Abstract
Background/Objectives: People with multiple sclerosis (MS) often experience sensory, psychomotor, and cognitive impairment, sphincter disturbances, and fatigue, which can affect their ability to perform work-related tasks, self-care, and daily activities. This study aimed to analyze the lifestyle changes, cognitive function, and disability outcomes over a seven-year follow-up period, exploring potential associations with predictive markers. Methods: At the end of the seven-year follow-up period, 32 participants returned for cognitive and clinical reassessment with the Twenty-Five-Foot Walk Test, Nine-Hole Peg Test, and Brief Repeatable Neuropsychological Battery. Lifestyle data were acquired via interviews regarding sleep quality, reading habits, technology use, physical activity levels, household responsibilities, and participation in leisure and cultural activities. Results: The occupational profile did not demonstrate significant changes, but 11 (34%) participants showed disability accumulation, and the number of relapses increased (p = 0.001). Over time, improvement was observed in verbal episodic memory and worsening in psychomotor speed. Better cognitive performance in mental agility was associated with higher levels of physical activity (p = 0.021) and technology use (p = 0.039). In addition, better cognition (verbal memory p = 0.038 and processing speed 0.015) and psychomotor speed (upper limbs p = 0.017 and lower limbs p = 0.003) and lower functional disability (p = 0.022) were associated with maintenance of household activities. Conclusions: The changes in verbal memory and psychomotor speed were more prominent over time, and verbal memory, psychomotor and processing speed, and mental agility were associated with good lifestyle habits, mainly household activities. The treatment strategies should include lifestyle changes and pharmacological interventions.
1. Introduction
Multiple sclerosis (MS) is an inflammatory and neurodegenerative disease characterized by a progressive worsening of disabilities and a range of associated symptoms. People with MS (pwMS) often experience visual and sensory alterations, psychomotor impairment, sphincter disturbances, fatigue, and cognitive deficits [1], which can significantly impact their ability to perform work-related tasks, self-care, and daily activities [2,3,4,5]. Walking difficulties are particularly disruptive, affecting quality of life (QoL), physical function, and participation in social and occupational activities [6,7]. Research has demonstrated that integrated care models prioritizing lifestyle factors can play a critical role in maintaining cognitive reserve in pwMS. For instance, the MS Brain Health Initiative advocates for a holistic approach to disease management, highlighting the importance of optimizing brain health through prompt diagnosis, early treatment initiation, and structured lifestyle interventions. This “brain-healthy lifestyle” includes six modifiable factors: physical activity, weight management, cognitive engagement, smoking cessation, responsible alcohol consumption, and therapy adherence [8].
The disability outcomes primarily focus on motor impairment; however, mental health is also profoundly affected in MS, with over a third of newly diagnosed individuals experiencing anxiety or depression, which correlates with reduced QoL [9]. Cognitive impairment [7], which is present in up to 45% of early-stage MS patients and can even occur in the preclinical phase [10], further deteriorates QoL [11,12,13]. Compared with cognitively preserved individuals, pwMS with cognitive impairment exhibit reduced engagement in daily life, work, and social activities [14] and it also interferes with treatment adherence, coping strategies, and the ability to benefit from rehabilitation interventions [15,16]. The relationship between cognitive function and daily activities has been underscored by previous research. For instance, a study assessing 41 pwMS found a strong correlation between performance on the Brief International Cognitive Assessment for MS (BICAMS) test and activity independence, as measured by computerized tools. The participants with MS performed significantly worse than the healthy controls [7,17] on both the BICAMS and activity-related metrics, with better BICAMS performance linked to more independent functioning [18].
Regular physical activity has emerged as a key modifiable factor with neuroprotective benefits. It not only alleviates fatigue and enhances mood but also may help to preserve cognitive function [19,20,21,22,23,24,25]. Additionally, physical exercise exerts a synergistic effect when combined with cognitive rehabilitation in pwMS with established cognitive impairment [17]. Although individual studies have linked lifestyle factors to MS severity, comprehensive data on their relative contributions to long-term outcomes remain limited. Therefore, the current study aimed to analyze lifestyle changes, cognitive function, and disability outcomes over a seven-year follow-up period, exploring potential associations with predictive markers. By integrating lifestyle factors into the understanding of MS progression, we hope to elucidate strategies that can enhance patient care and improve long-term outcomes.
2. Materials and Methods
2.1. Ethical Approval
This is a prospective and exploratory study, approved by the Ethics Committee for Research Projects Analysis (CAPPesq 2.454.027/2014) of the Hospital das Clínicas of Medicine School of the University of São Paulo, and conducted in accordance with the Helsinki Declaration of 1975, revised in 2008. All participants provided written informed consent prior to participation.
2.2. Participants
A total of 32 individuals diagnosed with multiple sclerosis (pwMS) were enrolled (baseline), with age between 18 and 65 years, more than 4 years of education, and diagnoses made according to the revised 2017 McDonald criteria [26]. Participants were recruited from the Neuroimmunology Clinic. The individuals were re-evaluated after seven years (follow-up) (only the 32 individuals with baseline and follow-up data were included in this study). Exclusion criteria included uncontrolled psychiatric disorder, other neurological disease, diabetes, and any other metabolic alteration without treatment; more details appear in previously published studies by our research group [27,28].
2.3. Procedures and Assessment
A multidisciplinary team conducted comprehensive assessments. Data collection included the following: age, sex, race or ethnicity, occupation, years of education, comorbidities [29], smoking habits, MS phenotype (classified as relapsing–remitting [RRMS] or progressive [PMS]), duration of symptoms, years since diagnosis, number of relapses, and current DMT. DMTs were categorized as high-efficacy if patients were receiving Natalizumab, Ocrelizumab, or Alemtuzumab.
Neurological function and disability progression were evaluated by neurologists (M.S.P. and G.A.S.F.) using the Expanded Disability Status Scale (EDSS) [30]. Psychomotor performance was also assessed through the Twenty-Five-Foot Walk Test (25-FWT) and the Nine-Hole Peg Test (9-HPT) [31]. Cognitive assessments were conducted by a trained neuropsychologist (K.R.C.) utilizing the Brief Repeatable Neuropsychological Battery [32]. Further details on the assessment procedures are available in prior publications [27].
