1. Introduction
Resistant hypertension (RH) is defined as uncontrolled blood pressure despite treatment with four or more antihypertensive medications including an angiotensin-converting enzyme inhibitor, diuretic, β-blocker, or calcium channel blocker [
1]. Obstructive sleep apnea (OSA) is one of the most common forms of sleep disorder, characterized by recurrent episodes of upper-airway closure leading to intermittent hypoxia and sleep fragmentation. Epidemiologic data suggest there may be a causal, bidirectional relationship between OSA and RH [
2,
3]. Intermittent hypoxia in OSA increases oxidative stress, metabolic dysregulation, and systemic inflammation, leading to renin-aldosterone activation as well as endothelial dysfunction, suggesting that OSA is an independent cause of resistant hypertension [
2,
3]. Conversely, excess aldosterone in RH increases the volume overload, causing blockage of the upper-airway muscles and intermittent hypoxia (OSA), thus suggesting a bidirectional relationship [
2,
3].
Although prior studies have identified OSA as a risk factor for RH, data regarding the risk of OSA in patients with RH are scarce. Bhandari and colleagues conducted a retrospective cohort study using data from Kaiser Permanente, an integrated health system [
4]. They concluded that patients with RH are 16% more likely to develop OSA compared to patients with non-RH. However, this study was limited by use of a time-fixed (i.e., time-independent) definition of RH and was also subject to immortal time bias and unmeasured confounding. Thus, it is still not clear to whether and what extent patients with an exposure to RH have a higher risk of incident OSA compared to non-RH exposure. Thus, we sought to evaluate the risk of OSA in a sample of patients with treated hypertension in the US comparing RH and non-RH exposure.
2. Results
2.1. Patient Baseline and Clinical Characteristics
Our initial sample consisted of 16,732,799 patients with at least two antihypertensive prescription claims within a year between January 2008 and December 2019. From this sample, we excluded patients without 12-months continuous medical and pharmacy enrollment before the cohort entry (n = 10,170,961), patients without a history of hypertension (n = 5,068,157), patients under 18 years old at the cohort entry date (n = 6,246), and patients with a diagnosis of OSA in the baseline period (n = 112,380). Our final cohort consisted of 1,375,055 patients meeting the definition for “treated hypertension.”
Table 1 describes the baseline characteristics of the cohort. The mean age was 50 years, and 50.6% patients were men. The majority of patients were aged 51–64 years (54.5%) and resided in the southern region of the United States (48.7%). Obesity (11.5%) and hyperlipidemia (41.3%) were the most common comorbidities, whereas antidepressants (19.6%) and opiates (27.6%) were the most common prescription medications used during the baseline period. The mean (SD) Quan–Charlson comorbidity score was 0.5 (1.1). Overall, the most commonly filled antihypertensive medications were beta blockers, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, and calcium channel blockers in RH and non-RH groups.
2.2. Classification of RH and Non-RH Exposures
Of 1,375,055 patients with treated hypertension, 13,584 patients met RH at some point during follow-up. The mean duration of follow-up was 762 days RH exposure and 854 days for non-RH exposure. We identified 1532 incident OSA cases in during RH exposure and 93,397 incident OSA cases during non-RH exposure.
