Abstract
Multiple sclerosis (MS) is associated with a high prevalence of emotional disorders affecting the health-related quality of life of patients and their families. Pseudobulbar affect (PBA), also referred to as pathological laughing and crying, is an under-recognized and under-treated co-morbidity. We conducted a systematic literature review of 16 studies to determine the prevalence and clinical characteristics of PBA in patients with MS of all ages. Based on conservative figures available from 8/16 studies, the prevalence of PBA in the context of MS was found to range between 2% and 10% (median 10%), with higher percentages in the female population. Possible reasons for the observed variability in the prevalence data include heterogeneity of the diagnostic methodologies and common presence of confounding factors, such as co-morbid affective disorders. The clinical presentation was found to be comparable to that of PBA in the context of other neurological disorders, as it reflected the location of underlying lesions (especially in the brainstem) rather than the associated pathology. Clinicians should be prompted to consider PBA in the differential diagnosis of emotional disorders in the context of MS by using both clinical criteria and psychometric instruments. Further studies should be conducted to develop standardized diagnostic protocols and to optimize therapeutic approaches for the clinical management of this patient population.
1. Introduction
The neuropathological process of multiple sclerosis (MS) is characterized by demyelinating lesions that can affect any structure of the central nervous system, particularly the white matter of the cerebral hemispheres, brainstem, optic nerves, spinal cord, and cerebellum. In addition to the presence of established cerebrospinal fluid biomarkers, neuroimaging findings provide evidence of pathological dissemination across both space and time [1,2]. The clinical phenomenology depends on the affected regions, and includes motor and sensory deficits, optic neuritis, diplopia, fatigue, cerebellar syndromes, sphincteric continence issues, and neuropsychiatric disorders. The latter are relatively common and range from specific cognitive deficits to affective disorders, with partial overlaps [3]. Both the biological mechanisms underlying MS and the physical and psychological burden of this chronic condition could be responsible for the development of neuropsychiatric features. It has been argued that alterations in the external expression of emotions, such as euphoria and apathy, may result directly from MS-related pathophysiological processes, whereas consistent alterations of the inner emotional states, such as depression and anxiety, might have a more complex and multifactorial pathogenesis, including psychological, social, neurobiological, immunological, and genetic factors [4,5].
From an epidemiological perspective, affective disorders are the most common psychiatric co-morbidity in MS, reported by the majority of patients [3,5]. The diagnosis of neuropsychiatric co-morbidities in patients with MS can be challenging [6,7]. Specifically, affective symptoms often present with manifestations that overlap with the clinical manifestations of MS, such as fatigue, irritability, reduced concentration, and changes in sleep and appetite [3,5]. It has been pointed out that affective disorders can be under-diagnosed and under-treated in patients with MS [3], despite their impact on illness progression, functional status, health-related quality of life, and suicidal risk [5].
Pseudobulbar affect (PBA), also referred to as pathological laughing and crying or involuntary emotional expression disorder [8], is a clinical syndrome characterized by short, intense, and frequent episodes of laughter and/or weeping with little or absent correlation to emotional stimuli [9]. Three subgroups of patients have been described: those presenting with outbursts of laughing only, those with outbursts of crying only, and those with both clinical manifestations [10]. Phenomenologically, these manifestations are barely distinguishable from emotion-related laughing and crying, and most patients maintain intact awareness of their symptoms, unless their underlying neurological conditions are complicated by cognitive impairment [10,11]. Consequently, the episodes of uncontrolled and context-inappropriate laughing and/or crying can cause embarrassment and discomfort that often end up in increasingly poor social interactions and isolation [11]. PBA has been reported in the context of MS, as well as in association with neurodegenerative conditions (Parkinson’s disease, multiple system atrophy, progressive supranuclear palsy, amyotrophic lateral sclerosis, dementias such as Alzheimer’s disease, etc.) and focal brain pathologies (traumatic brain injury, brain tumor, stroke, etc.) [9,11]. The pathophysiology of PBA is complex and not fully understood; however, the available evidence suggests the involvement of cortico–ponto–cerebellar networks that appear to be responsible for the modulation and regulation of emotional responses [10,11].
Little is known about the exact prevalence of PBA in patients with MS, with reported figures showing a wide variability. Outbursts of crying seem to occur more frequently than laughing episodes and patients’ awareness is typically spared [7,12]. PBA might be more commonly associated with advanced stages of the chronic progressive form of MS, and appears to be linked with severe disability [12]. It does not seem to have any correlation with MS relapses [12]; however, there might be a connection between PBA and cognitive impairment, particularly deficits in processing speed, visuospatial memory, verbal learning, and fluency [7,13]. The emotional incontinence that characterizes PBA is often perceived as ego-dystonic by the patient and can cause significant social embarrassment, as well as frustrated urges to voluntarily control it [12].
