
Digital Biomarkers in the Assessment of Mobility in Individuals with Multiple Sclerosis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
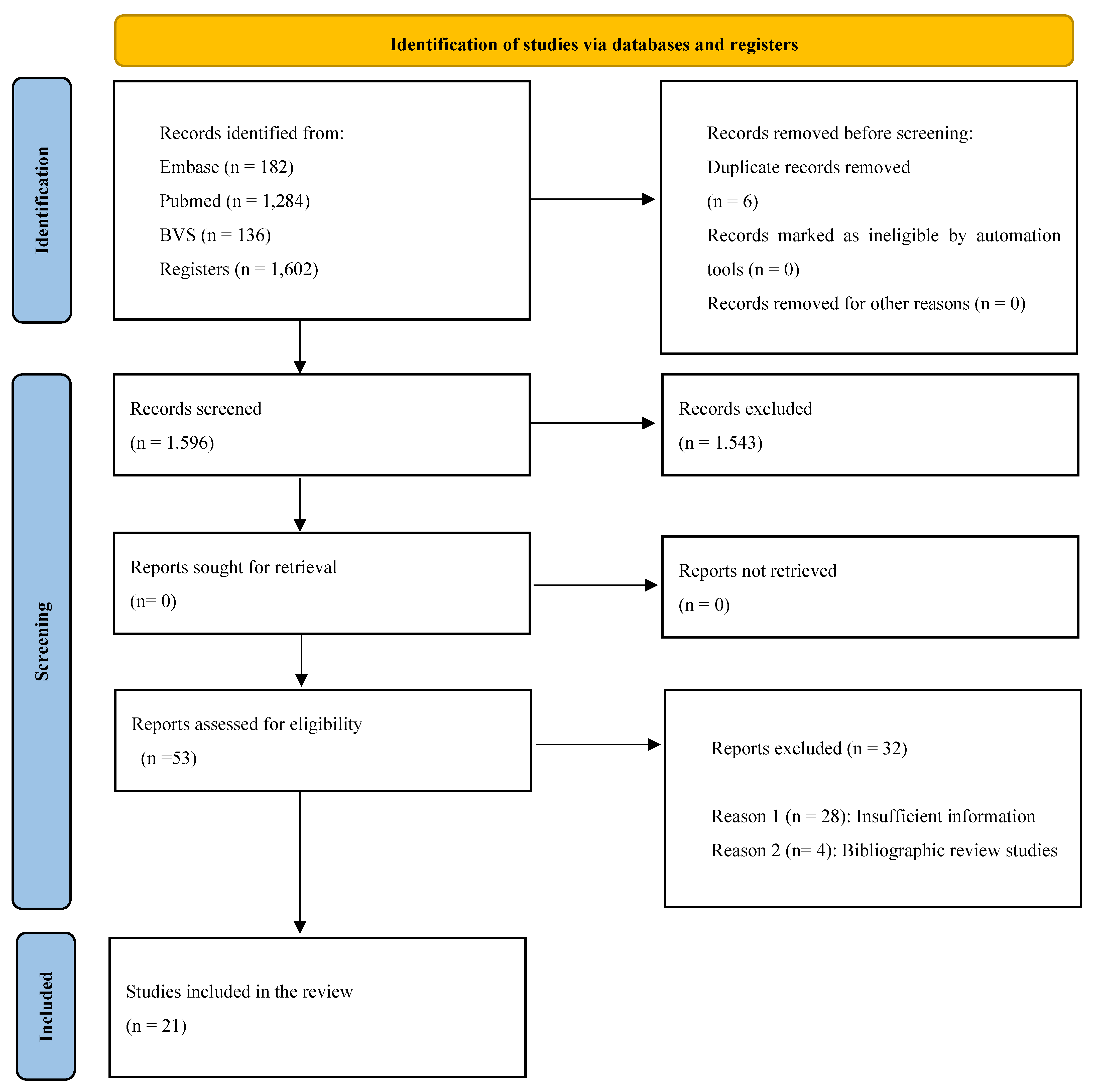
2.3. Article Selection Process
3. Results
3.1. Characteristics of the Studies
3.2. Characteristics of the Instruments Used
3.3. Objective Biomarkers Reference Methods
3.4. Subjective Biomarkers Reference Methods
4. Discussion
Limitations and Future Considerations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- ABEM; Brazilian Multiple Sclerosis Association. What Is Multiple Sclerosis (MS); Brazilian Multiple Sclerosis Association: São Paulo, Brazil, 2023. [Google Scholar]
- Yamout, B.I.; Alroughani, R. Multiple Sclerosis. Semin. Neurol. 2018, 38, 212–225. [Google Scholar] [PubMed]
- WHO (World Health Organization). Multiple Sclerosis; WHO: Geneva, Switzerland, 2023.