At the follow-up visit, lifestyle factors were evaluated through interviews covering a range of topics, including sleep quality, reading habits, technology use, physical activity levels, household responsibilities, and participation in leisure and cultural activities. The topics and frequency structuring were selected from the Cognitive Reserve Index Questionnaire (CRIq) [33].
2.4. Clinical Classification Criteria
Disease progression was assessed by confirmed disability accumulation (CDA), based on the comparison between data obtained at follow-up and baseline, and confirmation through evaluation of medical records [34]. CDA events were considered as (a) an increase in EDSS of ≥1.0 point for participants with a baseline EDSS ≤ 5.5 or ≥0.5 points for those with a baseline EDSS > 5.5, and (b) a ≥ 20% decline in 25-FWT or 9-HPT performance compared to previous assessments. Conversely, progression independent of relapse activity (PIRA) was defined as disability accumulation confirmed at least three months after a relapse-free interval in the preceding year [35]. No evidence of disease activity (NEDA-3) was defined as the absence of relapses, CDA, and new MRI-detected lesions in the prior year [36].
2.5. Statistical Analysis
In cross-sectional or repeated measures analyses, the variables were treated as continuous, with scores on cognitive tests and scales used in their raw state. These represent a count of points whose distributions demonstrate a tendency towards asymmetry, which was evident for some of the variables in Shapiro–Wilk normality test. Consequently, in order to achieve greater homogeneity in the statistical tests adopted, we elected to use those statistics that are appropriate for asymmetric distributions.
Descriptive analyses were conducted using the Wilcoxon signed-rank test for continuous variables and the McNemar or Likelihood Ratio tests for categorical variables. Correlations between variables were assessed using Spearman’s rank correlation coefficient. Generalized Estimating Equation (GEE) models (binary logistic regression and gamma distribution with log link) were employed to analyze longitudinal data, both with and without adjustments for potential confounding factors. Cognitive tests were adjusted for age and years of education, psychomotor speed tasks were adjusted for age, and EDSS was not adjusted. Cross-sectional analyses were conducted to compare variables between the different phenotypes (RRMS and PMS) at baseline or follow-up. When necessary, the Likelihood Ratio was employed for different proportions, and the Mann–Whitney U test was used for continuous measurements.
Statistical analyses were conducted using SPSS version 20, with a significance threshold set at p < 0.05.
3. Results
3.1. Sample Characterization
Among the thirty-two participants, nineteen (59.4%) were initially classified as RRMS and thirteen (40.6%) as PMS. At follow-up, three participants previously classified as RRMS showed sustained CDA and therefore were converted to SPMS. As a result, the final classification of the sample was sixteen participants (50%) as PMS and sixteen (50%) as RRMS, with no statistically significant changes (p = 0.250). Table 1 presents the changes in participant characteristics.

Table 1.
Characterization of the participants.
The occupational profile did not exhibit significant changes overall; at both baseline and follow-up, the majority of pwMS receiving government assistance were of the progressive phenotype (25% at baseline: RRMS = 2, PMS = 6; 44% at follow-up: RRMS = 3, PMS = 11). Notably, seven pwMS (RRMS = 1, PMS = 6) discontinued work and became reliant on government financial assistance, with the progressive phenotype exhibiting the highest frequency of this transition. Conversely, two pwMS (RRMS = 1, PMS = 1) who initially received temporary government assistance subsequently returned to employment.
At baseline, the majority of the unemployed pwMS were classified as RRMS (n = 7), while, at follow-up, the majority were classified as PMS (n = 3). Among the nine pwMS who were unemployed at baseline, three initiated occupational activities (all RRMS), three began receiving government assistance (one RRMS, one PMS, and one RRMS who converted to PMS), and three remained unemployed (one PMS and two RRMS who converted to PMS).
3.2. Clinical, Cognitive, and Disability Changes
Over the seven-year follow-up period, eleven participants (34%) showed CDA. Considering the previous year, three participants met the PIRA criteria, while nine of the eighteen participants met the NEDA-3 criteria.
Although the participants with PMS had a longer mean disease duration compared to those with RRMS (PMS: 18.5 ± 7.2 years vs. RRMS: 13.6 ± 6.2 years; p = 0.381), the difference was not statistically significant. Conversely, the RRMS participants had a longer time since diagnosis compared to the PMS participants (RRMS: 12.7 ± 4.9 years vs. PMS: 10.4 ± 4.6 years; p = 0.094), although neither difference reached statistical significance.
Over the seven years, the number of relapses increased significantly (baseline: 4.6 ±4.7 vs. follow-up: 5.2 ± 5.1; p = 0.001). As expected, the relapse rates during follow-up were higher in the RRMS group (0.8 ± 0.9) compared to the PMS group (0.4 ± 0.8), but this was not statistically significant (p = 0.082). At baseline, ten participants (31%) were using high-efficacy DMTs. Of the ten patients at baseline, seven (70%) maintained high-efficacy treatment at follow-up and three (30%) interrupted treatment. Among the fifteen participants on high-efficacy DMTs at follow-up, eight (53%) began DMT use during the study period. The majority of the pwMS had RRMS at both baseline (6 of 10—60%) and follow-up (12 of 15—80%). Longitudinally, the number of comorbidities between baseline and follow-up did not change, and there was no difference between the RRMS and PMS groups regarding comorbidity burden.