Despite its impact on the lives of both patients and their caregivers, PBA is often underdiagnosed, partially because it can be easily confused with other psychiatric and neurological conditions [11,14]. The resources currently available for the diagnosis are clinical criteria that evaluate the main characteristics of this condition (Poeck’s criteria) [15] and psychometric instruments. Poeck’s criteria for PBA include emotional response inappropriate to the situation, incongruence of emotions and affective response, inability to control the duration and severity of the episode, and emotional expression not leading to a feeling of relief for the patient. A similar set of criteria was proposed by Cummings et al., who emphasized the fact that PBA is a change from the individual’s normal emotional responses [8]. These clinical criteria are not specific to patients with MS and might therefore fail to capture clinical aspects that are intrinsic to this patient population. The psychometric instruments most commonly used to assess PBA are the Center for Neurologic Study Lability Scale (CNS-LS), a self-report questionnaire consisting of seven questions divided into two sections, one focusing on laughter and the other on labile tearfulness [16], and the Pathological Laughter and Crying Scale (PLACS), an interviewer-rated instrument comprising 16 items graded from zero (seldom or never) to three (often) [17].
The differential diagnosis between PBA and other affective disorders, such as depression or mania, is often challenging. From a clinical perspective, the fact that the emotional outbursts are ego-dystonic and cause significant distress to the patient, who feels unable to control it, can prove useful in the differential diagnosis with bipolar affective disorder [12]. Reaching the correct diagnosis in a timely manner would be crucial, as PBA typically responds to pharmacotherapy, alongside psychoeducation and psychological support [9]. We set out to conduct a systematic literature review in order to determine the prevalence and clinical characteristics of PBA in patients with MS across the lifespan.
2. Materials and Methods
2.1. Eligibility Criteria
The protocol of this systematic literature review was registered with PROSPERO, the international prospective register of systematic reviews (Registration ID CRD42024518201), outlining rationale, aims, search strategy, and data synthesis plans. The review conformed to the guidelines described in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement [18,19]. Studies were included for review if they met the following eligibility criteria with regard to participants: We included studies of PBA in patients of all ages with a diagnosis of MS (no restrictions on time since onset of PBA). We excluded studies on PBA due to any neurological disorder other than MS (traumatic brain injury, stroke, amyotrophic lateral sclerosis, Alzheimer’s disease, Parkinson’s disease, thyroid pathologies, and other conditions) by using Boolean operators and reviewing the full texts of potentially eligible articles. As for publication type and study design, we included original quantitative studies on PBA in MS conducted according to cross-sectional, observational, cohort, and case–control protocols. We did not set any limits in terms of context. Studies across different settings such as hospital, residential nursing home, supported living, and independent living in the community were included. We excluded qualitative studies, reviews, and unpublished “grey” literature. Studies published in languages other than English were also excluded.
2.2. Search Strategy
Comprehensive systematic searches of MEDLINE and PsycINFO databases were completed for this review. As for the search strategy, Boolean operators (AND, OR) were used to restrict the searches to studies focusing on PBA in patients with MS: “MS” OR “multiple sclerosis” AND “emotionalism” OR “emotional lability” OR “emotional dysregulation” OR “involuntary emotional expression disorder” OR “involuntary crying” OR “involuntary laughing” OR “pathological laughing” OR “pathological crying” OR “pseudobulbar affect” OR “emotional incontinence” OR “inappropriate laughing” OR “inappropriate crying”. Keywords and Medical Subject Headings (MeSH) [20] were also used when completing the search strategy.
2.3. Article Selection Process
Once the searches were completed, titles and abstracts were screened according to eligibility criteria. If a decision for eligibility was not able to be made at the title and abstract screening stage due to insufficient information, the full article was reviewed. Following this, the full texts of identified studies were further screened with reasons for exclusion noted. Reference lists of studies were hand-searched to check if any potential studies were not captured by the search strategy. A data extraction template was designed to include a descriptive summary of the studies included in this review [21]. Extracted data for the included studies were as follows: authors, year, country, setting, study design, size of the clinical sample (with age and gender distribution), diagnostic approach to MS and measures of PBA used, prevalence of PBA, independent variables/predictors/correlates of PBA, and other study findings in relation to the review question. Two researchers (S.C. and A.E.C.) were involved in the data extraction process and any discrepancies were resolved through open discussion between the researchers. These included study relevance for inclusion in the present review, methodological quality of the reviewed studies, and heterogeneity in the reporting of clinical data. The final search was conducted on 28 February 2024; therefore, only research published up to this point was included in the review.
2.4. Assessment of Methodological Quality and Risk of Bias
Due to the significant heterogeneity in how PBA was measured and the relatively small sample sizes of the reviewed studies, a narrative synthesis was completed rather than a meta-analysis. The systematic review followed the narrative synthesis framework of Popay et al. [22] to describe the prevalence, clinical characteristics, and predictors of PBA in MS. The narrative synthesis adopted a textual approach to summarize and explain the findings of the reviewed studies, explore relationships in the data, and assess the robustness of the synthesis.
