Abstract
Recently, study abroad and elective programs have been facilitated via university partnerships based on student-exchange agreements. This study examined international medical student exchange agreements, focusing on reciprocity and stratification in the Japanese context. An empirical analysis was conducted using 581 agreements involving student exchanges with medical institutions in foreign countries based on a survey conducted by the Japanese Ministry of Education. We found that the average reciprocity rate via mutual tuition waivers was 52.84%: equivalent in Asia, slightly lower in Europe (49.61%), and higher in North America (58.06%). Europe has a balanced inbound and outbound exchange, Asia has a higher inbound exchange, and North America has an excess of outbound exchange from Japan. Moreover, selective institutions, such as former imperial or medical universities, have more than twice the number of agreements per university compared to others. In conclusion, it can be observed that international medical university partnerships are stratified, and reciprocity is intertwined with tuition waivers and the number of exchange students in the partnering institutions. As the results highlight the distinct characteristics of international education partnerships in Japan’s medical field compared to partnerships in all academic fields, it is necessary to investigate and develop international partnerships separately by field.
1. Introduction
The international mobility of physicians has recently gained global attention [1,2], largely because of its direct impact on national and regional healthcare systems, as well as the various political and socioeconomic issues involved in the international mobility of highly skilled workers. International experiences for individual physicians, including studying abroad and elective medical training, are also considered significant for the personal development of adolescent physicians and medical students [3]. Among the various study abroad programs in the medical field, student exchange programs are regarded as a powerful strategy for the further development of international education [4].
Recently, studying abroad and participating in international elective programs have been facilitated using university partnerships. For instance, Japan has witnessed an increase in the number of medical students participating in study abroad or elective programs, with over 60% of students participating using international agreements. This number increased from 55.8% in the Academic Year (AY) 2010 to 63.13% in AY 2011–2013 [5]. Before COVID-19, in AY 2018, 61.26% of outbound students from Japan, across all fields, studied at overseas universities and institutions via university agreements [6]. Given that such international agreements determine the characteristics of international exchange, including destination, number of students, duration, and study content, they inherently affect the quantity and quality of international medical education.
Despite their importance, to the best of the author’s knowledge, no previous studies have analyzed international medical student exchange agreements on a national scale. This may be due to relatively new attention to institutional-level analysis, as stated below, and difficulties in data collection. Given that Japan’s Ministry of Education, Culture, Sports, Science, and Technology (MEXT) has surveyed national universities’ (excluding distance learning universities and junior colleges) international exchange agreements with overseas institutions since AY 2007, this study empirically investigates international medical partnerships among universities using Japan as a case study. The actual use of these international agreements is also a matter of concern; in many cases, student exchanges do not occur under the relevant agreements. Furthermore, the higher education community tends to consider the number of partnerships as a symbol of success rather than valuing quality [7,8]. While there has been a strategic trend in recent years toward reducing the number of partnerships to focus on quality, the perspective that quantity is more important still persists [8].
The characteristics of internationalization in higher education have evolved in response to social changes over time [9]. This includes a shift from traditional concepts of mutual benefits between universities to commercialization and self-interest [8]. Reciprocity has traditionally been a significant concept in international partnerships, but it is usually not defined in university partnerships. Some scholars have defined reciprocity as the balance between the number of outbound and inbound students [10], whereas others have considered the existence of agreements and local needs as indicators of reciprocity [11]. Meanwhile, one study regarded mutuality in international partnerships at Cambodian universities as equity, autonomy, solidarity, and participation [12], while another saw the mutual waiver of tuition as an indicator of reciprocity [13]. Considering the availability of data, previous studies’ definitions, and the context of Japan, this study defines reciprocity as a waiver of tuition and a balance in the number of outbound and inbound students.
Previous studies have highlighted two tendencies in medical inter-university partnerships: they are not always mutually beneficial [10], and the nature of international exchanges by United States universities varies depending on the region of the partner, with reciprocity being stronger when the partner has more resources [11]. In Japan’s case, reciprocity in partnerships targeting all fields is higher in non-English speaking countries compared to English-speaking countries, indicating little correlation to partners’ resources [13]. Medical partnerships in Japan may align with the overall trends observed in Japan or with the trends observed in medical partnerships in other countries.
Increased attention is currently being paid to institutional stratification in students’ international exchange, representing a relatively new perspective; previous studies have primarily analyzed this topic from either a micro or macro perspective [14]. Institutional stratification is the arrangement of universities into strata dependent on their category, mission, academic standards, prestige, financing methods, or the number of stakeholders. Recently, stratification can also be observed in universities’ international partnerships. As expected, higher-tier universities tend to have better international partnerships, including longer durations of studying abroad and a greater number of credit-bearing programs [13]. There are more instances of studying abroad among national universities compared to private universities, and this gap has widened since 2010 [15]. Japanese medical schools are also stratified by ranking and selectivity, as long-established institutions generally hold higher rankings, with a few exceptions for universities located in metropolitan areas such as Tokyo [16]. Top-tier universities may have had more time to establish international partnerships and are attractive partners for foreign institutions.
Based on these considerations, the main objective of this study is to examine and clarify international medical student exchange agreements in Japanese universities, with a particular focus on reciprocity and stratification. To mitigate the influence of the COVID-19 pandemic, this study specifically focused on agreements in the AY 2017, which served as the basis for student mobility in AY 2018, representing the period with the largest number of international students before the pandemic.
