolving patient expectations to technological innovation and global health crises, numerous forces are reshaping healthcare into a more agile, efficient, and responsive system.
3.3.1. Technological Advancements
The global evolution of medical tools and technologies reflects the medical community’s long-standing pursuit of improved care. From early inventions like Dr. Laennec’s 19th-century stethoscope to today’s use of AI in diagnostics, healthcare has continuously evolved [55]. In the digital age, tools such as AI-driven diagnostics, online consultations, and smartphone-based monitoring are transforming care delivery. For instance, smartphone-based photoplethysmography combined with AI has shown promise in detecting conditions like diabetes [56]. AI applications extend to radiology, pathology, and drug development, where they aid in recruitment, trial simulations, and scenario modeling [57,58].
3.3.2. Digital Citizen Societies
Each generation grows up surrounded by the technologies of its era. Generation Z, having never known a world without the internet, is often referred to as “digital natives” [59]. They are quick to adapt and expect technology to be integrated into everyday life—including healthcare. As both patients and future HCPs, these individuals will expect health services to reflect their digitally connected lifestyles [60]. Healthcare systems must adapt to this demand by adopting smart solutions that align with the expectations of a tech-savvy population.
3.3.3. Shifting Models of Patient Care
As medical science advances, so too does the capacity to extend life expectancy and improve quality of life. The global aging population is growing rapidly, and healthcare systems must accommodate the unique needs of older adults. Remote care options, supported by sensors and monitoring devices, allow elderly individuals to receive quality care while remaining at home [61]. Examples from Japan and Osaka show how smart home technologies—ranging from biomedical devices to motion and appliance sensors—can facilitate independent living and proactive health monitoring [62,63].
3.3.4. Healthcare Workforce Shortages
The ubiquitous global shortage of HCPs has prompted the exploration of technological solutions to ease staff burdens. AI systems that provide continuous patient monitoring can reduce the need for constant manual oversight by nurses or HCPs [64]. These tools free up time for more complex, human-centered interactions while ensuring high-quality monitoring. Additionally, the explosion of healthcare data calls for systems capable of managing and analyzing large datasets efficiently—something that AI and digital platforms can facilitate [65].
3.3.5. Rising Costs of Healthcare Delivery
With healthcare expenditures projected to reach unsustainable levels—potentially consuming 20–30% of national GDP in most countries by 2050 [66]—cost-efficiency has become a top priority. SHC technologies help mitigate this issue by reducing errors, enabling round-the-clock patient monitoring, and streamlining administrative tasks [67]. Investments in digital infrastructure and cloud-based solutions have been shown to reduce operational overhead and increase record-keeping accuracy [68].
3.3.6. Impact of COVID-19
The COVID-19 pandemic fundamentally altered how healthcare is accessed and delivered. With strict lockdowns in place, remote consultations became essential, enabling patients to receive care via digital platforms [69]. While initially met with skepticism, remote consultations per se gained widespread acceptance due to their effectiveness and convenience (albeit long-term implications of the ruptures caused by the lack of normative face-to-face consultations continue to negatively affect health systems worldwide) [70]. Countries such as the UK, France, and Sweden experienced dramatic increases in teleconsultation usage, prompting the development of supporting policies and training programs [71,72]. This event validated the practicality of SHC and accelerated its integration into mainstream services.
3.4. SHC Deployment Challenges
As society embraces rapid technological evolution, services such as healthcare are increasingly integrating digital tools to improve outcomes and efficiency. Among these innovations is the concept of the smart hospital, which employs advanced technologies—such as AI, the IoT, big data, robotics, and automation—to enhance patient care, streamline operations, and improve the healthcare system’s overall efficiency [73,74].
By integrating smartphones, smartwatches, sensors, actuators, and connected devices into hospital infrastructure, often utilizing latent hardware and software that patients use in their lives (e.g., a low-cost healthcare app can be integrated into customers’ existing smartphones), smart hospitals aim to optimize workflows, reduce human error, and facilitate early diagnosis and prevention. While these innovations promise long-term cost savings and improved access, the transition to SHC remains slow due to a variety of technical, ethical, economic, and operational challenges [37]. The key challenges in SHC implementation are described below.