The Quality Assessment Tool for Observational Cohort and Cross-sectional Studies (QATOCCS) was used to rate the methodological quality of the reviewed studies [23]. According to this tool, the following features were examined: researcher bias, sample bias, sample size, time effects, accuracy and reliability of outcome measures, drop-out rates, and whether confounding variables were accounted for. The QATOCCS consists of 14 questions, with each element rated using “yes”, “no”, “cannot determine”, “not reported” or “not applicable”. Based on the ratings for individual items, the reviewed studies were critically appraised to provide an overall rating of “good” (if at least 10 items were rated as “yes”—or 9 with additional reasons such as “not applicable”), “fair” (at least 7 items rated “yes”, but falling short of meeting the criteria for a “good” rating), or “poor” (fewer than 7 items rated “yes”). Finally, the reviewed studies were graded according to the level of evidence using the Scottish Intercollegiate Guidelines Network (SIGN) system [24]. This tool assigns scores based on the quality of evidence, with grades ranging from 1++ (for high quality meta-analyses, with a very low risk of bias) to 4 (for expert opinion and formal consensus).
3. Results
3.1. Characteristics of the Reviewed Studies
Initial searches of the scientific databases yielded 2904 results, with a total of 1547 studies once duplicates were removed. The titles and abstracts of the studies from the search results were assessed for eligibility and studies were excluded if they did not meet the review criteria (1452 studies). A total of 95 studies were reviewed in full-text and reasons for exclusion at this stage were recorded. Following eligibility checking, 16 studies were regarded as eligible for review. The PRISMA flowchart displaying the selection process of the reviewed studies is shown in Figure 1.
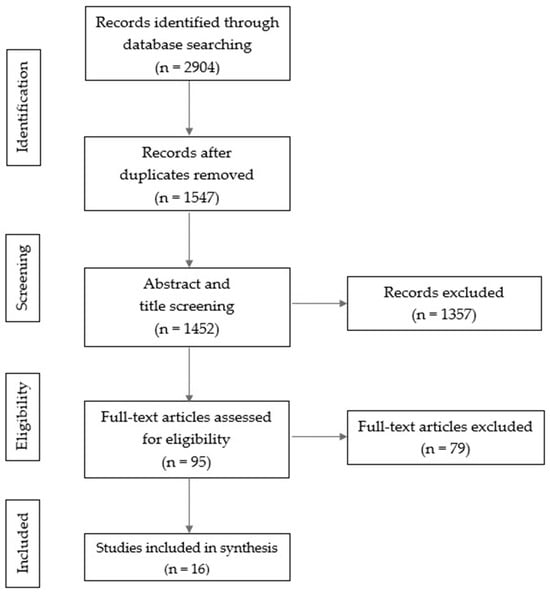
Figure 1.
PRISMA flow diagram illustrating the study selection process.
Seven of the reviewed studies had a cross-sectional design [25,26,27,28,29,30,31], and four a case–control design [32,33,34,35]. We also included in our review two retrospective studies [36,37], two case reports [38,39], and one double-blind, placebo-controlled study [40], which presented relevant data. A summary of the methodological aspects of the reviewed studies is provided in Table 1, whereas the main findings are presented in Table 2.

Table 1.
Summary of the reviewed studies on pseudobulbar affect in patients with multiple sclerosis—methodological aspects.
Table 2.
Summary of the reviewed studies on pseudobulbar affect in patients with multiple sclerosis—main findings.
According to QATOCCS scores, the methodological quality of the reviewed studies was rated as “good” in five studies [25,30,33,35,40], “fair” in nine studies [26,27,28,29,31,32,34,36,37], and “poor” in two studies [38,39]. PBA was assessed using the CNS-LS in 11 of the reviewed studies [25,26,27,28,29,30,31,35,36,37,40]. Poeck’s criteria were used in four studies [32,33,34,39]. Three studies [26,32,33] used the PLACS. Finally, PBA was diagnosed according to the clinical assessment, without using standardized measures, in a single study [38].
3.2. Prevalence of Pseudobulbar Affect
The prevalence of PBA in patients with MS was estimated in eight studies [26,27,28,29,30,32,33,36] that used different assessment methods and cut-offs, resulting in a wide range of figures, from 2% (cut-off: CNS-LS > 21) to 47% (cut-off: CNS-LS > 13). A large cross-sectional study by Fitzgerald et al. [30] showed how, as the CNS-LS cut-off increased, the prevalence of PBA significantly decreased: 21% with CNS-LS > 13, 7% with CNS-LS > 17, and 2% with CNS-LS > 21. Likewise, a cross-sectional study by Work et al. [26] showed significant variability in the prevalence rates, depending on the use of different methods to diagnose PBA in patients with MS: prevalence figures varied from 46% when CNS-LS > 13 was used, to 10% with PLACS > 13. According to the validation study of the CNS-LS, scores above 17 are associated to a sensitivity of 0.94 and a specificity of 0.83 for the diagnosis of PBA in MS [16]. Therefore, based on the reviewed studies that used more rigorous diagnostic procedures and more stringent cut-offs, it was possible to derive a conservative prevalence figure for PBA in the context of MS ranging between 2% and 10%, with a median of 10% as reported by two large samples reported in three studies [26,32,33]. With regard to gender, nine studies reported a higher prevalence of female patients with MS diagnosed with PBA [25,27,29,30,32,33,34,35,40]. In five of the remaining studies, gender was not specified [26,28,31,36,37], whereas the two case reports described one male patient [38] and one female patient [39], respectively.