The research questions of this study are as follows:
- -
- What are the characteristics of international medical exchange agreements in Japan?
- -
- How is reciprocity manifested in these agreements?
- -
- How does stratification among Japanese universities affect the characteristics of international medical exchange agreements?
By addressing these research questions, this study aims to provide insights into the nature of international medical student exchange agreements in Japan, including their characteristics (whether they are actively used or not) and reciprocity, as well as the relationship with institutional stratification.
1.1. Japan’s Higher and Medical Education
In AY 2021, 54.9% of Japanese high school graduates enrolled in universities for four or more years of study. These universities can be categorized into three types: national, municipal, and private. National universities are established by the Japanese national government, municipal universities by the regional government, and private universities by individuals or education-incorporated institutions. The number of universities in each category was 86, 98, and 619, respectively [17]. Given that private universities account for almost three-quarters of the total, it can be said that financial support for Japanese higher education primarily comes from students’ families. University selection in Japan is influenced by factors such as university type, history, and size. The Research 11 Consortium, which includes nine national and two private universities with long histories and large student populations, represents the leading research universities in Japan. Among the nine national universities are seven former imperial universities, which had been established by the 1886 Imperial University Ordinance and are regarded as the most selective and comprehensive research-type universities in Japan.
There are 82 universities with medical schools in Japan offering six-year medical education programs. In 2017, approximately 9420 students enrolled in medical schools, accounting for 2.18% of the total undergraduate enrollment that academic year. An average of 116 new medical students enrolled in the medical schools. Medical education is a popular choice among prospective students in Japan due to the prestige and high income associated with the medical profession. While tuition costs for medical education vary depending on university type, national and municipal universities have comparable costs. On average, the cost of a six-year medical education program is approximately 4 million yen (approximately 30,880 US dollars, when the exchange rate is 1 USD to 129.5 JPY as of January 2023). Private universities’ tuition costs are generally 5–12 times higher than those of public universities. Consequently, students at public universities may have more financial resources to pursue study-abroad opportunities compared to students at private universities, all other things being equal.
1.2. International Student Exchange in Japan
Since its establishment in the 1880s, modern Japanese higher education was internationalized; it became domesticated over time, with the transition from foreign language instruction and staff to Japanese. However, since the 2000s, Japanese universities have actively promoted internationalization in response to globalization, following the trends observed in other advanced countries [18]. The increase in internationalization efforts can be attributed to government initiatives, with several related policies focusing on both inbound and outbound student and faculty mobility. While government initiatives for the internationalization of higher education have increased, they are often directed toward larger universities [19].
In terms of student mobility, there remains an imbalance between inbound and outbound students in Japan. Prior to COVID-19, in AY 2018, the number of inbound students studying at Japanese higher education institutions was approximately twice that of outbound students (208,901 inbound students compared to 115,146 outbound students from Japanese universities) [20,21].
Japan’s study abroad trends are changing, with their duration and destinations becoming more diversified, including shorter terms and a higher number of Asian destination countries [17]. Recent years have seen a remarkable increase in outbound short-term study abroad programs in Japan [22]. Consequently, the number of exchange programs that do not involve credit transfers or tuition fees may have increased. An analysis of exchange agreements across all Japanese universities revealed lower reciprocity in English-speaking countries. Furthermore, it showed stratification in the agreements among Japanese universities, with higher agreement quantity and quality observed among top-tier Japanese universities [13].
2. Materials and Methods
The MEXT conducted a survey of international agreements between overseas institutions and Japanese universities, excluding correspondence universities, open universities, and junior colleges. Its data include various agreements involving research arrangements or staff and student exchange between one Japanese institution and one overseas institution at either the university or departmental level. As this study focuses on the partnership between institutions, the data were changed to a one-to-one correspondence between Japanese universities and their partners.
Identifying agreements by medical schools in Japanese comprehensive universities was challenging because many Japanese universities with medical schools do not include the words “medicine” in their names, and there were no flags for agreements conducted by medical schools. Therefore, the author extracted agreements that included “Medicine” or “Medical Science” in the name of the partner foreign institutions and excluded data from institutions with words like “Veterinary”, “Nursing”, “Pharmacy”, “Dentistry”, and “Oral Medicine”, to focus on the medical field. Agreements from Japanese universities without medical departments were also excluded. As a result, 628 agreements fit the above conditions, and among them, 581 (2.06% of all agreements after one-to-one correspondence) involved student exchange, leaving 27,608 agreements that did not meet these criteria. While 81 universities had medical schools in AY 2017, only 75 were included in the dataset.
Then, a selectivity index was added to the data based on the information on the deviation scores of medical schools from the entrance exams or tests conducted by the cram schools Sundai and Kawaijuku (the latest version in 2022). Medical schools were also classified according to selectivity [16] to investigate the stratification of agreements into four categories for public universities and three categories for private universities. The number of universities per category varied from 3 to 19. The National Defense Medical College was included in the overall analysis but not in the analysis by founder category because it was not classified in the founder category or selectivity.
