
Supporting Functional Goals in Spinal Muscular Atrophy: A Case Report of The Cognitive Orientation to Daily Occupational Performance (CO-OP) Approach


Abstract
1. Introduction
2. Materials and Methods
2.1. Participant
2.2. Outcome Measures
2.3. Intervention
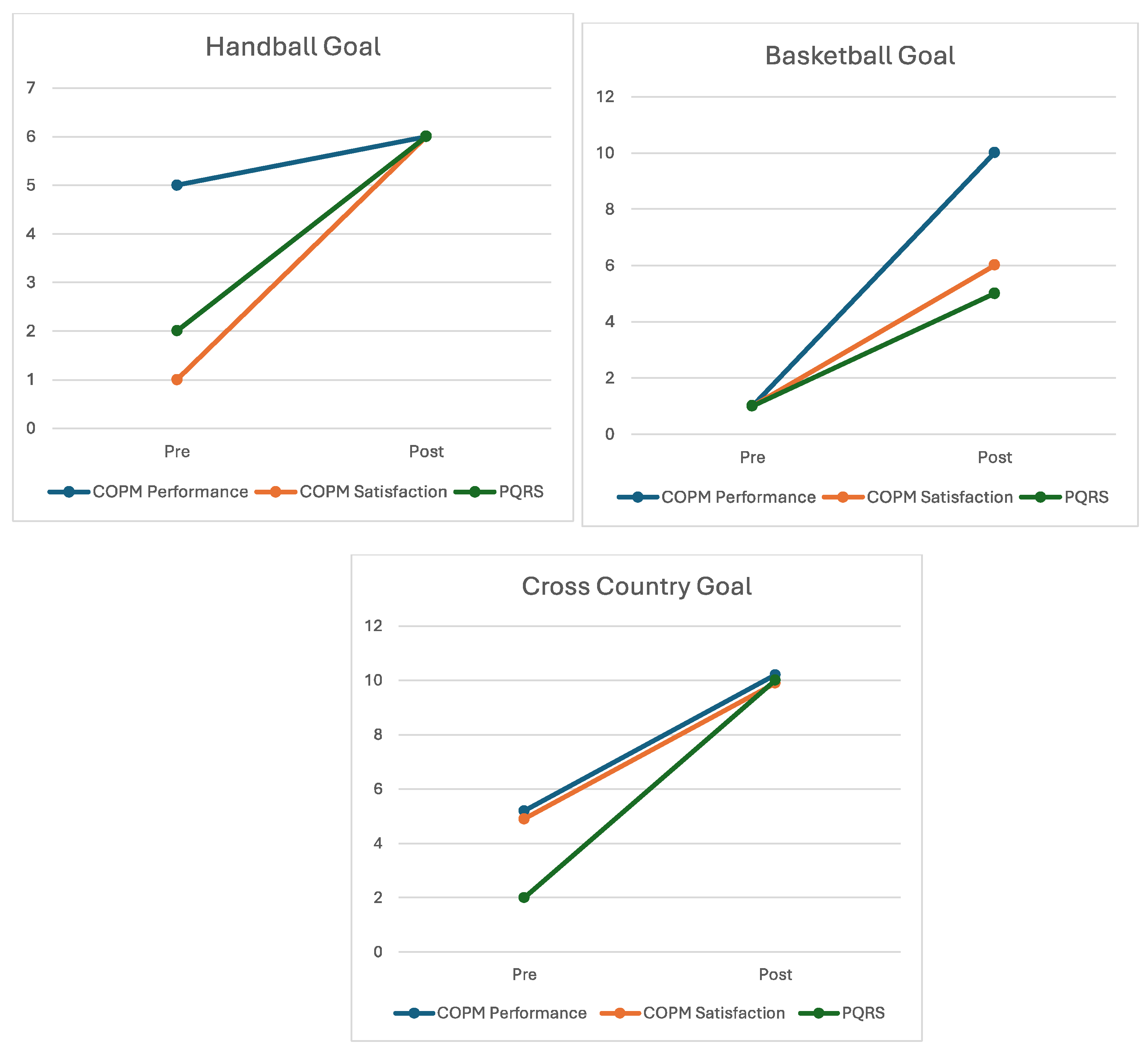
3. Results
- “I want to play handball at recess and lunch with my friends”
- “I want to play wheelchair basketball”
- “I want to race at the cross-country carnival like the other kids in my class”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mercuri, E.; Finkel, R.S.; Muntoni, F.; Wirth, B.; Montes, J.; Main, M.; Mazzone, E.S.; Vitale, M.; Snyder, B.; Quijano-Roy, S.; et al. Diagnosis and management of spinal muscular atrophy: Part 1: Recommendations for diagnosis, rehabilitation, orthopedic and nutritional care. Neuromuscul. Disord. 2018, 28, 103–115. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Masson, R.; Brusa, C.; Scoto, M.; Baranello, G. Brain, cognition, and language development in spinal muscular atrophy type 1: A scoping review. Dev. Med. Child Neurol. 2021, 63, 527–536. [Google Scholar] [CrossRef]
- Prior, T.W.; Leach, M.E.; Finanger, E. Spinal Muscular Atrophy. In GeneReviews®; Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Mirzaa, G., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 2000. [Google Scholar]
- von Gontard, A.; Zerres, K.; Backes, M.; Laufersweiler-Plass, C.; Wendland, C.; Melchers, P.; Lehmkuhl, G.; Rudnik-Schöneborn, S. Intelligence and cognitive function in children and adolescents with spinal muscular atrophy. Neuromuscul. Disord. 2002, 12, 130–136. [Google Scholar] [CrossRef]
- Polido, G.J.; de Miranda, M.M.V.; Carvas, N.; Mendonça, R.H.; Caromano, F.A.; Reed, U.C.; Zanoteli, E.; Voos, M.C. Cognitive performance of children with spinal muscular atrophy: A systematic review. Dement. Neuropsychol. 2019, 13, 436–443. [Google Scholar] [CrossRef]
- Cramm, J.M.; Strating, M.M.H.; Roebroeck, M.E.; Nieboer, A.P. The Importance of General Self-Efficacy for the Quality of Life of Adolescents with Chronic Conditions. Soc. Indic. Res. 2013, 113, 551–561. [Google Scholar] [CrossRef]
- Livingstone, R.; Paleg, G. Enhancing Function, Fun and Participation with Assistive Devices, Adaptive Positioning, and Augmented Mobility for Young Children with Infantile-Onset Spinal Muscular Atrophy: A Scoping Review and Illustrative Case Report. Disabilities 2021, 1, 1–22. [Google Scholar] [CrossRef]