3.3. Clinical Correlates of Pseudobulbar Affect
3.3.1. Cognitive and Affective Symptoms
A mix of laughing and/or crying was reported in all the studies with the exception of the two single case reports of a male with pathological laughing [38] and a female with pathological crying [39]. Four studies [30,31,36,37] found a correlation between diagnosis of PBA and lower educational level of patients with MS. An association between PBA and cognitive impairment was found in five studies [25,30,32,33,36], while patients with severe cognitive impairment were excluded from three studies [29,35,37]. As for co-morbid psychiatric disorders, relevant clinical data were available from seven studies reporting affective symptoms or depression [27,30,31,32,33,36,37] (patients with psychiatric co-morbidities were excluded from two studies [35,40]). Co-morbid anxiety was reported in three studies [31,32,36]. The study by Özer et al. [31] documented worse anxiety and depression in patients with PBA.
3.3.2. Quality of Life and Disability
Moreover, Brooks et al. [28] found a direct correlation between use of psychotropic medication and CNS-LS scores, as well as an association between the presence of PBA and poorer quality of life. Likewise, Colamonico et al. [27] found higher levels of distress, absenteeism, and reduced work efficiency in patients with PBA and their caregivers. Two studies [32,36] assessed the level of disability using the Expanded Disability Status Scale (EDSS), finding higher scores in patients with PBA.
3.4. Pathophysiology of Pseudobulbar Affect
3.4.1. Clinical Course
The studies that assessed the relationship between PBA and the course of MS found conflicting results: in the study by Feinstein at al. [33], 91% of patients with PBA had chronic progressive MS, whereas in the study by Hanna et al. [36], 74% of patients were affected by relapsing-remitting MS.
3.4.2. Structural Neuroimaging
The phenomenology of PBA in patients with MS was found to be similar to that reported by patients with PBA in the context of other neurological conditions, suggesting that the clinical manifestations are influenced by the anatomical location of the brain lesions [28]. Specifically, these lesions disrupt cortico–ponto–cerebellar networks responsible for regulating emotional expression. Ghaffar et al. [34] observed significantly higher brainstem hypointense lesion volume in individuals with PBA, along with differences in hyperintense lesion volume in five regions (left medial inferior frontal, left inferior parietal, right medial superior frontal, right medial inferior frontal, and right inferior parietal). According to a logistic regression model explaining 70% of the variance, brainstem hypointense, left inferior parietal hyperintense and left and right medial inferior frontal hyperintense lesion volumes predicted the development of PBA. Luhoway et al. [37] also assessed lesion volume and location in patients with MS and found that PBA was associated with fewer posterior lesions.
3.4.3. Functional Neuroimaging
Patterns of brain activations in response to emotional and neutral stimuli were investigated in patients with PBA in the context of MS. Haiman et al. [25] detected increased activity in somatosensory and motor areas in response to neutral stimuli, suggesting greater emotional reactivity to neutral stimuli in specific brain areas among individuals with PBA compared to those without PBA. A further study by the same group found specific activations in areas involved in emotional processing and visual processing in response to neutral stimuli [35].
3.5. Treatment of Pseudobulbar Affect
Three studies [35,39,40] addressed the treatment of PBA, with focus on pharmacotherapy. In the absence of evidence-based guidelines to refer to, the studies had an exploratory nature. The possible effects on PBA of disease-modifying treatment for MS was not addressed. A large randomized double-blind placebo-controlled trial by Panitch et al. [40] found a significant reduction in the severity and frequency of PBA episodes, with a decrease in CNS-LS scores, after dextromethorphan/quinidine therapy compared to placebo. Collateral findings included a rapid and sustained pharmacological action and a potential beneficial effect on chronic pain, as well as an overall favorable safety profile. A case–control study by Haiman et al. [35] showed an improvement in cognitive and behavioral performance (with reduction of positive symptoms and disinhibition) after treatment with dextromethorphan/quinidine, with normalization of electrophysiological parameters. Finally, Johnson and Nichols [39] found that treatment with valproic acid resulted in significant improvement in symptoms of PBA in one patient with MS.