- Wallin, M. Global, regional, and national burden of multiple sclerosis 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 269–285. [Google Scholar] [CrossRef] [PubMed]
- MSIF (Multiple Sclerosis International Federation). Atlas of MS, 3rd ed.; Multiple Sclerosis International Federation: London, UK, 2020. [Google Scholar]
- Guerreiro, C.T.; Baptistela, B.L.; Machado, O.A.; Almeida, E.C.D.; Vieira, M.R. Multiple sclerosis and the body structure and function, activity and participation components of the International Classification of Functioning, Disability and Health (ICF) model. Rev. Atenas Higeia 2019, 1, 25–30. [Google Scholar]
- Backus, D. Increasing Physical Activity and Participation in People with Multiple Sclerosis: A Review. Arch. Phys. Med. Rehabil. 2016, 97, S210–S217. [Google Scholar] [CrossRef]
- Franco, R.C.; Curib, H.T.; Andrade, L.F.; Ferretti, E.C. Understanding the difficulties and contextual factors in the daily activities of people with multiple sclerosis: A pilot study. Cad. Bras. Ter. Ocup. 2022, 30, e2942. [Google Scholar] [CrossRef]
- Maggio, M.G.; Russo, M.; Cuzzola, M.F.; Destro, M.; Rosa, G.L.; Molonia, F.; Bramanti, P.; Lombardo, G.; De Luca, R.; Calabrò, R.S. Virtual reality in multiple sclerosis rehabilitation: A review of cognitive and motor outcomes. J. Clin. Neurosci. 2019, 65, 106–111. [Google Scholar] [CrossRef]
- Woelfle, T.; Bourhuignon, L.; Lorscheider, J.; Kappos, L.; Naegelin, Y.; Jutzeler, C.R. Wearable Sensor Technologies to Assess Motor Functions in People with Multiple Sclerosis: Systematic Scoping Review and Perspective. J. Med. Internet Res. 2023, 25, e44428. [Google Scholar] [CrossRef]
- Neto, F.S.S.; Jesuíno, A.D.S.A.; Amorim, D.N.P.; Silva, M.A. Aplicativos móveis para estimulação cognitiva de idosos em processo demencial: Uma revisão sistemática. Res. Soc. Dev. 2023, 12, e19212441086. [Google Scholar] [CrossRef]
- Sasaki, J.; Coutinho, A.; Santos, C.; Bertuol, C.; Minatto, G.; Berria, J.; Tonosaki, L.; Lima, L.; Marchesan, M.; Silveira, P.; et al. Orientações para utilização de acelerômetros no Brasil. Rev. Bras. Atividade Física Saúde 2017, 22, 110–126. [Google Scholar] [CrossRef]
- Dillenseger, A.; Weidemann, M.L.; Trentzsch, K.; Inojosa, H.; Haase, R.; Schriefer, D.; Voigt, I.; Scholz, M.; Akgun, K.; Ziemssen, T. Digital Biomarkers in Multiple Sclerosis. Brain Sci. 2021, 11, 1519. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Schamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Souza, M.T.; Silva, M.D.; Carvalho, R. Revisão integrativa: O que é e como fazer. Einstein 2010, 8, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Meyer, B.M.; Cohen, J.G.; Donahue, N.; Fox, S.R.; O’Leary, A.; Brown, A.J.; Leahy, C.; VanDyk, T.; DePetrillo, P.; Ceruolo, M.; et al. Chest-Based Wearables and Individualized Distributions for Assessing Postural Sway in Persons with Multiple Sclerosis. IEEE Trans. Neural Syst. Rehabil. Eng. 2023, 31, 2132–2139. [Google Scholar] [CrossRef]
- Micó-Amigo, M.E.; Bonci, T.; Paraschiv-Ionescu, A.; Ullrich, M.; Kirk, C.; Soltani, A.; Kuderle, A.; Gazit, E.; Salis, F.; Alcock, L.; et al. Assessing real-world gait with digital technology? Validation, insights and recommendations from the Mobilise-D consortium. J. NeuroEng. Rehabil. 2023, 20, 78. [Google Scholar] [CrossRef] [PubMed]
- Tulipani, L.J.; Meyer, B.; Allen, D.; Solomon, A.J.; McGinnis, R.S. Evaluation of the unsupervised performance of the 30-second chair standing test assessed by portable sensors to predict fall status in multiple sclerosis. Gait Posture 2022, 94, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Tulipani, L.J.; Meyer, B.; Fox, S.; Solomon, A.J.; McGinnis, R. The Sit-to-Stand Transition as a Biomarker for Impairment: Comparison of Instrumented 30-Second Chair Stand Test and Daily Life Transitions in Multiple Sclerosis. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 1213–1222. [Google Scholar] [CrossRef]
- Woelfle, T.; Pless, S.; Wiencierz, A.; Kappos, L.; Naegelin, Y.; Lorscheider, J. Practice Effects of Mobile Tests of Cognition, Dexterity, and Mobility on Patients with Multiple Sclerosis: Data Analysis of a Smartphone-Based Observational Study. J. Med. Internet Res. 2021, 23, e30394. [Google Scholar] [CrossRef]
- Atrsaei, A.; Dadashi, F.; Mariani, B.; Gonzenbach, R.; Aminian, K. Toward a remote assessment of walking bout and speed: Application in patients with multiple sclerosis. IEEE J. Biomed. Health Inform. 2021, 25, 217–4228. [Google Scholar] [CrossRef]
- Mosquera-Lopez, C.; Wan, E.; Shastry, M.; Folsom, J.; Leitschuh, J.; Condon, J. Automated Detection of Real-World Falls: Modeled from People with Multiple Sclerosis. IEEE J. Biomed. Health Inform. 2021, 25, 1975–1984. [Google Scholar] [CrossRef]