3.4.1. Reduced Human Interaction and Patient Monitoring
One of the primary concerns is the diminished presence of human HCPs. While technology can provide alerts (e.g., for a flatlining heart rate), it cannot replace the compassion and human-centered care of HCPs, nor indeed their clinical judgments [75]. Over-reliance on automation may lead to impersonal care and reduced patient trust.
3.4.2. Data Accuracy and Reliability
Smart hospitals depend on data to function efficiently. However, inaccurate or faulty data input can lead to errors, such as misdiagnosis, incorrect medication dosage, and treatment errors [76]. Implementing robust protocols to verify data integrity is essential to avoid harmful consequences for patients.
3.4.3. Data Security and Privacy
With smart hospitals relying heavily on cloud computing and internet-based communication, data breaches pose a significant risk. Unsecured systems can lead to stolen medical records, privacy violations, and loss of trust among patients [77,78]. Ensuring strong cybersecurity and employing skilled IT staff is essential to safeguarding sensitive health information.
3.4.4. Interoperability and System Performance
A hospital’s IoT ecosystem must support simultaneous usage by multiple users and devices. Without optimized authentication and data delivery systems, delays or system crashes can occur, compromising care [75,79]. Staff may also face difficulties adapting to new technologies if not properly trained [80].
3.4.5. Ethical Concerns and Trust in AI
AI, while efficient, lacks emotional intelligence and accountability. There is concern over its ability to make complex ethical decisions or be held responsible for medical errors. Disagreements between AI outputs and clinical judgment may also create confusion about whose decision to trust [81].
3.4.6. High Financial Costs
Although smart hospitals can reduce operational costs over time, the initial investment is significant. Costs include infrastructure development, software and hardware acquisition, staff training, and continuous upgrades [81,82]. For instance, implementing an RFID system alone—comprising tags, readers, middleware, and supporting infrastructure—can cost millions [83].
4. Discussion
SHC heralds a fundamental change from legacy to modern healthcare service delivery, toward anticipatory, interwoven, and connected devices, systems, and technologies. The reviewed studies indicate the key drivers of SHC development, adoption, and use, as well as commensurate challenges. SHC is posited on integrating digital solutions to optimize care quality, access, and efficiency, including by leveraging AI, big data analytics, the IoMT, and cloud computing.
Many of the obvious advantages of SHC, including increased accessibility and cost efficiency, are anchored in the way it transcends the physical barriers to care entailed with traditional clinical appointments and service delivery models. For instance, monitoring patients remotely and in real time (e.g., with constant monitoring of vital signs such as heart rate) via smart technologies enables health systems to address patient needs much more effectively and in a timely way, preventing exacerbation and optimizing health system resource use. This increases patient engagement and satisfaction, reducing the long-term escalations in symptom severity and treatment needs and costs.
On a practical, systemic level, increasing SHC proliferation and adoption is driven by technological advancements in technologies themselves, and increasing cost effectiveness (i.e., declining costs of smart solutions, and the fact that the majority of patients customarily use smartphones and other supporting infrastructure for SHC). Such solutions are vital, given the increasing numbers and proportions of older people worldwide, requiring more complex health interventions, and the systematic shortage of HCPs across the globe. As exposed during the COVID-19 pandemic from 2020 onwards, legacy systems are highly vulnerable to various threats, while digital solutions can make services more efficient and ensure their availability under disruption.
While it is beyond the scope of this review to make specific recommendations for policymaking, it is evident that the implications of these findings indicate that policymakers should take into account these potential benefits when considering the appropriate adoption of SHC in clinical practice.
However, while SHC offers obvious advantages, its implementation in practice can be problematic, especially with regard to handling (i.e., storing and communicating) patients’ sensitive data, cybersecurity, system compatibility factors (across multiple institutions and departments), and ethical issues (e.g., concerning the use of AI in making clinical decisions). More practical barriers include investment and ongoing costs, digital literacy issues (among patients, HCPs, and other users), and change resistance in complex healthcare service networks. Such challenges can only be addressed through an integrated and consultative strategic planning approach, including all related stakeholders and actively addressing multiple objectives, priorities, and concerns, to ensure that high-quality and equitable care delivery results from the SHC system.
