Abstract
The integration of Artificial Intelligence and Robotics (AI/R) in healthcare presents both opportunities and challenges, especially in developing countries. This study assessed the attitudes and perceptions of Vietnamese healthcare undergraduates towards AI/R applications in healthcare and elderly care. In 2023, a cross-sectional survey was conducted among 1221 Vietnamese healthcare undergraduates. The questionnaire covered demographic, academic, social, and mental factors, as well as attitudes towards AI/R applications measured by a five-level Likert scale. Key findings revealed that respondents were primarily majoring in medicine (60.9%) and pharmacy (29.4%). Awareness and interest in AI/R were high (89.9% and 88.3%, respectively), but formal training was significantly lacking (5.9%). A substantial majority (89.9%) expressed a need for AI/R training. Respondents perceived considerable benefits of AI/R, particularly in data synchronization (mean [M] = 3.83), workload reduction for medical staff (M = 3.79), and delivering multiple healthcare benefits (M = 3.82). Moderate concerns were noted regarding security and privacy (M = 3.46), potential over-reliance on technology (M = 3.43), and AI/R potentially replacing medical staff (M = 3.38). Overall, perceived benefits (M = 3.67) outweighed concerns (M = 3.38), (p < 0.001). Additionally, participants aware of AI/R and those planning to study abroad showed greater interest and training needs in AI/R. Higher GPA and self-esteem were associated with a greater interest in AI/R research. The study highlights a significant gap in formal AI/R training, not only in availability but also in the absence of structured, outcome-based curricula, despite the strong interest among healthcare students in acquiring knowledge and skills in this area. These findings suggest the need for enhanced educational programs to train healthcare students with the necessary competencies to apply AI/R technologies effectively.
1. Introduction
The rapid advancement of Artificial Intelligence (AI) and Robotics (R) is revolutionizing various sectors, including healthcare. Artificial Intelligence/Robotics (AI/R) applications in healthcare promise to enhance diagnostics, administrative tasks, and patient care by providing advanced tools for medical professionals [1,2]. However, the successful integration of these technologies into health systems, particularly in developing countries, poses significant challenges including limited infrastructure, legal liability concerns, data privacy issues, and a lack of adequately trained personnel [3,4,5] and requires a well-prepared workforce, especially in case of medical legal liability [6]. A systematic review about preferences for the use of AI in healthcare has shown that patients, the public, and professionals possessed a positive attitude towards AI healthcare applications [7].
AI/R is at the initial stage of being incorporated into medical education [8,9], but significant progress has only been made in recent years [10]. However, there is limited knowledge about integration of AI/R content into higher education training programs. A disparity has been reported between medical students’ enthusiasm and the training programs provided by the universities [11,12]. Despite the growing body of literature on AI/R in medical education, existing studies are disproportionately focused on medical students in high-income countries, leaving a significant gap in our understanding of how students in other health disciplines, such as nursing, pharmacy, and traditional medicine in low- and middle-income contexts, perceive and engage with these technologies.
Vietnam, like many developing countries, is experiencing a growing interest in incorporating AI/R into its healthcare infrastructure. This interest is driven by the potential benefits of AI/R, such as improving healthcare delivery, reducing the burden on medical staff, and addressing the needs of an aging population. Efforts have been taken in updating curricula with new trends and technologies [13].
Despite these promising prospects, there is limited research on the awareness, attitudes, and preparedness of healthcare students in Vietnam regarding AI/R technologies. Exploring these factors is essential for developing targeted education initiatives that can equip future health professionals with the necessary skills and knowledge to apply AI/R effectively. Taking these evidence gaps, in 2023, a pilot study on a small sample size was conducted on exploring interest and educational gap in AI/R usage for elderly care in healthcare undergraduates [14]. We hypothesized that background demographic, academic, mental, and social factors may contribute to the interest and training needs of AI/R (Figure 1). While the study confirmed a high level of interest and perceived need for training, its small sample size limited generalizability, and it did not detect significant associations between background characteristics and AI/R interest. These limitations highlighted the need for an expanded, more representative investigation to clarify influencing factors and support curriculum development. Based on previous findings and conceptual reasoning, we hypothesize the following: (H1) students with prior awareness of AI/R will report higher interest and training needs in AI/R; (H2) higher academic performance (Grade Point Average, GPA) and self-esteem will be positively associated with interest in AI/R and willingness to engage in AI/R-related research; (H3) students with plans to study abroad will report greater interest and perceived training needs in AI/R.