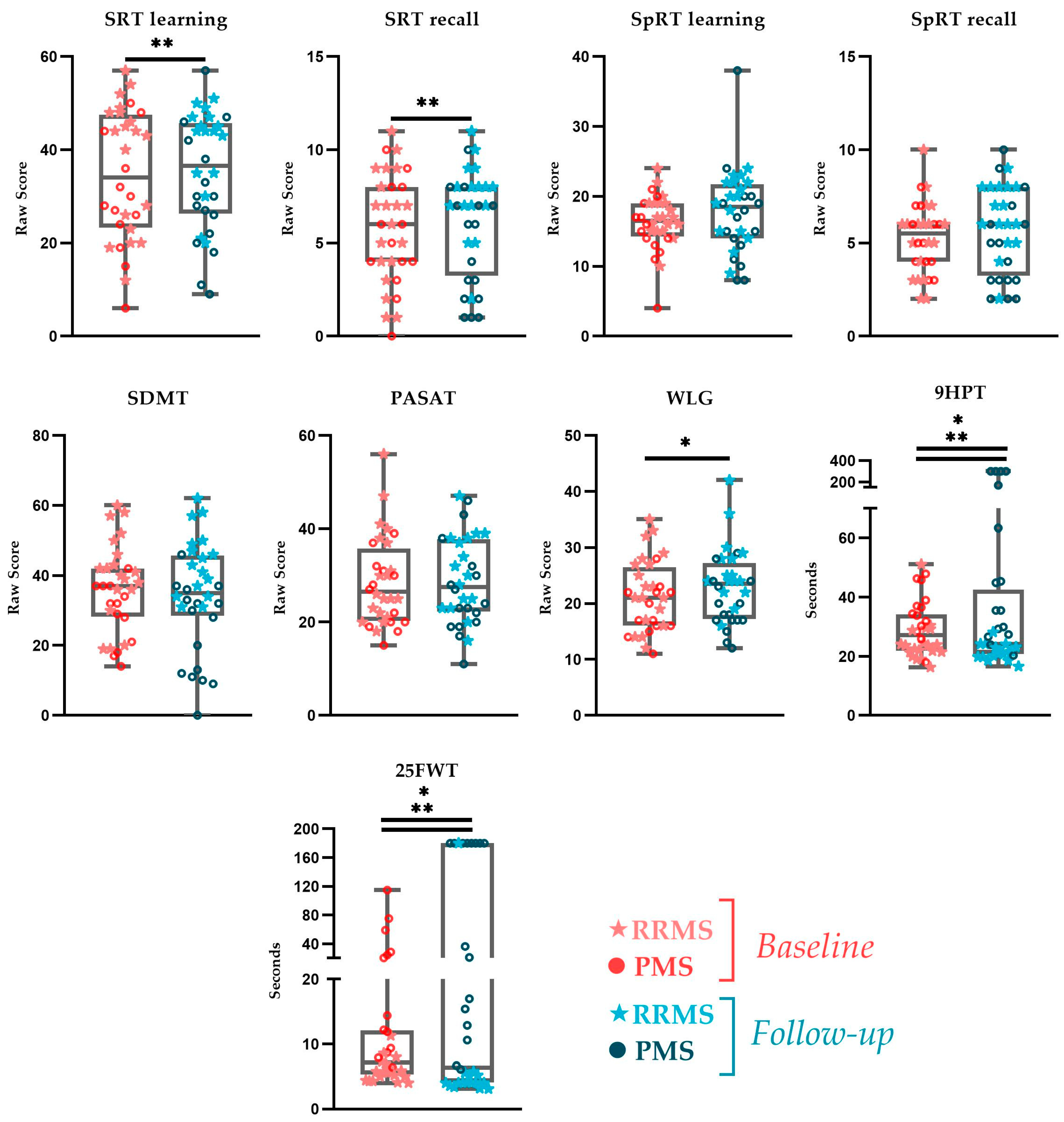
In the initial analyses, unadjusted for potential confounding factors, significant differences were observed in the comparisons of follow-up with baseline, with improvement in lexical access speed (WLG), while psychomotor speed for the upper and lower limbs (9HPT and 25FWT) as well as overall disability assessed by the EDSS (Figure 1) worsened. After adjusting for bias, when pertinent, the significant improvement in verbal episodic memory (SRT learning and recall) and the worsening in motor speed (9HPT and 25FWT) persisted (Figure 1).
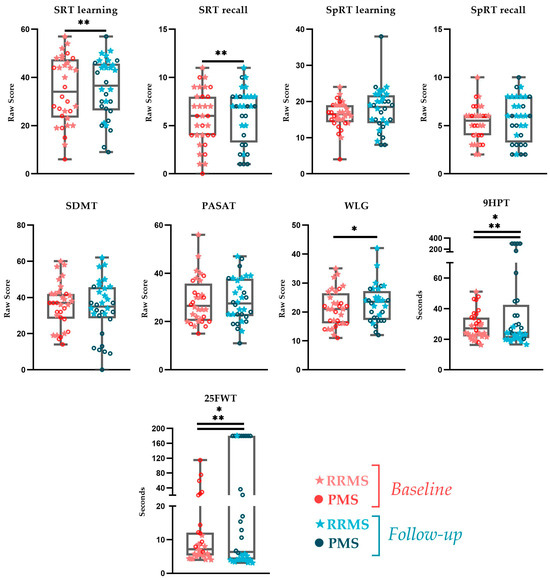
Figure 1.
Longitudinal comparisons for cognitive test and psychomotor speed tasks. Legend: the graphs show crude scores. (*) Generalized Equation Estimation time effect. (**) Generalized Equation Estimation time effect adjusted for age and years of education. Acronyms: PASAT—Paced Auditory Serial Addition Test; SDMT—Symbol Digit Modalities Test; SpRT—Spatial Recall Test; SRT—Selective Reminding Test; WLG—Word List Generation; 9HPT—Nine-Hole Peg Test; 25FWT—Twenty-Five-Foot Walk Test.
Considering phenotypes, there was a significant improvement in verbal episodic memory in the RRMS group (SRT learning β = 0.161, p = 0.016 and recall β = 0.293, p = 0.003), while, for PMS, significant worsening was observed in psychomotor speed (9HPT β = 1.180, p < 0.001 and 25FWT β = 1.423, p < 0.001). Longitudinal comparisons were significant for disabilities exclusively for the PMS phenotype (EDSS β = 0.071, p = 0.025).
