While the imaging of arteries and veins by CT, MRI, and angiography is standard practice in large and small hospitals as well as in outpatient practices in developed countries, the diverse and sophisticated radiological procedures for imaging lymph ducts are often unknown and available only in a few specialized institutions. The latter may be because the performance of so-called lymphangiography, i.e., the selective visualization of the lymph ducts including lymph nodes and lymphatic pathology using contrast material, requires expert knowledge and specific resources. In addition, the pathologies of the lymphatic system are much rarer compared to diseases of the arterial and venous systems, such that a sufficient number of cases has thus far only been encountered in centers for lymphatic disease. Nevertheless, in recent years, various radiological procedures have developed into highly clinically effective methods. The purpose of this Editorial is to highlight the clinically relevant aspects of lymphangiography. This perspective is based on the nearly 40 years of continuous experience of the three German Centers for Lymphatic Imaging and Intervention: Heidelberg University Hospital, the Stuttgart Clinics and Bonn University Hospital. In an emphatically pragmatic way, the indications, technical implementation, and results of the various approaches with respect to lymphangiography are explained and presented. In a concluding outlook, specific interventions for the minimally invasive treatment of lymphatic fistulas are discussed, among other topics
Lymphatic pathologies can be classified as iatrogenic or spontaneous [
1,
2]. Typical iatrogenic forms include postoperative lymphatic fistulae and lymphatic fistulae after chemotherapy (e.g., in patients with types of non-Hodgkin’s lymphoma such as chylaskos or chylothorax) [
3]. The much rarer spontaneous lymphatic fistulas, which are typically diagnosed in babies, infants, and young children but can occur in the elderly, include complex lymphatic vascular anomalies and malformations as well as protein-loosing-enteropathy and plastic bronchitis [
2]. Depending on the drainage volume, a distinction is made between high-output and low-output fistulas, with a threshold of 500 mL per day in adults (
Figure 1) [
1,
2,
4].
A lymphatic fistula is a serious clinical problem for the affected patient and should never be underestimated. Uncontrollable dehydration, electrolyte imbalance, renal failure, protein loss, leukocyte loss, and superinfection are just a few of the dreadful complications. The consequences range from impaired quality of life, e.g., in patients with chronic low-output fistulas (multiple daily changes of wound dressings, months of dietary modification, or years of outpatient follow-up services), to death, typically in patients with acute high-output fistulas. From an emotional perspective, these aspects are dealt with as opportunities and challenges in a recent report published by Nature Research Custom Media (
https://www.nature.com/articles/d42473-022-00400-x; accessed on 14 December 2022). The following aspects present a purely scientific approach that provides evidence for how lymphangiography can contribute to the diagnosis and treatment of these difficult-to-treat patient populations.
Lymphangiography is only indicated in refractory lymphatic fistulas, i.e., when conservative measures such as parenteral fat-free feeding, percutaneous drainage therapy, and repeated subcutaneous octreotide injections fail to achieve the desired clinical outcome [
1,
2,
3]. In clinically unclear situations with a questionable persistence of lymphatic fistulas, e.g., under or after conservative therapy, the so-called Patent Blue test can be used. In this regard, the color change of the drainage fluid after a subcutaneous injection of Patent Blue into the first, second, and third interdigital spaces of the foot provides direct clinical evidence of the lymphatic fistula. In a broader sense, the Patent Blue test can be described as the simplest form of a lymphangiography, since, after the interstitial injection, the dye is mainly transported away centrally via the superficial lymph ducts, travelling from the lower extremities first via the groin and retroperitoneum to the cisterna chyli, and from thence via the thoracic duct to the left venous angle. If the aforementioned physiological lymphatic run-off is disturbed by a lymphatic fistula, pathological extravasation of Patent Blue is observed at the site of the fistula, thus providing visual evidence of the fistula (
Figure 2).
Lymphangiography can be offered either as “conventional lymphangiography” under radiographic control with an oil-containing contrast material (Lipiodol Ultrafluid; Guerbet, Villepinte, France) or as “MR lymphangiography” with a gadolinium-containing contrast material (e.g., Gadovist; Bayer, Germany) [
2,
5]. The decisive factor in both procedures is the selective and super-selective injection of the contrast material directly into the lymphatic system, as only in this way can high-resolution imaging of lymphatic pathology be achieved with the greatest possible accuracy.