4. Discussion
The results of our systematic literature review provided an estimate prevalence figure for PBA in the context of MS ranging between 2% and 10%, based on the studies that used more rigorous diagnostic procedures and more stringent cut-offs. The overall findings are highly variable, as previously reported [11]; however, the median figure of 10% could be extrapolated from the available evidence. The exact prevalence of PBA in MS appears to be difficult to establish due to the implementation of heterogeneous diagnostic protocols across the individual studies. Moreover, the relatively common occurrence of psychiatric co-morbidities (especially affective symptoms or depression) in the clinical samples could introduce potential confounding factors.
The observed correlation between PBA and the female sex suggests a greater susceptibility of women with MS to the development of this pathological condition. Preliminary evidence also indicates that a lower level of education could be a risk factor for the development of PBA and cognitive decline in the context of MS. The correlation between PBA and cognitive impairment of varying degrees indicate that cognitive deficits in MS could serve as both a risk factor for the development of PBA and a direct or indirect consequence of it [7,12]. With regard to psychiatric co-morbidities, the reviewed literature also highlighted a correlation between PBA and affective symptoms or a formal diagnosis of depression. There is a degree of overlap between the two clinical pictures; however, it is important to underline that the clinical manifestations of PBA strongly impact the emotional, psychological, and social aspects of patients’ lives, potentially facilitating the onset or worsening of depression. In general, PBA in the context of MS tends to increase patients’ overall disability, resulting in poorer quality of life, decreased autonomy, and distress for both patients and their caregivers. However, caution is needed in the interpretation of these data, in the light of the well-known challenges in the differential diagnosis between PBA and other neuropsychiatric co-morbidities that can mimic its symptoms.
Our review confirmed the existence of conflicting results about the relationship between PBA and MS course: both the relapsing–remitting course and the chronic progressive course have been reported to be selectively associated with the development of PBA [12]. These data remain difficult to interpret, also in consideration of the fact that a few studies included only patients affected by a particular MS course—there is a clear need for further research addressing the relationship between MS course and PBA.
The results of the reviewed studies shed some light on the pathophysiology of PBA, as lesions in specific brain areas, especially within the brainstem, were consistently found to be more strongly associated with the development of this condition in the context of MS. Of relevance are the results of the studies using magnetic resonance imaging in patients with PBA compared to patients without PBA [34,37]. Previous studies primarily focused on the combined role of the brainstem and the cerebellum, particularly of the cortico–ponto–cerebellar networks [10,11]. Moreover, there is evidence that the presence of PBA results in abnormal and excessive activation of certain brain areas in response to neutral stimuli, particularly areas of the somatosensory cortex and regions involved in emotion processing and visual stimuli, which may explain the incongruous emotional reactions (uncontrollable laughter or crying) typical of PBA [25]. Taken together, these findings suggest that disinhibition of a gate control mechanism for emotional expression might lead to the lower emotional expression threshold of PBA. Finally, it has emerged that the development of PBA is more closely linked to the cerebral localization of the lesions affecting the central nervous system lesions, rather than to the specific type of neurological pathology.
Therapeutic options for PBA have been examined in a limited number of studies, mainly focusing on patients with other neurological disorders. Specifically, there is a lack of evidence about the pharmacotherapy of PBA in patients with MS, and little is known about the possible effects of disease-modifying treatment on PBA in this patient population. In general, serotonergic pharmacotherapy appears to be effective in the treatment of PBA, with dopaminergic pharmacotherapy as a valid alternative in case of contraindications to serotonergic agents [9]. In addition to selective serotonin reuptake inhibitors, other commonly used antidepressants such as duloxetine, venlafaxine, and mirtazapine have been shown to be potentially useful, with rapid improvement in symptoms (often within a few days), further suggesting that PBA and depression are distinct clinical entities [12]. The combination of dextromethorphan and quinidine (to date, the only FDA-approved treatment for PBA) has uncompetitive NMDA receptor antagonist properties resulting in good tolerability, as well as an excellent efficacy profile both in the short and long term, as assessed by disease-specific measures [41,42]. In a double-blind experimental study on dextromethorphan and quinidine therapy with an average observation period of 89 days, patients with MS and PBA reported reduced CNS-LS scores, frequency of symptoms, and pain intensity, as well as improved quality of life and social relationships, compared to the placebo group [40]. A further controlled study with a relatively small sample size (six patients and six controls) found significant electrophysiological changes in brain activity in patients after treatment with dextromethorphan and quinidine [35]. Available alternative options include valproic acid, which proved successful in the treatment of PBA in a patient with MS who had failed to respond to the dextromethorphan/quinidine combination [39].