- Cheng, W.; Bourkr, A.K.; Lipsmeier, F.; Bernasconi, C.; Belachew, S.; Gossens, C.; Graves, J.S.; Montalban, X.; Lindemann, M. U-turn speed is a valid and reliable smartphone-based measure of multiple sclerosis-related gait and balance impairment. Gait Posture 2021, 84, 120–126. [Google Scholar] [CrossRef]
- Tulipani, L.J.; Meyer, B.; Larie, D.; Solomon, A.J.; McGinnis, R.S. Metrics extracted from a single wearable sensor during sit-stand transitions relate to mobility impairment and fall risk in people with multiple sclerosis. Gait Posture 2020, 80, 361–366. [Google Scholar] [CrossRef]
- Pau, M.; Porta, M.; Coghe, G.; Frau, J.; Lorefice, L.; Cocco, E. Does Multiple Sclerosis Differently Impact Physical Activity in Women and Man? A Quantitative Study Based on Wearable Accelerometers. Int. J. Environ. Res. Public Health 2020, 17, 8848. [Google Scholar] [CrossRef] [PubMed]
- Shema-Shiratzky, S.; Hillel, I.; Mirelman, A.; Regev, K.; Hsieh, K.L.; Karni, A.; Devos, H.; Sosnoff, J.J.; Hausdorff, J.M. A wearable sensor identifies changes in community walking in multiple sclerosis: Con-tributors to real-world gait quality and physical activity. J. Neurol. 2020, 267, 1912–1921. [Google Scholar] [CrossRef]
- Shema-Shiratzky, S.; Gazit, E.; Sun, R.; Regev, K.; Karni, A.; Sosnoff, J.J.; Herman, T.; Mirelman, A.; Hausdorff, J.M. Deterioration of specific aspects of gait during the instrumented 6-minute walk test among people with multiple sclerosis. J. Neurol. 2019, 266, 3022–3030. [Google Scholar] [CrossRef] [PubMed]
- Midaglia, L.; Mulero, P.; Montalban, X.; Graves, J.; Hauser, S.L.; Julian, L.; Baker, M.; Schadrack, J.; Gossens, C.; Scotland, A.; et al. Adherence and Satisfaction of Smartphone- and Smartwatch-Based Remote Active Testing and Passive Monitoring in People with Multiple Sclerosis: Nonrandomized Interventional Feasibility Study. J. Med. Internet Res. 2019, 21, e14863. [Google Scholar] [CrossRef]
- Flachenecker, F.; Gabner, H.; Hannik, J.; Lee, D.; Flachenecker, P.; Winkler, J.; Eskofier, B.; Linker, R.A.; Klucken, J. Objective sensor-based gait measures reflect motor impairment in multiple sclerosis patients: Reliability and clinical validation of a wearable sensor device. Mult. Scler. Relat. Disord. 2019, 39, 101903. [Google Scholar] [CrossRef] [PubMed]
- Chitnis, T.; Glanz, B.I.; Gonzalez, C.; Healy, B.C.; Saraceno, T.J.; Sattarnezhad, N.; Diaz-Cruz, C.; Polgar-Turcsanyi, M.; Tummala, S.; Baksh, R.; et al. Quantifying neurologic disease using biosensor measurements in-clinic and in free-living settings in multiple sclerosis. NPJ Digit. Med. 2019, 2, 123. [Google Scholar] [CrossRef]
- DasMahapatra, P.; Chiauzzi, E.; Bhalerao, R.; Rhodes, J. Free-Living Physical Activity Monitoring in Adult US Patients with Multiple Sclerosis Using a Consumer Wearable Device. Digit. Biomark. 2018, 2, 47–63. [Google Scholar] [CrossRef]
- Psarakis, M.; Greene, D.A.; Cole, M.H.; Lord, S.R.; Hoang, P.; Brodie, M. Wearable technology reveals gait compensations, unstable walking patterns and fatigue in people with multiple sclerosis. Physiol. Meas. 2018, 39, 075004. [Google Scholar] [CrossRef]
- Moon, Y.; McGinnis, R.S.; Seargers, K.; Motl, R.W.; Sheth, N.; Wright, J.A., Jr.; Ghaffari, R.; Sosnoff, J.J. Monitoring gait in multiple sclerosis with novel wearable motion sensors. PLoS ONE 2017, 12, e0171346. [Google Scholar] [CrossRef] [PubMed]
- Sebastião, E.; Learmonth, Y.C.; Motl, R.W. Mobility measures differentiate falls risk status in people with multiple sclerosis: An exploratory study. NeuroRehabilitation 2017, 40, 153–161. [Google Scholar] [CrossRef]
- Spain, R.I.; Mancini, M.; Horak, F.B.; Boudette, D. Body-worn sensors capture variability, but not decline, of gait and balance measures in multiple sclerosis over 18 months. Gait Posture 2014, 39, 958–964. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; Sandroff, B.M.; Sosnoff, J.J. Accelerometry as a measure of walking behavior in multiple sclerosis. Acta Neurol. Scand. 2013, 127, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, J.E.; da Silva, K.S.; da Costa, B.G.G.; John, D. Measuring physical activity using accelerometers. In Computer-Assisted and Web-Based Innovations in Psychology, Special Education, and Health; Elsevier Inc.: Amsterdam, The Netherlands, 2016. [Google Scholar] [CrossRef]
- Skender, S.; Ose, J.; Chang-Claude, J.; Paskow, M.; Bruhmann, B.; Siegel, E.M.; Steindorf, K.; Ulrich, C.M. Accelerometry and physical activity questionnaires—A systematic review. BMC Public Health 2016, 16, 515. [Google Scholar] [CrossRef]
