
Loop Diuretics and Sarcopenia: A Potential Association



Abstract
:1. Introduction
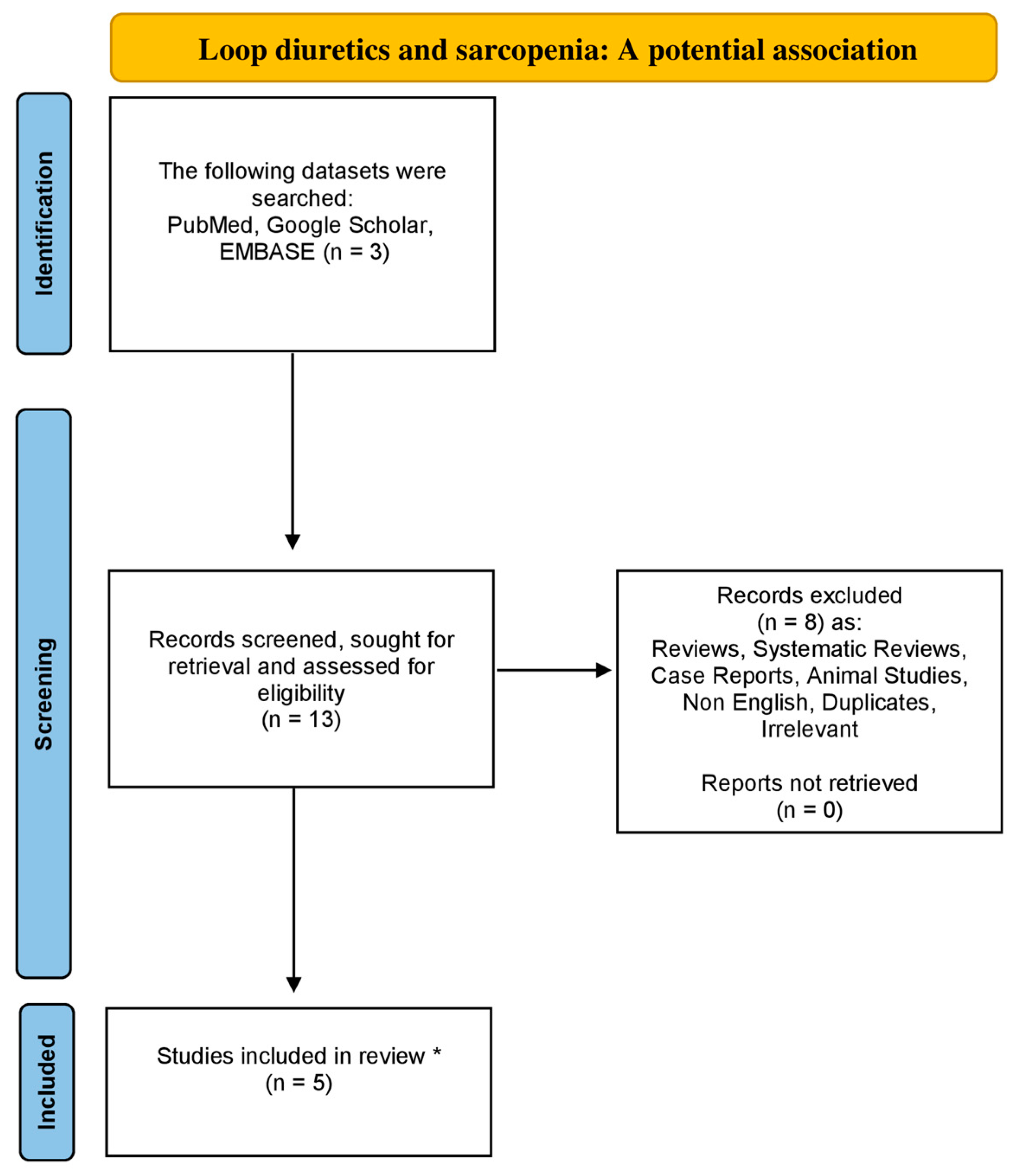
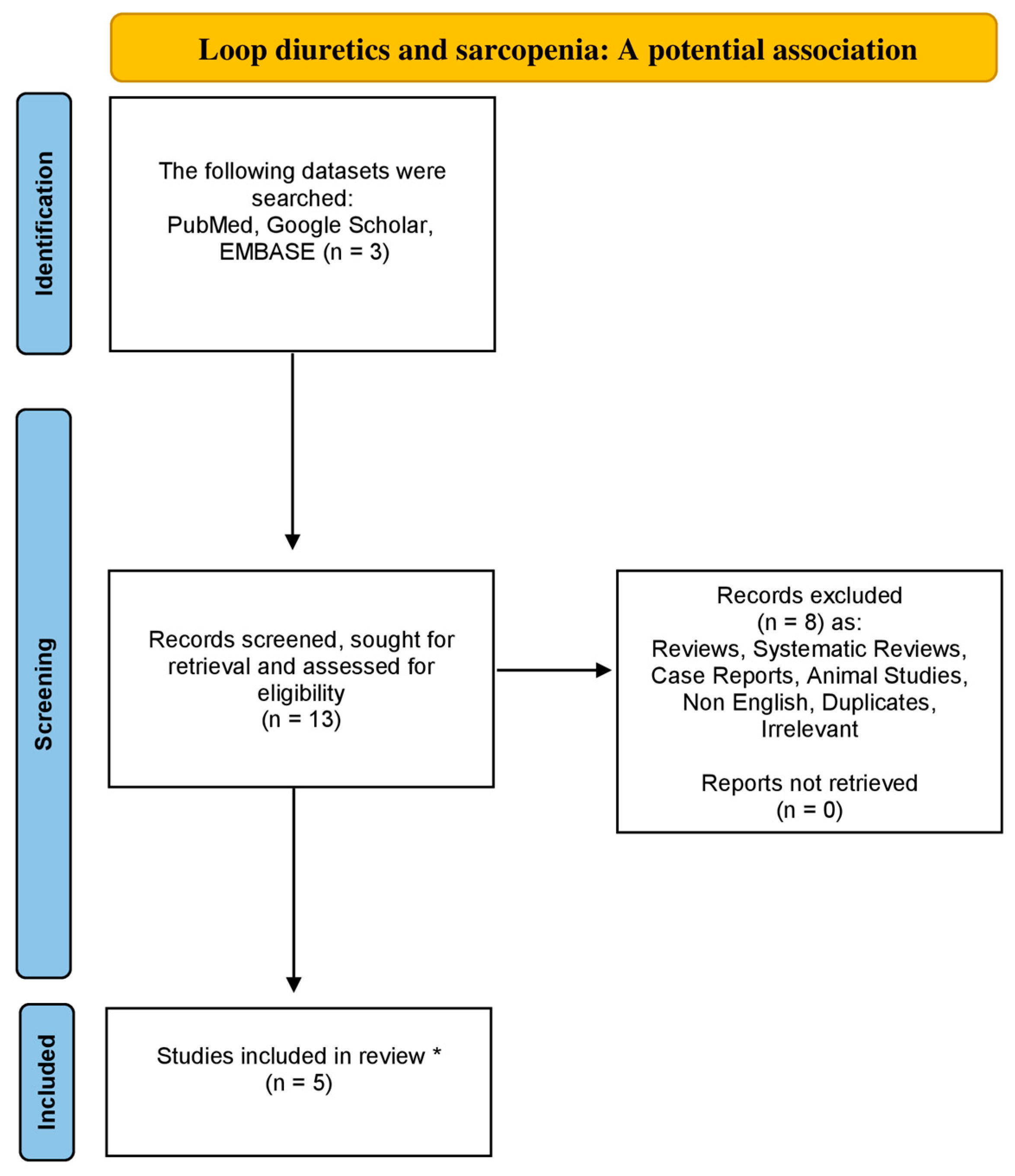
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sayer, A.A.; Cruz-Jentoft, A. Sarcopenia definition, diagnosis and treatment: Consensus is growing. Age Ageing 2022, 51, afac220. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.Y.; Bruyere, O. Health Outcomes of Sarcopenia: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, A.; Cuppari, L.; Stenvinkel, P.; Lindholm, B.; Avesani, C.M. Sarcopenia in chronic kidney disease: What have we learned so far? J. Nephrol. 2021, 34, 1347–1372. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Bahat, G.; Erdogan, T.; Ilhan, B. SARC-F and other screening tests for sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2022, 25, 37–42. [Google Scholar] [CrossRef]
- Rossi, A.P.; Urbani, S.; Gattazzo, S.; Nori, N.; Fantin, F.; Zoico, E.; Mazzali, G.; Muollo, V.; Ghoch, M.E.; Zamboni, M. The Mini Sarcopenia Risk Assessment (MSRA) Questionnaire score as a predictor of skeletal muscle mass loss. Aging Clin. Exp. Res. 2021, 33, 2593–2597. [Google Scholar] [CrossRef]
- Tseng, T.G.; Lu, C.K.; Hsiao, Y.H.; Pan, S.C.; Tai, C.J.; Lee, M.C. Development of Taiwan Risk Score for Sarcopenia (TRSS) for Sarcopenia Screening among Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2020, 17, 2859. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Gray, S.R.; Forrest, E.; Welsh, P.; Sattar, N.; Celis-Morales, C.; Ho, F.K.; Pell, J.P. Associations of muscle mass and grip strength with severe NAFLD: A prospective study of 333,295 UK Biobank participants. J. Hepatol. 2022, 76, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.Y.; Kim, M.; Kim, K.S.; Kim, S.; Won, C.W. Chair stand test as a proxy for physical performance and muscle strength in sarcopenia diagnosis: The Korean frailty and aging cohort study. Aging Clin. Exp. Res. 2022, 34, 2449–2456. [Google Scholar] [CrossRef] [PubMed]
- Chianca, V.; Albano, D.; Messina, C.; Gitto, S.; Ruffo, G.; Guarino, S.; Del Grande, F.; Sconfienza, L.M. Sarcopenia: Imaging assessment and clinical application. Abdom. Radiol. 2022, 47, 3205–3216. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Messina, C.; Vitale, J.; Sconfienza, L.M. Imaging of sarcopenia: Old evidence and new insights. Eur. Radiol. 2020, 30, 2199–2208. [Google Scholar] [CrossRef] [PubMed]