2.3. Risk of OSA
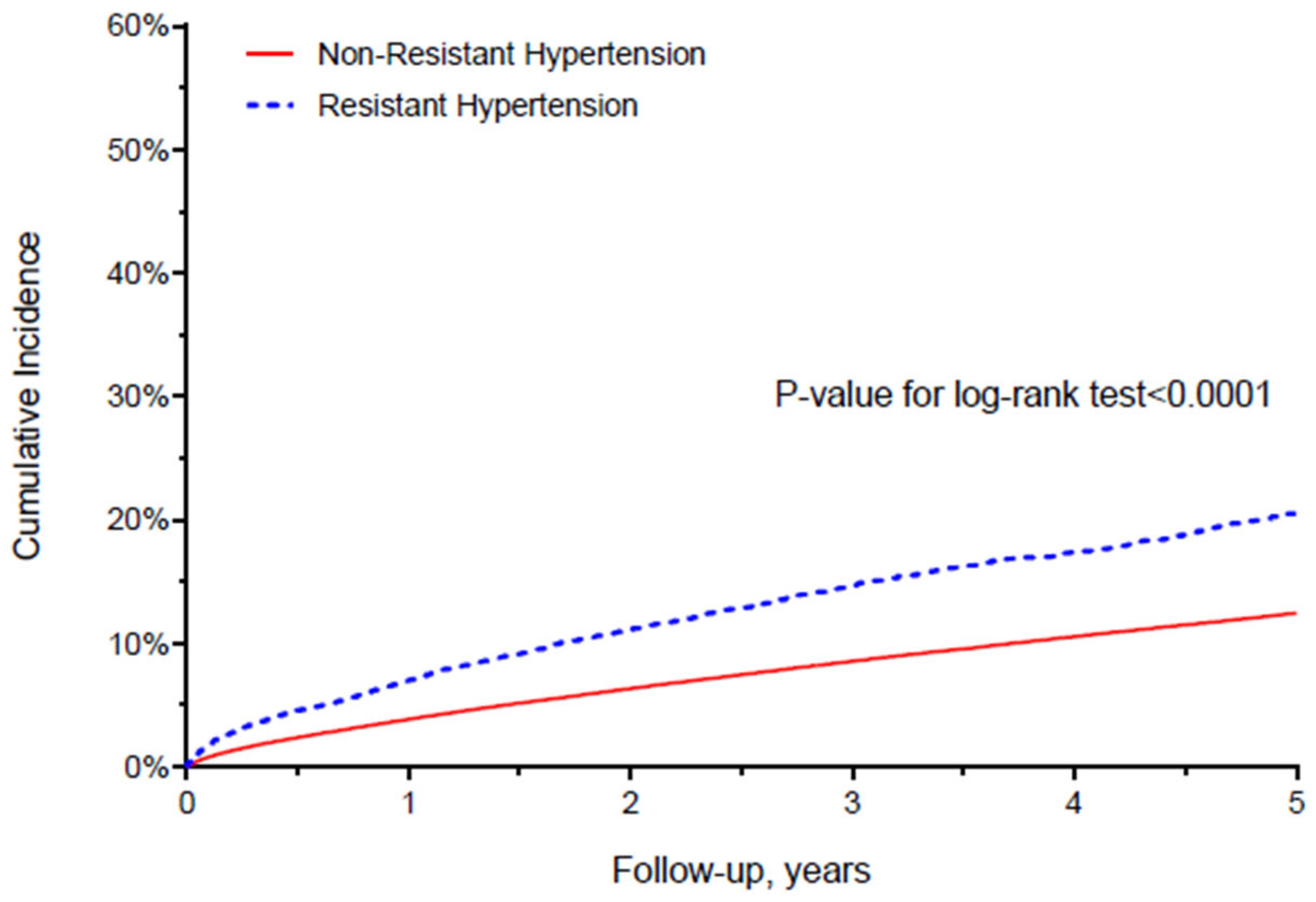
The crude incidence rates of OSA were 54.0 and 29.0 per 1000 person-years for RH exposure and non-RH exposure, respectively. The Kaplan–Meier survival curve (
Figure 1 indicated that patients with RH exposure had a higher risk of OSA with significant log-rank test results (
p < 0.0001) in crude analysis. In the multivariable Cox proportional hazards model adjusted for demographics (age, sex, region), clinical comorbidities (Quan–Charlson comorbidity score, asthma, obesity, heart failure, anemia, depression, anxiety, hyperlipidemia, stroke, migraine, chronic kidney disease, coronary artery disease, transient ischemic attack, substance use disorder), prescription-medication utilization (antidiabetics, antihistamines, antidepressants, anticonvulsants, antipsychotics, barbiturates, benzodiazepines, and opioids) and healthcare resource utilization (number of outpatient visits, and number of inpatient visits), compared to non-RH, RH exposure incurred a 60% increased risk of OSA (adjusted hazard ratio (aHR): 1.60; 95% CI, 1.52–1.68) (
Table 2).
3. Discussion
To the best of our knowledge, this is the largest study to date to examine the risk of OSA associated with RH compared to non-RH. Our principal findings suggest that RH exposure was associated with a 60% increased risk of OSA compared to non-RH. The results from this study provide a novel contribution to the literature by quantifying the risk for development of incident OSA in patients with and without RH exposure.
