INTRODUCTION
Ankyloglossia or the deviation of the lingual frenulum has been reported to cause changes in tongue movement, thus impairing food functions and affecting speech (Chu & Blom, 2009; Obladen, 2009). Despite being a common condition, it is still not well defined in terms of diagnosis, treatment and prognosis.
With regards to frenulum alteration, we can see different types of alteration, for example, the lingual frenulum can be attached in the anterior aspect of the tongue near the tongue tip, and/or the length of the frenulum can be short. The anterior frenulum is known to affect the production of speech sounds, especially those that require refined movement of the tongue tip and body.
When the frenulum is short, it has a big impact upon the posture of the tongue, which remains on the floor of the mouth, and less impact on the movements of the tongue. Therefore, in such a condition, speech is less affected. In such cases, it is common that speech is produced utilizing a narrower range of motion by the articulators. When the frenulum is short and attached near the tip of the tongue, it generates a greater impact on speech, since the whole tongue remains on the mouth floor, with limited movements by the anterior part of the tongue (Marchesan, 2004).
Figure 1.
Photographic records of pre-frenectomy (a) and post-frenectomy. (b) in 4 cases of lingual frenectomy.
Figure 1.
Photographic records of pre-frenectomy (a) and post-frenectomy. (b) in 4 cases of lingual frenectomy.
In our clinical practice, we have observed that, the most common deviations found in produced by patients with an abnormal lingual frenulum, is the alveolar tap [r] (Camargo et al., 2013) and the alveolar fricatives [s] [z] productions. Other characteristics that affect articulation due to the limited tongue movement have to do with compensatory strategies or adaptations of jaw movements (e.g. excessive lateralization and anteriorization), and increased salivation, which can cause inaccuracies in speech production.
Although ankyloglossia is still subject to much controversy, surgical interventions have been proposed since ancient Greek medicine. One possible type of corrective surgery is lingual frenectomy, which is considered to be a safe and effective procedure for releasing the tongue-tie. This revision can lead to improved lingual function (Acevedo et al., 2010; Knox, 2010). The most common indicators of ankyloglossia are speech/articulation problems (64%), restricted movement (18%) and lactation problems/nutrition (8%) (Hall & Renfrew, 2005).
As for the results of surgery, improvement in mobility of the tongue and in the articulation of speech is the most reported effect (Klockars & Pitkaränta 2009; Obladen, 2009; Tuli & Singh, 2010). In Brazil, speech problems are very common in later ages, because the lingual frenectomy is not performed in early childhood. This can cause alteration and compensation of function related to the oral sensory-motor system, especially those that affect speech production. In this study, from the pre- operative period to the follow-up, we found that with the surgical release of the frenulum, the subjects' tongue movement amplitude increased, which yielded improved speech articulation, as well as an increase in the functional efficiency of the oral musculature for feeding functions, such as chewing and swallowing improved. During the immediate postoperative period, we observed improved speech production, for some adult patients. In some cases, however, change in speech production was not noticed in the early post frenectomy stage by random listeners or even the therapist, even though the extent of the functional articulation was observed to be significantly better.
Detailed characterization of the correlation between acoustic and perceptual characteristics of speech in subjects with abnormal lingual frenulum can assist in the process of treatment planning, therapeutic procedures and the evaluation process. There are no validated assessment protocols for treating patients with a disordered frenulum that have been used by medical professionals. In essence, there are no set ways to evaluate and interpret the results proposed. Marchesan (2004; 2005; 2010) has described speech problems as resulting from the alterations of the lingual frenulum and proposed protocols for evaluating this structure. The acoustic analysis, especially the characterization of the formant frequency of vowels, allows one to detail the mechanisms of the speech production, by inferring, from the acoustic data, the positioning of the tongue in the horizontal and vertical axes. Concerning this aspect, the aim in this study was to compare, from acoustic point of view, the formant frequencies (F1 and F2) for the seven oral vowels of Brazilian Portuguese Language (BP), when produced by the subject both pre- and post-lingual frenotomy (a minimum six-month interval).
MATERIAL AND METHODS
Seven subjects, 06y 3m-14y 07m, assessed and diagnosed with lingual frenulum alteration, without language and/or hearing disorders, were selected from patients attended by a Non-Government Organization. They participated in two sessions of speech data collection (audio recording).