- Guglielmi, G.; Ponti, F.; Agostini, M.; Amadori, M.; Battista, G.; Bazzocchi, A. The role of DXA in sarcopenia. Aging Clin. Exp. Res. 2016, 28, 1047–1060. [Google Scholar] [CrossRef]
- Aleixo, G.F.P.; Shachar, S.S.; Nyrop, K.A.; Muss, H.B.; Battaglini, C.L.; Williams, G.R. Bioelectrical Impedance Analysis for the Assessment of Sarcopenia in Patients with Cancer: A Systematic Review. Oncologist 2020, 25, 170–182. [Google Scholar] [CrossRef]
- Kostka, J.; Sosowska, N.; Guligowska, A.; Kostka, T. A Proposed Method of Converting Gait Speed and TUG Test in Older Subjects. Int. J. Environ. Res. Public Health 2022, 19, 12145. [Google Scholar] [CrossRef]
- Lee, S.Y.; Choo, P.L.; Pang, B.W.J.; Lau, L.K.; Jabbar, K.A.; Seah, W.T.; Chen, K.K.; Ng, T.P.; Wee, S.L. SPPB reference values and performance in assessing sarcopenia in community-dwelling Singaporeans—Yishun study. BMC Geriatr. 2021, 21, 213. [Google Scholar] [CrossRef]
- Hurst, C.; Robinson, S.M.; Witham, M.D.; Dodds, R.M.; Granic, A.; Buckland, C.; De Biase, S.; Finnegan, S.; Rochester, L.; Skelton, D.A.; et al. Resistance exercise as a treatment for sarcopenia: Prescription and delivery. Age Ageing 2022, 51, afac003. [Google Scholar] [CrossRef]
- Beckwee, D.; Delaere, A.; Aelbrecht, S.; Baert, V.; Beaudart, C.; Bruyere, O.; de Saint-Hubert, M.; Bautmans, I. Exercise Interventions for the Prevention and Treatment of Sarcopenia. A Systematic Umbrella Review. J. Nutr. Health Aging 2019, 23, 494–502. [Google Scholar] [CrossRef]
- Anton, S.D.; Hida, A.; Mankowski, R.; Layne, A.; Solberg, L.M.; Mainous, A.G.; Buford, T. Nutrition and Exercise in Sarcopenia. Curr. Protein Pept. Sci. 2018, 19, 649–667. [Google Scholar] [CrossRef] [PubMed]
- Karakousis, N.D.; Gourgoulianis, K.I.; Kotsiou, O.S. Sarcopenia and Tuberculosis: Is There Any Connection? J. Pers. Med. 2023, 13, 1102. [Google Scholar] [CrossRef] [PubMed]
- Cannataro, R.; Carbone, L.; Petro, J.L.; Cione, E.; Vargas, S.; Angulo, H.; Forero, D.A.; Odriozola-Martinez, A.; Kreider, R.B.; Bonilla, D.A. Sarcopenia: Etiology, Nutritional Approaches, and miRNAs. Int. J. Mol. Sci. 2021, 22, 9724. [Google Scholar] [CrossRef] [PubMed]