The accuracy of the dataset was verified using the agreements of the school/graduate school of medicine at Nagoya University, a national research university, as an example. As of 11 June 2022, the number of agreements displayed on their homepage was 39, more than double that of the 19 institutions included in this study’s dataset. Approximately half of the institutions were not included in the dataset because the partner institutions listed on the homepage did not have “Medicine” in their names, such as the Chinese University of Hong Kong. Institutions that signed agreements after 2018 were also listed on the homepage but were not included in the dataset. Therefore, the number of agreements included in this study could be small, and it would be more appropriate to investigate the proportion rather than the actual number.
There are two specific advantages in comparing international education partnerships in all fields with those in the medical field. First, it helps better understand the characteristics of international agreements in the medical field. Second, it highlights the existence of field-specific differences. For example, students studying STEM subjects are generally less likely to participate in study-abroad programs compared to those in the humanities and social sciences [23]. Differences in agreements between medical and other fields indicate the need to investigate and develop international partnerships separately for different fields.
3. Results
3.1. Regions and Reciprocity of Tuition Waiver
The breakdown of the 581 agreements by type shows that national universities account for the majority at 76.25%, municipal universities at 4.13%, and private universities at 19.62%. The proportion of Japanese medical schools by founder type was 51.85% for national universities, 9.88% for public universities, and 38.27% for private universities. In comparison, the proportion of national universities in the number of agreements is approximately 25% points higher than that of medical schools, whereas both municipal and private universities have proportions that are roughly half that of medical schools. This indicates that national universities have more agreements than municipal or private universities.
The basic statistics are presented in Table 1. There are eight categories for the region. The average number of outbound students per agreement is 1.76, whereas that of inbound students is 1.54. The average number of students with credits per agreement ranges from 0.27 to 0.72, indicating a certain proportion of agreements without any student exchange. The maximum number of students per agreement is mostly over 30, suggesting the presence of agreements with significant utilization and outcomes.

Table 1.
Basic statistics.
Table 2 presents the number of agreements and the ratio of tuition waivers by region and country. In terms of regions, Asia has the largest proportion, accounting for 60.59%, followed by Europe at 21.86% and North America at 10.67%. Together, these three regions make up over 93% of the total. The top three countries with the largest number of agreements are China, the U.S., and Taiwan, accounting for 24.78%, 9.64%, and 8.09%, respectively, while seven of the top 10 countries with the largest number of agreements are from Asia. The three non-Asian countries are the U.S., Russia, and Germany.