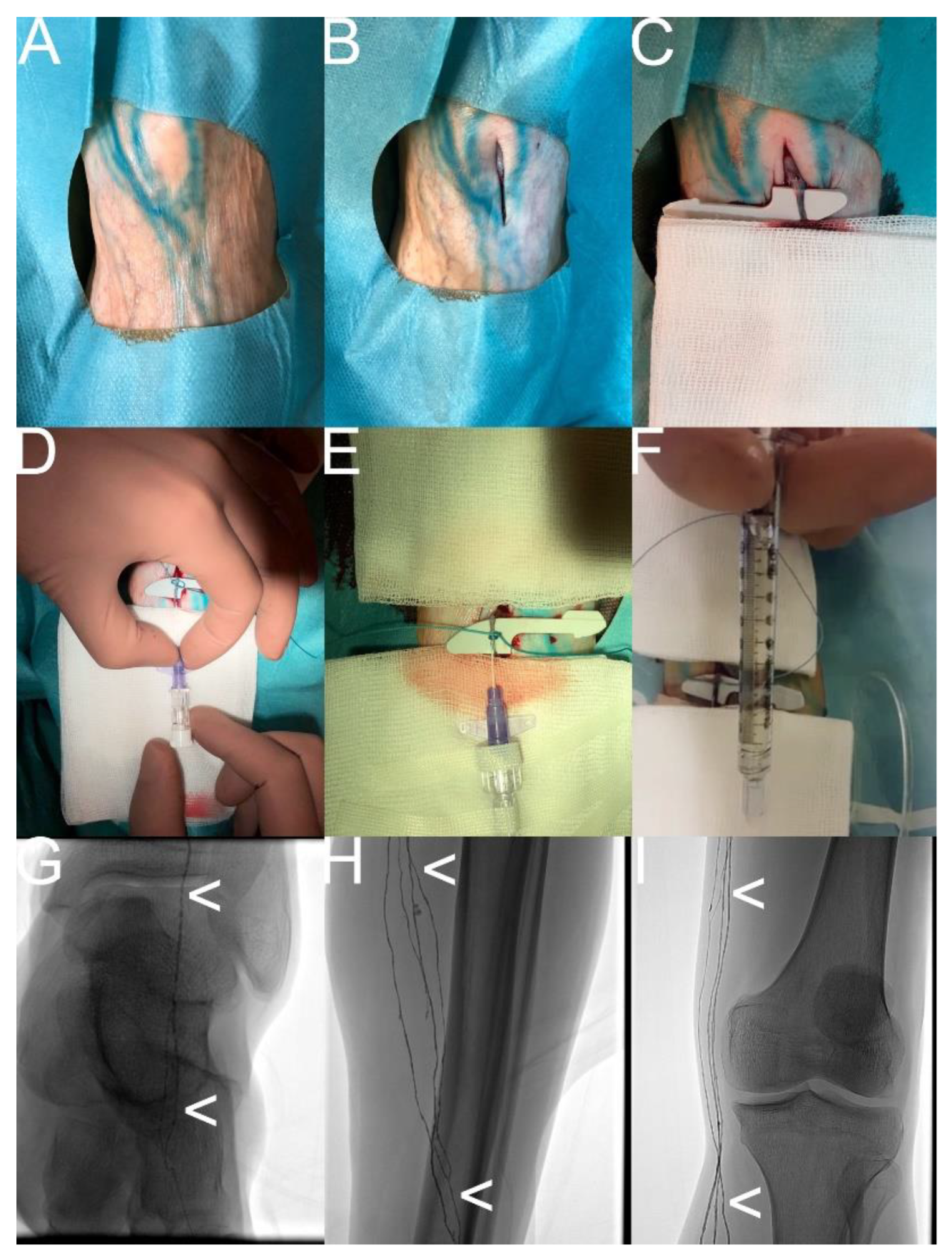
In “conventional lymphangiography”, the contrast material is injected either directly into a dissected and punctured lymph duct on the dorsum of the foot (“transpedal lymphangiography”) or into a lymph node after an ultrasound-guided percutaneous puncture, e.g., inguinal, retroperitoneal, axillary, or cervical (“intranodal lymphangiography”). The contrast material must be injected slowly at a flow rate between 0.07 and 2 mL per min, depending on the run-off capacity of the lymph duct. According to the instructions for use, the maximum dose of the oil-containing contrast material to be applied is 0.25 mL per kg body weight, but much higher doses have been reported in different clinical series [
1,
4,
6]. Depending on the location of the lymphatic fistula, imaging by conventional radiography or CT is performed a few minutes to several hours following the contrast material’s injection [
7]. While pathologic extravasation can be documented after only a few seconds to minutes for lymphatic fistulas in the groin, this direct radiological evidence of a lymphatic fistula can take several hours or even several days to appear in thoracic, cervical, or axillary locations.