Although OSA is an important public health concern and is highly prevalent in the US, OSA is underrecognized and underdiagnosed in the RH population [
5]. Inadequate treatment of OSA with continuous positive-airway-pressure therapy can not only lead to uncontrolled blood pressure in patients with RH [
6] but also to unnecessary treatment intensification with an additional antihypertensive, thus increasing the risk of hypotension and other severe adverse effects. Given the high clinical and financial burden associated with OSA for payers and patients/families [
7], such findings may provide insights on the further development of strategies and policies to facilitate screening and regular monitoring of OSA among patients with RH.
A major strength of this study is the use of a large, diverse population and being representative of commercially insured adults in the U.S. Additionally, the mean follow-up time was more than 2 years. Therefore, we could assess the longer-term risk of OSA in patients with and without RH. Despite these strengths, this study has some limitations. First, we used a sample of commercially insured individuals, with possibly limited generalizability to Medicaid and Medicare populations. Second, we did not have access to polysomnography laboratory results and therefore relied on ICD-9-CM and ICD-10-CM diagnosis codes to identify patients with OSA, which may have introduced misclassification. However, since we used the same outcome definition for the exposure groups (i.e., RH and non-RH), any misclassification is likely to be non-differential and likely to bias results to the null. Third, because this is an observational study, it may be susceptible to residual confounding.
4. Materials and Methods
4.1. Data Source
We conducted a retrospective cohort analysis using IBM MarketScan
® commercial claims database from January 2008 to December 2019. This database consists of nationwide administrative claims data over 180 million beneficiaries and their dependents covered under a variety of health benefit plans [
8]. This database is representative of ≈49% of the US population receiving health insurance under employer-sponsored programs.
4.2. Study Population
The study population consisted of adults (≥18 years old) who had at least two antihypertensive prescription drug claims within a calendar year from January 2008 to December 2019. We required evidence of a second prescription fill to ensure that patients were treated for hypertension. To avoid immortal time bias, patients entered the cohort on the date of the second antihypertensive refill date (i.e., index date of cohort entry) after a 365-day period of continuous medical and pharmacy enrollment (i.e., baseline period). During the baseline period, patients were required to have at least one inpatient or two outpatient diagnosis code for hypertension (International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM): 401.x; International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM): I10.x). Patients with a diagnosis of OSA (the outcome) in the baseline period were excluded.
4.3. Exposure Definition
To assess the association between exposure to RH and the risk of developing OSA, a time-dependent exposure analysis was performed. Exposure was classified as non-RH (treatment with ≤3 antihypertensive drugs concurrently) or RH (treatment with ≥4 antihypertensive drugs concurrently for at least 60 days) [
9]. Patients meeting RH criteria were considered to have RH indefinitely thereafter. The 60-day period was chosen to ensure persistent, concurrent use of ≥4 antihypertensive drug classes. The first day of overlapping use of ≥4 antihypertensive drugs for at least 60 days was defined as the index date for the RH exposure.
4.4. Study Outcome and Follow up
The primary outcome of interest was OSA identified by requiring at least one inpatient hospital discharge or two outpatient visits on different days with a qualifying diagnosis of OSA in any position using ICD-9-CM (780.51, 780.57, 780.53, 327.23; or ICD-10-CM (G47.30, G47.33, G47.39) codes. The earliest date of diagnosis of OSA was identified as the date of outcome.