Table 2.
Numbers of agreements and rate of mutual tuition waiver by region and country.
The average tuition waiver rate is 52.84%, which is the same in Asia, slightly lower in Europe (49.61%), and higher in North America (58.06%). The trends for medical school agreements differ from those of overall Japanese agreements in all academic fields, with an average tuition waiver rate of 57.26%, the same as in Asia, higher in Europe (64.35%), and lower in North America (48.07%) [13]. The tuition waiver rate for medical school agreements is approximately 5% points lower in Asia, 15% points lower in Europe, and 10% higher in North America.
Tuition reciprocity rates vary among the top 10 countries. In the Asian region, Taiwan and South Korea have rates exceeding 60%, while China (47.92%), Mongolia (43.75%), and Vietnam (31.43%) have lower rates. All three non-Asian countries (U.S., Russia, and Germany) have rates exceeding 60%.
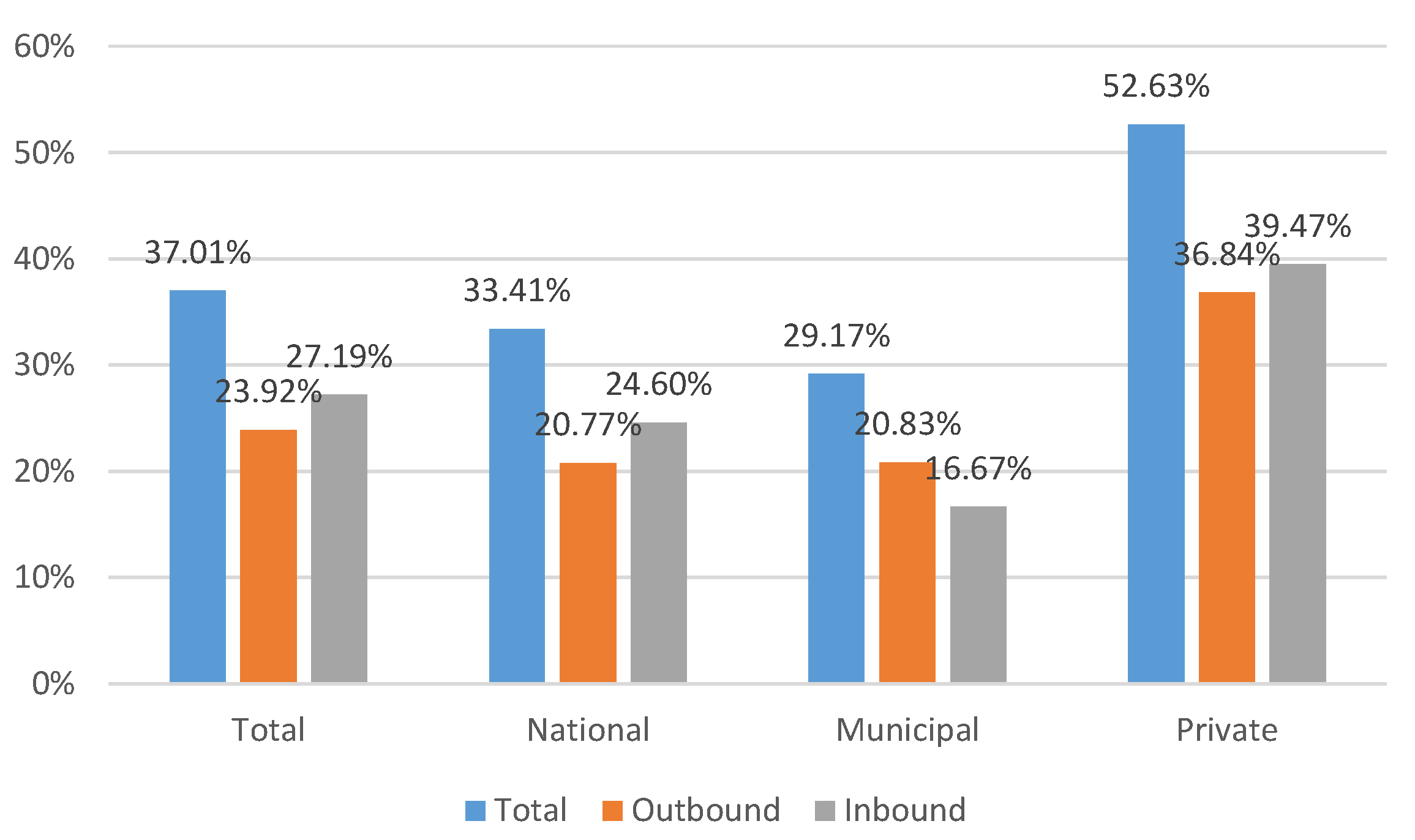
The proportion of agreements actively used for student exchange, as indicated by the proportion of agreements with at least one outbound or inbound exchange student in AY2017, is presented in Figure 1 by founder type and in Figure 2 by region. It must be noted that the present data on exchange students include both undergraduate and graduate students. However, most of the exchanges involve clinical practice at the undergraduate level, with fewer exchanges at the graduate level. In Figure 1, the average usage rate is 37.01%, although the rate is less than 30% for both inbound (27.19%) and outbound (23.92%). When comparing university types, notable differences are observed between public (national and municipal) and private institutions for both inbound and outbound exchanges. The utilization rate for public institutions is approximately 30% (33.41% for national and 29.17% for municipal), whereas that for private institutions is 52.63%. In terms of the balance between inbound and outbound exchange, the rate of inbound exchange is slightly higher for both national and private institutions, while the rate of outbound exchange is higher only for municipal institutions.

Figure 1.
Rate of agreement utilization by founder types.

Figure 2.
Rate of agreement utilization by major region.
In Figure 2, the total proportion of active agreements is higher in North America at 51.61%, whereas that of Asia and Europe is approximately 35% (33.52 for Asia and 37.01 for Europe). Inbound exchanges show little difference among the three regions, ranging from approximately 26% to 28%. However, the outbound exchange rate varies regionally. It is approximately 10% lower than the rate of inbound exchange in Asia, relatively balanced in Europe, and almost double in North America. Figure 3 indicates that Japanese universities use their agreements differently by region, emphasizing outbound exchange in North America.

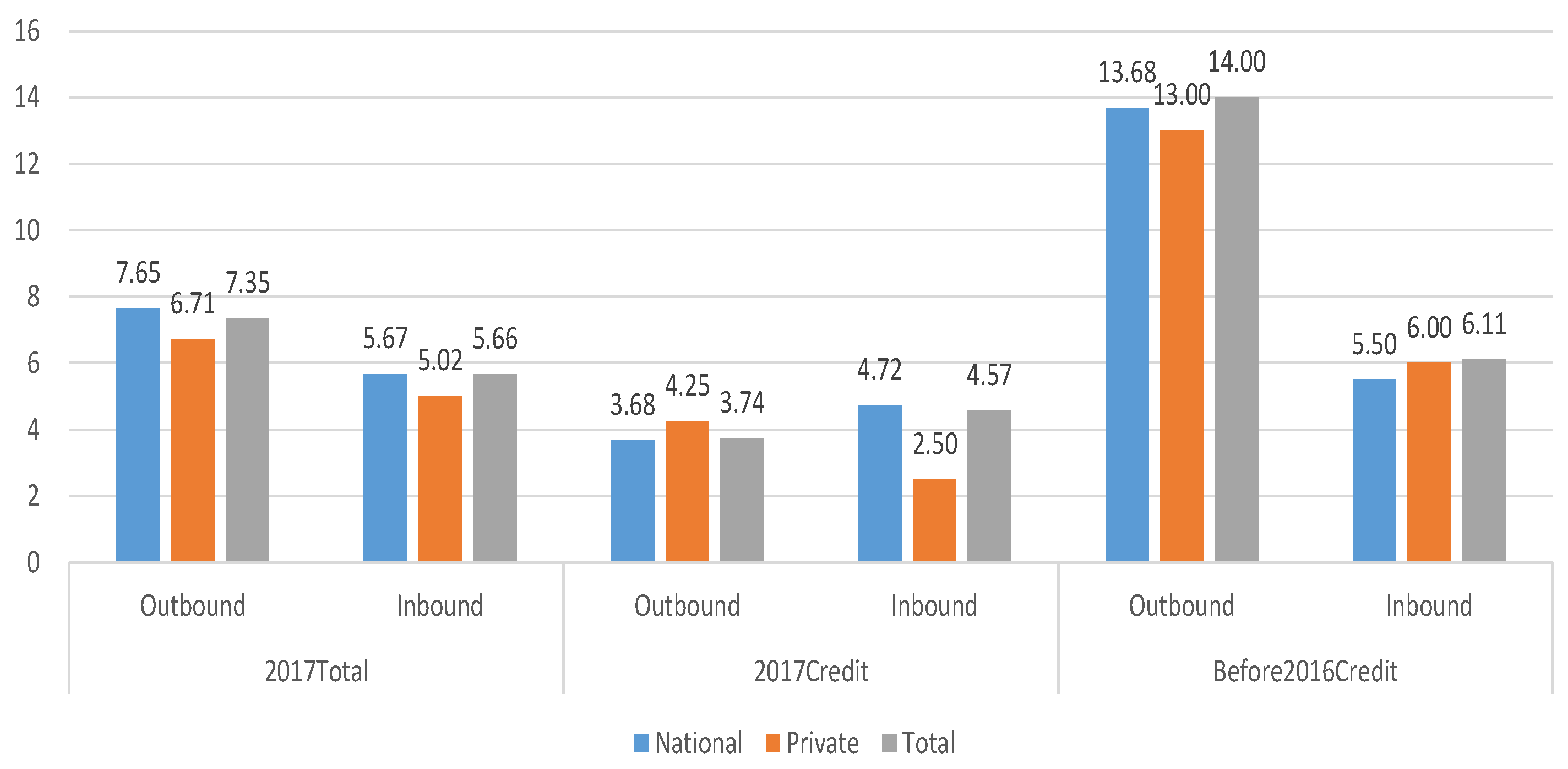
Figure 3.
Number of students per agreement by university type.