5. Conclusions
SHC can reshape care delivery by using digital tools to make services more effective, affordable, sustainable, and person-centered. Real impacts depend on needs-led implementation, engaging diverse stakeholders (especially clinicians, patients, and health system managers). This is necessary to align solutions with service user needs, and with everyday workflows, while protecting privacy and safety. Success can be judged by tangible outcomes that improve quality of care, rather than technology uptake per se. In this vein, policy should prioritize interoperability as a first-order requirement. Health records, images, devices, and remote-monitoring data need to move safely and consistently across organizations and borders. This calls for the adoption of internationally recognized data and messaging standards, vendor conformance and certification during procurement, and explicit integration milestones so information flows are reliable from day one.
Workforce capability is equally crucial. HCPs benefit from role-specific training, protected time to learn, and local “super-user” support so digital tools are used confidently and appropriately. Change-management support, clear clinical governance, and feedback loops that link training to quality and safety indicators help secure lasting adoption.
Ethical assurance and equity should be operationalized in practice (rather than merely stated in principle). Fairness checks and bias audits, transparent rationales for AI-supported recommendations, human-in-the-loop oversight, and privacy/security impact assessments anchor autonomy, beneficence, and accountability in daily practice. At the same time, digital inclusion (e.g., last-mile connectivity, low-bandwidth options, assisted access, multilingual interfaces, and accessible design) can prevent the emergence of new disparities, particularly for older adults, rural communities, and people with disabilities.
Robust infrastructure and staged scaling reduce risk. Secure cloud and edge platforms, sound device management, and cyber-resilience offer a technical foundation, while regulatory sandboxes and real-world pilots can de-risk innovation before wider rollout. Transparent evaluation that reports clinical, operational, and economic outcomes enables systems to learn what truly works, and why.
There is a need for further research to identify the contribution of SHC at each stage of the patient journey, so that health systems can design governance, training, and interoperable architectures that unlock the full potential of digital healthcare transformation and support effective, large-scale deployment of SHC.
Author Contributions
Conceptualization, A.A. and Z.H.; methodology, A.A.; article review, A.A.; writing—original draft preparation, A.A.; writing—review and editing, Z.H.; supervision, N.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AI | Artificial Intelligence |
| AMI | Ambient Intelligence |
| CDSS | Clinical Decision Support System |
| EHealth | Electronic health |
| HCPs | Healthcare professionals |
| ICTs | Information and communication technologies |
| IoMT | Internet of Medical Things |
| IoT | Internet of Things |
| MHealth | Mobile health |
| RFID | Radio Frequency Identification |
| SHC | Smart healthcare |
References
- Gopal, G.; Suter-Crazzolara, C.; Toldo, L.; Eberhardt, W. Digital transformation in healthcare–architectures of present and future information technologies. Clin. Chem. Lab. Med. 2019, 57, 328–335. [Google Scholar] [CrossRef]