- Novak, J.E.; Ellison, D.H. Diuretics in States of Volume Overload: Core Curriculum 2022. Am. J. Kidney Dis. 2022, 80, 264–276. [Google Scholar] [CrossRef]
- Carone, L.; Oxberry, S.G.; Twycross, R.; Charlesworth, S.; Mihalyo, M.; Wilcock, A. Furosemide. J. Pain Symptom Manag. 2016, 52, 144–150. [Google Scholar] [CrossRef]
- Maideen, N.M.P.; Balasubramanian, R.; Muthusamy, S. A Comprehensive Review of the Pharmacologic Perspective on Loop Diuretic Drug Interactions with Therapeutically Used Drugs. Curr. Drug Metab. 2022, 23, 188–199. [Google Scholar] [CrossRef]
- Ponto, L.L.; Schoenwald, R.D. Furosemide (frusemide). A pharmacokinetic/pharmacodynamic review (Part I). Clin. Pharmacokinet. 1990, 18, 381–408. [Google Scholar] [CrossRef]
- Pana, A.; Sourtzi, P.; Kalokairinou, A.; Velonaki, V.S. Sarcopenia and polypharmacy among older adults: A scoping review of the literature. Arch. Gerontol. Geriatr. 2022, 98, 104520. [Google Scholar] [CrossRef]
- Ishikawa, S.; Naito, S.; Iimori, S.; Takahashi, D.; Zeniya, M.; Sato, H.; Nomura, N.; Sohara, E.; Okado, T.; Uchida, S.; et al. Loop diuretics are associated with greater risk of sarcopenia in patients with non-dialysis-dependent chronic kidney disease. PLoS ONE 2018, 13, e0192990. [Google Scholar] [CrossRef]
- Hanai, T.; Shiraki, M.; Miwa, T.; Watanabe, S.; Imai, K.; Suetsugu, A.; Takai, K.; Moriwaki, H.; Shimizu, M. Effect of loop diuretics on skeletal muscle depletion in patients with liver cirrhosis. Hepatol. Res. 2019, 49, 82–95. [Google Scholar] [CrossRef]
- Nakano, I.; Tsuda, M.; Kinugawa, S.; Fukushima, A.; Kakutani, N.; Takada, S.; Yokota, T. Loop diuretic use is associated with skeletal muscle wasting in patients with heart failure. J. Cardiol. 2020, 76, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Saitoh, M.; Dos Santos, M.R.; Emami, A.; Ishida, J.; Ebner, N.; Valentova, M.; Bekfani, T.; Sandek, A.; Lainscak, M.; Doehner, W.; et al. Anorexia, functional capacity, and clinical outcome in patients with chronic heart failure: Results from the Studies Investigating Co-morbidities Aggravating Heart Failure (SICA-HF). ESC Heart Fail. 2017, 4, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Sawada, Y.; Kawaratani, H.; Kubo, T.; Fujinaga, Y.; Furukawa, M.; Saikawa, S.; Sato, S.; Takaya, H.; Kaji, K.; Shimozato, N.; et al. Effect of furosemide on muscle cramps in patients with liver cirrhosis. J. Gastroenterol. Hepatol. 2020, 35, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Karakousis, N.D.; Pyrgioti, E.E.; Georgakopoulos, P.N.; Papanas, N. Sarcopenia, Frailty and Diabetic Foot: A Mini Narrative Review. Int. J. Low. Extrem. Wounds 2022, 15347346221111420. [Google Scholar] [CrossRef] [PubMed]