Figure 3 and Vid. 1 show the technique for “conventional lymphangiography” according to the protocol of the Stuttgart Clinics.
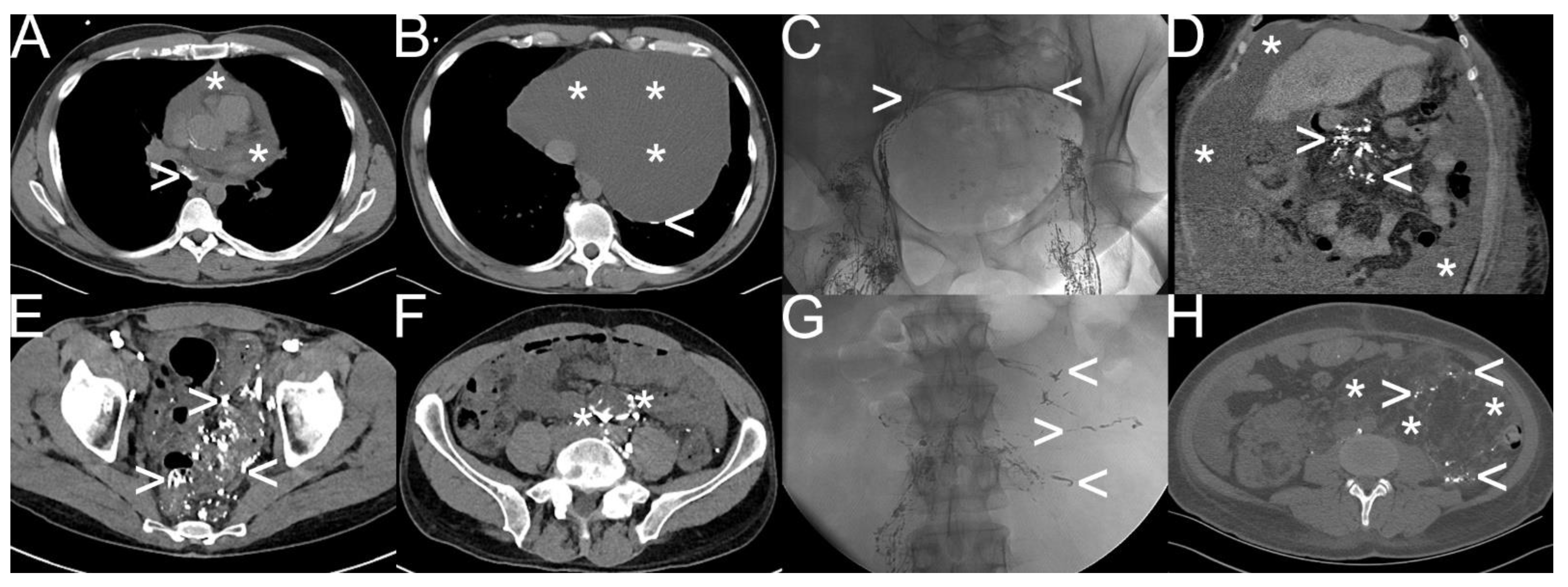
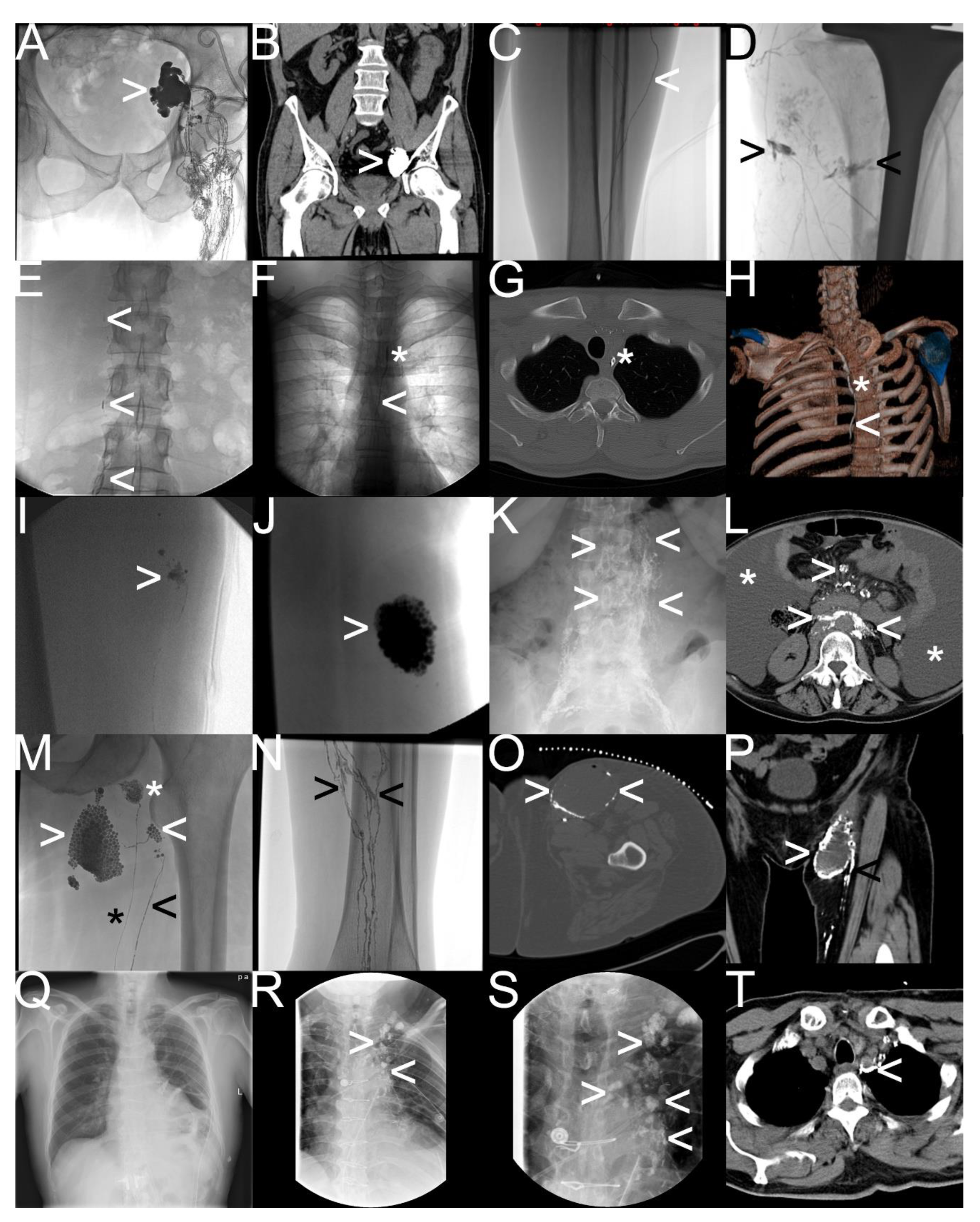
Figure 4 and
Figure 5 show different types of spontaneous and iatrogenic lymphatic fistulas detected by “conventional lymphangiography”.
“MR lymphangiography” is also divided into two forms: the first form, “interstitial MR lymphangiography”, entailing an intracutaneous injection of diluted contrast material containing gadolinium (e.g., 1:1 gadolinium/saline mixture) into the first, second, and third interdigital spaces of an extremity, and the second, “intranodal MR lymphangiography”, entailing an injection of a pure gadolinium-containing contrast agent typically into inguinal lymph nodes. Further information on the performance of “MR lymphangiography” can be found in the multiple publications of the Bonn University Hospital [
5,
8,
9,
10,
11,
12]. The advantage of “MR lymphangiography” is the possibility of high-temporal resolution dynamic imaging of even atypical lymphatic fistulas including tiny feeders; the disadvantage is the off-label nature of gadolinium-containing contrast material’s injection and the additional time required.