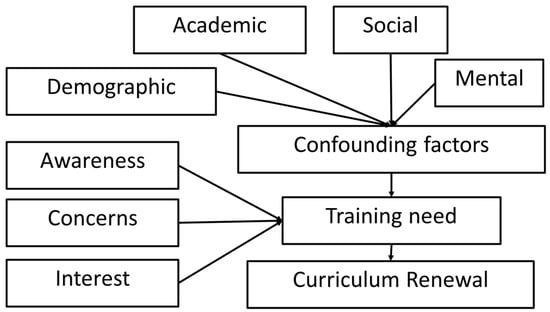
Figure 1.
Conceptual framework proposed by the authors.
The objectives of this study are as follows: (1) to explore their awareness and attitudes towards benefits and concerns of AI/R applications in healthcare; and (2) to identify their training needs and interest in AI/R-related research. The current study will provide insights into the current state of AI/R education among healthcare students in Vietnam. Additionally, it will highlight areas where educational interventions are needed to enhance students’ readiness to integrate AI/R technologies into their future professional practice. By addressing these educational gaps, this research aims to contribute to the development of a competent and technologically savvy healthcare workforce capable of meeting the demands of modern healthcare systems.
2. Materials and Methods
A cross-sectional survey was carried out with undergraduate students from a Vietnamese public university specialized in healthcare in 2023. The sample size was calculated using the Cochran formula for categorical data, assuming a 50% proportion for maximum variability, a 95% confidence level, and a 3% margin of error. This yielded a required sample size of 1067 students. Invitations were distributed via institutional email lists and in-class announcements, with access to the online survey (Google Forms) provided through a voluntary sign-up link. The responses were collected over a four-week period. All undergraduate students enrolled in health-related programs (including medicine, pharmacy, nursing, traditional medicine, preventive medicine, and medical technology) were eligible to participate. There were no exclusion criteria beyond voluntary consent. A total of 1500 students were invited to participate in the online survey, and 1221 completed the questionnaire, resulting in a response rate of 81.4%. The questionnaire was developed based on the one used in a previous pilot study [14], which was informed by the published literature on AI/R perceptions in medical education and itself was developed based on published instruments from studies examining AI in medical and healthcare education [6,9,11,12,15,16]. The adaptation process involved the following: (1) a targeted literature review to identify relevant constructs (awareness, interest, perceived benefits, concerns, attitudes towards elderly care applications, training needs, and socio-demographic/academic characteristics); (2) expert review by two health technology and medical education specialists to ensure content validity and alignment with study objectives; and (3) refinement for clarity, cultural appropriateness, and relevance to the Vietnamese healthcare education context. The instrument was reviewed by two education and health technology experts for content relevance and translated into Vietnamese using forward-backward translation. It was administered bilingually (English and Vietnamese) to support comprehension and inclusivity among participants. A pilot test with 30 students confirmed clarity, comprehension, and cultural appropriateness. Internal consistency was high across scales: Perceived Benefits (Cronbach’s α = 0.94), Concerns (α = 0.89), and Self-Esteem (α = 0.84).
The instrument consisted of six sections: (1) demographic, academic, and social characteristics; (2) mental factors measured by a four-point Likert scale based on the Rosenberg scale for assessing self-esteem [17]; (3) awareness, interest, and training experiences regarding AI/R; (4) perceived benefits of AI/R (8 items); (6) concerns about AI/R (5 items); and (6) attitudes toward AI/R applications in elderly care (20 items). All attitudinal items were measured on a five-point Likert scale, where 1 = Strongly Disagree, 2 = Disagree, 3 = Neutral, 4 = Agree, and 5 = Strongly Agree. GPA categories were self-reported based on the institutional grading scale and were interpreted by students as follows: Lower average (≤6.0), Average (6.1–6.9), Upper average (7.0–7.4), Good (7.5–7.9), Upper good (8.0–8.4), and Excellent (≥8.5) on a 10-point scale.