- Thacharodi, A.; Singh, P.; Meenatchi, R.; Tawfeeq Ahmed, Z.H.; Kumar, R.R.; V, N.; Kavish, S.; Maqbool, M.; Hassan, S. Revolutionizing healthcare and medicine: The impact of modern technologies for a healthier future—A comprehensive review. Health Care Sci. 2024, 3, 329–349. [Google Scholar] [CrossRef]
- Ahmad, K.A.B.; Khujamatov, H.; Akhmedov, N.; Bajuri, M.Y.; Ahmad, M.N.; Ahmadian, A. Emerging trends and evolutions for smart city healthcare systems. Sustain. Cities Soc. 2022, 80, 103695. [Google Scholar] [CrossRef]
- Yin, H.; Akmandor, A.O.; Mosenia, A.; Jha, N.K. Smart healthcare. Found. Trends Electron. Des. Autom. 2018, 12, 401–466. [Google Scholar] [CrossRef]
- Du-Harpur, X.; Watt, F.M.; Luscombe, N.M.; Lynch, M.D. What is AI? Applications of artificial intelligence to dermatology. Brit. J. Dermatol. 2020, 183, 423–430. [Google Scholar] [CrossRef]
- Wan, J.; Al-awlaqi, M.A.A.H.; Li, M.; O’Grady, M.; Gu, X.; Wang, J.; Cao, N. Wearable IoT enabled real-time health monitoring system. J. Wirel. Commun. Netw. 2018, 298. [Google Scholar] [CrossRef]
- Guo, C.; Chen, J. Big data analytics in healthcare. In Knowledge Technology and Systems: Toward Establishing Knowledge Systems Science; Nakamori, Y., Ed.; Springer: Cham, Switzerland, 2023; pp. 27–70. ISBN 978-981-99-1075-5. [Google Scholar] [CrossRef]
- Faridi, F.; Sarwar, H.; Ahtisham, M.; Jamal, K. Cloud computing approaches in health care. Mater. Today Proc. 2022, 51, 1217–1223. [Google Scholar] [CrossRef]
- Sood, S.; Mbarika, V.; Jugoo, S.; Dookhy, R.; Doarn, C.R.; Prakash, N.; Merrell, R.C. What is telemedicine? A collection of 104 peer-reviewed perspectives and theoretical underpinnings. Telemed. e-Health 2007, 13, 573–590. [Google Scholar] [CrossRef] [PubMed]
- Dias, D.; Paulo Silva Cunha, J. Wearable health devices—Vital sign monitoring, systems and technologies. Sensors 2018, 18, 2414. [Google Scholar] [CrossRef] [PubMed]
- Pagliari, C.; Sloan, D.; Gregor, P.; Sullivan, F.; Detmer, D.; Kahan, J.P.; Oortwijn, W.; MacGillivray, S. What is eHealth (4): A scoping exercise to map the field. J. Med. Internet Res. 2005, 7, e391. [Google Scholar] [CrossRef] [PubMed]
- Cortez, N. The mobile health revolution. UCDL Rev. 2013, 47, 1173. [Google Scholar]
- Beeler, P.E.; Bates, D.W.; Hug, B.L. Clinical decision support systems. Swiss Med. Wkly. 2014, 144, w14073. [Google Scholar] [CrossRef] [PubMed]
- Mechanic, O.J.; Persaud, Y.; Kimball, A.B. TeleHealth Systems; StatPearls Publishing: Treasure Island, FL, USA, 2017. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459384/ (accessed on 3 February 2025).
- Koçak, B.; Durmaz, E.Ş.; Ateş, E.; Kılıçkesmez, Ö. Radiomics with artificial intelligence: A practical guide for beginners. Diagn. Interv. Radiol. 2019, 25, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Krukowski, A.; Barca, C.C.; Rodríguez, J.M.; Vogiatzaki, E. Personal health record. In Cyberphysical Systems for Epilepsy and Related Brain Disorders: Multi-Parametric Monitoring and Analysis for Diagnosis and Optimal Disease Management; Voros, N., Antonopoulos, C., Eds.; Springer: Cham, Switzerland, 2015; pp. 205–238. ISBN 978-3-319-20049-1. [Google Scholar] [CrossRef]
- Kamel, M.; George, L. Remote patient tracking and monitoring system. Int. J. Comput. Sci. Mob. Comput. 2013, 2, 88–94. [Google Scholar]
- Jarrahi, M.H.; Eshraghi, A. Digital natives vs digital immigrants: A multidimensional view on interaction with social technologies in organizations. J. Enterp. Inf. Manag. 2019, 32, 1051–1070. [Google Scholar] [CrossRef]
- Chua, J.A. Cybersecurity in the healthcare industry. Physician Leadersh. J. 2021, 8, 69–72. Available online: https://www.physicianleaders.org/articles/cybersecurity-healthcare-industry-collaborative-approach (accessed on 3 February 2025).