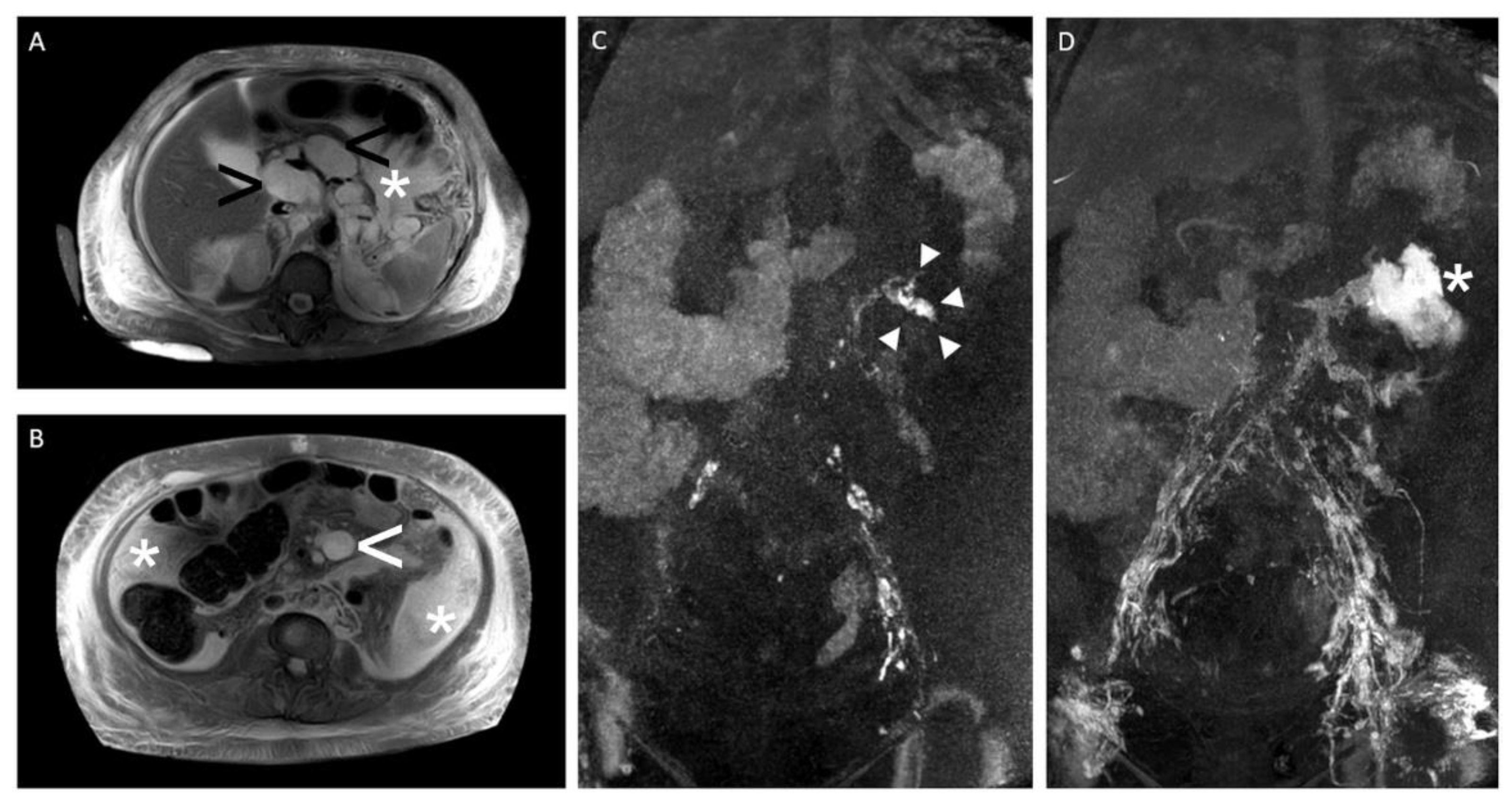
Figure 6 and
Figure 7 show typical findings of lymphatic fistulas in “MR lymphangiography”.
Ultimately, the choice of the appropriate form of lymphangiography depends on the type and location of the lymphatic fistula, the interdisciplinary treatment strategy employed, and the expertise of the center [
2,
4,
5,
7,
11,
12,
13].
