Abstract
We present an 81-year-old male with an extensive past medical history and an enlarging abdominal aortic aneurysm (AAA). Axial imaging showed dense aortoiliac calcification with a complete occlusion of the right common iliac and high-grade stenosis of the left common iliac artery (CIA). Shockwave Intravascular Lithotripsy and the pave-and-crack technique utilizing an endoconduit were used to dilate the left external iliac artery and the CIA to facilitate placement of an aortic stent graft and exclude the patient’s AAA. This method gives surgeons the ability to treat patients with AAAs endovascularly, despite a heavily diseased and/or diminutive iliac anatomy. We also present a contemporary literature review of the utilization of the pave-and-crack technique as well as tips and tricks of how we do it.
1. Introduction
The annual incidence of new abdominal aortic aneurysm (AAA) diagnoses in Western populations ranges from approximately 0.4% to 0.67%, corresponding to 2.5 to 6.5 cases per 1000 person-years [1]. Endovascular aneurysm repair (EVAR) has gained widespread acceptance as the primary treatment modality for AAA, particularly among high-risk populations, including elderly patients with significant cardiovascular comorbidities [2].
Age is a critical determinant of AAA incidence. For instance, one study demonstrated that the incidence among males aged 65 to 74 years was 55 cases per 100,000 person-years. This figure rose to 112 per 100,000 person-years for those aged 75 to 85 years and further increased to 298 per 100,000 person-years in males over 85 years of age [3].
The success of EVAR heavily depends on the patient’s vascular anatomy [4]. The substantial caliber of endoprosthesis delivery systems can present technical challenges in patients with complex iliac anatomy, including severe atherosclerotic disease, stenosis, or tortuosity [5].
In a retrospective cohort study by Liang et al., involving 247 patients who underwent percutaneous EVAR, access site failures were observed in 5.9% of femoral arteries. Contributing factors included smaller femoral artery diameters, stenosis exceeding 50%, and the need for urgent or emergent interventions [6].
Traditional management strategies for such cases include open aortic repair, open iliac conduit placement, and iliac angioplasty with or without stenting. However, recent advancements, such as the intravascular lithotripsy (IVL) and the pave-and-crack method, have been developed to address mismatches between delivery device dimensions and patient arterial anatomy. These techniques enable dilation of the external iliac arteries (EIAs) and common iliac arteries (CIAs), facilitating the safe insertion of an aortic stent graft to exclude AAAs [7]. Adverse iliac artery anatomy remains a major obstacle to successful EVAR and is a leading cause of conversion to open repair [8].
This report highlights a case where the pave-and-crack technique, combined with IVL, was employed. This innovative approach has received limited attention in the literature, particularly regarding its role as an adjunctive method in AAA management. The pave-and-crack technique involves the placement of covered stents, or endoconduits, within the iliac arteries, followed by controlled dilation to achieve larger vessel diameters and an intentional rupture of the access vessels [4]. By utilizing covered stent grafts, this method minimizes the need for extensive arterial dissection and mitigates the risk of catastrophic complications, such as “iliac on a stick”. Moreover, it eliminates the necessity for open retroperitoneal access, thereby reducing complications such as increased blood loss, prolonged operative times, extended hospital stays, and heightened postoperative morbidity and mortality [8].
2. Case Presentation
An 81-year-old male with a past medical history of peripheral arterial disease (PAD), coronary artery disease status post coronary stenting, stage three chronic kidney disease, and lung cancer for which he underwent a left pneumonectomy and right wedge resection presented to our clinic with an asymptomatic infrarenal AAA with extensive calcifications. He had a left superficial femoral artery (SFA) endarterectomy with a patch angioplasty performed in 2019 for claudication. After that procedure, his symptoms were controlled well, and he was surveilled with CTAs. His AAA had enlarged from 4.5 cm in 2021 to 5.5 cm in 2024. Imaging also showed a chronic occlusion of the right common and external iliac arteries (EIA) with reconstitution of flow to the SFA from collateral vessels, as well as severe tandem stenoses of the left CIA and EIA (Figure 1a). He was not a candidate for open repair due to comorbid conditions and significant aortic calcifications, precluding safe aortic clamping. Notably, his ABIs were 0.57/1.07 and he did not endorse any claudication symptoms.
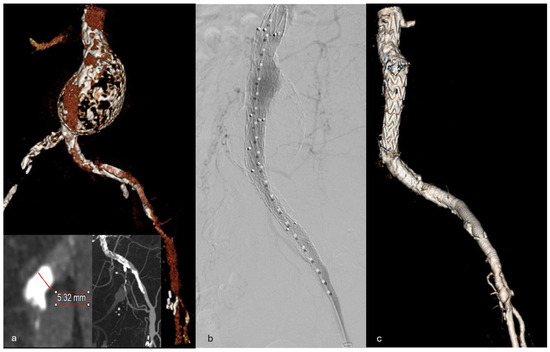
Figure 1.