- Arvidsson, D.; Fridolfsson, J.; Borjesson, M. Measurement of physical activity in clinical practice using accelerometers. J. Intern. Med. 2019, 286, 137–153. [Google Scholar] [CrossRef] [PubMed]
- Khalil, H.; Al-Shorman, A.; El-Salem, K.; Abdo, N.; Alghwiri, A.A.; Aburub, A.; Shalabi, S.; Al-Mustafa, F. Fear of falling in people with multiple sclerosis: Which clinical characteristics are important? Phys. Ther. 2017, 97, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Brønd, C.; Arvidsson, D. Sampling frequency affects ActiGraph accelerometry raw data processing for activity counts. J. Appl. Physiol. 2016, 120, 362–369. [Google Scholar] [CrossRef]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer data collection and processing criteria for assessing physical activity and other outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Akenhead, R.; French, D.; Thompson, K.G.; Hayes, P.R. The acceleration-dependent validity and reliability of the 10 Hz GPS. J. Sci. Med. Sport 2014, 17, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Carmona, C.D. What is the most appropriate sampling frequency to record workload based on accelerometry? A case study in soccer. Proc. Inst. Mech. Eng. Part P J. Sports Eng. Technol. 2021, 235, 114–121. [Google Scholar] [CrossRef]
- Khan, A.; Hammerla, N.; Mellor, S.; Plotz, T. Optimization of sampling rates for accelerometer-based human activity recognition. Pattern Recognit. Lett. 2016, 73, 33–40. [Google Scholar] [CrossRef]
- Ader, L.G.M.; Greene, B.R.; McManus, K.; Tubridy, N.; Caulfield, B. Short sessions of gait data and body-worn inertial sensors can provide reliable measures of spatio-temporal gait parameters from bilateral gait data for people with multiple sclerosis. Biosensors 2020, 10, 128. [Google Scholar] [CrossRef]

{kind=link}
| Title | Objectives | Sample | Digital Biomarkers | Results |
|---|---|---|---|---|
| Chest-Based Wearables and Individualized Distributions for Assessing Postural Sway in Persons with Multiple Sclerosis [16] | To validate postural sway measurements from a chest accelerometer. | 16 people (4 M, 12 F, mean ± standard deviation age 50.6 ± 10.5 years) with multiple sclerosis. | Wearable accelerometer on the chest and sacrum using BioStamp nPoint ® sensors (Medidata) to capture movement patterns and postural sway, and frequency and intensity of falls, fatigue, rhythm and balance. | Chest sway measurements can differentiate between standing and falling tasks and are significantly related to patient-reported measures of balance confidence, fatigue and walking difficulty. |
| Assessing real-world gait with digital technology? Validation, insights and recommendations from the Mobilise-D consortium [17] | To evaluate digital mobility in six cohorts via gait data for gait sequencing. | 60 participants, distributed in different groups. 20 were healthy elderly, 20 had Parkinson’s disease and another 20 had multiple sclerosis. | McRoberts Dynaport MM+ wearable device (100 Hz sampling frequency; triaxial acceleration range: ±8 g, resolution: 1 mg; triaxial gyroscope range: ±2000 degrees per second (dps), resolution: 70 mdps), attached to the back and used in tests, such as the 6 Minute Walk, to capture movement patterns, gait index, cadence (count of steps per minute), rhythm and balance. | The choice of algorithm for estimating gait sequence detection and cadence should be cohort-specific (e.g., slow walkers and those with gait impairments). The short walking distance and slow walking speed worsened the performance of the algorithms. |
| Evaluation of unsupervised 30-s chair stand test performance assessed by wearable sensors to predict fall status in multiple sclerosis [18] | To evaluate the unsupervised 30-Second Chair Stand Test (30CST) in multiple sclerosis via accelerometer and compare it with the supervised 30CST. | 37 people with multiple sclerosis. | MC10 BioStamp triaxial accelerometer (250 Hz, ±16 G) recorded from ten inertial sensors (MC10, Inc., Lexington, MA, USA) adhered to the skin and smartphone with MC10 Link App to capture the sit-to-stand and stand-to-sit transition time, with the aim of detecting the risk of falls and standing time. | Individuals with a history of falls (Group F) (n = 21) and those with no history of falls (Group NF) (n = 16) showed statistically significant differences in age and 30CST performance (p = 0.013, d = 0.88). |