The recordings were done in an acoustic environment, with the help of the BCA 2000 mixer (Behringer), Sound Forge software and AKG C140 headset microphone at two distinct moments: (a) pre-surgery and (b) post-surgery (
Figure 1). The criteria to be included were: (a) diagnosed lingual frenulum alteration, frenectomy indicated (pre-surgical planning), and (b) attended over six months of speech therapy post-surgical period. The subjects were clinically assessed by the lingual frenulum protocol, which evaluates lingual aspects (Marchesan, 2010) and those of the possibilities of movement, as well as their possible interference in the functions of speech, breathing, swallowing and chewing.
Table 1.
F1 and F2 frequency values (mean and standard deviation-SD) for the BP oral vowels produced by speakers before and after frenectomy.
Table 1.
F1 and F2 frequency values (mean and standard deviation-SD) for the BP oral vowels produced by speakers before and after frenectomy.
The speech samples consisted of words inserted within a carrier sentence, containing the seven oral vowels of the BP. The vowel sounds were acoustically analyzed in PRAAT, a free access software (available at
http://www.fon.hum.uva.nl/praat/). Formant frequencies (F1 and F2) values were obtained in Hz. The data were submitted to the CartaFormantesLogDoc.praat script, developed by Eduardo Velázquez (adaptation from Mietta & Lennes, 2004), in order to generate the vowel charts for both pre- and post- surgical data. Data were also compared to the International Phonetic Alphabet (IPA) description of Brazilian Portuguese (Barbosa & Albano, 2004).
Statistical Analysis (ANOVA) was also conducted to compare average frequencies of F1 and F2 for the different vowels at moments (a) and (b), with significance value established at p <0.05. The research project was approved by the CEFAC Ethics Committee: 082/11.
RESULTS
The F1 and F2 formant frequency values and their standard deviation values for pre- and post-surgical lingual frenectomy are displayed in
Table 1. The vowel charts, and their distribution of F1 and F2 values are presented in
Figure 2 and Figure 3 for pre- and post-surgical stages, respectively.
DISCUSSION
The findings support the assumption that lingual frenectomy increases the mobility of the tongue, making possible the restoration of oral functions previously described (Klockars, Pitkaränta, 