- Kuziemsky, C.E.; Peyton, L. A framework for understanding process interoperability and health information technology. Health Policy Technol. 2016, 5, 196–203. [Google Scholar] [CrossRef]
- Ajami, S.; Rajabzadeh, A. Radio frequency identification (RFID) technology and patient safety. J. Res. Med. Sci. 2013, 18, 809–813. [Google Scholar]
- Cook, D.J.; Augusto, J.C.; Jakkula, V.R. Review: Ambient intelligence: Technologies, applications, and opportunities. Pervasive Mob. Comput. 2009, 5, 277–298. [Google Scholar] [CrossRef]
- Vishnu, S.; Ramson, S.J.; Jegan, R. Internet of medical things (IoMT)—An overview. In Proceedings of the 2020 5th International. Conference on Devices, Circuits and Systems (ICDCS), Coimbatore, India, 5–6 March 2020; IEEE: New York, NY, USA, 2020; pp. 101–104. [Google Scholar] [CrossRef]
- Zhao, W.; Luo, X.; Qiu, T. Smart healthcare. Appl. Sci. 2017, 7, 1176. [Google Scholar] [CrossRef]
- Dukhanin, V.; Topazian, R.; DeCamp, M. Metrics and evaluation tools for patient engagement in healthcare organization and system-level decision-making: A systematic review. Int. J. Health Policy. Manag. 2018, 7, 889. [Google Scholar] [CrossRef]
- Holzinger, A.; Röcker, C.; Ziefle, M. From smart health to smart hospitals. In Smart Health: Open Problems and Future Challenges; Holzinger, A., Röcker, C., Ziefle, M., Eds.; Springer: Cham, Switzerland, 2015; pp. 1–20. ISBN 978-3-319-16226-3. [Google Scholar] [CrossRef]
- Quaranta-Finsiel, A.A. “Smart hospitals” in the environment and in the territory. J. Clin. Comput. 1988, 17, 23–27. [Google Scholar]
- Kaldoudi, E. Smart hospital: The future of healthcare. Comput. Struct. Biotechnol. J. 2024, 24, 87–88. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.; Yang, W.; Le Grange, J.M.; Wang, P.; Huang, W.; Ye, Z. Smart healthcare: Making medical care more intelligent. Glob. Health J. 2019, 3, 62–65. [Google Scholar] [CrossRef]
- Dhar, J.; Ranganathan, A. Machine learning capabilities in medical diagnosis applications: Computational results for hepatitis disease. Int. J. Biomed. Eng. Technol. 2015, 17, 330–340. [Google Scholar] [CrossRef]
- Sulaiman, H.; Wickramasinghe, N. Assimilating healthcare information systems in a Malaysian hospital. Commun. Assoc. Inf. Syst. 2014, 34, 77. [Google Scholar] [CrossRef]
- Zaw, T.O.K.; Muthaiyah, S.; Jasbi, A. Contextualization of smart healthcare: A systematic review. In Proceedings of the 2021 7th International Conference on Research and Innovation in Information Systems (ICRIIS), Johor Bahru, Malaysia, 25–26 October 2021; IEEE: New York, NY, USA, 2021; pp. 1–6. [Google Scholar] [CrossRef]
- Vidyasekar, A.D. Strategic Opportunity Analysis of the Global Smart City Market: Smart City Market Is Likely to Be Worth A Cumulative 1.565 Trillion by 2020. 2013. Available online: http://www.digitaljournal.com/pr/1601758 (accessed on 3 February 2025).
- Sundaravadivel, P.; Kougianos, E.; Mohanty, S.P.; Ganapathiraju, M.K. Everything you wanted to know about smart health care: Evaluating the different technologies and components of the internet of things for better health. IEEE Consum. Electron. Mag. 2017, 7, 18–28. [Google Scholar] [CrossRef]