In the survey, AI/R was presented as a broad category encompassing both software-based AI systems and hardware-integrated robotics relevant to healthcare practice. To aid respondent comprehension and ensure consistent interpretation, the questionnaire provided concrete examples of AI applications—such as electronic medical record data synchronization, diagnostic decision support, patient monitoring, and medication reminders—and robotic applications—such as patient lifting, cleaning and sanitization, and automated food delivery. These examples were drawn from the existing literature on healthcare AI/R [3,7,18] and reflected use cases that are feasible or emerging in the Vietnamese healthcare context.
Descriptive statistics were used to analyze participant characteristics. Spearman’s correlation was employed to assess associations between independent variables and training interest in AI/R. A paired samples t-test was conducted to compare perceived benefits and concerns. Cronbach’s Alpha was calculated to evaluate internal consistency. All analyses were performed using IBM Statistical Package for the Social Sciences (SPSS) version 27. Descriptive statistics for Likert-scale items are reported as means (M) and standard deviations (SD), as the data were approximately normally distributed based on skewness and histogram inspection. For variables exhibiting mild skewness, both the mean and median are reported for completeness. Participants were informed about the study’s purpose, and participation was voluntary, confidential, and anonymous.
3. Results
The characteristics of the respondents are shown in Table 1. Two thirds (66.5%) of the participants are female. The highest group is in their 2nd year (50.7%). More respondents are majoring in medicine (60.9%) and pharmacy (29.4%). The most common GPA category is “Average” (30.7%), followed by “Upper average” (28.2%). Regarding English proficiency, 82.5% perceived to have a basic level, while 12.0% were studying a second foreign language besides English. Most of the population is unmarried (99.2%) and do not receive any scholarship (90.3%). Most live in rental accommodation, either alone (37.6%) or shared (32.9%). A significant portion do not have a part-time job (67.3%). The majority perceive their family income as middle-level (66.8%), with a notable portion perceiving it as low (32.7%). A large proportion do not plan to study abroad (44.3%), while 38.3% may consider it later. The average self-esteem score among the participants is 26.1 (average), with the median score slightly lower at 25.0, suggesting that the distribution is slightly skewed. The standard deviation of 3.10 indicates that the scores are relatively close to the mean. The reliability, measured by Cronbach’s Alpha (0.84), suggests that the scale is reliable in this population.

Table 1.
Participants demographic, academic, socioeconomical and mental characteristics (N = 1221).
Table 2 presents the respondents’ awareness, interest, training, and perceived training gaps related to AI/R in healthcare. A substantial proportion (89.9%) have heard about AI/R in healthcare, showing a high awareness. A large proportion (88.3%) of the participants expresses interest in AI/R in healthcare. Only a small part (5.9%) of the respondents have had training on AI/R in healthcare, indicating a gap in education. Moreover, a major part (89.9%) of the participants expresses a need for receiving AI/R healthcare training, showing a gap that they want to be addressed.
Table 2.
Awareness, interest, and training gaps (N = 1221).
Table 3 illustrates the perceived benefits of AI/R. Overall, respondents view AI/R as highly beneficial, particularly in terms of assisting with data synchronization inside hospitals and across networks (mean [M] = 3.83), which corresponds to a response between “Agree” and “Strongly Agree”. They also recognize that AI/R offer multiple advantages to healthcare (M = 3.82) and can significantly reduce the workload of medical staff (M = 3.79), enabling them to focus on specialized jobs.
Table 3.
Perceived benefits of AI/R (N = 1221).
Table 4 presents the concerns expressed by respondents regarding the use of AI/R in healthcare. The data reveals a moderate level of apprehension of several issues such as privacy and security of patients and themselves (M = 3.46), which falls between “Neutral” and “Agree”, indicating moderate concern, the potential for excessive reliance on technology affecting patient and healthcare staff autonomy (M = 3.43), and the possibility of AI/robotics replacing doctors and medical staff in the future (M = 3.38).