(a) Preoperative CTA 3D reconstruction of aortic aneurysm with calcified and diminutive left iliac artery. Inserts showing dense iliac calcification. (b) Aorto-uni-iliac (AUI) completion angiogram. (c) Postoperative CTA 3D reconstruction of AUI, VBX and Viabahn.
We performed a left groin cutdown, and his prior patch was accessed in the standard fashion with a micropuncture kit. Next, after heparinization, Shockwave IVL (Shockwave Medical Inc., Santa Clara, CA, USA) of his left CIA, down to his proximal common femoral artery, was performed to 7 mm without vessel rupture. Then an 8 L by 79 mm VBX stent (W.L. Gore & Associates Inc., Flagstaff, AZ, USA) was advanced into the proximal CIA and dilated to nominal pressures to size match the aorto-uni iliac (AUI) device. Next, an 8 mm × 250 mm Viabahn stent (W.L. Gore & Associates Inc., Flagstaff, AZ, USA) was deployed with adequate overlap all the way out of the CFA and out of the groin to use as a handle (Figure 2a). An umbilical tape was used as a Rummel tourniquet around a GORE Dry Seal sheath within the Viabahn stent (Figure 2b). We then sequentially ballooned all the way out of the left CFA into the externalized Viabahn stent, with an 8 mm × 40 mm high-pressure Conquest balloon (Becton, Dickinson and Company, Franklin Lakes, NJ, USA), using the pave-and-crack technique rupturing the iliac system without hemodynamic consequences. An 18 Fr DrySeal sheath (W.L. Gore & Associates Inc., Flagstaff, AZ, USA) was easily advanced through the endoconduit, and a 23 mm × 102 mm AUI graft (Medtronic, Minneapolis, MN, USA) was deployed infrarenally. Next, a 16 cm × 10 mm bridging limb was deployed between the stent graft and the AUI. Finally, the VBX was then dilated to 10 mm proximally for a successful size match into the limb (Figure 3a). The graft was then ballooned, and a completion angiogram demonstrated brisk flow within the aortoiliac graft, without flow into the aneurysm sac (Figure 1b). The Viabahn stent was cut flush to the left CFA, and an anterior slit was made and tacked down with several sutures (Figure 2c and Figure 3c). The femoral artery and groin were primarily closed (importantly, for a virgin CFA we recommend patch angioplasty, as shown in Figure 3d). Flourosopcy time was less than 35 min, with a total dose of 1.4 Gy of radiation, with 90 cc of contrast used, and an EBL of 100 cc. The patient recovered well and was discharged the following day. He was followed up at 6 months without any complications or endoleak with sac regression.
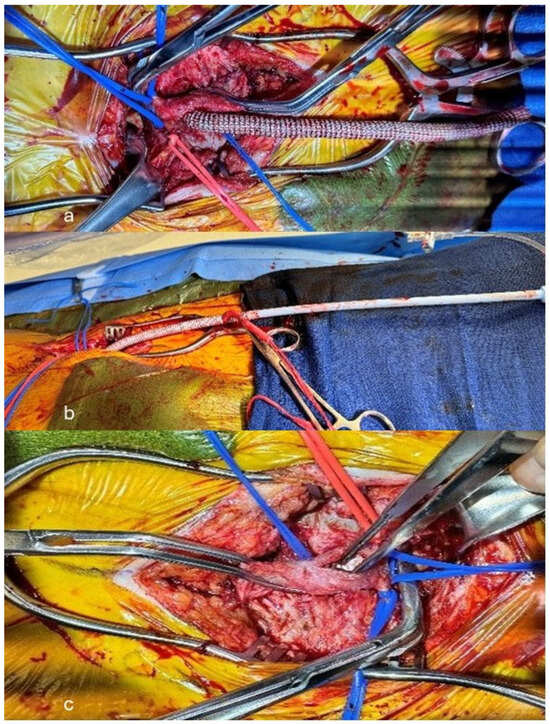
Figure 2.
(a) Open left common femoral artery access, with 8 mm × 250 mm Viabhan stent graft externalized. (b) Externalized endoconduit with 18 Fr DrySeal sheath secured with Rummel tourniquet. (c) Forming an anterior slit though the CFA and endoconduit with tacking suture to the endoconduit.

Figure 3.
(a) Animation of AUI, VBX and Endoconduit. (b) Cutting the endoconduit flush with the CFA. (c) Forming an anterior slit though the CFA and endoconduit with tacking suture to the endoconduit. (d) Patch from the endoconduit to CFA.