2009; Aras et al., 2010; Acevedo et al., 2010; Knox, 2010; Tuli & Singh, 2010). However, the motor and timing controls of speech movements are not naturally restored after surgery and this condition mainly affects the adequacy of the speech production vowel patterns (Gregio et al., 2006; Ball & Gibbon, 2002). Access to acoustic analysis helps to identify different patterns of sound production in the pre- and post-surgical stages, so that the sounds classically described as “inaccurate” in the clinical evaluation, especially the vowels, can be analyzed to reveal the peculiarities in their acoustic structure.
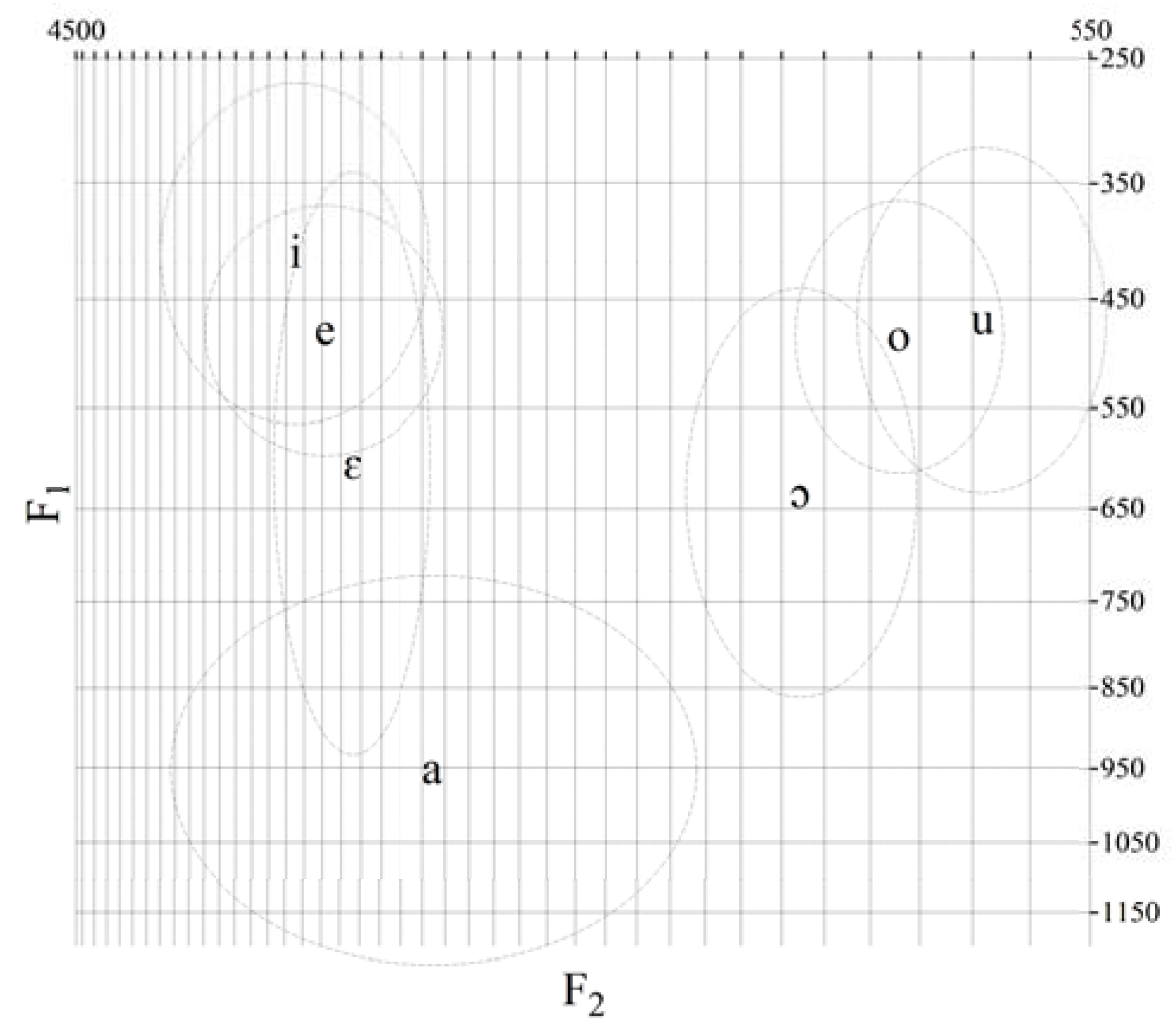
Figure 2.
Vowel chart (F1 and F2 distributions) for the BP oral vowels produced by speakers before frenectomy.
Figure 2.
Vowel chart (F1 and F2 distributions) for the BP oral vowels produced by speakers before frenectomy.
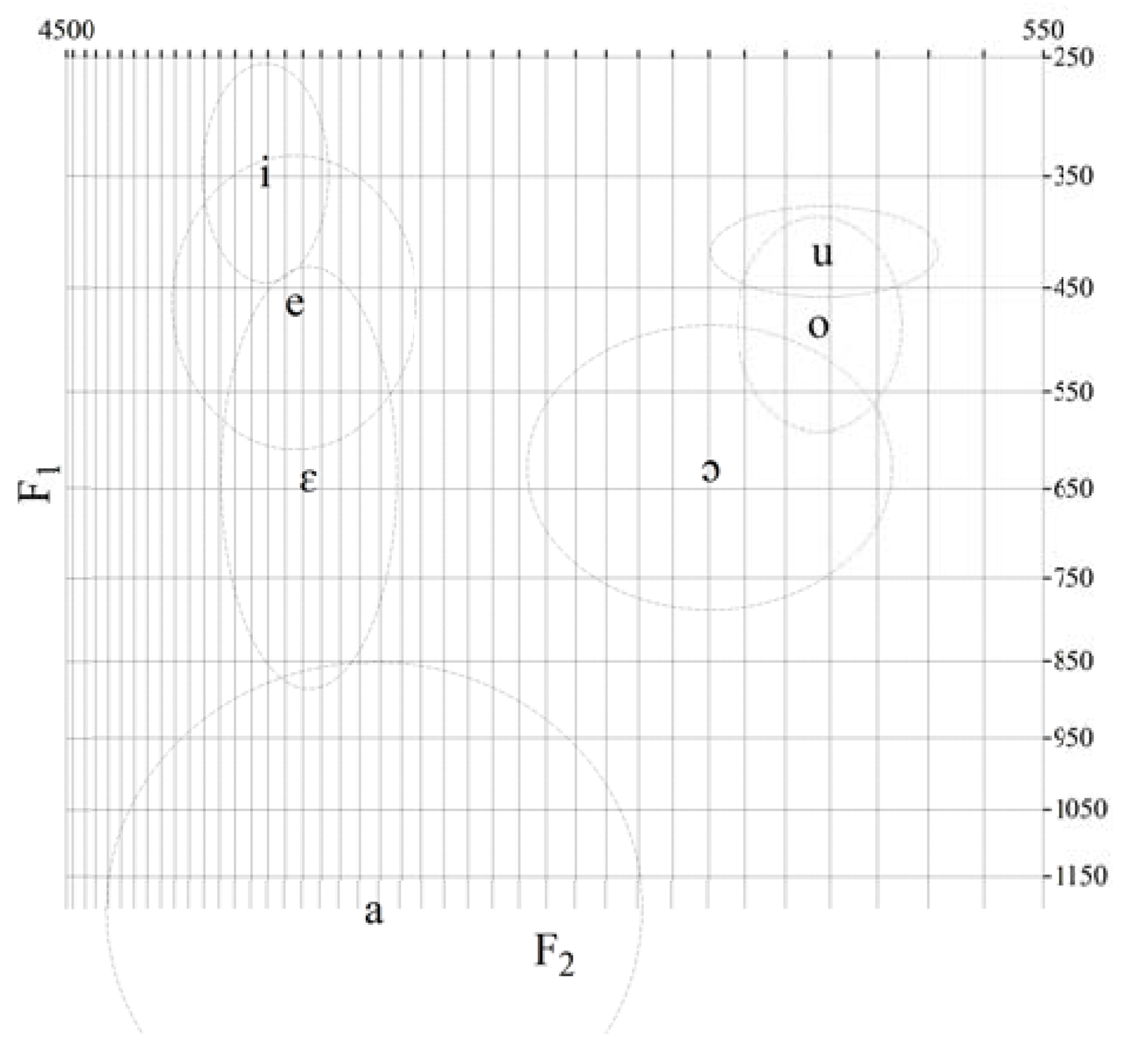
Figure 3.
Vowel chart (F1 and F2 distributions) for the BP oral vowels produced by speakers after frenectomy.
Figure 3.
Vowel chart (F1 and F2 distributions) for the BP oral vowels produced by speakers after frenectomy.
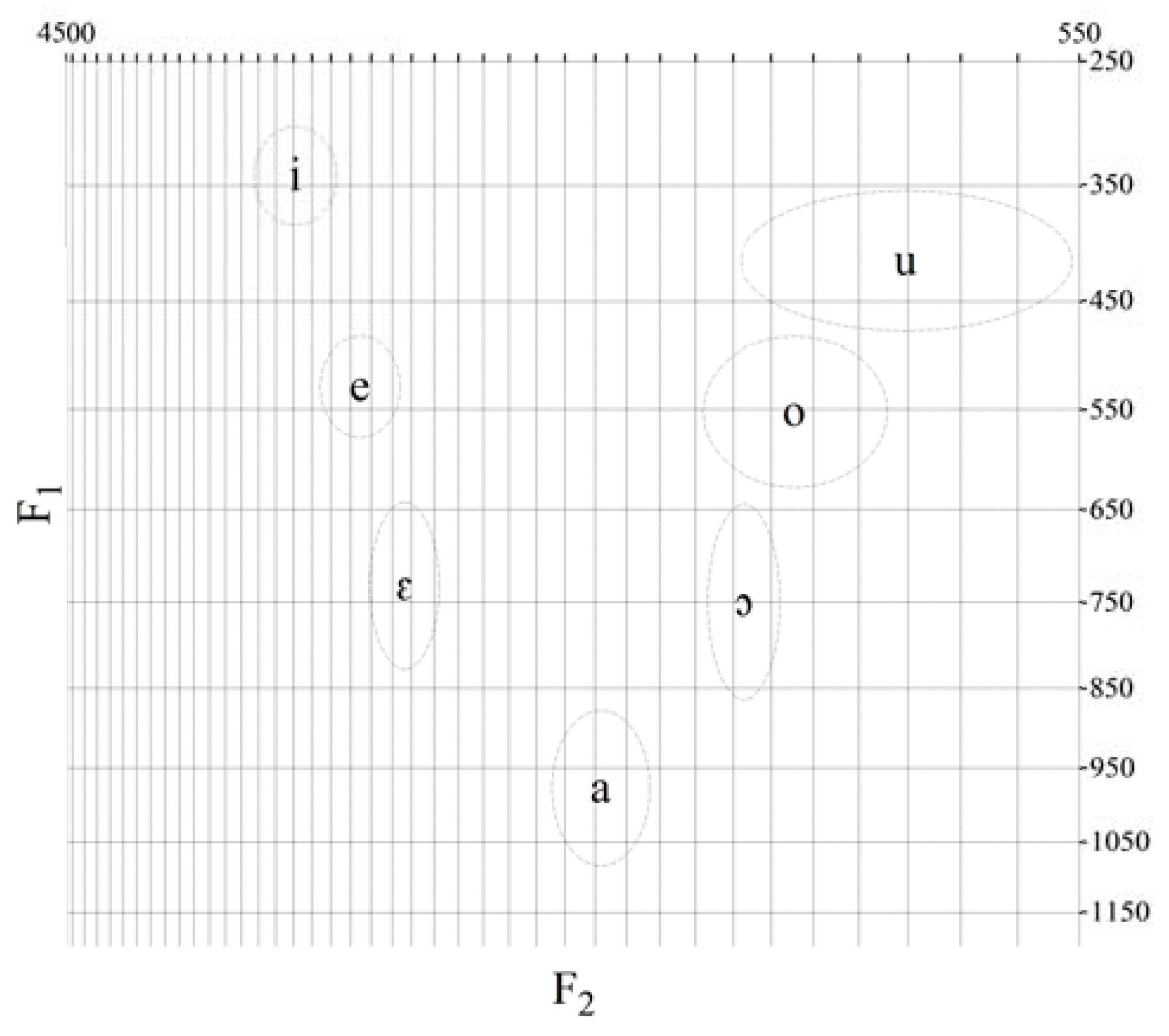
Figure 4.