Figure 3 displays the average number of exchange students per agreement with one or more participants in study-abroad programs in AY 2017. Three variables were represented: (1) the total number of students who studied abroad in AY 2017 (2017Total); (2) the number of students who studied abroad with credit in AY 2017 (2017Credit); and (3) the number of students who studied abroad with credit in AY 2016 or earlier (Before2016credit). In Figure 3, the total figures for each variable include all types of universities, although national and private universities are shown separately because of their significant volume of agreement.
Three tendencies were observed, as shown in Figure 3. First, once the agreements were utilized, the number of outbound students in the Before2016credit category was more than double the number of inbound students (on average, 6.11 for inbound and 14.00 for outbound). Second, the figure indicates a similar number of exchange students per agreement between national and private universities, with a difference of less than one student per agreement, except for inbound students in 2017 with credit. The number of outbound students is higher in both AY2017Total and Before2016Credit, but not in 2017Credit for national universities and the total.
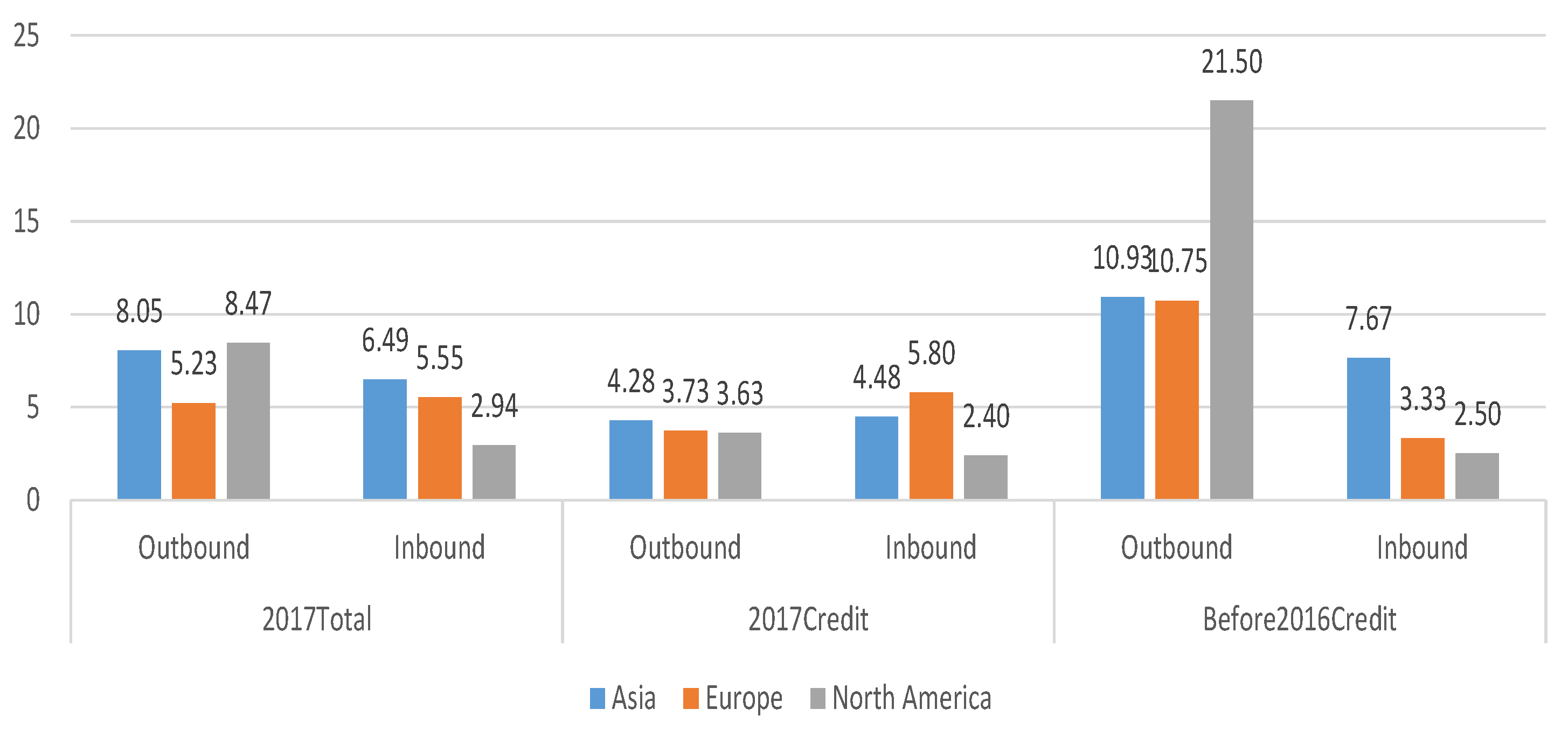
Figure 4 displays the number of students per agreement utilized by each region in AY 2017. A clear trend can be observed in the Before2016Credit category, which represents a longer period compared to the single-year variables, regardless of credit. In AY 2016 or earlier, the number of outbound students exceeded the number of inbound students, with North America showing a particularly significant difference: 21.50 outbound students and 2.50 inbound students. The balance between outbound and inbound students varies by region, with a relatively balanced distribution in Asia and an excess of outbound students in North America. In 2017, more students studied abroad without credit than with credit, although this trend was less pronounced in Europe, where credit programs have more participants than other programs.

Figure 4.
Number of students per agreement by region.
3.2. Stratification in International Partnership
Table 3 presents the stratification both between university types (public and private) and within each university type. First, there is a distinction between public and private universities. Among national universities, the top two classifications have approximately 16 agreements each, while the last two classifications have around 6–7 agreements. Among private universities, the top category has approximately six agreements, while the other two classifications have 3–4 agreements. Since the number of students per university does not vary significantly, the difference in the number of agreements directly reflects the difference in international partnerships per student. Therefore, the number of agreements per private university student is less than half that of students belonging to the top category of public universities.
Table 3.
Agreements by stratification of universities.