- Zeadally, S.; Siddiqui, F.; Baig, Z.; Ibrahim, A. Smart healthcare: Challenges and potential solutions using internet of things (IoT) and big data analytics. PSU Res. Rev. 2020, 4, 149–168. [Google Scholar] [CrossRef]
- Harwood, T.G.; Garry, T. An overview of content analysis. Mark. Rev. 2003, 3, 479–498. [Google Scholar] [CrossRef]
- Sligo, J.; Gauld, R.; Roberts, V.; Villa, L. A literature review for large-scale health information system project planning, implementation and evaluation. Int. J. Med. Inf. 2017, 97, 86–97. [Google Scholar] [CrossRef]
- Sarkar, M.; Lee, T.H.; Sahoo, P.K. Smart healthcare: Exploring the internet of medical things with ambient intelligence. Electronics 2024, 13, 2309. [Google Scholar] [CrossRef]
- Kwon, H.; An, S.; Lee, H.-Y.; Cha, W.C.; Kim, S.; Cho, M.; Kong, H.-J. Review of smart hospital services in real healthcare environments. Healthc. Inform. Res. 2022, 28, 3–15. [Google Scholar] [CrossRef]
- Kathirvel, S.; Chakraborty, S. Rural Community Health Workers’ Readiness for Mobile-Phone-Based Telemedicine Uptake in India. J. Rural Med. 2022, 17, 166–170. [Google Scholar]
- Tan, H.Y.; Tan, J.K.; Lam, L.T.; Tan, D.H.; Chua, Y.X. Insights into Singapore’s national strategy for primary care reform: Physician attitudes, facilitators and barriers to healthier SG. BMC Health Serv. Res. 2025, 25, 1021. [Google Scholar] [CrossRef]
- Woon, B. [Singapore] Health Database in an IT society. Jpn. Med. Assoc. J. 2014, 57, 212–215. [Google Scholar]
- Yang, Y.; Venkatachalam, I.; Low, C.T.; Foo, M.Z.Q.; Aung, M.K.; See, S.W.J.; Aung, M.O.; Chan, D.Y.W.; Arora, S.; Sim, J.X.Y.; et al. Transforming healthcare system: Outcomes of Healthier-SG from a large tertiary-care hospital in Singapore. Health Policy Technol. 2025, 14, 100968. [Google Scholar] [CrossRef]
- Man, R.E.K.; Ho, A.X.Y.; Lee, E.P.X.; Fenwick, E.K.D.; Aravindhan, A.; Ho, K.C.; Tan, G.S.W.; Ting, D.S.W.; Wong, T.Y.; Yeo, K.K.; et al. Awareness and attitudes of elderly Southeast Asian adults towards telehealth during the COVID-19 pandemic: A qualitative study. Singap. Med. J. 2025, 66, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Dastidar, B.G.; Jani, A.R.; Suri, S.; Nagaraja, V.H. Reimagining India’s National Telemedicine Service to improve access to care. Lancet Reg. Health Southeast Asia 2024, 30, 100480. [Google Scholar] [CrossRef] [PubMed]
- Verma, N.; Buch, B.; Taralekar, R.; Acharya, S. Diagnostic concordance of telemedicine as compared with face-to-face care in primary health care clinics in rural India: Randomized crossover trial. JMIR Form. Res. 2023, 7, e42775. [Google Scholar] [CrossRef]
- Joshi, K.; Modi, B.; Katoch, C.D.S. Utilization of telemedicine services of institute of national importance in the western region of India: A mixed-method study. J. Fam. Med. Prim. Care 2024, 13, 3782–3787. [Google Scholar] [CrossRef]
- Nagaraja, V.H.; Dastidar, B.G.; Suri, S.; Jani, A.R. Perspectives and use of telemedicine by doctors in India: A cross-sectional study. Health Policy Technol. 2024, 13, 100845. [Google Scholar] [CrossRef]
- Narwadiya, S.C.; Rao, D.R. Telemedicine in India: An impact analysis. Intell. Hosp. 2025, 1, 100004. [Google Scholar] [CrossRef]
- NHS. About the NHS App. 2023. Available online: https://www.nhs.uk/nhs-app/about-the-nhs-app/ (accessed on 3 February 2025).