Table 4.
Concerns of AI/R (N = 1221).
Table 5 compares the perceived benefits versus concerns associated with the AI/R application in healthcare. Although respondents express an average level of concern (M = 3.38), the perceived benefits (M = 3.67) are significantly greater t(1220) = 12.94, p < 0.001, as indicated by a paired samples t-test (p < 0.001). The high internal consistency of the two scales indicates their reliability.
Table 5.
Comparison of perceived benefits and concerns (N = 1221).
Table 6 suggests that participants who have heard about AI/R and who plan to study abroad tend to have interest and training needs and want to do research on AI/R. Individuals with higher GPAs tend to want to pursue research about AI/R. Participants with higher self-esteem also tend to become interested in AI/R and want to conduct research on AI/R. The results show no significant relationship of sex, grade, major, language proficiency, marital and living status, or income and part-time job.
Table 6.
Associations of the AI/R needs with various factors (N = 1221).
The data on respondents’ attitudes towards elderly care applications of AI/R highlights the most favored functionalities in these technologies (Table 7). Among AI applications, the highest mean scores are seen in tasks such as supporting the turning on and off of lights and surrounding electronic devices (M = 3.76), reminding patients according to specific schedules like taking medicine (M = 3.75), providing useful information about weather, news, and community services for patients (M = 3.75), and supporting communication with doctors or medical staff (M = 3.75). These scores indicate a strong preference for AI in enhancing convenience, ensuring timely reminders, providing valuable information, and facilitating communication for the elderly. For robotics applications, the top-rated functionalities include supporting the lifting of heavy objects (M = 3.74), cleaning and sanitizing patient room spaces or homes (M = 3.73), and delivering food to patients (M = 3.70). This suggests a significant reliance on robotics for physical tasks that aid in the daily living and health maintenance of elderly individuals. Overall, the data underscores a positive attitude towards incorporating both AI/R in elderly care, with AI excelling in informational and reminder functions, while robotics is favored for physical assistance.
Table 7.
Attitude towards elderly care applications of AI/R (N = 1221).
4. Discussion
4.1. Awareness and Interest in AI/R
The findings of the current study indicate a high level of awareness (89.9%) and interest (88.3%) among respondents regarding AI/R in healthcare. This finding is consistent with numerous studies conducted on students with different majors in various countries [6,11,15,19,20]. This widespread awareness suggests that information about AI/R technologies is effectively reaching the healthcare student population. The substantial interest underscores the perceived potential and relevance of these technologies in the future of healthcare. Compared to counterparts in high-income countries, Vietnamese students appear to report even stronger enthusiasm for AI/R despite receiving less formal training. This contrast highlights a global inequity in AI/R education access, as students in lower-resource settings may be more eager to adopt innovations but lack institutional infrastructure or curricular offerings to do so effectively [6,15].
4.2. Training and Perceived Training Needs
Our results show that despite the high levels of awareness and interest, only a small fraction (5.9%) of respondents have received formal training in AI/R, highlighting a significant gap in the current educational curriculum. The overwhelming majority (89.9%) expressing a need for AI/R training suggests that students recognize the importance of these skills and are eager to bridge this gap. This position aligns with existing evidence regarding the gaps in medical education [12]. These training gaps have also been reported among undergraduate medical students [15,21], nursing students [22], pharmacy students [16], graduate students [11] and professionals [20] from various settings. In all, 66.4% of respondents believed that AI should be taught at the undergraduate level [11,23]. This finding points to a need for educational institutions to revise and integrate AI/R training into their training curricula [9]. This is consistent with the prevailing trend that medical education should evolve to embrace the era of AI [24].
4.3. Perceived Benefits and Concerns of AI/R in Healthcare
Respondents perceive considerable benefits from AI/R technologies, particularly in data synchronization (M = 3.83), enhancing multiple healthcare aspects (M = 3.82), and reducing the workload of medical staff (M = 3.79). These perceptions align with the potential of AI/R to streamline healthcare operations and improve efficiency, allowing medical staff to focus on more complex and critical tasks. This positive perception is well aligned with the existing research literature [7]. Moreover, students believed that AI would benefit their careers [25].