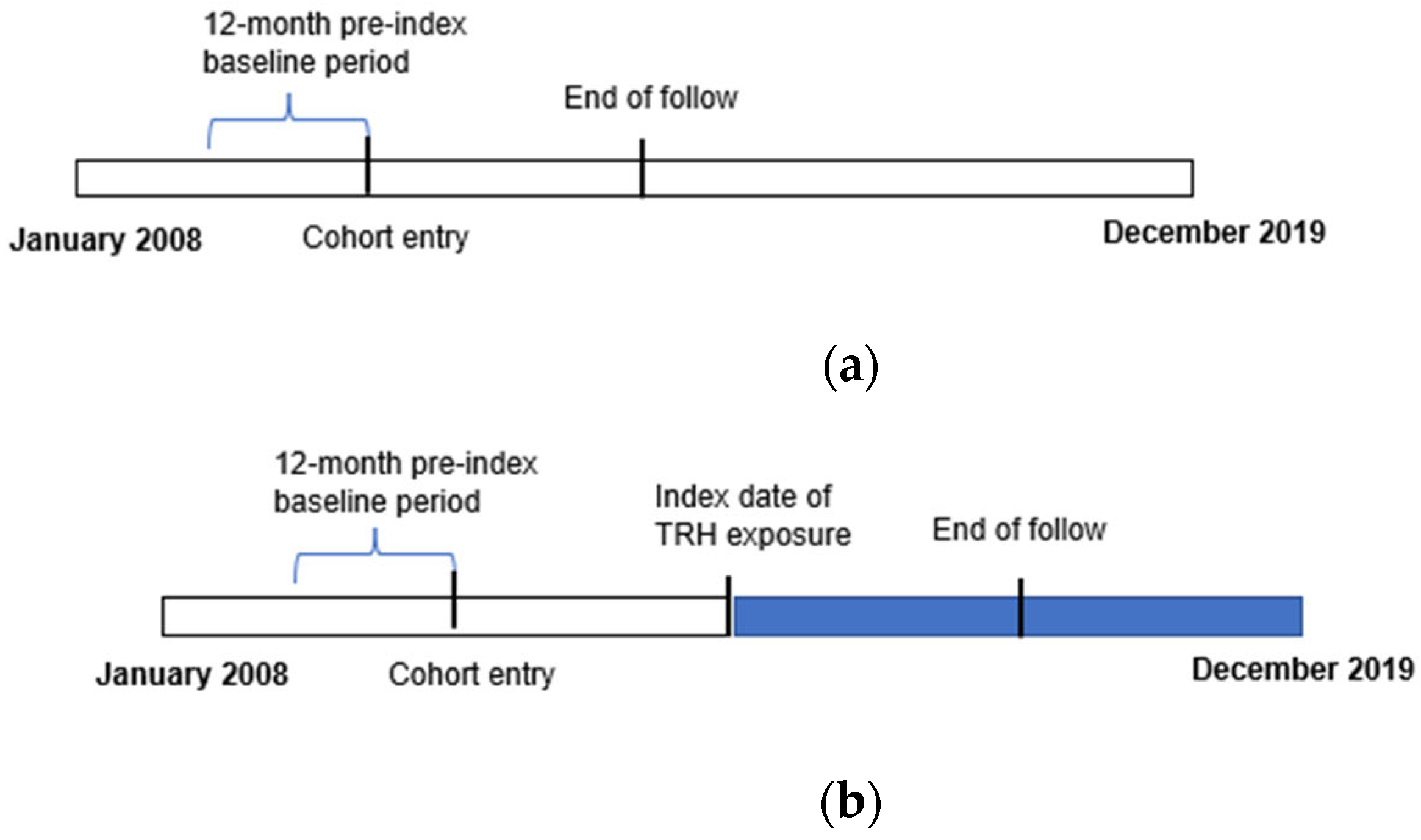
All patients entered the cohort on the day of second prescription fill of antihypertensives (i.e., index date). Patients were followed from the index date until the earliest of first occurrence of: the outcome, end of continuous medical and pharmacy enrollment or the study end date (31 December 2019). For patients meeting RH criteria, exposure was classified as non-RH until the RH definition was met, and as RH thereafter, whereas for those never meeting RH criteria, all follow-up time was classified as non-RH (
Figure 2a,b).
4.5. Baseline Covariates
Potential confounders were identified through a literature review and measured during the baseline period, including the index date. We assessed demographic characteristics (i.e., age, sex, region) and specific comorbidities of interest (i.e., asthma, obesity, heart failure, anemia, depression, anxiety, hyperlipidemia, stroke, migraine, chronic kidney disease, coronary artery disease, transient ischemic attack, and substance use disorder). Additionally, to better account for potential confounding by other comorbidities, we also measured the Quan–Charlson comorbidity index score (calculated based on the presence of ICD-9-CM and ICD-10-CM diagnosis codes) which includes 17 comorbidities [
10]. We also assessed prescription medication use (i.e., antidiabetics, antihistamines, antidepressants, anticonvulsants, antipsychotics, barbiturates, benzodiazepines and opioids) and healthcare utilization patterns (i.e., number of outpatient visits and number of inpatient hospital visits).