- Wosik, J.; Fudim, M.; Cameron, B.; Gellad, Z.F.; Cho, A.; Phinney, D.; Curtis, S.; Roman, M.; Poon, E.G.; Ferranti, J.; et al. Telehealth transformation: COVID-19 and the rise of virtual care. J. Am. Med. Inform. Assoc. 2020, 27, 957–962. [Google Scholar] [CrossRef]
- Kumar, S.; Merchant, S.; Reynolds, R. Tele-ICU: Efficacy and cost-effectiveness approach of remotely managing the critical care. Open Med. Inform. J. 2013, 7, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, B.A.; Dorman, T.; Breslow, M.J.; Pronovost, P.; Jenckes, M.; Zhang, N.; Anderson, G.; Rubin, H. Intensive care unit telemedicine: Alternate paradigm for providing continuous intensivist care. Crit. Care Med. 2000, 28, 3925–3931. [Google Scholar] [CrossRef]
- Almarri, A.; Hunaiti, Z.; Daoud, M.S.; Manivannan, N. Shaping the future of healthcare: The key characteristics and drivers of smart hospitals. In Proceedings of the 2024 Global Digital Health Knowledge Exchange & Empowerment Conference (gDigiHealthKEE), Abu Dhabi, United Arab Emirates, 24–26 September 2024; IEEE: New York, NY, USA, 2024; pp. 1–7. [Google Scholar] [CrossRef]
- Cheng, T.O. How Laënnec invented the stethoscope. Int. J. Cardiol. 2007, 118, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Avram, R.; Olgin, J.E.; Kuhar, P.; Hughes, J.W.; Marcus, G.M.; Pletcher, M.J.; Aschbacher, K.; Tison, G.H. A digital biomarker of diabetes from smartphone-based vascular signals. Nat. Med. 2020, 26, 1576–1582. [Google Scholar] [CrossRef] [PubMed]
- Lamberti, M.J.; Wilkinson, M.; Donzanti, B.A.; Wohlhieter, G.E.; Parikh, S.; Wilkins, R.G.; Getz, K. A study on the application and use of artificial intelligence to support drug development. Clin. Ther. 2019, 41, 1414–1426. [Google Scholar] [CrossRef]
- Barisoni, L.; Lafata, K.J.; Hewitt, S.M.; Madabhushi, A.; Balis, U.G. Digital pathology and computational image analysis in nephropathology. Nat. Rev. Nephrol. 2020, 16, 669–685. [Google Scholar] [CrossRef]
- Foo, C.; Woon, T.H.; Chia, H.X.; Yap, J.C.H.; Lee, W.S.; Lee, C.E.; Valderas, J.M.; Tan, C.; Teo, K.W. Healthier SG: A gateway for evolving public-private-population partnerships in population health. Lancet Reg. Health West. Pac. 2025, 60, 101606. [Google Scholar] [CrossRef]
- Wang, S.-K.; Hsu, H.-Y.; Campbell, T.; Coster, D.C.; Longhurst, M. An investigation of middle school science teachers and students use of technology inside and outside of classrooms: Considering whether digital natives are more technology savvy than their teachers. Educ. Technol. Res. Dev. 2014, 62, 637–662. [Google Scholar] [CrossRef]
- Lu, J.; Hao, Q.; Jing, M. Consuming, sharing, and creating content: How young students use new social media in and outside school. Comput. Hum. Behav. Rep. 2016, 64, 55–64. [Google Scholar] [CrossRef]
- Chan, M.; Campo, E.; Estève, D.; Fourniols, J.Y. Smart homes—Current features and future perspectives. Maturitas 2009, 64, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Tamura, T.; Ogawa, M.; Yoda, M.; Togawa, T. Fully automated health monitoring system in the home. Med. Eng. Phys. 1998, 20, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Vrančić, A.; Zadravec, H.; Orehovački, T. The role of smart homes in providing care for older adults: A systematic literature review from 2010 to 2023. Smart Cities 2024, 7, 1502–1550. [Google Scholar] [CrossRef]
- Patil, S.; Shankar, H. Transforming healthcare: Harnessing the power of AI in the modern era. Int. J. Multidiscip. Sci. Arts 2023, 2, 60–70. [Google Scholar] [CrossRef]
- Jakobs, R. How Tech Can Tackle Healthcare Workloads and Staff Shortages. Available online: https://www.weforum.org/agenda/2023/01/healthcare-workloads-and-staff-shortages-davos23/ (accessed on 3 February 2025).
- Drouin, J.P.; Hediger, V.; Henke, N. Health Care Costs: A Market-Based View. Available online: https://www.mckinsey.com/~/media/mckinsey/dotcom/client_service/healthcare%20systems%20and%20services/pdfs/healthcare-costs-a-market-based-view.pdf (accessed on 3 February 2025).