“Conventional lymphangiography” shows a technical success rate of 75–100% with a very low rate of major complications [
1,
3,
4]. According to systematic reviews, direct or indirect radiologic fistula detection is successful in 58–95% of cases, with the additional use of CT associated with better results [
1,
3]. In addition, it is notable that “conventional lymphangiography” with an oil-containing contrast material has both diagnostic and therapeutic effects. Due to its high viscosity, there is a blockage of the feeders by the oil-containing contrast material, which, in many cases, can already lead to healing. Accordingly, cure rates of up to 70%—after single or repeat conventional lymphangiography—have been reported in the literature, with worse clinical outcomes for high-output fistulas [
1,
3,
4,
7]. In the most extensive paper on transpedal lymphangiography involving 355 patients, the Heidelberg University Hospital was able to define two positive predictors of healing: a drainage volume of <500 mL per day and a pathologic extravasation of the contrast material [
4]. Therefore, “conventional lymphangiography” with an oil-containing contrast material is used as second-line therapy in different centers [
1,
2,
3].
“MR lymphangiography” provides remarkable results as a purely diagnostic procedure. In patients with chylothorax, “interstitial MR lymphangiography” provides clinically useful information in 92% of patients, such as the identification of anatomic variants in 88% of patients. Procedure-related complications were not observed [
9]. Compared with “interstitial MR lymphangiography”, “intranodal MR lymphangiography” is more complex to perform but provides better information regarding the dynamics of central lymphatic run-off [
5]. For example, the correct identification of pathologic drainage in the upper abdomen can provide important information used to determine the further treatment strategy. Dynamic MR lymphangiography can detect retrograde lymphatic drainage from the cisterna chyli into the mesenteric lymphatics in chylaskos or antegrade collateral lymphatic drainage via the liver and diaphragm directly into the thoracic duct, bypassing the cisterna chyli in the chylothorax [
14].
As described, lymphangiography is a technically reliable, safe, and effective procedure for the radiological imaging of the lymphatic system and fistulas. Our discipline now offers not only the possibility of detection and localization but also treatment. The image-guided percutaneous interventions for lymphatic fistulas, developed or optimized in recent years, are diverse. They may have several advantages over surgical and conservative procedures, including higher clinical success rates, lower procedure-related complication rates, and cost effectiveness. The standard procedures include CT-guided “interstitial embolization” for iliac lymphocele or chylaskos and fluoroscopy-guided antegrade or retrograde “thoracic duct embolization” for postoperative chylothorax or plastic bronchitis. More information regarding the armamentarium can be found in the literature, including the reviews “Back to the Future: Lipiodol in Lymphography-From Diagnostics to Theranostics” and “Radiological management of postoperative lymphorrhea” [
2,
3]. A brief overview is provided in
Table 1.
The anticipated future increase in demand regarding medical services for the treatment of lymphatic pathology presents challenges for the field of radiology and its clinical partners. The standardization and broader implementation of radiological procedures, the implementation of generally accepted interdisciplinary treatment regimens, and, finally, the establishment of evidence-based guidelines are all urgently needed. One important step could have been realized on 19 March 2022 when the “1st Surgical-Radiological RoundTable for the Improvement of the Interdisciplinary Treatment of Patients with Postoperative Lymphatic Fistulas” took place in Frankfurt am Main, Germany. Participants from different institutions discussed topics such as perspectives, levels of evidence, and action plans (ES. 1). In addition to the purely medical aspects, the health economic aspects were also discussed. For example, the significant reduction in the length of stay for patients with acute postoperative lymphatic fistulas after therapeutic lymphangiography could be an interesting strategic lever for case managers and controllers. More detailed information on these key performance indicators—with possible simultaneous improvements in economic and medical quality—can be found, for example, in two original papers by our group [
4,
14]. The initiative of this first RoundTable serves to consolidate and further develop a constructive interdisciplinary dialogue with the primary objective of improving the quality of patient care already established in the short term.
Note: Following the ultrasound-guided positioning of a 23G spinal needle into the hilar region of an inguinal lymph node, this footage shows the fluoroscopy-guided injection of an oil-containing contrast material together with a visualization of the inguinal and iliac lymph ducts and lymph nodes.
Supplementary File S1 “1st Surgical-Radiological RoundTable for the Improvement of the Interdisciplinary Treatment of Patients with Postoperative Lymphatic Fistulas“—Agenda and preliminary results.
Note: Excerpt after editing some of the original data documented in the German language.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}