3. Discussion
Endovascular repair has become the de facto technique to treat the majority of AAAs; however, these repairs are only possible if endoprostheses can be delivered to the aorta [2]. Pave-and-crack is a technique first described in 2007, and since then only a handful of case reports or series describe utilizing this method [5]. The literature that does exist shows positive outcomes with this technique [5,6,9,10,11,12,13,14,15]. Our literature review showed a 30-day morbidity rate of only four–one of the patients experienced a distal embolization that was treated intra-operatively, another experienced a femoral pseudoaneurysm that was treated with manual compression, and two experienced groin infections that were treated with negative pressure wound vacuum therapy. The literature review also showed a 30-day mortality rate of 4%, with one of the patients being treated for a ruptured AAA (Table 1). Furthermore, we also had excellent outcomes with the pave-and-crack technique for a patient that otherwise would not have been offered an AAA repair. Our patient underwent post-operative surveillance imaging after two months, which demonstrated patency of his AUI and iliac stent grafts. He experienced no intra-operative or immediate post-operative complications.

Table 1.
Chart of the recent literature citing the use of the pave-and-crack technique and its outcomes.
The intravascular lithotripsy is a more widely utilized technique to treat PAD and disrupt long segments of atherosclerosis. We combined this approach with the pave-and-crack technique to treat this patient’s aortic aneurysm and to deliver an AUI device. We felt that lithotripsy could help facilitate the passage of the Viabahn stent, but it is not required to be used with pave-and-crack. The decision to utilize both techniques should be left to the discretion of the surgeon.
When deciding on an endoconduit, the patency of the hypogastric is important. If treating an infrarenal aneurysm with a patent hypogastric, we would encourage proximal hypogastric embolization to prevent potential backbleeding when cracking the common and external iliac arteries. Alternatively, in cases with long-segment lumbar/intercostal artery coverage, an endoconduit may be a poor option, when relying on pelvic spinal perfusion via the hypogastric. After an open CFA exposure and standard access with a micropuncture kit, we chose to use the IVL, due to the severe calcific disease present. For conduit creation, we chose to use a balloon expandable stent graft (8 L × 79 mm VBX) in the CIA, that could be dilated proximally to accommodate the iliac limb, while maintaining its nominal size distally to marry into the Viabahn stent. Alternatively, if only creating an endoconduit, a single self-expanding stent graft, such as an 8 mm × 250 mm Viabahn, is sufficient without a balloon-expandable stent graft. After successful aortic endoprosthesis delivery, we applied proximal and distal clamps on the CFA and transected the Viabahn stent flush with the artery (Figure 3b). We then created a longitudinal arteriotomy with anterior stent slit/transection and tacked this to the arterial wall (Figure 2c and Figure 3c). This allowed for patch closure of the common femoral artery (Figure 3d).
Our literature review noted a two-case series, that followed a combined 86 patients treated with the pave-and-crack technique. However, only one of these case series reported on patients treated for AAA (19 patients). The mean follow up for this case series was 17 months, which showed that the primary assisted patency of the endoconduit was 88.9%. Re-intervention was necessary for five of the patients, but only for one patient it was regarding the endoconduit. Ultimately, a longer follow up and further studies, on a greater number of patients, are required to determine the long-term patency and complication rates for patients with AAAs, treated with the pave-and-crack technique; nevertheless, this is a viable technique for prohibitive iliac anatomy.
4. Conclusions
Pave-and-crack makes it possible to accomplish an endovascular repair of an AAA in patients that have severe stenosis or atherosclerosis of their iliac arteries, that would otherwise prohibit the delivery of large endoprosthesis devices. The literature supports that this is a generally safe and successful technique to enlarge prohibitive iliac access. This increases the population of patients with AAA that surgeons can treat—especially when patients are poor candidates for open surgery based on calcification of their aorta and/or comorbidities.
5. Patient Consent Statement
The patient provided written consent for the publication of this case report.