- Hammell, K.W. Quality of life, participation and occupational rights: A capabilities perspective. Aust. Occup. Ther. J. 2015, 62, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Polatajko, H.J.; Mandich, A.D.; Miller, L.T.; Macnab, J.J. Cognitive orientation to daily occupational performance (CO-OP): Part II—The evidence. Phys. Occup. Ther. Pediatr. 2001, 20, 83–106. [Google Scholar] [CrossRef]
- Polatajko, H.J.; Mandich, A.D.; Missiuna, C.; Miller, L.T.; Macnab, J.J.; Malloy-Miller, T.; Kinsella, E.A. Cognitive orientation to daily occupational performance (CO-OP): Part III—The protocol in brief. Phys. Occup. Ther. Pediatr. 2001, 20, 107–123. [Google Scholar] [CrossRef]
- Dawson, D.R.; McEwan, S.E.; Polatajko, H.J. Cognitive Orientation to Daily Occupational Performance in Occupational Therapy: Using the CO-OP Approach (TM) to Enable Participation Across the Lifespan; AOTA Press: Bethesda, MD, USA, 2017. [Google Scholar]
- Cameron, D.; Craig, T.; Edwards, B.; Missiuna, C.; Schwellnus, H.; Polatajko, H.J. Cognitive Orientation to daily Occupational Performance (CO-OP): A New Approach for Children with Cerebral Palsy. Phys. Occup. Ther. Pediatr. 2017, 37, 183–198. [Google Scholar] [CrossRef]
- McColl, M.A.; Law, M.; Baptiste, S.; Pollock, N.; Carswell, A.; Polatajko, H.J. Targeted applications of the Canadian Occupational Performance Measure. Can. J. Occup. Ther. 2005, 72, 298–300. [Google Scholar] [CrossRef] [PubMed]
- Missiuna, C.; DeMatteo, C.; Hanna, S.; Mandich, A.; Law, M.; Mahoney, W.; Scott, L. Exploring the use of cognitive intervention for children with acquired brain injury. Phys. Occup. Ther. Pediatr. 2010, 30, 205–219. [Google Scholar] [CrossRef] [PubMed]
- Jackman, M.; Novak, I.; Lannin, N.; Froude, E.; Miller, L.; Galea, C. Effectiveness of Cognitive Orientation to daily Occupational Performance over and above functional hand splints for children with cerebral palsy or brain injury: A randomized controlled trial. BMC Pediatr. 2018, 18, 248. [Google Scholar] [CrossRef] [PubMed]
- Dawson, D.R.; Gaya, A.; Hunt, A.; Levine, B.; Lemsky, C.; Polatajko, H.J. Using the cognitive orientation to occupational performance (CO-OP) with adults with executive dysfunction following traumatic brain injury. Can. J. Occup. Ther. 2009, 76, 115–127. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Baptiste, S.; Carswell, A.; McColl, M.; Polatajko, H.J.; Pollock, N. COPM Canadian Occupational Performance Measure, 4th ed.; CAOT Publications ACE: Ottowa, ON, Canada, 2005. [Google Scholar]