3.3. Lifestyle and Associations with Clinical, Cognitive, and Functional Disabilities
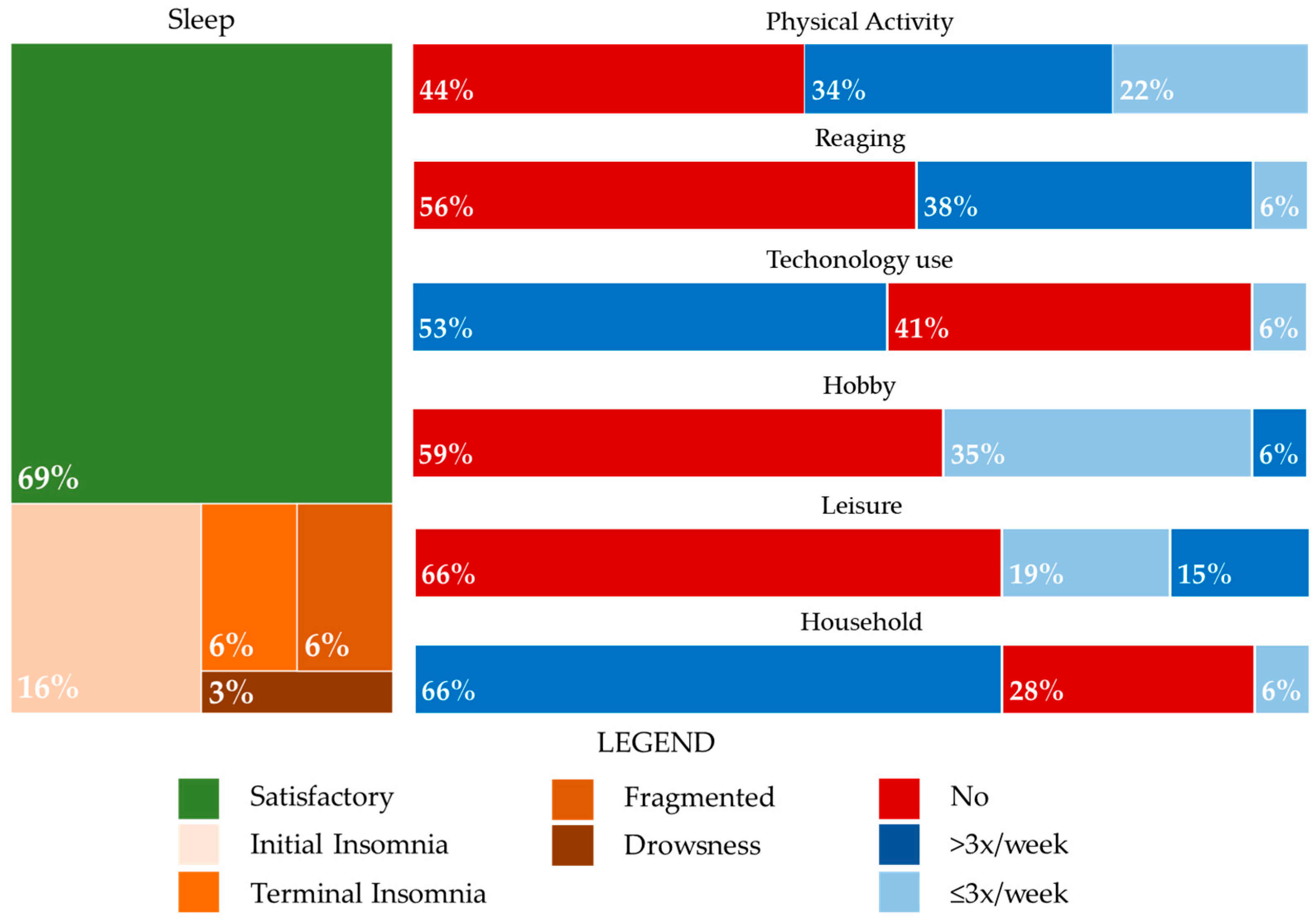
Lifestyle factors were also assessed at follow-up. A significant reduction in smoking was observed, with the number of participants who smoked decreasing from eleven (34%) at baseline to four (13%) at follow-up (p = 0.016). Among the individuals who continued smoking, all reported consumption of less than one pack per week. Of those who quit smoking, four were from the PMS and three from the RRMS groups, with three experiencing CDA and five having a disease duration exceeding 10 years. Figure 2 illustrates the frequency and proportion of lifestyle activities across the entire sample.
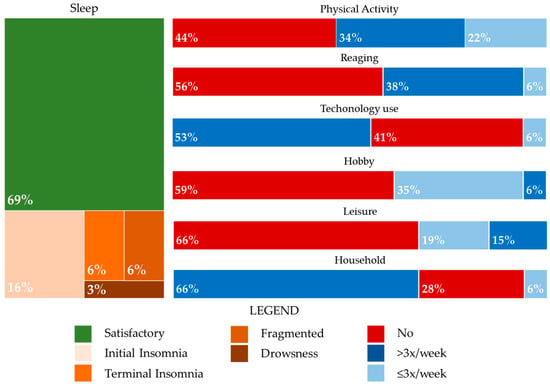
Figure 2.
Lifestyle activities at follow-up: frequency and proportion.
The sleep quality was reported to be similar between the RRMS and PMS groups, with initial insomnia being the most common sleep disturbance. A sedentary lifestyle was more prevalent among the participants with PMS (RRMS: 5; PMS: 9; p = 0.154), as was lower technology use (RRMS: 3; PMS: 10; p = 0.012). The PMS group also reported less engagement in leisure activities (RRMS: 9; PMS: 12; p = 0.264), hobbies (RRMS: 6; PMS: 13; p = 0.012), and household activities (RRMS: 0; PMS: 9; p < 0.001).
Reading habits were slightly more common among the participants with PMS, with news (n = 9; RRMS: 3, PMS: 6; p = 0.476) and literature books (n = 10; RRMS: 5, PMS: 5) being the preferred genres. Scholarly book reading (n = 3; RRMS: 1, PMS: 2) and social media texts (n = 4; RRMS: 2, PMS: 2) were less frequently reported. There was no significant correlation between years of education and reading frequency (r = 0.202, p = 0.269).
In the follow-up analysis, adjusted when necessary for age and years of education, there were no significant associations between cognitive function or disability status and sleep quality, leisure activities, or reading habits. However, better performance on the PASAT, a measure of mental agility, was associated with the practice of physical activity (β = 0.123, p = 0.021), technology use (β = 0.128, p = 0.039), and household activities (β = 0.090, p = 0.050). Better verbal memory recall (SRT—β = 0.405, p = 0.038), fast processing speed (SDMT—β = 0.086, p = 0.015), lower psychomotor speed (9HPT—β = −0.014, p = 0.017), and worse walking capacity (25FWT—β = −0.057, p = 0.003) were associated with the practice of household activity. Lower values of EDSS were associated with hobby activity (β = −0.555, p = 0.022). Lower learning visuospatial memory was associated with the practice of hobby activity (β = −0.149, p = 0.044), but the participants engaged in hobby activities were primarily in the RRMS group, with higher values of EDSS and a tendency to CDA.