4.6. Statistical Analysis
We conducted descriptive analysis of categorical variables and reported numbers and percentages. The incidence rate of OSA was calculated as the number of OSA events divided by the observed time at risk, expressed per 1000 person-years. A Kaplan–Meier curve was generated to visualize the OSA risk over time between the RH and non-RH patients, and its significance was tested using the Log-rank test. A Cox proportional hazards model with time-varying exposure (RH vs. non-RH) was used to compare the risk of developing OSA in RH patients compared with non-RH patients, adjusting for potential confounders. SAS 9.4 (SAS Institute Inc., Cary, NC, USA) was used for data analyses and data management. All probability values were considered significant at p < 0.05.
5. Conclusions
In this large population-based cohort study of adults with treated hypertension, exposure with RH was associated with a significant increased risk of OSA. Overall, this study offers an important step in quantifying the risk of OSA in patients with RH. Importantly, the findings of this study suggests that screening of OSA is necessary in patients with RH. Greater efforts are needed to develop strategies to facilitate screening, monitoring and treatment of OSA.
Author Contributions
Conceptualization, R.D. and S.M.S.; methodology, R.D., H.P. and S.M.S.; software, R.D.; validation, R.D., H.P. and S.M.S.; formal analysis, R.D.; investigation, R.D.; resources, R.D.; data curation, R.D.; writing—original draft preparation, R.D. and S.M.S.; writing—review and editing, R.D., H.P., J.D.B. and S.M.S.; visualization, R.D.; supervision, S.M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Institutional Review Board at the University of Florida.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is contained within the article.
Conflicts of Interest
The authors report no conflict of interest.
References
- Sheppard, J.P.; Martin, U.; McManus, R.J. Diagnosis and management of resistant hypertension. Heart 2017, 103, 1295–1302. [Google Scholar] [CrossRef] [PubMed]
- Van Ryswyk, E.; Mukherjee, S.; Chai-Coetzer, C.L.; Vakulin, A.; McEvoy, R.D. Sleep Disorders, Including Sleep Apnea and Hypertension. Am. J. Hypertens. 2018, 31, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Torres, G.; Sánchez-de-la-Torre, M.; Barbé, F. Relationship Between OSA and Hypertension. Chest 2015, 148, 824–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhandari, S.K.; Shi, J.; Molnar, M.Z.; Rasgon, S.A.; Derose, S.F.; Kovesdy, C.P.; Calhoun, D.A.; Kalantar-Zadeh, K.; Jacobsen, S.J.; Sim, J.J. Comparisons of sleep apnoea rate and outcomes among patients with resistant and non-resistant hypertension. Respirology 2016, 21, 1486–1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demede, M.; Pandey, A.; Zizi, F.; Bachmann, R.; Donat, M.; McFarlane, S.I.; Jean-Louis, G.; Ogedegbe, G. Resistant Hypertension and Obstructive Sleep Apnea in the Primary-Care Setting. Int. J. Hypertens. 2011, 2011, 340929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joyeux-Faure, M.; Baguet, J.P.; Barone-Rochette, G.; Faure, P.; Sosner, P.; Mounier-Vehier, C.; Lévy, P.; Tamisier, R.; Pépin, J.-L. Continuous Positive Airway Pressure Reduces Night-Time Blood Pressure and Heart Rate in Patients with Obstructive Sleep Apnea and Resistant Hypertension: The RHOOSAS Randomized Controlled Trial. Front. Neurol. 2018, 9, 318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knauert, M.; Naik, S.; Gillespie, M.B.; Kryger, M. Clinical consequences and economic costs of untreated obstructive sleep apnea syndrome. World J. Otorhinolaryngol. Head Neck Surg. 2015, 1, 17–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietrich, E.; Desai, R.; Garg, M.; Park, H.; Smith, S.M. Reimbursement of ambulatory blood pressure monitoring in the US commercial insurance marketplace. J. Clin. Hypertens. 2019, 22, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.; Park, H.; Dietrich, E.A.; Smith, S.M. Trends in ambulatory blood pressure monitoring use for confirmation or monitoring of hypertension and resistant hypertension among the commercially insured in the U.S., 2008–2017. Int. J. Cardiol. Hypertens. 2020, 6, 100033. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).







{kind=link}
{kind=link}