- Karakousis, N.D.; Biliou, S.; Pyrgioti, E.E.; Georgakopoulos, P.N.; Liakopoulos, V.; Papanas, N. Frailty, sarcopenia and diabetic kidney disease: Where do we stand? Int. Urol. Nephrol. 2023, 55, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Karakousis, N.D.; Kotsiou, O.S.; Gourgoulianis, K.I. Bronchial Asthma and Sarcopenia: An Upcoming Potential Interaction. J. Pers. Med. 2022, 12, 1556. [Google Scholar] [CrossRef]
- Meza-Valderrama, D.; Marco, E.; Davalos-Yerovi, V.; Muns, M.D.; Tejero-Sanchez, M.; Duarte, E.; Sanchez-Rodriguez, D. Sarcopenia, Malnutrition, and Cachexia: Adapting Definitions and Terminology of Nutritional Disorders in Older People with Cancer. Nutrients 2021, 13, 761. [Google Scholar] [CrossRef]
- Benz, E.; Trajanoska, K.; Lahousse, L.; Schoufour, J.D.; Terzikhan, N.; De Roos, E.; de Jonge, G.B.; Williams, R.; Franco, O.H.; Brusselle, G.; et al. Sarcopenia in COPD: A systematic review and meta-analysis. Eur. Respir. Rev. 2019, 28, 190049. [Google Scholar] [CrossRef]

{kind=link}
| Authors/[Reference] | Study Design | Study Population | Main Outcomes | Sarcopenia Assessment |
|---|---|---|---|---|
| Ishikawa et al./[29] | Cross-sectional | A total of 260 subjects with NDD-CKD. | In total, 25.0% of subjects had sarcopenia. Increased risk of sarcopenia was importantly related to age, male gender, DM, BMI, LD use (OR, 4.59; 95% CI, 1.81–11.61; p = 0.001). | AWGS |
| Hanai et al./[30] | Retrospective | A total of 226 liver cirrhosis subjects. During follow-up period, 82 subjects died. | Therapeutic dosage of LDs inversely correlated with ΔSMA when conducted using simple (r = −0.27; p < 0.0001) and multiple regression analyses (t = −3.07; p = 0.002). Overall, survival rates decreased more in subjects treated with LDs at >20 mg than those treated at ≤20 mg (median, 66 vs. 97 months; p = 0.002). LDs of >20 mg (HR, 1.86; 95% CI, 1.03–3.24; p = 0.039) and ΔSMA of ≤−3.1% (HR, 3.87; 95% CI, 2.32–6.60; p < 0.0001) independently related to mortality. | Skeletal muscle cross-sectional area at the level of L3 vertebra measured using CT. |