- Cusick, A.; McIntyre, S.; Novak, I.; Lannin, N.; Lowe, K. A comparison of goal attainment scaling and the Canadian Occupational Performance Measure for paediatric rehabilitation research. Pediatr. Rehabil. 2006, 9, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Pollock, N.; Sharma, N.; Christenson, C.; Law, M.; Gorter, J.W.; Darrah, J. Change in Parent-Identified Goals in Young Children with Cerebral Palsy Receiving a Context-Focused Intervention: Associations with Child, Goal and Intervention Factors. Phys. Occup. Ther. Pediatr. 2014, 34, 62–74. [Google Scholar] [CrossRef] [PubMed]
- McColl, M.A.; Denis, C.B.; Douglas, K.L.; Gilmour, J.; Haveman, N.; Petersen, M.; Presswell, B.; Law, M. A Clinically Significant Difference on the COPM: A Review. Can. J. Occup. Ther. 2023, 90, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Martini, R.; Rios, J.; Polatajko, H.; Wolf, T.; McEwen, S. The performance quality rating scale (PQRS): Reliability, convergent validity, and internal responsiveness for two scoring systems. Disabil. Rehabil. 2015, 37, 231–238. [Google Scholar] [CrossRef]
- Scammell, E.M.; Bates, S.V.; Houldin, A.; Polatajko, H.J. The Cognitive Orientation to daily Occupational Performance (CO-OP): A scoping review. Can. J. Occup. Ther. 2016, 83, 216–225. [Google Scholar] [CrossRef]
- Jackman, M.; Lannin, N.; Galea, C.; Sakzewski, L.; Miller, L.; Novak, I. What is the threshold dose of upper limb training for children with cerebral palsy to improve function? A systematic review. Aust. Occup. Ther. J. 2020, 67, 269–280. [Google Scholar] [CrossRef]
- Brown, R.; Pressley, M.; Van Meter, P.; Schuder, T. A quasi-experimental validation of transactional strategies instruction with low-achieving second-grade readers. J. Educ. Psychol. 1996, 88, 18–37. [Google Scholar] [CrossRef]
- Yao, M.; Ma, Y.; Qian, R.; Xia, Y.; Yuan, C.; Bai, G.; Mao, S. Quality of life of children with spinal muscular atrophy and their caregivers from the perspective of caregivers: A Chinese cross-sectional study. Orphanet. J. Rare Dis. 2021, 16, 7. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.; Ziviani, J.; Ware, R.S.; Boyd, R.N. Mastery motivation: A way of understanding therapy outcomes for children with unilateral cerebral palsy. Disabil. Rehabil. 2015, 37, 1439–1445. [Google Scholar] [CrossRef] [PubMed]
- Jackman, M.; Novak, I.; Lannin, N.A.; Galea, C.; Froude, E. The Cognitive Orientation to daily Occupational Performance (CO-OP) Approach: Best responders in children with cerebral palsy and brain injury. Res. Dev. Disabil. 2018, 78, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Majnemer, A.; Shevell, M.; Law, M.; Poulin, C.; Rosenbaum, P. Level of motivation in mastering challenging tasks in children with cerebral palsy. Dev. Med. Child Neurol. 2010, 52, 1120–1126. [Google Scholar] [CrossRef]