Although it is not easy to adjust for selectivity between different types of universities, one variable is the university entrance exam score. Currently, the score of the top category in private universities is 69.00, which lies between the first and second categories of public universities. The number of agreements per private university student is less than half that of the first and second categories of national universities, indicating a stratification between university types. Second, there is stratification within the same type of university. The top category contained more than twice the number in the bottom categories. In conclusion, selectivity appears to be moderately related to the number of agreements, with higher tiers having more agreements, with a small exception.
Figure 5 illustrates the proportion of regions in the partnerships categorized by university stratification. Examining this by university type, the distribution of national institutions closely aligns with the overall distribution of regions. However, private institutions show some variation, with approximately 12% points higher representation in North America and 5% points lower representation in Asia compared with the overall distribution.

Figure 5.
Proportion of region by stratification of university. Note: The total does not add up to 100% as other regions are excluded.
Notable differences can be observed both between university types and within private universities. The most significant difference is observed in the proportion of partnerships with North America. The top categories in both national and private institutions had a larger proportion of partnerships with North America compared to others. The difference was particularly prominent, with a gap of approximately 30%, reaching 15.45% for public universities and 44.44% for private ones. Conversely, the lowest categories in both public and private institutions had smaller proportions, but the difference was more pronounced in private institutions at 5.83% for public universities and 11.54% for private universities. In private universities, the higher the category, the more pronounced the proportion of partnerships with North America and the less pronounced the proportion with Asia or Europe.
4. Discussion
This study aimed to examine study-abroad agreements established using international partnerships among medical schools in Japan, focusing on reciprocity and stratification. In recent years, there has been an increase in the number of medical students participating in study abroad and elective programs, with over 60% of students taking part via these agreements. This highlights the fundamental role of international partnerships in providing international experiences for medical students. In other words, these agreements influence the quantity and quality of international medical education. The significance of this study lies in its empirical analysis of the characteristics of international education involving medical schools in Japan at a macro scale.
4.1. Characteristics of International Medical Exchange Agreements in Japan
Based on an analysis of national data, the regional distribution of agreements among medical schools was as follows: 60.59% in Asia, 21.86% in Europe, and 10.67% in North America, with these three regions accounting for over 93% of all agreements. When comparing these results with agreements across all fields, as presented by Kato and Ota [13], Asia has approximately 10% more agreements in medical fields, while Europe and North America have approximately 5% fewer agreements.