4. Discussion
The current longitudinal and exploratory study investigated the disease-related changes in pwMS and their associations with lifestyle factors. The findings showed that MS-related cognitive impairments and functional disabilities had significant and mostly negative associations with lifestyle. The accumulation of disability in MS is a complex multifactorial process, and recent research has enriched our understanding beyond the traditional markers of disease activity, particularly with regard to PIRA [35]. Although highly effective DMTs have improved the suppression of classic disease activity, such as relapse and new focal lesions on MRI, they show limited efficacy in halting the ongoing accumulation of disability, especially in the progressive stages [35,37]. For instance, although the majority of the patients in our cohort were being treated with high-efficacy DMTs, with no significant difference in DMT use between the baseline and follow-up, we observed CDA in one-third of the patients over the seven-year follow-up period. Additionally, three patients experienced PIRA in the final year of observation, with worsened functional outcomes in tests such as the SDMT, EDSS, 9HPT, and 25FWT regardless of the MS phenotype.
It is worth noting that most of the participants achieved NEDA-3 when considering the clinical data in the previous year, which may have contributed to the improvement in cognitive performance observed in our cohort. Whilst the improvement in the measures of lexical access speed was better explained by age and years of education, it is known that years of education has a protective effect [38]; the increase in verbal episodic memory occurred only for pwRRMS. This may indicate the potential for accurate treatment to maintain cognitive performance and, consequently, the capacity to undertake daily activities, such as physical exercise, technology use, and household activities. Similar results were observed in prior studies, one with a follow-up of 6 years, and associated with MRI volumetric measures, such as higher cortical volume in the regions of the left hemispheric and subcortical regions at baseline [39,40]. In contrast, we observed worsening in disabilities, particularly in psychomotor speed in pwPMS, as expected in the clinical course of a progressive disease [41,42].
Despite the cognitive improvement, the burden of MS on employment capacity was evident in our study, with over half of the patients being either unemployed or receiving government benefits at both baseline and follow-up. The worsening disability, mostly in terms of motor function, can more directly justify these findings. This trend is consistent globally, where the unemployment rates range from 30% to 43% within 11 to 19 years of disease onset [43,44,45,46], and MS diagnosis is also known to more than triple the likelihood of the patient losing their existing job [12,47,48]. Job retention was diminished in patients with progressive MS, consistent with previous data linking more severe MS phenotypes and fatigue to lower employment rates [46,47,49]. Our study suggests that those patients with RRMS were more likely to transition from unemployment to occupational activities. Contrarily, pwPMS were more likely to be receiving government benefits, strengthening the notion that disability accumulation in PMS is mostly an irreversible process [41,42,49].
The significant reduction in smoking observed at follow-up is a notable finding. Although the reasons for smoking cessation were not explored in depth, it is encouraging that this behavioral change occurred among both the RRMS and PMS participants, and especially those with longer disease duration and clinical disability. This finding highlights the need to reinforce lifestyle changes at any disease stage as smoking cessation is linked to slower disease progression and a reduced risk of reaching disability milestones [50,51]. Thus, assessing lifestyle habits and their potential associations with functional outcomes may reveal the extent to which changes in a patient’s routine can positively influence their functional status and vice versa [3,26,46].
Our data also suggest that those participants with PMS tended to present more sedentary behavior, reporting lower levels of physical activity, technology use, and engagement in leisure or household activities. Although not all these differences reached statistical significance, they reveal a concerning trend in individuals with greater disability accumulation, who may be at risk of further decline due to inactivity [50,52,53]. Interestingly, the participants with PMS read more than those with RRMS; this lifestyle habit plays a fundamental role in maintaining cognitive status [54] and does not require great psychomotor demands. Better cognitive performance and psychomotor speed and less disability were associated with sleep quality, leisure activities, physical activity, technology use, and household engagement, similar to previous studies [50,52,53]. Those participants who engaged in hobbies prevailed in the RRMS group and had higher EDSS scores, with a tendency toward CDA; this may explain the poorer performance in visual memory since the presence of relapses and the accumulation of impairments led to a worse cognitive status.
The 7-year follow-up is one of the strengths of our study, which enabled us to observe changes in both clinical and lifestyle factors over time. However, the relatively small sample size limits the generalizability of our findings, and the absence of certain baseline lifestyle data, such as technology use and household activity, may have hindered a more detailed analysis of their long-term impact. Additionally, our reliance on self-reported lifestyle measures introduces the possibility of recall bias. Furthermore, we did not collect data on healthy control participants, which could contribute to more robust comparisons. At the same time, associations of lifestyle data with neuroimaging acquisitions may provide further insights into the findings of this work.
5. Conclusions
In conclusion, the current study provides additional evidence of the complex interplay between MS progression, disability accumulation, and lifestyle factors. Changes in occupational activities and abandonment/loss of occupational activity can be justified by these aspects. At the same time, verbal memory, psychomotor and processing speed, and mental agility were associated with good lifestyle habits, mainly maintenance of household activities. While DMTs play a crucial role in managing disease activity, our findings highlight the importance of maintaining physical and cognitive engagement in order to mitigate the effects of disability and cognitive decline. Future research should explore interventions that promote activity and participation in daily life as part of a comprehensive management strategy for pwMS.
Author Contributions
K.R.C.: data curation, conceptualization, formal analysis, writing and review, original draft preparation; G.A.S.F.: data curation, conceptualization, formal analysis, writing and review, original draft preparation; M.S.P.: data curation, conceptualization, review, original draft preparation; S.L.A.-P.: review original draft; D.C.: review original draft; C.A.B.: review original draft; D.d.P.F.: conceptualization, validation, review original draft, supervision and validation. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by São Paulo Research Foundation [grant number 2018/15167–1]. D.d.P.F. is a research fellow of the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq 302527/2022-2). K.R.C. has a research fellowship from Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo “Adote um pesquisador” program (HCFMUSP: cg19215).
Institutional Review Board Statement
This study was approved by the Ethics Committee for Research Projects Analysis (CAPPesq 2.454.027/2014) of the Hospital das Clínicas of Medicine School of the University of São Paulo on 19 April 2014.