Previous studies have revealed commonly perceived risks included data privacy, reduced work autonomy, algorithmic bias, health inequities, and greater workload to acquire AI skills [7].The current study reveals moderate concerns regarding the security and privacy of patients (M = 3.46), potential over-reliance on technology (M = 3.43), and the fear of AI/R replacing medical staff (M = 3.38). The found low concern about legal liability in case of a medical error is consistent with a previous report [6]. These concerns reflect the need for addressing ethical and practical implications of AI/R implementation to ensure that these technologies augment rather than diminish the role of healthcare professionals. These results align with the fact that healthcare professionals generally view AI positively. The applications of AI in healthcare present promising opportunities but also introduce challenges [26].
It has been reported that students see AI as a partner rather than a competitor [25], and professionals indicated that AI would not replace them in their profession [7]. The comparison of perceived benefits (M = 3.67) and concerns (M = 3.38) reveals that the benefits of AI/R outweigh the concerns (p < 0.001). This positive balance suggests a generally favorable attitude towards AI/R adoption among healthcare students, provided that their concerns are adequately addressed through proper guidelines and safeguards. This result is consistent with a previous pilot study [14]. This optimism may reflect aspirational thinking among students who view technology as a vehicle for innovation and improved patient care. In the Vietnamese context, strong national messaging around digital transformation and the modernization of healthcare may further shape these favorable perceptions. Students likely associate AI/R with professional opportunity more than disruption, particularly in a setting where healthcare resources remain stretched and automation is often framed as a solution.
4.4. Factors Influencing Interest and Training Needs
The data show that participants who have prior awareness of AI/R and those planning to study abroad exhibit higher interest and training needs in AI/R. Higher GPA and self-esteem are also associated with greater interest and desire to engage in AI/R research. These associations highlight the influence of academic and personal factors on students’ attitudes towards AI/R, suggesting targeted strategies for enhancing AI/R education among different student demographics. These findings add new perspectives about the current literature. It has been reported that income, educational background, and experience with technologies were predictors of attitude of pharmacy students toward using AI in pharmacy practice [16]. Among nursing students, factors associated with students’ readiness to apply AI included hi-tech proficiency, knowledge of AI fundamentals, and perceived AI application in nursing practice [22]. It also has been reported that knowledge of healthcare students significantly differed depending on gender, major, experience, and income. The positive attitudes vary by year level and income, and the proportion with favorable perspectives regarding AI varies by age and major [25].
4.5. Attitudes Towards AI/R in Elderly Care
The analysis of attitudes towards AI/R applications in elderly care reveals a strong preference for AI in tasks that enhance convenience and communication, such as turning on/off lights (M = 3.76), reminding patients to take medicine (M = 3.75), and providing information (M = 3.75). Robotics, on the other hand, are favored for physical assistance tasks like lifting heavy objects (M = 3.74), cleaning (M = 3.73), and delivering food (M = 3.70). These preferences indicate the complementary roles of AI/R in supporting elderly care, with AI excelling in informational and reminder functions and robotics in physical tasks. These findings consolidate the high interest in applying robotics for elderly care [18] as well as receiving training on this new discipline [27].
To address the educational gap, we recommend a multi-tiered approach to AI/R training in healthcare curricula. Introductory elective courses on AI fundamentals could be offered in the early years of study, while more advanced online modules and case-based simulations could be incorporated in clinical years. Simulation-based training and interdisciplinary workshops involving computer science and healthcare faculties may also foster practical understanding. These modular approaches offer flexibility and scalability, particularly in resource-limited settings, and align with emerging best practices in digital health education [9,11].
The current study suggests a critical opportunity for Vietnamese health education institutions to act proactively. Integrating AI/R content through elective courses, interdisciplinary workshops, and online learning modules would address the evident student demand. Moreover, embedding AI/R training across both foundational and clinical years would support skill development aligned with future healthcare needs.