| The Sit-to-Stand Transition as a Biomarker for Impairment: Comparison of Instrumented 30-Second Chair Stand Test and Daily Life Transitions in multiple sclerosis [19] | To compare measurements from wearable sensors and the supervised/unsupervised 30-Second Chair Stand Test (30CST) to understand fall risk, sensory and pyramidal impairment. | 37 people with multiple sclerosis. | Two inertial sensors (MC10, Inc., Lexington, MA, USA), one on the right thigh and one on the chest, which recorded data from the MC10 BioStamp triaxial accelerometer (250 Hz sampling rate, ±16 G) and smartphone with MC10 Link App sensors to capture sit–stand and stand–sit transition time to detect falls risk and standing time. | Best fall risk discrimination: Chest acceleration of the supervised 30CST (Area under the curve (AUC) = 0.89)). Chest indicated sensory impairment, but different task in daily life. Discrimination of pyramidal impairment: chest acceleration in the supervised 30CST (AUC = 0.89). Highest AUC daily life: mean sit-to-lift time in fall classification (0.81). |
| Practice Effects of Mobile Tests of Cognition, Dexterity, and Mobility on Patients with Multiple Sclerosis: Data Analysis of a Smartphone-Based Observational Study [20] | To examine the effects of short-term learning and long-term practice on six active tests of cognition, agility and mobility in a user-scheduled high-frequency smartphone test. | 264 people with multiple sclerosis. | Data from the Floodlight Open app, which collects data from smartphone-based tests of people with multiple sclerosis, such as the 2-Minute Walk, Half Lap and Static Balance tests, to capture gait speed, gait reversal and static balance. | In the Half Lap (n = 15,051) and Static Balance (n = 16,797), only short-term learning effects were observed, which were interrupted after a maximum of 5 attempts. No short-term or long-term learning effects were observed in the 2-Minute Walk (n = 14,393). |
| Toward a Remote Assessment of Walking Bout and Speed: Application in Patients with Multiple Sclerosis [21] | To develop and validate a new gait speed estimation method based on machine learning to predict gait speed in clinical and home assessments using a sensor in the lumbar region. | 35 people with multiple sclerosis. | Three Physilog 5® inertial measurement units (IMU) (Physilog, Gait Up, Lausanne, Switzerland), one on the waist and two on the feet, i.e., one on each foot, with three axes, which included 3D accelerometer and gyroscope data recorded at a sampling rate of 128 Hz and smartphone to connect to the IMUs, used in the 10-Meter Walk Test to capture gait speed. | Compared to the silver standard multisensory reference, a bias close to zero and a gait speed accuracy of 0.15 m/s were achieved. In addition, the proposed machine learning-based gait detection method had a median specificity of 96.8%, sensitivity of 93.0%, an accuracy of 96.4% and an F1 score (2 × true positive/2 × true positive + false positive + false negative) of 78.6% in detecting walking at home. |
| Automated Detection of Real-World Falls: Modeled from People with Multiple Sclerosis [22] | To describe the development of a context-sensitive fall detection system based on an inertial sensor and an imbalance-tolerant time-of-flight sensor that trains and evaluates real falls in patients with multiple sclerosis. | 25 people with multiple sclerosis. | Body-worn triaxial accelerometer and a context-sensitive motion monitoring system that uses indoor wireless time-of-flight (ToF) beacons positioned around a house to track a person’s movement and detect the risk of falls. | In a dataset obtained from 25 people with multiple sclerosis observed for 8 weeks in a free-living environment, 54 falls were observed and the system achieved a sensitivity of 92.14% and a false positive rate of 0.65 per day. |
| U-turn speed is a valid and reliable smartphone-based measure of multiple sclerosis-related gait and balance impairment [23] | To assess the feasibility of remote patient monitoring using digital technology in people with multiple sclerosis. | 76 people with multiple sclerosis and 25 healthy controls. | Samsung Galaxy S7 smartphone (triaxial accelerometer and gyroscope sensors with a sample rate of 50 Hz) used to carry out tests, such as the Timed 25-Foot Walk (T25FW) and the 5 U-Turn Test (5UTT) to capture turning speed. | The minimum detectable change in the 5UTT return rate was low in multiple sclerosis patients (19.42%), and the accuracy of this measurement tool compared to existing measures of walking performance in the clinic was excellent. |