The reviewed studies varied in both methodological quality and level of evidence. Most studies were conducted on small samples of patients, due to the relatively low prevalence of PBA in MS and/or to difficulties in patient recruitment. In addition to publication bias, selection bias could have affected the recruitment process in clinic-based samples. The studies with the largest sample sizes had access to large patient registries, so that questionnaires were administered remotely [26,28,30]. Confounding factors could have affected the results of the reviewed studies, especially where patients with depression or on antidepressant therapy were not excluded from the clinical samples [30]. Potentially confounding factors related to co-morbid conditions could only be accounted for where relevant clinical data were available (half of the 14 studies in which patients with psychiatric co-morbidities had not been excluded). For example, patients with MS might have other neuropsychiatric disorders prone to the development of PBA, and younger patients might have a known family burden on other conditions that carry a susceptibility towards PBA. Moreover, there was variability in the diagnostic instruments used to diagnose PBA. Most of the reviewed studies (11 out of 16) employed the CNS-LS questionnaire. Despite being the only validated tool for the diagnosis of PBA in patients with MS and being easy to administer, the CNS-LS has a few possible shortcomings: First, it is a self-reported tool that does not incorporate the clinician’s impression. Second, the reviewed studies used different cut-off scores for the diagnosis of PBA: three studies showed that small differences in cut-off scores resulted in significantly different prevalence rates of PBA in MS [26,28,30]. Overall, due to the lack of uniformity in the choice of the diagnostic score, calculating the prevalence of PBA becomes more complex. Third, it has been highlighted that higher CNS-LS scores are associated with a higher prevalence of depression and/or a greater use of psychopharmacology, potential confounding factors for the diagnosis of PBA in patients with MS [28].
The search strategy of our systematic literature review has intrinsic limitations. The study selection process may be subject to publication bias, as studies with significant results are more likely to be published. Additionally, we may have missed out potentially relevant studies published in languages other than English and/or indexed in databases that were not searched. Finally, despite efforts to minimize bias, subjectivity in study selection and data extraction could have affected our results. These limitations underscore the importance of cautious interpretation of our findings and prompt further work using complementary research methodologies.
Based on the results of our systematic literature review, it would be important for clinicians to pay particular attention to the differential diagnosis of emotional dysregulation in the context of MS, considering PBA alongside other affective disorders, and acknowledging potential overlaps in their clinical presentations. Specifically, in the absence of MS-specific screening instruments, patients with MS should be screened for PBA using both validated clinical criteria (e.g., Poeck’s criteria) and self-report psychometric tools (e.g., CNS-LS questionnaire) with conservative cut-offs (e.g., CNS-LS > 17 for clinically significant PBA and CNS-LS > 21 for more severe PBA) in order to improve specificity for a condition that can be easily misdiagnosed. In the absence of evidence-based guidelines and large trials comparing serotonergic agents with other pharmacological options, the treatment of PBA in patients with MS should be tailored on the individual clinical presentation, taking into account disease-related factors and concomitant pharmacotherapy for the underlying condition (Figure 2).
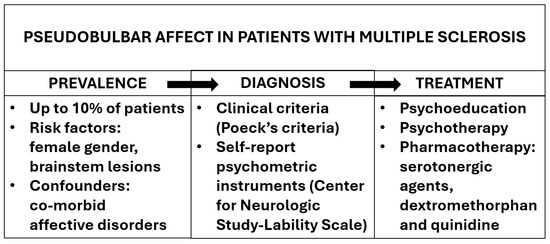
Figure 2.
Conceptual model of the prevalence, diagnosis, and treatment of pseudobulbar affect in patients with multiple sclerosis, based on the findings of the present literature review. The arrows indicate the flow of the thought process, from clinical suspicion to management.
5. Conclusions
According to the results of our systematic literature review, up to one in ten patients with MS can present with PBA. Clinicians should be prompted to consider this condition in the differential diagnosis of emotional disorders in the context of MS by using both clinical criteria and psychometric instruments and to implement treatment strategies as appropriate. Further studies should be conducted on larger and more diverse clinical samples using standardized diagnostic methodologies. Specifically, it would be useful to validate CNS-LS cut-off scores in different patient populations (for both diagnostic and treatment outcome purposes), accounting for the presence of co-morbid depression as a possible confounding factor. Another knowledge gap that needs to be addressed concerns the risk factors for the development of PBA in the context of MS. Inter-individual variables, including lesion localization and use of disease-modifying treatment, should be taken into account when devising future studies. A better understanding of the pathophysiological processes involved would facilitate the implementation of preventive measures and early diagnosis, as well as the development of targeted therapeutic strategies for the clinical management of this disabling condition.