This research has limitations. The cross-sectional design captures perceptions at a single point in time, which may not reflect changes over time or the impact of ongoing educational interventions. As the study was conducted at a single university in Vietnam, the findings may not be generalizable to all healthcare student populations in Vietnam or other countries. Institutional culture, curriculum differences, and regional technological exposure may influence students’ perceptions and needs. While multivariable regression would provide deeper insight into independent predictors of AI/R engagement, it was not performed in this exploratory study due to limited outcome variance and unbalanced categorical predictors. The findings should therefore be interpreted as preliminary associations rather than causal relationships. Future studies should aim to include multi-institutional samples for broader representation. Additionally, self-reported data may have biases. The absence of qualitative data limits our ability to explore deeper motivations or contextual factors underlying students’ perceptions. Finally, while the study highlights the need for AI/R training, it does not assess the specific content or effectiveness of existing curricula, leaving a gap in understanding how best to implement AI/R education in healthcare programs.
5. Conclusions
This study highlights the significant interest and awareness among Vietnamese undergraduates regarding AI/R applications in healthcare, despite a notable gap in formal training. The findings reveal a strong perceived need for AI/R education, with students expressing enthusiasm for integrating these technologies into their future practice. The disparity between students’ interest and the current educational offerings underscores the urgent need for universities to enhance their curricula to include comprehensive AI/R training. By addressing this gap, educational institutions can better prepare future healthcare professionals to effectively utilize AI/R technologies, ultimately improving healthcare delivery and patient outcomes. This study provides valuable insights for policymakers and educators aiming to develop targeted strategies for integrating AI/R into healthcare education.
In light of these findings, healthcare curricula in Vietnam and similar contexts could integrate both foundational and application-specific AI/R content. Foundational modules might include AI fundamentals, data analytics, machine learning principles, and ethics of AI in healthcare, while applied modules could address specific technologies such as clinical decision-support systems, medical imaging AI, hospital automation tools, and patient-assistive robotics for elderly care. To ensure effective learning, pedagogical practices should combine didactic lectures with experiential methods, including simulation-based training using AI-enabled platforms, case-based learning with real-world clinical scenarios, and interdisciplinary workshops involving healthcare, computer science, and engineering faculties. Embedding these components into both pre-clinical and clinical stages would help students build not only technical competence but also critical judgment in applying AI/R responsibly in practice. Such curriculum reform can bridge the current training gap and prepare future healthcare professionals to lead the safe and effective adoption of AI/R technologies.
Author Contributions
Conceptualization, N.B.D. and N.H.T.; methodology, N.B.D., Q.N.P. and N.H.T.; software, N.B.D. and N.H.T.; validation, all authors; formal analysis, all authors; investigation, N.B.D. and Q.N.P.; resources, all authors; data curation, N.B.D. and N.H.T.; writing—original draft preparation, N.B.D. and N.H.T.; writing—review and editing, all authors; visualization, N.H.T. and N.B.D.; supervision, N.H.T.; project administration, N.B.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethical Committee of Thai Binh University of Medicine and Pharmacy (No. 926 on 7 September 2023). Participation was entirely voluntary. Informed consent was obtained electronically, students were shown an information sheet explaining the purpose, risks, and confidentiality of the study, and were required to check an “I agree to participate” box before accessing the survey. To ensure confidentiality in the online format, no personal identifiable information was collected. The Google Forms platform was configured to avoid logging email addresses or IP addresses. Data were stored on a password-protected institutional server accessible only to the research team.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study when they checked the agree button on the online survey form.