| Metrics extracted from a single wearable sensor during sit-stand transitions relate to mobility impairment and fall risk in people with multiple sclerosis [24] | Obtain accelerometer-based metrics from a minimum number of sensors to characterize sitting and standing performance in people with multiple sclerosis during the 30-s chair stand test (30CST). | 38 people with multiple sclerosis with an average age of 50.6 ± 12.1. | MC10 BioStamp triaxial accelerometer (250 Hz sampling rate, ±16 G) recorded from inertial sensors ( MC10, Inc., Lexington, MA, USA) adhered to the skin in the region of the right thigh and chest used to perform tests, such as the 30CST Test, to capture balance and fatigue confidence, sit–stand transition time and stand–sit transition time to detect the risk of falls. | Acceleration-based scores were significantly correlated with several clinical indicators reflecting disease severity, balance confidence and fatigue. Logistic regression performed better for classifying fall conditions incorporating accelerometer features (74% accuracy, (Area Under the Curve (AUC) = 0.78)) compared to standard treatment (68% accuracy, AUC = 0.74) or patient-reported outcomes (71% accuracy, AUC = 0.75). |
| Does Multiple Sclerosis Differently Impact Physical Activity in Women and Man? A Quantitative Study Based on Wearable Accelerometers [25] | To investigate possible differences between women and men with multiple sclerosis in the amount and intensity of physical activity performed during a week. | 45 people with multiple sclerosis (23 F, 22 M, average age 50.3) and 41 unaffected individuals of the same age and gender. | ActiGraph model GT3X triaxial accelerometer (Acticorp Co., Pensacola, FL, USA) used 24 h a day for 7 days to detect patterns of physical activity and sedentary behavior, the number of daily steps and vector magnitude count. | Women’s physical activity patterns were characterized by greater sedentary behavior and decreased light activity compared to men, with similar levels of moderate and vigorous physical activity. |
| A wearable sensor identifies alterations in community ambulation in multiple sclerosis: contributors to real-world gait quality and physical activity [26] | To evaluate community walking and physical activity in patients with multiple sclerosis and healthy controls, and to compare laboratory walking with community walking. | 104 subjects, 44 people with multiple sclerosis and 60 healthy controls. | Opal triaxial accelerometer (APDM Wearable Technologies, Portland, OR, USA) worn on the lower back in tests, such as the Timed 25-Foot Walk (T35FW), to detect changes in ambulation due to gait speed and step variability. | During the community walk, people with multiple sclerosis took fewer steps and walked more slowly, with greater asymmetry and greater step variability, compared to healthy controls (p < 0.001). Greater impairment is associated with reduced step count and reduced community walking speed. |
| Deterioration of specific aspects of gait during the instrumented 6 min walk test among people with multiple sclerosis [27] | To identify gait characteristics that worsen during sustained walking and to investigate their clinical correlation with walking fatigue in patients with multiple sclerosis. | 58 people with multiple sclerosis. | Opal triaxial accelerometer (APDM Wearable Technologies Portland, OR, USA) worn on the lower back in tests, such as the 6-Minute Walk (6 MWT), to detect gait pace, rhythm, variability, asymmetry, complexity, fatigue and the risk of falls. | Individuals with moderate impairment (n = 24) walked worse than the group with mild impairment (n = 34) in most gait domains. A group x fatigue interaction effect was observed for gait rhythm and complexity. These rates decreased over time in the moderate impairment group, but not in the mild impairment group. |
| Adherence and Satisfaction of Smartphone- and Smartwatch-Based Remote Active Testing and Passive Monitoring in People with Multiple Sclerosis: Nonrandomized Interventional Feasibility Study [28] | To assess the feasibility of remote active testing and passive monitoring using smartphones and smartwatch technology in people with multiple sclerosis with regard to adherence to and satisfaction with the FloodLight test battery. | People with multiple sclerosis (20 to 57 years; Expanded Disability Status Scale 0–5.5; n = 76) and healthy controls (n = 25). | FloodLight study, which combines continuous sensor data capture with smartphones and smartwatches, used in tests, such as the Timed 25-Foot Walk Test (T25FW), to detect gait speed and turnaround time. | People with multiple sclerosis had 70% (16.68/24 weeks) adherence in the active trials and 79% (18.89/24 weeks) in the passive surveillance. The average satisfaction score was 73.7 out of 100. Neither adherence nor satisfaction were related to any specific characteristics of the population. More than 80% (61/72) of multiple sclerosis patients had at least an acceptable effect on activities of daily living as assessed by the battery of tests. |