- Jackman, M.; Novak, I.; Lannin, N.; Froude, E. Parents’ experience of undertaking an intensive cognitive orientation to daily occupational performance (CO-OP) group for children with cerebral palsy. Disabil. Rehabil. 2017, 39, 1018–1024. [Google Scholar] [CrossRef]
- Polatajko, H.J.; Mandich, A.; Martini, R. Dynamic Performance Analysis: A Framework for Understanding Occupational Performance. Am. J. Occup. Ther. 2000, 54, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Case, L.E.; Apkon, S.D.; Eagle, M.; Gulyas, A.; Juel, L.; Matthews, D.; Newton, R.A.; Posselt, H.F. Rehabilitation Management of the Patient With Duchenne Muscular Dystrophy. Pediatrics 2018, 142, S17–S33. [Google Scholar] [CrossRef]
- Bravo, L.; Killela, M.K.; Reyes, B.L.; Santos, K.M.B.; Torres, V.; Huang, C.C.; Jacob, E. Self-Management, Self-Efficacy, and Health-Related Quality of Life in Children With Chronic Illness and Medical Complexity. J. Pediatr. Health Care 2020, 34, 304–314. [Google Scholar] [CrossRef]
- Hudson, P.; Trauer, T.; Kelly, B.; O’Connor, M.; Thomas, K.; Summers, M.; Zordan, R.; White, V. Reducing the psychological distress of family caregivers of home-based palliative care patients: Short-term effects from a randomised controlled trial. Psychooncology 2013, 22, 1987–1993. [Google Scholar] [CrossRef]
- Lorig, K.R.; Holman, H. Self-management education: History, definition, outcomes, and mechanisms. Ann. Behav. Med. 2003, 26, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Yarcheski, A.; Mahon, N.E.; Yarcheski, T.J.; Cannella, B.L. A meta-analysis of predictors of positive health practices. J. Nurs. Scholarsh. 2004, 36, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Finney Rutten, L.J.; Hesse, B.W.; St. Sauver, J.L.; Wilson, P.; Chawla, N.; Hartigan, D.B.; Moser, R.P.; Taplin, S.; Glasgow, R.; Arora, N.K. Health Self-Efficacy Among Populations with Multiple Chronic Conditions: The Value of Patient-Centered Communication. Adv. Ther. 2016, 33, 1440–1451. [Google Scholar] [CrossRef] [PubMed]
- Holman, H.; Lorig, K. Patient self-management: A key to effectiveness and efficiency in care of chronic disease. Public Health Rep. 2004, 119, 239–243. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Goal | Pre-Intervention Score | Post-Intervention Score | Change Score |
|---|---|---|---|
| Handball | |||
| COPM Performance | 5/10 | 6/10 | 1 |
| COPM Satisfaction | 1/10 | 6/10 | 5 |
| PQRS | 2/10 | 6/10 | 4 |
| Basketball | |||
| COPM Performance | 1/10 | 10/10 | 9 |
| COPM Satisfaction | 1/10 | 6/10 | 5 |
| PQRS | 1/10 | 5/10 | 4 |
| Cross-Country Running | |||