Vowel chart (F1 and F2 distributions) for the BP oral vowels produced by children without lingual frenulum disorders (source: acoustic measures from Oliveira and Camargo (2016) p. 110).
Figure 4.
Vowel chart (F1 and F2 distributions) for the BP oral vowels produced by children without lingual frenulum disorders (source: acoustic measures from Oliveira and Camargo (2016) p. 110).
The observed changes in vowel formant frequencies values were interpreted as revealing a tendency towards greater anteriorization of the tongue. This included the production of vowels, including the high back vowels, over a six- month period after the lingual frenectomy. However, the limited excursion of the tongue in the anterior- posterior axis persisted, as we can observe in
Figure 2 and Figure 3.
The vowel charts (figures 2 and 3) enabled us to observe the overlapping of vowel spaces, pre – frenotomy stage (a) and post-frenotomy – stage (b). At stage (b) partial excursion of the anterior vowels [i], [e] and [ε] spaces, but they are still overlapped, suggesting that the excursion in height axis was not totally matched. The same can be indicated for posterior vowels, despite the fact that the vowel spaces are a little more differentiated post-operatively, there is still some evidence of limited excursion of the tongue body in the posterior vowels.
In relation to F1 values, the most significant changes were found to occur in [a], [e] and [u]. For [a], when compared to Oliveira & Camargo (2016), the data in our study indicated that the tongue body (and/or the jaw) was still lower. It is worth mentioning that we also found more tongue raising in the post-operative stage, for the vowels [e] and, especially, for [u]. For F2 mean and dispersion values, as displayed in
Table 1, the most significant changes were found to occur in the group of anterior vowels for [ε], which had a tendency to occur with the tongue in a more anterior tongue posture. For back vowel [u], changes in F2 values also found a tendency towards a more anterior tongue posture. Although statistically significant differences for F2 average values were not found for vowel [a], dispersion values indicate a tendency towards an anterior tongue posture. When comparing F1 and F2 values found in this study to the ones mentioned in studies of BP vowels produced by a population without speech alterations-
Figure 4 (Oliveira & Camargo 2016), it is notable that some of the values measured in this study do not fit the expectations for age and gender.
The results in our study were interpreted as showing a tendency, over a minimum six-month interval after lingual frenectomy, for greater anterior-wise mobilization of the tongue in the production of vowels, which includes both the back and the high vowels. Furthermore, it also revealed continued limited extension of the tongue in the anterior-posterior axis, especially for back vowels.
Based on that, speech therapy becomes a relevant and complementary treatment procedure. Because management of lingual frenulum alteration is still controversial among professionals (Obladen, 2009), the inclusion of protocols for evaluation and management of various alterations of the lingual frenulum may be beneficial. In reality, this outcome becomes more evident when considering that surgery is not commonly performed in young kids. In this case, acoustic analysis could prove to be an important tool to follow up the speech adaptations developed after frenectomy.
CONCLUSIONS
Changes in formant frequencies (F1 and F2) indicated that the range of motion and the function of the tongue improved over a period of six months after lingual frenectomy, revealing greater anterior mobilization, given speech therapy, although some limited height range was found to persist. The data reinforced the complexity of tongue (and jaw) movements during speech and the effects of frenectomy on speech production. Guidelines to speech rehabilitation can also be drawn from the discussed data.



{kind=link}
{kind=link}
{kind=link}
{kind=link}