| Objective sensor-based gait measures reflect motor impairment in multiple sclerosis patients: Reliability and clinical validation of a wearable sensor device [29] | To investigate whether sensor-based gait analysis can detect gait disturbances in patients with multiple sclerosis. | 102 people with multiple sclerosis and 22 healthy controls. | Triaxial accelerometer and gyroscope, recorded from SHIMMER 3 sensors (Shimmer Research Ltd., Dublin, Ireland), attached to both shoes, when performing tests, such as the 25-Foot Walk Test (25FWT), to detect average stride length, gait speed, toe-off angle, support time and swing time. | Subgroup analysis between healthy controls and people with multiple sclerosis (EDSS ≤ 3.5 and EDSS 4.0–7.0) revealed significant differences in several gait metrics, especially in fast walking speed. For example, the stride length in fast walking was 33.6 cm, while in self-selected walking, it was 16.3 cm. |
| Quantifying neurologic disease using biosensor measurements in-clinic and in free-living settings in multiple sclerosis [30] | To evaluate the feasibility and correlation of wearable biosensors with traditional clinical measures of disability both in the clinic and in free living in patients with multiple sclerosis. | 25 people with multiple sclerosis. | Biosensors to detect support time, angular angle/velocity of turning, average speed of turning, balance, postural sway and mobility posture. | Feasibility, adherence and expansion between biosensors and traditional clinical measures (Expanded Disability Status Scale (EDSS) and MS Functional Composite-4 (MSFC-4)) were evaluated. Biosensor features correlated with EDSS and MSFC-4 scores at visit 2, including mobility stance time (−0.546), turning angle (0.437) and maximum angular velocity (0.653). |
| Free-Living Physical Activity Monitoring in Adult US Patients with Multiple Sclerosis Using a Consumer Wearable Device [31] | To advance the literature on the usefulness of free-living physical activity screening from secondary analyses of a pilot study in patients with multiple sclerosis. | 114 people with multiple sclerosis (mean age 52 years, female (75%), relapsing-remitting type (79%)). | Online network of patients with chronic diseases, PatientLikeMe-FitbitOne, and wearable device, used to detect the number of daily steps and the inability to move. | 23-day study: average of 20.1 days of data (87% adherence), 4393 steps/day. Multiple Sclerosis Rating Scale (MSRS) pre-study mean: 32.72% with gait disturbances. Step count reliability: interclass correlation coefficient (ICC) 0.55 (daily), 0.7 (2 days) 0.9 (7 days). Disease severity (MSRS) was an independent predictor of step count after controlling for covariates (p < 0.001). |
| Wearable technology reveals gait compensations, unstable walking patterns and fatigue in people with multiple sclerosis [32] | To quantify the patterns of head and pelvic movement that occur in Pulse Width Modulation-impaired patients and determine how these secondary gait compensations impact gait stability. | 12 healthy participants and 12 people with multiple sclerosis. | Two Opal triaxial accelerometers (APDM, Wearable Technologies, Portland, OR, USA, 128 Hz sampling frequency), one fixed to the head and the other to the pelvis, used to perform tests, such as the 6-Minute Walk Test (6 MWT), to detect gait variability, mobility index (reduced mobility), risk of falls, gait asymmetry, fatigue and gait compensation measures. | People with multiple sclerosis vs. healthy controls: greater vertical asymmetry in cephalic and pelvic movements (Cohen’s d = 1.85 and 1.60). In patients with multiple sclerosis, increased compensatory movement related to: decreased amplitude of active ankle movement (r = −0.71), greater EDSS (r = 0.58), unstable gait (r = −0.76), decreased range of motion (r = −0.71) and increased volatility (r = 0.83). |
| Monitoring gait in multiple sclerosis with novel wearable motion sensors [33] | To investigate the precision and accuracy of a new wearable device, BioStampRC, as a measure of gait of people with multiple sclerosis with various gait functions. | 45 people with multiple sclerosis (Mild multiple sclerosis = 15, Moderate multiple sclerosis = 15, Severe multiple sclerosis = 15) and 15 healthy control subjects. | BioStampRC wireless Inertial Sensormounted on the skin, MTx (Xsens, Enschede, The Netherlands) on the legs and ActGraph model GT3X triaxial accelerometer (Acticorp Co., Pensacola, FL, USA,) on the hip, used to perform tests, such as the 25-Foot Walk Test (T25FW), 6-Minute Walk Test (6 MWT) and Timed Up and Go (TUG), to detect the number of steps, speed and length of gait. | Average accuracy ± precision for BioStampRC: 2 ± 2 steps error, 6 ± 9 ms error for stride time, 6 ± 7 ms error for step time (0.6–2.6% relative error). Lower accuracy ± precision in swing time (25 ± 19 ms error, 5 ± 4% relative error). GT3X with lower accuracy ± precision (8 ± 14% relative error) in estimating number of steps. MTx and BioStampRC detected significant differences in gait in multiple sclerosis patients of different levels of disability (p < 0.01). |