Author Contributions
Conceptualization, A.E.C.; methodology, A.E.C.; formal analysis, S.C. and A.E.C.; data curation, S.C. and A.E.C.; writing—original draft preparation, S.C. and A.E.C.; writing—review and editing, S.C., G.P., A.R., R.N. and A.E.C.; supervision, A.E.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Poser, C.M.; Paty, D.W.; Scheinberg, L.; McDonald, W.I.; Davis, F.A.; Ebers, G.C.; Johnson, K.P.; Sibley, W.A.; Silberberg, D.H.; Tourtellotte, W.W. New diagnostic criteria for multiple sclerosis: Guidelines for research protocols. Ann. Neurol. 1983, 13, 227–231. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Paparrigopoulos, T.; Ferentinos, P.; Kouzoupis, A.; Koutsis, G.; Papadimitriou, G.N. The neuropsychiatry of multiple sclerosis: Focus on disorders of mood, affect and behaviour. Int. Rev. Psychiatry 2010, 22, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Minden, S.L.; Feinstein, A.; Kalb, R.C.; Miller, D.; Mohr, D.C.; Patten, S.B.; Bever, C.; Schiffer, R.B., Jr.; Gronseth, G.S.; Narayanaswami, P. Guideline Development Subcommittee of the American Academy of Neurology. Evidence-based guideline: Assessment and management of psychiatric disorders in individuals with MS: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2014, 82, 174–181. [Google Scholar] [PubMed]
- Raimo, S.; Santangelo, G.; Trojano, L. The emotional disorders associated with multiple sclerosis. Handb. Clin. Neurol. 2021, 183, 197–220. [Google Scholar] [PubMed]
- Murphy, R.; O’Donoghue, S.; Counihan, T.; McDonald, C.; Calabresi, P.A.; Ahmed, M.A.; Kaplin, A.; Hallahan, B. Neuropsychiatric syndromes of multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2017, 88, 697–708. [Google Scholar] [CrossRef] [PubMed]
- Filser, M.; Buchner, A.; Fink, G.R.; Gold, S.M.; Penner, I.K. The manifestation of affective symptoms in multiple sclerosis and discussion of the currently available diagnostic assessment tools. J. Neurol. 2023, 270, 171–207. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.L.; Arciniegas, D.B.; Brooks, B.R.; Herndon, R.M.; Lauterbach, E.C.; Pioro, E.P.; Robinson, R.G.; Scharre, D.W.; Schiffer, R.B.; Weintraub, D. Defining and diagnosing involuntary emotional expression disorder. CNS Spectr. 2006, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wortzel, H.S.; Oster, T.J.; Anderson, C.A.; Arciniegas, D.B. Pathological laughing and crying: Epidemiology, pathophysiology and treatment. CNS Drugs 2008, 22, 531–545. [Google Scholar] [CrossRef]
- Parvizi, J.; Coburn, K.L.; Shillcutt, S.D.; Coffey, C.E.; Lauterbach, E.C.; Mendez, M.F. Neuroanatomy of pathological laughing and crying: A report of the American Neuropsychiatric Association Committee on Research. J. Neuropsychiatry Clin. Neurosci. 2009, 21, 75–87. [Google Scholar] [CrossRef]
- Ahmed, A.; Simmons, Z. Pseudobulbar affect: Prevalence and management. Ther. Clin. Risk Manag. 2013, 9, 483–489. [Google Scholar] [PubMed]
- Iacovides, A.; Andreoulakis, E. Bipolar disorder and resembling special psychopathological manifestations in multiple sclerosis: A review. Curr. Opin. Psychiatry 2011, 24, 336–340. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, S.; Gracey, F.; Trigg, E.; Broomfield, N. Predictors and correlates of emotionalism across acquired and progressive neurological conditions: A systematic review. Neuropsychol. Rehabil. 2023, 33, 945–987. [Google Scholar] [CrossRef] [PubMed]
- Cavanna, A.E.; Ali, F.; Leckman, J.F.; Robertson, M.M. Pathological laughter in Gilles de la Tourette syndrome: An unusual phonic tic. Mov. Disord. 2010, 25, 2233–2239. [Google Scholar] [CrossRef] [PubMed]
- Poeck, K. Handbook of Clinical Neurology; Academic Press: Cambridge, MA, USA, 1969. [Google Scholar]
- Moore, S.R.; Gresham, L.S.; Bromberg, M.B.; Kasarkis, E.J.; Smith, R.A. A self report measure of affective lability. J. Neurol. Neurosurg. Psychiatry 1997, 63, 89–93. [Google Scholar] [CrossRef]
- Robinson, R.G.; Parikh, R.M.; Lipsey, J.R.; Starkstein, S.E.; Price, T.R. Pathological laughing and crying following stroke: Validation of a measurement scale and a double-blind treatment study. Am. J. Psychiatry 1993, 150, 286–293. [Google Scholar] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B.; PRISMA-S Group. PRISMA-S: An extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef] [PubMed]
- Rogers, F.B. Medical subject headings. Bull. Med. Libr. Assoc. 1963, 51, 114–116. [Google Scholar]
- Centre for Reviews and Dissemination. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Healthcare; University of York: York, UK, 2008. [Google Scholar]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews; ESRC Methods Programme: Swindon, UK, 2006. [Google Scholar]
- National Heart, Lung, and Blood Institute. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies; Department of Health and Human Services, National Institutes of Health: Bethesda, MD, USA, 2014.