Informed Consent Statement
All participants were informed about the risks and benefits of the study. Any doubts were resolved, and participants provided written informed consent prior to participation.
Data Availability Statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request. The data are not publicly available due to ethical restrictions.
Acknowledgments
We would like to thank all pwMS who collaborated with us and agreed to be called for further investigative examinations, in addition to the biomedical technologist and nurse teams from the Center of Nuclear Medicine of the Radiology Institute of the Hospital das Clínicas Faculdade de Medicina da Universidade de São Paulo for their technical assistance and support.
Conflicts of Interest
The authors declare no conflicts of interest.
Correction Statement
This article has been republished with a minor correction to the Institutional Review Board Statement. This change does not affect the scientific content of the article.
References
- Dendrou, C.A.; Fugger, L.; Friese, M.A. Immunopathology of Multiple Sclerosis. Nat. Rev. Immunol. 2015, 15, 545–558. [Google Scholar] [CrossRef] [PubMed]
- Amtmann, D.; Bamer, A.M.; Kim, J.; Chung, H.; Salem, R. People with Multiple Sclerosis Report Significantly Worse Symptoms and Health Related Quality of Life than the US General Population as Measured by PROMIS and NeuroQoL Outcome Measures. Disabil. Health J. 2018, 11, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Lobentanz, I.S.; Asenbaum, S.; Vass, K.; Sauter, C.; Klosch, G.; Kollegger, H.; Kristoferitsch, W.; Zeitlhofer, J. Factors Influencing Quality of Life in Multiple Sclerosis Patients: Disability, Depressive Mood, Fatigue and Sleep Quality. Acta Neurol. Scand. 2004, 110, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Morales-Gonzáles, J.M.; Benito-León, J.; Rivera-Navarro, J.; Mitchell, A.J.; GEDMA Study Group. A Systematic Approach to Analyse Health-Related Quality of Life in Multiple Sclerosis: The GEDMA Study. Mult. Scler. J. 2004, 10, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Ruet, A.; Deloire, M.; Hamel, D.; Ouallet, J.-C.; Petry, K.; Brochet, B. Cognitive Impairment, Health-Related Quality of Life and Vocational Status at Early Stages of Multiple Sclerosis: A 7-Year Longitudinal Study. J. Neurol. 2013, 260, 776–784. [Google Scholar] [CrossRef] [PubMed]
- LaRocca, N.G. Impact of Walking Impairment in Multiple Sclerosis: Perspectives of Patients and Care Partners. Patient Patient-Centered Outcomes Res. 2011, 4, 189–201. [Google Scholar] [CrossRef]
- Motl, R.W.; Snook, E.M.; McAuley, E.; Scott, J.A.; Hinkle, M.L. Demographic Correlates of Physical Activity in Individuals with Multiple Sclerosis. Disabil. Rehabil. 2007, 29, 1301–1304. [Google Scholar] [CrossRef] [PubMed]
- Giovannoni, G.; Butzkueven, H.; Dhib-Jalbut, S.; Hobart, J.; Kobelt, G.; Pepper, G.; Sormani, M.P.; Thalheim, C.; Traboulsee, A.; Vollmer, T. Brain Health: Time Matters in Multiple Sclerosis; Oxford PharmaGenesis Ltd.: Oxford, UK, 2015. [Google Scholar] [CrossRef]
- Janssens, A.C.J.W.; Van Doorn, P.A.; De Boer, J.B.; Van Der Meché, F.G.A.; Passchier, J.; Hintzen, R.Q. Impact of Recently Diagnosed Multiple Sclerosis on Quality of Life, Anxiety, Depression and Distress of Patients and Partners: Quality of Life and Emotional Well-Being in MS. Acta Neurol. Scand. 2003, 108, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Cortese, M.; Riise, T.; Bjørnevik, K.; Bhan, A.; Farbu, E.; Grytten, N.; Hogenesch, I.; Midgard, R.; Smith Simonsen, C.; Telstad, W.; et al. Preclinical Disease Activity in Multiple Sclerosis: A Prospective Study of Cognitive Performance Prior to First Symptom. Ann. Neurol. 2016, 80, 616–624. [Google Scholar] [CrossRef]
- DiGiuseppe, G.; Blair, M.; Morrow, S.A. Short Report: Prevalence of Cognitive Impairment in Newly Diagnosed Relapsing-Remitting Multiple Sclerosis. Int. J. MS Care 2018, 20, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.; Rashid, W.; Cercignani, M.; Langdon, D. Cognitive Impairment among Patients with Multiple Sclerosis: Associations with Employment and Quality of Life. Postgrad. Med. J. 2017, 93, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Oset, M.; Stasiolek, M.; Matysiak, M. Cognitive Dysfunction in the Early Stages of Multiple Sclerosis—How Much and How Important? Curr. Neurol. Neurosci. Rep. 2020, 20, 22. [Google Scholar] [CrossRef] [PubMed]
- Fenu, G.; Fronza, M.; Lorefice, L.; Arru, M.; Coghe, G.; Frau, J.; Marrosu, M.G.; Cocco, E. Performance in Daily Activities, Cognitive Impairment and Perception in Multiple Sclerosis Patients and Their Caregivers. BMC Neurol. 2018, 18, 212. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.P.; Zipoli, V.; Portaccio, E. Multiple Sclerosis-Related Cognitive Changes: A Review of Cross-Sectional and Longitudinal Studies. J. Neurol. Sci. 2006, 245, 41–46. [Google Scholar] [CrossRef]
- Goretti, B.; Portaccio, E.; Zipoli, V.; Hakiki, B.; Siracusa, G.; Sorbi, S.; Amato, M.P. Coping Strategies, Psychological Variables and Their Relationship with Quality of Life in Multiple Sclerosis. Neurol. Sci. 2009, 30, 15–20. [Google Scholar] [CrossRef]