| Mobility measures differentiate falls risk status in persons with multiple sclerosis: An exploratory study [34] | To examine differences in mobility metrics, postural control and cognition in people with multiple sclerosis with distinct fall risk status; and to investigate predictors of participation in fall risk groups using discriminant analysis. | 47 people with multiple sclerosis. | ActiGraph accelerometer model GT3X (Acticorp Co., Pensacola, FL, USA), used to perform tests, such as the 25-Foot Walk Test (T25FW), 6-Minute Walk Test (6 MWT), Timed Up and Go (TUG), Multiple Sclerosis Walking Scale 12 (MSWS-12) and Six-Spot Step Test (SSST), to detect the number of steps per day and the risk of falls. | The fall risk group showed significantly worse (p < 0.05) mobility measures (MSWS-12, 6 MWT and steps/day) compared to the normal fall risk group. Discriminant analysis of MSWS-12 and 6 MWT as significant predictors (p < 0.05) for the fall risk group, explaining 55% of the variance. |
| Body-worn sensors capture variability, but not decline, of gait and balance measures in multiple sclerosis over 18 months [35] | To determine whether body-worn sensors detected any decline in gait and balance measures in people with multiple sclerosis over time. | 27 people with multiple sclerosis (13 mildly disabled; self-rated Expanded Disability Status Scale 0 to 3.5; 14 moderately disabled; self-rated expanded disability status scale 4.0 to 5.5). | Six body-worn MTx sensors (Xsens, Enschede, The Netherlands), each including a three-dimensional gyroscope and triaxial accelerometer sampling at 50 Hz, used in tests, such as the Timed 25-Foot Walk Test (T25FW), the Multiple Sclerosis Walk Scale 12 (MSWS12) and the Activities of Balance Confidence Scale (ABC), to detect gait variability. | Although no parameter worsened over time, the multiple sclerosis cohort with moderate disability performed worse than the cohort with mild disability, which, in turn, was worse than the controls on measures of walking and balance. In addition, the cohort with moderate disability had greater variation between visits than the other cohorts (p < 0.05, Bonferroni corrected). |
| Accelerometry as a measure of walking behavior in multiple sclerosis [36] | To validate accelerometer output based on associations with Expanded Disability Status Scale (EDSS), PDDS- Patient Determined Disease Steps Scale (PDDS), Multiple Sclerosis Walking Scale 12 (MSWS-12), Timed 25-Foot Walk Test (T25FW), 6-Minute Walk Test (6 MWT), O2 cost and gait parameters. | 256 people with multiple sclerosis. | ActiGraph accelerometer model GT3X (Health One Technology, Fort Walton Beach, FL, USA), used when carrying out tests such as the T35FW and the 6 MWT, to detect special and temporal gait parameters, such as walking speed, cadence-number of steps per minute, stride length and stride time. | Accelerometer output was significantly correlated with EDSS (ρ = −0.522), PDDS (ρ = −0.551), MSWS-12 (ρ = −0.617), T25FW (ρ = −0.595) and 6 MWT (ρ = 0.630) scores.) performance and O2 cost of walking (ρ = −0.457). Regarding gait parameters, accelerometer output was significantly correlated with speed (ρ = 0.420), cadence (ρ = 0.349), step time (ρ = −0.353), step length (ρ = 0.395), double support (ρ = −0.424) and single support (ρ = 0.400). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Queiroz, R.S.; Alves, J.H.; Sasaki, J.E. Digital Biomarkers in the Assessment of Mobility in Individuals with Multiple Sclerosis. Sclerosis 2023, 1, 134-150. https://doi.org/10.3390/sclerosis1030014
de Queiroz RS, Alves JH, Sasaki JE. Digital Biomarkers in the Assessment of Mobility in Individuals with Multiple Sclerosis. Sclerosis. 2023; 1(3):134-150. https://doi.org/10.3390/sclerosis1030014
Chicago/Turabian Stylede Queiroz, Rayssa Soares, José Humberto Alves, and Jeffer Eidi Sasaki. 2023. "Digital Biomarkers in the Assessment of Mobility in Individuals with Multiple Sclerosis" Sclerosis 1, no. 3: 134-150. https://doi.org/10.3390/sclerosis1030014
APA Stylede Queiroz, R. S., Alves, J. H., & Sasaki, J. E. (2023). Digital Biomarkers in the Assessment of Mobility in Individuals with Multiple Sclerosis. Sclerosis, 1(3), 134-150. https://doi.org/10.3390/sclerosis1030014