- Miller, J. The Scottish intercollegiate guidelines network (SIGN). Br. J. Diabetes Vasc. Dis. 2002, 2, 47–49. [Google Scholar] [CrossRef]
- Haiman, G.; Pratt, H.; Miller, A. Brain responses to verbal stimuli among multiple sclerosis patients with pseudobulbar affect. J. Neurol. Sci. 2008, 271, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Work, S.S.; Colamonico, J.A.; Bradley, W.G.; Kaye, R.E. Pseudobulbar affect: An under-recognized and under-treated neurological disorder. Adv. Ther. 2011, 28, 586–601. [Google Scholar] [CrossRef]
- Colamonico, J.; Formella, A.; Bradley, W. Pseudobulbar affect: Burden of illness in the USA. Adv. Ther. 2012, 29, 775–798. [Google Scholar] [CrossRef]
- Brooks, B.R.; Crumpacker, D.; Fellus, J.; Kantor, D.; Kaye, R.E. PRISM: A novel research tool to assess the prevalence of pseudobulbar affect symptoms across neurological conditions. PLoS ONE 2013, 8, 8. [Google Scholar] [CrossRef]
- Vidović, V.; Rovazdi, M.Č.; Kraml, O.; Kes, V.B. Pseudobulbar affect in multiple sclerosis patients. Acta Clin Croat. 2015, 54, 159–163. [Google Scholar]
- Fitzgerald, K.C.; Salter, A.; Tyry, T.; Fox, R.J.; Cutter, G.; Marrie, R.A. Pseudobulbar affect: Prevalence and association with symptoms in multiple sclerosis. Neurol. Clin. Pract. 2018, 8, 472–481. [Google Scholar] [CrossRef]
- Özer, D.; Ata, E.E.; Dikeç, G.; Demir, S. The relationship between stress, anxiety, and depression levels and pseudobulbar affect in patients with multiple sclerosis. Contemp. Nurse 2022, 58, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, A.; Feinstein, K.; Gray, T.; O’Connor, P. Prevalence and neurobehavioral correlates of pathological laughing and crying in multiple sclerosis. Arch. Neurol. 1997, 54, 1116–1121. [Google Scholar] [CrossRef]
- Feinstein, A.; O’Connor, P.; Gray, T.; Feinstein, K. Pathological laughing and crying in multiple sclerosis: A preliminary report suggesting a role for the prefrontal cortex. Mult. Scler. 1999, 5, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Ghaffar, O.; Chamelian, L.; Feinstein, A. Neuroanatomy of pseudobulbar affect: A quantitative MRI study in multiple sclerosis. J. Neurol. 2008, 255, 406–412. [Google Scholar] [CrossRef]
- Haiman, G.; Pratt, H.; Miller, A. Effects of dextromethorphan/quinidine on auditory event-related potentials in multiple sclerosis patients with pseudobulbar affect. J. Clin. Psychopharmacol. 2009, 29, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Hanna, J.; Feinstein, A.; Morrow, S.A. The association of pathological laughing and crying and cognitive impairment in multiple sclerosis. J. Neurol. Sci. 2016, 361, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Luhoway, J.A.; Sharma, M.; Menon, S.; Rosehart, H.; Morrow, S.A. Posterior fossa lesion load and pathological laughing and crying in multiple sclerosis. Int. J. MS Care 2019, 21, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Swamy, M.N.; Johri, S.; Gorthi, S.P.; Dubey, A.K.; Sharma, J.R.; Ramdas, G.V.; Yadav, K.K. Pathological laughter, multiple sclerosis, behavioural abnormality. Med. J. Armed Forces India 2006, 62, 383–384. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Johnson, B.; Nichols, S. Crying and suicidal, but not depressed. Pseudobulbar affect in multiple sclerosis successfully treated with valproic acid: Case report and literature review. Palliat. Support. Care 2015, 13, 1797–1801. [Google Scholar] [CrossRef] [PubMed]
- Panitch, H.S.; Thisted, R.A.; Smith, R.A.; Wynn, D.R.; Wymer, J.P.; Achiron, A.; Vollmer, T.L.; Mandler, R.N.; Dietrich, D.W.; Fletcher, M.; et al. Pseudobulbar Affect in Multiple Sclerosis Study Group. Randomized, controlled trial of dextromethorphan/quinidine for pseudobulbar affect in multiple sclerosis. Ann. Neurol. 2006, 59, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Schoedel, K.A.; Morrow, S.A.; Sellers, E.M. Evaluating the safety and efficacy of dextromethorphan/quinidine in the treatment of pseudobulbar affect. Neuropsychiatr. Dis. Treat. 2014, 10, 1161–1174. [Google Scholar] [CrossRef][Green Version]
- Yang, L.P.H.; Deeks, E.D. Dextromethorphan/quinidine: A review of its use in adults with pseudobulbar affect. Drugs 2015, 75, 83–90. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).