The results of this study highlight the distinct characteristics of international partnerships in the medical field compared to partnerships across all fields in Japan. Specifically, there is a higher reciprocity of tuition waivers in the United States for medical partnerships, whereas, in Europe, this reciprocity is more prevalent in the overall results for Japan. This difference may be attributed to the specific requirements and priorities of the medical field, such as the emphasis on professional learning with credits rather than focusing on language or multicultural experiences. Medical students often pursue advanced programs abroad to gain specialized knowledge and enhance their professional careers [3]. This could be applied to Japanese medical students, even as it diverges from the general trend in Japan, where students in their early undergraduate years are encouraged to participate in short-term study abroad programs with the aim of maximizing their undergraduate educational benefits.
4.2. Manifestation of Reciprocity in These Agreements
This study found that the average reciprocity rate through mutual tuition waivers in medical schools is 52.84%. This is consistent with the average rate in Asia, slightly lower in Europe (49.61%) and higher in North America at 58.06%. These findings also differ from the results obtained for all fields in Japan, where the average reciprocity rate is approximately 15% higher in Europe and 10% lower in North America.
According to Kato and Ota [13], the results for all fields can be interpreted as European universities relying more on public funding, while higher education in English-speaking countries relies more on private funds, prioritizing the financial contributions of foreign students. However, this interpretation does not align with the results of this study in the medical field. One possible explanation for the divide is the different demands of Japanese medical students from their peers in other fields. Japanese medical students might prefer study-abroad programs that offer field-specific learning and credit transfer rather than focusing solely on language enhancement or multicultural experiences. In this context, the significance of tuition waiver agreements in the United States could be attributed to the preference for study-abroad programs with credit transfers. Although the reason for this regional disparity between the total and medical fields is unclear, it highlights the importance of investigating international partnerships by field to gain a better understanding of the dynamics.
Reciprocity is also defined by the balance between the number of inbound and outbound students. In terms of student exchange, the results indicate a relatively balanced exchange in Europe, a slightly higher proportion of inbound students from Asia, and a significant excess of outbound students from Japan to North America. This imbalance is particularly notable in the cumulative number of students with credits, which is significantly higher for North America.
The current imbalance in student exchange may raise questions among stakeholders regarding the sustainability of agreements if mutual benefit is considered the foundation of the partnership. A more balanced exchange relationship is necessary to maintain mutually beneficial partnerships. Achieving this balance may require a careful assessment of the relationship between supply and demand, as well as consideration of the specific factors that contribute to the current imbalance.
The two types of reciprocity analyzed in this study, tuition waivers and a balance between outbound and inbound students, were not observed to be directly related. Although tuition waivers should encourage students to participate in exchange programs, this is not necessarily balanced between the two parties, which is based more on demand. Further investigations and careful analyses are necessary to better understand the specific reasons and dynamics behind these findings in the medical field.
4.3. Relationship between University Stratification and International Medical Exchange Agreements
Public universities in Japan have more agreements than private universities. They utilized approximately a third of the agreements, which is significantly lower than private universities by approximately 20% points. This suggests that national universities may have more room for active partnerships or may focus on quantity rather than quality with regard to internationalization in higher education.
Additionally, the study reveals stratification among universities, where highly selective institutions, such as former imperial or medical universities, have more than twice the number of agreements per university compared to others. This finding aligns with the overall trend across Japan, which could lead to higher tiers having an advantage in international partnerships, like the Mathai effect. This is not just quantity but also quality. For instance, there are regional composition differences based on university tiers, with higher agreement rates for private universities observed in North America. These phenomena may increase the established gaps among Japanese medical schools. If international partnerships become more commercially oriented, higher-tier medical schools with bigger budgets could have an advantage, adding to the financial favoring through government initiatives for internationalization at universities [19].
Similar to the international migration of highly skilled workers, the balance between the outflow and inflow of physicians varies widely among countries. According to Adovor et al. [24], medical doctors in Japan have low international mobility. In contrast, the number of Japanese medical students studying abroad or participating in elective programs has steadily increased, and this trend has been continuously monitored since the 1990s [3,5]. This can be explained by the vulnerable state of the country’s healthcare system, which is affected by the excess of pharmaceutical and medical equipment imports. University stakeholders consider this an alarming situation and recognize the significance of international education in maintaining Japan’s position in the global medical market through international cooperation and competition. In this sense, the maximization of nationwide opportunities for study abroad is one possible direction from the macro perspective. The reality, however, indicates stratified opportunities. This Japanese case analysis can provide international scholars the opportunity to consider student exchange agreements at the macro level.
The data used by this study do not include study abroad participants’ individual attributes, such as gender or socioeconomic status, like household revenue. While these attributes might relate to university characteristics, further research is needed to explore this area. This study has several limitations. First, the study did not encompass the entirety of the agreements related to medical schools because of limitations in data manipulation. Future studies should focus on these agreements. Second, it is worth considering that approximately 40% of Japanese medical students who studied abroad did not participate in programs under such agreements. Additionally, medical students may opt to participate in university-wide study-abroad programs, such as language study programs, during their early undergraduate years. Alternatively, they may join programs specific to the STEM fields. These opportunities should be considered to understand medical students’ international experiences.
Funding
This work was supported by JSPS KAKENHI, Grant Number 20K01604.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original data used in this study are available in Japanese at https://www.mext.go.jp/a_menu/koutou/shitu/1287263.htm (accessed on 1 June 2020).
Acknowledgments
The author would like to thank members in the editorial board for their supports and anonymous referees for their helpful comments.