Data Availability Statement
The data presented in this study are available from the corresponding author via reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AI | Artificial Intelligence |
| R | Robotics |
| AI/R | Artificial Intelligence and Robotics |
| GPA | Grade Point Average |
| SD | Standard Deviation |
| SPSS | Statistical Package for the Social Sciences |
References
- Bohr, A.; Memarzadeh, K. Chapter 2—The Rise of Artificial Intelligence in Healthcare Applications. In Artificial Intelligence in Healthcare; Bohr, A., Memarzadeh, K., Eds.; Academic Press: Cambridge, UK, 2020; pp. 25–60. [Google Scholar] [CrossRef]
- Yoon, S.N.; Lee, D. Artificial Intelligence and Robots in Healthcare: What Are the Success Factors for Technology-Based Service Encounters? Int. J. Healthc. Manag. 2019, 12, 218–225. [Google Scholar] [CrossRef]
- Broadbent, E.; Kuo, I.H.; Lee, Y.I.; Rabindran, J.; Kerse, N.; Stafford, R.; MacDonald, B.A. Attitudes and Reactions to a Healthcare Robot. Telemed. e-Health 2010, 16, 608–613. [Google Scholar] [CrossRef]
- Hamet, P.; Tremblay, J. Artificial Intelligence in Medicine. Metabolism 2017, 69, S36–S40. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.; Allan, S.; Coghlan, S.; Cooper, P. A Governance Model for the Application of AI in Health Care. J. Am. Med. Inform. Assoc. 2019, 27, 491–497. [Google Scholar] [CrossRef] [PubMed]
- AlZaabi, A.; AlMaskari, S.; AalAbdulsalam, A. Are Physicians and Medical Students Ready for Artificial Intelligence Applications in Healthcare? Digit. Health 2023, 9, 20552076231152167. [Google Scholar] [CrossRef]
- Vo, V.; Chen, G.; Aquino, Y.S.J.; Carter, S.M.; Do, Q.N.; Woode, M.E. Multi-Stakeholder Preferences for the Use of Artificial Intelligence in Healthcare: A Systematic Review and Thematic Analysis. Soc. Sci. Med. 2023, 338, 116357. [Google Scholar] [CrossRef] [PubMed]
- Masters, K. Artificial Intelligence in Medical Education. Med. Teach. 2019, 41, 976–980. [Google Scholar] [CrossRef]
- Paranjape, K.; Schinkel, M.; Nannan Panday, R.; Car, J.; Nanayakkara, P. Introducing Artificial Intelligence Training in Medical Education. JMIR Med. Educ. 2019, 5, e16048. [Google Scholar] [CrossRef]
- Chan, K.S.; Zary, N. Applications and Challenges of Implementing Artificial Intelligence in Medical Education: Integrative Review. JMIR Med. Educ. 2019, 5, e13930. [Google Scholar] [CrossRef]
- Stewart, J.; Lu, J.; Gahungu, N.; Goudie, A.; Fegan, P.G.; Bennamoun, M.; Sprivulis, P.; Dwivedi, G. Western Australian Medical Students’ Attitudes towards Artificial Intelligence in Healthcare. PLoS ONE 2023, 18, e0290642. [Google Scholar] [CrossRef]
- Machleid, F.; Kaczmarczyk, R.; Johann, D.; Balčiūnas, J.; Atienza-Carbonell, B.; von Maltzahn, F.; Mosch, L. Perceptions of Digital Health Education Among European Medical Students: Mixed Methods Survey. J. Med. Internet Res. 2020, 22, e19827. [Google Scholar] [CrossRef]
- Duong, D.B.; Phan, T.; Trung, N.Q.; Le, B.N.; Do, H.M.; Nguyen, H.M.; Tang, S.H.; Pham, V.A.; Le, B.K.; Le, L.C.; et al. Innovations in Medical Education in Vietnam. BMJ Innov. 2021, 7, S23–S29. [Google Scholar] [CrossRef]
- Tran, H.; Phan, N.; Nguyen, T.; Nguyen, T.; Pham, T.; Dang, B. Assessing Interest and Educational Gaps in AI and Robotics Applications for Elderly Care Among Healthcare Students. In Proceedings of the Asian Conference on Aging & Gerontology 2024, Tokyo, Japan, 25–29 March 2024; pp. 1–7. [Google Scholar] [CrossRef]
- Pucchio, A.; Rathagirishnan, R.; Caton, N.; Gariscsak, P.J.; Del Papa, J.; Nabhen, J.J.; Vo, V.; Lee, W.; Moraes, F.Y. Exploration of Exposure to Artificial Intelligence in Undergraduate Medical Education: A Canadian Cross-Sectional Mixed-Methods Study. BMC Med. Educ. 2022, 22, 815. [Google Scholar] [CrossRef] [PubMed]
- Hasan, H.E.; Jaber, D.; Al Tabbah, S.; Lawand, N.; Habib, H.A.; Farahat, N.M. Knowledge, Attitude and Practice among Pharmacy Students and Faculty Members towards Artificial Intelligence in Pharmacy Practice: A Multinational Cross-Sectional Study. PLoS ONE 2024, 19, e0296884. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M. Rosenberg Self-Esteem Scale (RSES). APA PsycNet. Available online: http://psycnet.apa.org/doi/10.1037/t01038-000 (accessed on 1 May 2025).