| Nakano et al./[31] | Cross-sectional | A total of 155 subjects with HF (age 67 ± 13 years, 69% men). | Thigh and arm circumferences were significantly small in the LD-treated group in comparison with those not treated (39.9 ± 4.8 vs. 43.5 ± 6.9 cm; p < 0.001 and 26.7 ± 3.5 vs. 28.9 ± 6.2 cm; p < 0.001, respectively). LDs were significantly related to smaller thigh circumference and independently related to smaller thigh circumference (β = −0.51; 95% CI −0.98 to −0.046; p = 0.032). | Thigh and arm circumferences |
| Saitoh et al./[32] | Prospective, observational | A total of 166 subjects with HF (25 female; 66 ± 12 years). 22 subjects (13%) died during follow-up. | Anorexic subjects are more likely to be on diuretic treatment (75.5% vs. 96.5%; p = 0.001) and LDs utilization (56.9% vs. 78.9%; p = 0.006). Subjects having both anorexia and cachexia demonstrated increased prevalence of sarcopenia. | DXA |
| Sawada et al./[33] | Cross-sectional questionnaire | A total of 152 subjects (mean age, 68.5 ± 11.5 years; 62.5% male; BMI, 24.3 ± 3.7) with liver cirrhosis | Two groups including subjects with or without muscle cramps. Body composition, grip strength and sarcopenia (p = 0.73) were similar in the 2 groups. Furosemide use was significantly higher in the muscle cramp group (24% vs. 9.5%; p = 0.01), while furosemide utilization (OR, 2.61; 95% CI, 1.01–6.78; p = 0.04) was the sole noteworthy predictor of muscle cramp occurrence. | CT imaging at the L3 vertebral level, hand grip strength and BIA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karakousis, N.D.; Georgakopoulos, P.N. Loop Diuretics and Sarcopenia: A Potential Association. Muscles 2023, 2, 317-326. https://doi.org/10.3390/muscles2040024
Karakousis ND, Georgakopoulos PN. Loop Diuretics and Sarcopenia: A Potential Association. Muscles. 2023; 2(4):317-326. https://doi.org/10.3390/muscles2040024
Chicago/Turabian StyleKarakousis, Nikolaos D., and Petros N. Georgakopoulos. 2023. "Loop Diuretics and Sarcopenia: A Potential Association" Muscles 2, no. 4: 317-326. https://doi.org/10.3390/muscles2040024
APA StyleKarakousis, N. D., & Georgakopoulos, P. N. (2023). Loop Diuretics and Sarcopenia: A Potential Association. Muscles, 2(4), 317-326. https://doi.org/10.3390/muscles2040024