Conflicts of Interest
The author has no competing interests to declare.
References
- Socha, K.; Lafortune, G. Recent Trends in International Migration of Doctors, Nurses and Medical Students; OECD: Paris, France, 2019. [Google Scholar] [CrossRef]
- Wismar, M.; Maier, C.B.; Glinos, I.A.; Dussault, G.; Figueras, J. Health Professional Mobility and Health Systems: Evidence from 17 European Countries. World Health Organization. Regional Office for Europe. 2011. Available online: https://apps.who.int/iris/handle/10665/170421 (accessed on 1 June 2022).
- Jeffrey, J.; Dumont, R.A.; Kim, G.Y.; Kuo, T. Effects of international health electives on medical student learning and career choice: Results of a systematic literature review. Fam. Med. 2011, 43, 21–28. [Google Scholar] [PubMed]
- Nishigori, H.; Takahashi, O.; Sugimoto, N.; Kitamura, K.; McMahon, G.T. A national survey of international electives for medical students in Japan: 2009–2010. Med. Teach. 2012, 34, 71–73. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Nishigori, H. National survey of international electives for global health in undergraduate medical education in Japan, 2011–2014. Nagoya J. Med. Sci. 2018, 80, 79–90. [Google Scholar] [CrossRef] [PubMed]
- JASSO. FY2019 Japanese Students Studying Abroad Survey Results. 2021. Available online: https://www.studyinjapan.go.jp/ja/_mt/2021/03/date2019n.pdf (accessed on 1 June 2022).
- De Wit, H.; Hunter, F.; Howard, L.; Egron-Polak, E. Internationalisation of Higher Education; European Parliament: Brussels, Belgium, 2015.
- Knight, J. Five myths about internationalization. Int. High. Educ. 2011, 62, 8532. [Google Scholar] [CrossRef]
- De Wit, H.; Merkx, G. History of the internationalization of higher education. In The Sage Handbook of International Education; Deardoff, D., de Wit, H., Heyl, J., Adams, T., Eds.; Sage: Los Angeles, CA, USA, 2012; pp. 43–60. [Google Scholar] [CrossRef]
- Yarmoshuk, A.N.; Cole, D.C.; Mwangu, M.; Guantai, A.N.; Zarowsky, C. Reciprocity in international interuniversity global health partnerships. High. Educ. 2020, 79, 395–414. [Google Scholar] [CrossRef]
- Umoren, R.A.; James, J.E.; Litzelman, D.K. Evidence of reciprocity in reports on international partnerships. Educ. Res. Int. 2012, 2012, 603270. [Google Scholar] [CrossRef]
- Leng, P. Mutuality in Cambodian international university partnerships: Looking beyond the global discourse. High. Educ. 2016, 72, 261–275. [Google Scholar] [CrossRef]
- Kato, M.; Ota, K. Student exchange agreement in Japanese higher education: Focusing on reciprocity and stratification. Nagoya J. High. Educ. 2023, 23, 165–188. [Google Scholar]
- Whatley, M. Institutional stratification in U.S. Study abroad participation and experiences. In Inequalities in Study Abroad and Student Mobility; Kommers, S., Bista, K., Eds.; Routledge: Oxford, UK, 2020; pp. 97–112. [Google Scholar] [CrossRef]
- Ota, K. Disparity trends in study abroad opportunities according to university status. J. Int. Educ. 2021, 27, 17–32. [Google Scholar]
- Medichen. Medical School Grading Check! We Will Introduce the Order in Ranking Format. Available online: https://medichen.tokyo/hierarchy-of-medical/ (accessed on 5 July 2023).
- MEXT. Survey on Enrollment of International Students and Number of Japanese Studying Abroad. 2021. Available online: https://www.mext.go.jp/content/20220603-mxt_gakushi02-100001342_2.pdf (accessed on 1 June 2022).
- Altbach, P.G.; Knight, J. The internationalization of higher education: Motivations and realities. J. Stud. Int. Educ. 2007, 11, 290–305. [Google Scholar] [CrossRef]
- Yonezawa, A.; Shimmi, Y. Transformation of university governance through internationalization: Challenges for top universities and government policies in Japan. High. Educ. 2015, 70, 173–186. [Google Scholar] [CrossRef]
- JASSO. FY2018 Japanese Students Studying Abroad Survey Results. 2018. Available online: https://www.studyinjapan.go.jp/ja/_mt/2020/08/date2018n.pdf (accessed on 1 June 2022).
- JASSO. FY2018 Foreign Student Enrollment Status Survey Results. 2018. Available online: https://www.studyinjapan.go.jp/ja/_mt/2020/08/date2018z.pdf (accessed on 1 June 2022).
- JASSO. FY2020 Japanese Students Studying Abroad Survey Results. 2022. Available online: https://www.studyinjapan.go.jp/ja/_mt/2022/11/date2020n.pdf (accessed on 1 June 2022).
- Stroud, A.H. Who plans (not) to study abroad? An examination of U.S. Student intent. J. Stud. Int. Educ. 2010, 14, 491–507. [Google Scholar] [CrossRef]
- Adovor, E.; Czaika, M.; Docquier, F.; Moullan, Y. Medical brain drain: How many, where, and why? J. Health Econ. 2021, 76, 102409. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).