- Allouch, S.B.; van Velsen, L. Social Robots for Elderly Care: An Inventory of Promising Use Cases and Business Models. Stud. Health Technol. Inform. 2020, 270, 1046–1050. [Google Scholar] [CrossRef]
- Pinto Dos Santos, D.; Giese, D.; Brodehl, S.; Chon, S.H.; Staab, W.; Kleinert, R.; Maintz, D.; Baeßler, B. Medical Students’ Attitude towards Artificial Intelligence: A Multicentre Survey. Eur. Radiol. 2019, 29, 1640–1646. [Google Scholar] [CrossRef]
- Yun, D.; Xiang, Y.; Liu, Z.; Lin, D.; Zhao, L.; Guo, C.; Xie, P.; Lin, H.; Liu, Y.; Zou, Y.; et al. Attitudes towards Medical Artificial Intelligence Talent Cultivation: An Online Survey Study. Ann. Transl. Med. 2020, 8, 708. [Google Scholar] [CrossRef]
- Alwadani, F.A.S.; Lone, A.; Hakami, M.T.; Moria, A.H.; Alamer, W.; Alghirash, R.A.; Alnawah, A.K.; Hadadi, A.S. Attitude and Understanding of Artificial Intelligence Among Saudi Medical Students: An Online Cross-Sectional Study. J. Multidiscip. Healthc. 2024, 17, 1887–1899. [Google Scholar] [CrossRef]
- Labrague, L.J.; Aguilar-Rosales, R.; Yboa, B.C.; Sabio, J.B. Factors Influencing Student Nurses’ Readiness to Adopt Artificial Intelligence (AI) in Their Studies and Their Perceived Barriers to Accessing AI Technology: A Cross-Sectional Study. Nurse Educ. Today 2023, 130, 105945. [Google Scholar] [CrossRef]
- Habib, M.M.; Hoodbhoy, Z.; Siddiqui, M.A.R. Knowledge, Attitudes, and Perceptions of Healthcare Students and Professionals on the Use of Artificial Intelligence in Healthcare in Pakistan. PLOS Digit. Health 2024, 3, e0000443. [Google Scholar] [CrossRef]
- Wartman, S.A.; Combs, C.D. Medical Education Must Move From the Information Age to the Age of Artificial Intelligence. Acad. Med. 2018, 93, 1107–1109. [Google Scholar] [CrossRef] [PubMed]
- Truong, N.M.; Vo, T.Q.; Tran, H.T.B.; Nguyen, H.T.; Pham, V.N.H. Healthcare Students’ Knowledge, Attitudes, and Perspectives toward Artificial Intelligence in the Southern Vietnam. Heliyon 2023, 9, e22653. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Yoon, S.N. Application of Artificial Intelligence-Based Technologies in the Healthcare Industry: Opportunities and Challenges. Int. J. Environ. Res. Public Health 2021, 18, 271. [Google Scholar] [CrossRef]
- Krückeberg, J.; Beume, D.P.; Klawunn, R.; Müller, J.; Griga, L.; Winkelhake, L.; Eich, L.; Kempe, N.; Albayrak, E. First Contact, First Learnings—Nursing Staff Approaching Robotics in Health Care. Stud. Health Technol. Inform. 2023, 302, 470–471. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Academic Society for International Medical Education. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).