| COPM Performance | 5/10 | 10/10 | 5 |
| COPM Satisfaction | 5/10 | 10/10 | 5 |
| PQRS | 2/10 | 10/10 | 8 |
| Enabling Principles | How Therapist Used Enabling Principle with Miss M |
|---|---|
| Make it fun | Being motivated to practice the goal of handball with carers and siblings and Miss M’s competitive nature to do so facilitated a continuous playful interaction throughout the problem-solving process between caregivers, therapist and the child. |
| Work towards independence | Miss M thrived with independence and taking the lead. They were eager to demonstrate their independence in use of the cognitive process through ‘homework’ recaps of their use of the ‘Goal–Plan–Do–Check’ and bringing back progress videos of their performance of handball at school each week to show the therapist. |
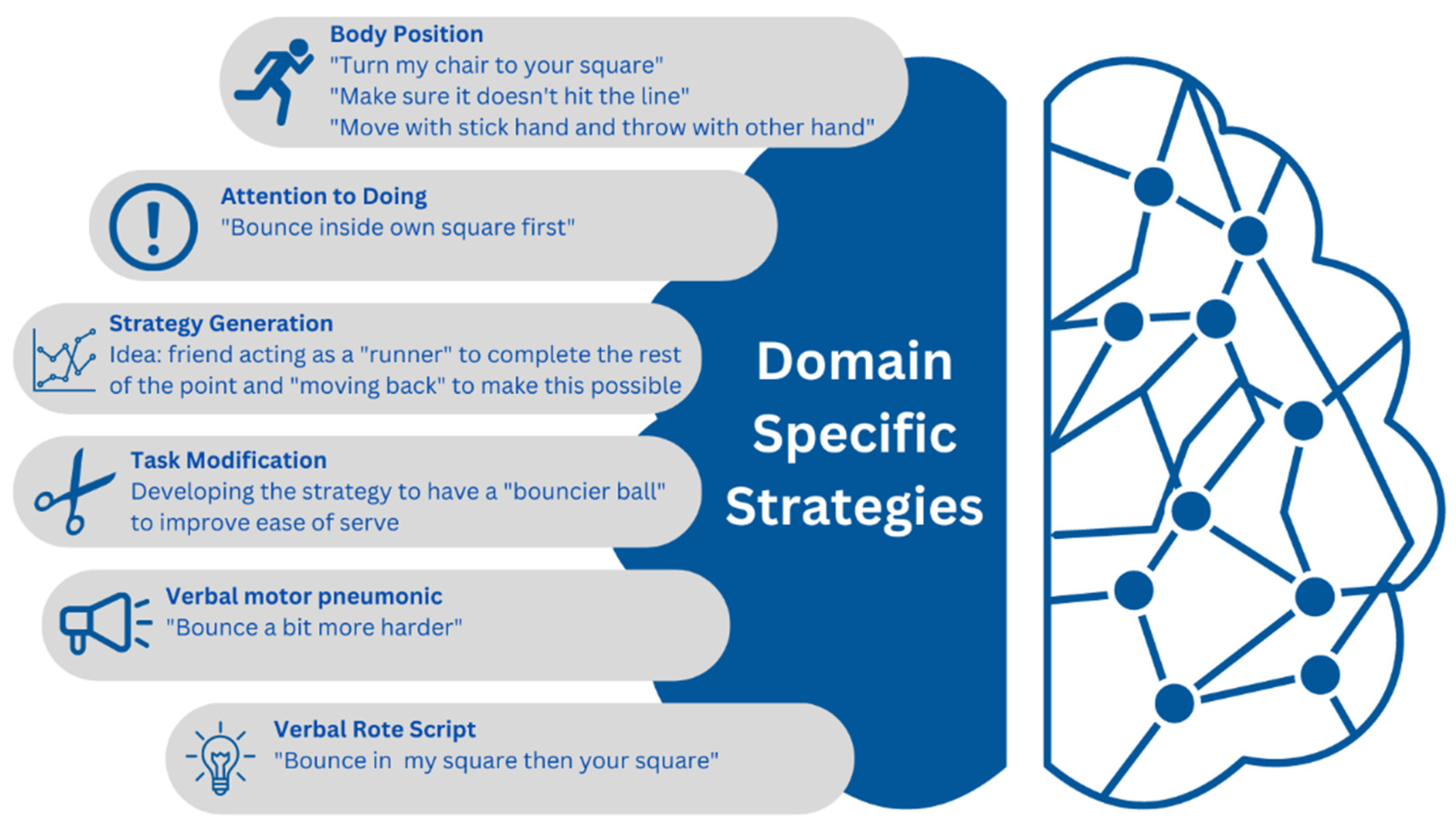
| Promote good strategy use | Supplementing task knowledge of school handball games and wheelchair soccer was utilised in order to enable effective strategy generation. Collaborating with the school sport’s teacher and principal allowed for further support of Miss M’s strategy generation and guidance. |
| One thing at a time | Only one performance breakdown was focused on at a time and the sequence of the activities were prescribed and lead by Miss M. When the therapist or caregiver felt that Miss M’s motivation was waning or they had reached their maximum strategy generation and required periods of consolidation, they would guide the child to progress onto their next goal. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taylor, S.; Novak, I.; Jackman, M. Supporting Functional Goals in Spinal Muscular Atrophy: A Case Report of The Cognitive Orientation to Daily Occupational Performance (CO-OP) Approach. Future 2024, 2, 46-55. https://doi.org/10.3390/future2020004
Taylor S, Novak I, Jackman M. Supporting Functional Goals in Spinal Muscular Atrophy: A Case Report of The Cognitive Orientation to Daily Occupational Performance (CO-OP) Approach. Future. 2024; 2(2):46-55. https://doi.org/10.3390/future2020004
Chicago/Turabian StyleTaylor, Stephanie, Iona Novak, and Michelle Jackman. 2024. "Supporting Functional Goals in Spinal Muscular Atrophy: A Case Report of The Cognitive Orientation to Daily Occupational Performance (CO-OP) Approach" Future 2, no. 2: 46-55. https://doi.org/10.3390/future2020004
APA StyleTaylor, S., Novak, I., & Jackman, M. (2024). Supporting Functional Goals in Spinal Muscular Atrophy: A Case Report of The Cognitive Orientation to Daily Occupational Performance (CO-OP) Approach. Future, 2(2), 46-55. https://doi.org/10.3390/future2020004