- Motl, R.W.; Sandroff, B.M.; DeLuca, J. Exercise Training and Cognitive Rehabilitation: A Symbiotic Approach for Rehabilitating Walking and Cognitive Functions in Multiple Sclerosis? Neurorehabil. Neural Repair 2016, 30, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Goverover, Y.; Chiaravalloti, N.; DeLuca, J. Brief International Cognitive Assessment for Multiple Sclerosis (BICAMS) and Performance of Everyday Life Tasks: Actual Reality. Mult. Scler. J. 2016, 22, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Ozkul, C.; Guclu-Gunduz, A.; Eldemir, K.; Apaydin, Y.; Yazici, G.; Irkec, C. Combined Exercise Training Improves Cognitive Functions in Multiple Sclerosis Patients with Cognitive Impairment: A Single-Blinded Randomized Controlled Trial. Mult. Scler. Relat. Disord. 2020, 45, 102419. [Google Scholar] [CrossRef]
- Motl, R.W.; Pilutti, L.A. The Benefits of Exercise Training in Multiple Sclerosis. Nat. Rev. Neurol. 2012, 8, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Cotman, C.W.; Berchtold, N.C.; Christie, L.-A. Exercise Builds Brain Health: Key Roles of Growth Factor Cascades and Inflammation. Trends Neurosci. 2007, 30, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Sandroff, B.M.; Klaren, R.E.; Pilutti, L.A.; Dlugonski, D.; Benedict, R.H.B.; Motl, R.W. Randomized Controlled Trial of Physical Activity, Cognition, and Walking in Multiple Sclerosis. J. Neurol. 2014, 261, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Sandroff, B.M.; Balto, J.M.; Klaren, R.E.; Sommer, S.K.; DeLuca, J.; Motl, R.W. Systematically Developed Pilot Randomized Controlled Trial of Exercise and Cognition in Persons with Multiple Sclerosis. Neurocase 2016, 22, 443–450. [Google Scholar] [CrossRef]
- Briken, S.; Gold, S.; Patra, S.; Vettorazzi, E.; Harbs, D.; Tallner, A.; Ketels, G.; Schulz, K.; Heesen, C. Effects of Exercise on Fitness and Cognition in Progressive MS: A Randomized, Controlled Pilot Trial. Mult. Scler. J. 2014, 20, 382–390. [Google Scholar] [CrossRef]
- Feys, P.; Moumdjian, L.; Van Halewyck, F.; Wens, I.; Eijnde, B.O.; Van Wijmeersch, B.; Popescu, V.; Van Asch, P. Effects of an Individual 12-Week Community-Located “Start-to-Run” Program on Physical Capacity, Walking, Fatigue, Cognitive Function, Brain Volumes, and Structures in Persons with Multiple Sclerosis. Mult. Scler. J. 2019, 25, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of Multiple Sclerosis: 2017 Revisions of the McDonald Criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Campanholo, K.; Pitombeira, M.; Rimkus, C.; Mendes, M.; Apóstolos-Pereira, S.; Busatto Filho, G.; Callegaro, D.; Buchpiguel, C.; Duran, F.; De Paula Faria, D. Myelin Imaging Measures as Predictors of Cognitive Impairment in MS Patients: A Hybrid PET-MRI Study. Mult. Scler. Relat. Disord. 2022, 57, 103331. [Google Scholar] [CrossRef] [PubMed]
- Pitombeira, M.S.; Koole, M.; Campanholo, K.R.; Souza, A.M.; Duran, F.L.S.; Solla, D.J.F.; Mendes, M.F.; Pereira, S.L.A.; Rimkus, C.M.; Busatto, G.F.; et al. Innate Immune Cells and Myelin Profile in Multiple Sclerosis: A Multi-Tracer PET/MR Study. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 4551–4566. [Google Scholar] [CrossRef]
- Horton, M.; Rudick, R.A.; Hara-Cleaver, C.; Marrie, R.A. Validation of a Self-Report Comorbidity Questionnaire for Multiple Sclerosis. Neuroepidemiology 2010, 35, 83–90. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating Neurologic Impairment in Multiple Sclerosis: An Expanded Disability Status Scale (EDSS). Neurology 1983, 33, 1444. [Google Scholar] [CrossRef]
- Rodrigues, J.d.L.; Ferreira, F.d.O.; Haase, V.G. Perfil do Desempenho Motor e Cognitivo na Idade Adulta e Velhice. Gerais Rev. Interinstitucional Psicol. 2008, 1, 20–33. Available online: https://pepsic.bvsalud.org/pdf/gerais/v1n1/v1n1a04.pdf (accessed on 6 November 2024).
- Damasceno, A.; Amaral, J.M.S.D.S.; Barreira, A.A.; Becker, J.; Callegaro, D.; Campanholo, K.R.; Damasceno, L.A.; Diniz, D.S.; Fragoso, Y.D.; Franco, P.S.; et al. Normative Values of the Brief Repeatable Battery of Neuropsychological Tests in a Brazilian Population Sample: Discrete and Regression–Based Norms. Arq. Neuropsiquiatr. 2018, 76, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, A.R.; Pereira, L.D. TRADUÇÃO, VALIDAÇÃO CULTURAL E SEMÂNTICA DO COGNITIVE RESERVE INDEX QUESTIONNAIRE (criq) PARA O PORTUGUÊS BRASILEIRO. Estud. Interdiscip. Sobre O Envelhec. 2022, 27. [Google Scholar] [CrossRef]
- Kappos, L.; Wolinsky, J.S.; Giovannoni, G.; Arnold, D.L.; Wang, Q.; Bernasconi, C.; Model, F.; Koendgen, H.; Manfrini, M.; Belachew, S.; et al. Contribution of Relapse-Independent Progression vs Relapse-Associated Worsening to Overall Confirmed Disability Accumulation in Typical Relapsing Multiple Sclerosis in a Pooled Analysis of 2 Randomized Clinical Trials. JAMA Neurol. 2020, 77, 1132. [Google Scholar] [CrossRef]
- Lublin, F.D.; Häring, D.A.; Ganjgahi, H.; Ocampo, A.; Hatami, F.; Čuklina, J.; Aarden, P.; Dahlke, F.; Arnold, D.L.; Wiendl, H.; et al. How Patients with Multiple Sclerosis Acquire Disability. Brain 2022, 145, 3147–3161. [Google Scholar] [CrossRef] [PubMed]