- Sakr, S.; Elgammal, A. Towards a comprehensive data analytics framework for smart healthcare services. Big Data Res. 2016, 4, 44–58. [Google Scholar] [CrossRef]
- Stoumpos, A.I.; Kitsios, F.; Talias, M.A. Digital transformation in healthcare: Technology acceptance and its applications. Int. J. Environ. Res. Public Health 2023, 20, 3407. [Google Scholar] [CrossRef]
- Richardson, E.; Aissat, D.; Williams, G.A.; Fahy, N. Keeping what works: Remote consultations during the COVID-19 pandemic. Eurohealth 2020, 26, 73–76. [Google Scholar]
- Pronk, N.P.; McEvoy, C. Equitable well-being, social trust, and the economy: An integrated health system’s perspectives on the long-term implications of COVID-19. Prog. Cardiovasc. Dis. 2023, 76, 57–60. [Google Scholar] [CrossRef]
- Donaghy, E.; Atherton, H.; Hammersley, V.; McNeilly, H.; Bikker, A.; Robbins, L.; Campbell, J.; McKinstry, B. Acceptability, benefits, and challenges of video consulting: A qualitative study in primary care. Br. J. Gen. Pract. 2019, 69, e586–e594. [Google Scholar] [CrossRef]
- NHS Digital. Appointments in General Practice Data. 2022. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/mi-appointments-in-general-practice/current (accessed on 3 February 2025).
- Nwobodo-Anyadiegwu, E.N.; Ditend, M.N.; Lumbwe, A.K. The benefits and challenges of implementing smart hospital projects: A systematic review. In Proceedings of the 2022 IEEE 28th International Conference on Engineering, Technology and Innovation (ICE/ITMC) & 31st International Association for Management of Technology (IAMOT) Joint Conference, Nancy, France, 19–23 June 2022; pp. 1–7. [Google Scholar] [CrossRef]
- Uslu, B.Ç.; Okay, E.; Dursun, E. Analysis of factors affecting IoT-based smart hospital design. J. Cloud Comput. 2020, 9, 67. [Google Scholar] [CrossRef]
- Sebastian, M.P. Smart Hospitals: Challenges and Opportunities. Available online: https://forms.iimk.ac.in/websiteadmin/FacultyPublications/Working%20Papers/3052smartHospitals_MPS2019.pdf (accessed on 3 February 2025).
- Ameri, A.; Salmanizadeh, F.; Keshvardoost, S.; Bahaadinbeigy, K. Investigating pharmacists’ views on telepharmacy: Prioritizing key relationships, barriers, and benefits. J. Pharm. Technol. 2020, 36, 171–178. [Google Scholar] [CrossRef]
- Rizk, D.K.A.A.; Hosny, H.M.; ElHorbety, S.; Salem, A.B. SMART hospital management systems based on internet of things: Challenges, intelligent solutions and functional requirements. Int. J. Intell. Comput. Inf. Sci. 2022, 22, 32–43. [Google Scholar] [CrossRef]
- de Paiva Marques Carvalho, T.; de Paiva, J.C.; de Medeiros Valentim, R.A.; Silva, C.B.P.; de Lima, D.F.; Silva, E.C. Sabiá: An authentication, authorization, and user data delivery architecture based on user consent for health information systems in Brazil. Res. Biomed. Eng. 2020, 36, 197–202. [Google Scholar] [CrossRef]
- Dawson, J.; Fisher, E.; Wiese, J. Hospital employee experiences caring for patients in smart patient rooms. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems (CHI’24), Honolulu, HI, USA, 11–16 May 2024; ACM: New York, NY, USA, 2024; pp. 1–16. [Google Scholar] [CrossRef]
- Renukappa, S.; Mudiyi, P.; Suresh, S.; Abdalla, W.; Subbarao, C. Evaluation of challenges for adoption of smart healthcare strategies. Smart Health 2022, 26, 100330. [Google Scholar] [CrossRef]
- Kruse, C.S.; Mileski, M.; Alaytsev, V.; Carol, E.; Williams, A. Adoption factors associated with electronic health record among long-term care facilities: A systematic review. BMJ Open 2015, 5, e006615. [Google Scholar] [CrossRef]
- Seckman, C.; Bauer, A.; Moser, T.; Paaske, S. The Benefits and Barriers to RFID Technology in Healthcare. Available online: https://www.himss.org/resources/benefits-and-barriers-rfid-technology-healthcare (accessed on 3 February 2025).





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).