Author Contributions
Conceptualization, S.G., Y.A., M.S. and R.D.; writing—original draft preparation, S.G., Y.A., M.S., R.D. and C.J.; writing—review and editing, J.V., B.M., Y.E., H.F., E.A., B.F. and A.F.; visualization, S.G., Y.A. and C.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This case report did not require ethical approval.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
There is no available data as this is a case report and literature review.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Vardulaki, K.A.; Prevost, T.C.; Walker, N.M.; Day, N.E.; Wilmink, A.B.; Quick, C.R.; Ashton, H.A.; Scott, R.A. Incidence among men of asymptomatic abdominal aortic aneurysms: Estimates from 500 screen detected cases. J. Med. Screen. 1999, 6, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Chaikof, E.L.; Dalman, R.L.; Eskandari, M.K.; Jackson, B.M.; Lee, W.A.; Mansour, M.A.; Mastracci, T.M.; Mell, M.; Murad, M.H.; Nguyen, L.L.; et al. The Society for Vascular Surgery Practice Guidelines on the care of patients with an abdominal aortic aneurysm. J. Vasc. Surg. 2018, 67, 2–77. [Google Scholar] [CrossRef] [PubMed]
- Howard, D.P.; Banerjee, A.; Fairhead, J.F.; Handa, A.; Silver, L.E.; Rothwell, P.M.; Oxford Vascular Study. Population-Based Study of Incidence of Acute Abdominal Aortic Aneurysms With Projected Impact of Screening Strategy. J. Am. Heart Assoc. 2015, 4, e001926, Erratum in J. Am. Heart Assoc. 2015, 4, e001992. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sidawy, A.N.; Perler, B.A.; Rutherford, R.B. Rutherford’s Vascular Surgery and Endovascular Therapy; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Hinchliffe, R.J.; Ivancev, K.; Sonesson, B.; Malina, M. “Paving and Cracking”: An Endovascular Technique to Facilitate the Introduction of Aortic Stent-Grafts through Stenosed Iliac Arteries. J. Endovasc. Ther. 2007, 14, 630–633. [Google Scholar] [CrossRef] [PubMed]
- Giusca, S.; Schmidt, A.; Korosoglou, G. ‘Pave-and-crack’ technique for the recanalization of severely calcified occlusive aorto-ilio-femoral disease in type-III Leriche syndrome: A case report. Eur. Heart J. Case Rep. 2021, 5, ytab059. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cuypers, P.W.; Laheij, R.; Buth, J. Which factors increase the risk of conversion to open surgeryfollowing endovascular abdominal aortic aneurysm repair. Eur. J. Vasc. Endovasc. Surg. 2000, 20, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Liang, P.; O’Donnell, T.F.X.; Swerdlow, N.J.; Li, C.; Lee, A.; Wyers, M.C.; Hamdan, A.D.; Schermerhorn, M.L. Preoperative risk score for access site failure in ultrasound-guided percutaneous aortic procedures. J. Vasc. Surg. 2019, 70, 1254–1262.e1. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lee, W.A.; Berceli, S.A.; Huber, T.S.; Ozaki, C.K.; Flynn, T.C.; Seeger, J.M. Morbidity with retroperitoneal procedures during endovascular abdominal aortic aneurysm repair. J. Vasc. Surg. 2003, 38, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Dias-Neto, M.; Matschuck, M.; Bausback, Y.; Banning-Eichenseher, U.; Steiner, S.; Branzan, D.; Staab, H.; Varcoe, R.L.; Scheinert, D.; Schmidt, A. Endovascular Treatment of Severely Calcified Femoropopliteal Lesions Using the “Pave-and-Crack” Technique: Technical Description and 12-Month Results. J. Endovasc. Ther. 2018, 25, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Asciutto, G.; Aronici, M.; Resch, T.; Sonesson, B.; Kristmundsson, T.; Dias, N.V. Endoconduits with “Pave-and-crack” Technique Avoid Open Ilio-femoral Conduits with Sustainable Mid-term Results. Eur. J. Vasc. Endovasc. Surg. 2017, 54, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Weinkauf, C.; Montero-Baker, M.; Mills, J.L. Dynamic Tailoring of the “Pave-and-crack” Technique in EVAR Cases with Prohibitive Iliac Artery Anatomy: Lessons from a Small Case Series. J. Vasc. Surg. 2013, 58, 555–556. [Google Scholar] [CrossRef][Green Version]
- Aratame, A.; Murakami, T.; Inno, G.; Nishiya, K.; Bito, Y.; Sakaguchi, M.; Aoyama, T. “Crack and Pave” and Intentional Protrusion of an Endoconduit into the Terminal Aorta for Endovascular Abdominal Aneurysm Repair. Osaka City Med. J. 2020, 66, 59–63. [Google Scholar]
- Kpodonu, J.; Rodriguez-Lopez, J.A.; Ramaiah, V.G.; Diethrich, E.B. “Cracking and Paving”: A Novel Technique to Deliver a Thoracic Endograft Despite Ilio-Femoral Occlusive Disease. J. Card. Surg. 2009, 24, 188–190. [Google Scholar] [CrossRef] [PubMed]
- Gallitto, E.; Palmerini, T.; Saia, F.; Gargiulo, M. Iliac “paving & cracking” technique for transcatheter aortic valve implantation. Catheter. Cardiovasc. Interv. 2022, 100, 464–470. [Google Scholar] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).