- Giovannoni, G.; Tomic, D.; Bright, J.R.; Havrdová, E. “No Evident Disease Activity”: The Use of Combined Assessments in the Management of Patients with Multiple Sclerosis. Mult. Scler. J. 2017, 23, 1179–1187. [Google Scholar] [CrossRef]
- Dobson, R.; Giovannoni, G. Multiple Sclerosis—A Review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef]
- Rimkus, C.D.M.; Avolio, I.M.B.; Miotto, E.C.; Pereira, S.A.; Mendes, M.F.; Callegaro, D.; Leite, C.D.C. The Protective Effects of High-Education Levels on Cognition in Different Stages of Multiple Sclerosis. Mult. Scler. Relat. Disord. 2018, 22, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Kania, K.; Pawlak, M.A.; Forycka, M.; Wiłkość-Dębczyńska, M.; Michalak, S.; Łukaszewska, A.; Wyciszkiewicz, A.; Wypych, A.; Serafin, Z.; Marcinkowska, J.; et al. Predicting Clinical Progression and Cognitive Decline in Patients with Relapsing-Remitting Multiple Sclerosis: A 6-Year Follow-up Study. Neurol. Neurochir. Pol. 2024, 58, 176–184. [Google Scholar] [CrossRef]
- Boa, I.N.F.; Rimkus, C.D.M.; Campanholo, K.R.; Pereira, S.L.A.; Junqueira, T.D.F.; Machado, M.D.A.R.; Callegaro, D.; Otaduy, M.C.G.; Leite, C.D.C.; Miotto, E.C. Longitudinal Analysis of Verbal Episodic Memory in Patients with Relapsing-Remitting Multiple Sclerosis. Arq. Neuropsiquiatr. 2018, 76, 302–309. [Google Scholar] [CrossRef]
- Sumowski, J.F.; Benedict, R.; Enzinger, C.; Filippi, M.; Geurts, J.J.; Hamalainen, P.; Hulst, H.; Inglese, M.; Leavitt, V.M.; Rocca, M.A.; et al. Cognition in Multiple Sclerosis: State of the Field and Priorities for the Future. Neurology 2018, 90, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Lassmann, H.; Van Horssen, J.; Mahad, D. Progressive Multiple Sclerosis: Pathology and Pathogenesis. Nat. Rev. Neurol. 2012, 8, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Moore, P.; Harding, K.E.; Clarkson, H.; Pickersgill, T.P.; Wardle, M.; Robertson, N.P. Demographic and Clinical Factors Associated with Changes in Employment in Multiple Sclerosis. Mult. Scler. J. 2013, 19, 1647–1654. [Google Scholar] [CrossRef] [PubMed]
- Fantoni-Quinton, S.; Kwiatkowski, A.; Vermersch, P.; Roux, B.; Hautecoeur, P.; Leroyer, A. Impact of Multiple Sclerosis on Employment and Use of Job-Retention Strategies: The Situation in France in 2015. J. Rehabil. Med. 2016, 48, 535–540. [Google Scholar] [CrossRef]
- Chiu, C.-Y.; Chan, F.; Edward Sharp, S.; Dutta, A.; Hartman, E.; Bezyak, J. Employment as a Health Promotion Intervention for Persons with Multiple Sclerosis. Work 2015, 52, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Bøe Lunde, H.M.; Telstad, W.; Grytten, N.; Kyte, L.; Aarseth, J.; Myhr, K.-M.; Bø, L. Employment among Patients with Multiple Sclerosis-A Population Study. PLoS ONE 2014, 9, e103317. [Google Scholar] [CrossRef]
- Raggi, A.; Covelli, V.; Schiavolin, S.; Scaratti, C.; Leonardi, M.; Willems, M. Work-Related Problems in Multiple Sclerosis: A Literature Review on Its Associates and Determinants. Disabil. Rehabil. 2016, 38, 936–944. [Google Scholar] [CrossRef]
- Salter, A.; Thomas, N.; Tyry, T.; Cutter, G.; Marrie, R.A. Employment and Absenteeism in Working-Age Persons with Multiple Sclerosis. J. Med. Econ. 2017, 20, 493–502. [Google Scholar] [CrossRef]
- Da Silva, N.L.; Takemoto, M.L.S.; Damasceno, A.; Fragoso, Y.D.; Finkelsztejn, A.; Becker, J.; Gonçalves, M.V.M.; Tilbery, C.; De Oliveira, E.M.L.; Callegaro, D.; et al. Cost Analysis of Multiple Sclerosis in Brazil: A Cross-Sectional Multicenter Study. BMC Health Serv. Res. 2016, 16, 102. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Neate, S.; Nag, N.; Bevens, W.; Jelinek, G.; Simpson-Yap, S.; Davenport, R.A.; Fidao, A.; Reece, J. Baseline Engagement with Healthy Lifestyles and Their Associations with Health Outcomes in People with Multiple Sclerosis Enrolled in an Online Multimodal Lifestyle Course. Eur. J. Neurol. 2024, 31, e16429. [Google Scholar] [CrossRef] [PubMed]
- Johansson, S.; Skjerbæk, A.G.; Nørgaard, M.; Boesen, F.; Hvid, L.G.; Dalgas, U. Associations between Fatigue Impact and Lifestyle Factors in People with Multiple Sclerosis – The Danish MS Hospitals Rehabilitation Study. Mult. Scler. Relat. Disord. 2021, 50, 102799. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.P.; Prestipino, E.; Bellinvia, A.; Niccolai, C.; Razzolini, L.; Pastò, L.; Fratangelo, R.; Tudisco, L.; Fonderico, M.; Mattiolo, P.L.; et al. Cognitive Impairment in Multiple Sclerosis: An Exploratory Analysis of Environmental and Lifestyle Risk Factors. PLoS ONE 2019, 14, e0222929. [Google Scholar] [CrossRef] [PubMed]
- Cederberg, K.L.J.; Jeng, B.; Sasaki, J.E.; Motl, R.W. Physical Activity and Sedentary Behavior Timing in Fatigued and Nonfatigued Adults With Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2022, 103, 1758–1765. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Pandigama, D.H.; Wrigglesworth, J.; Owen, A.; Woods, R.L.; Chong, T.T.-J.; Orchard, S.G.; Shah, R.C.; Sheets, K.M.; McNeil, J.J.; et al. Lifestyle Enrichment in Later Life and Its Association With Dementia Risk. JAMA Netw. Open 2023, 6, e2323690. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).