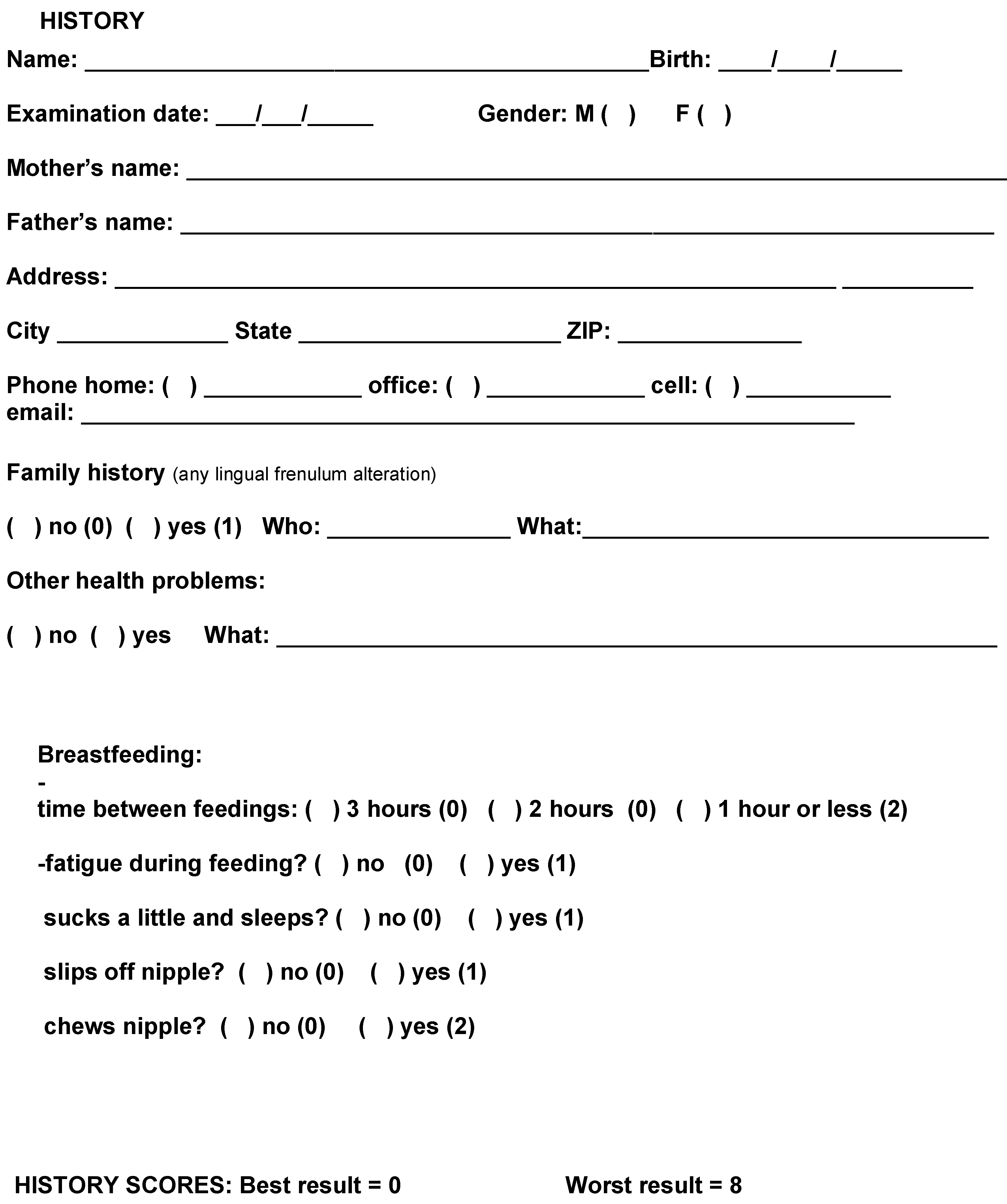
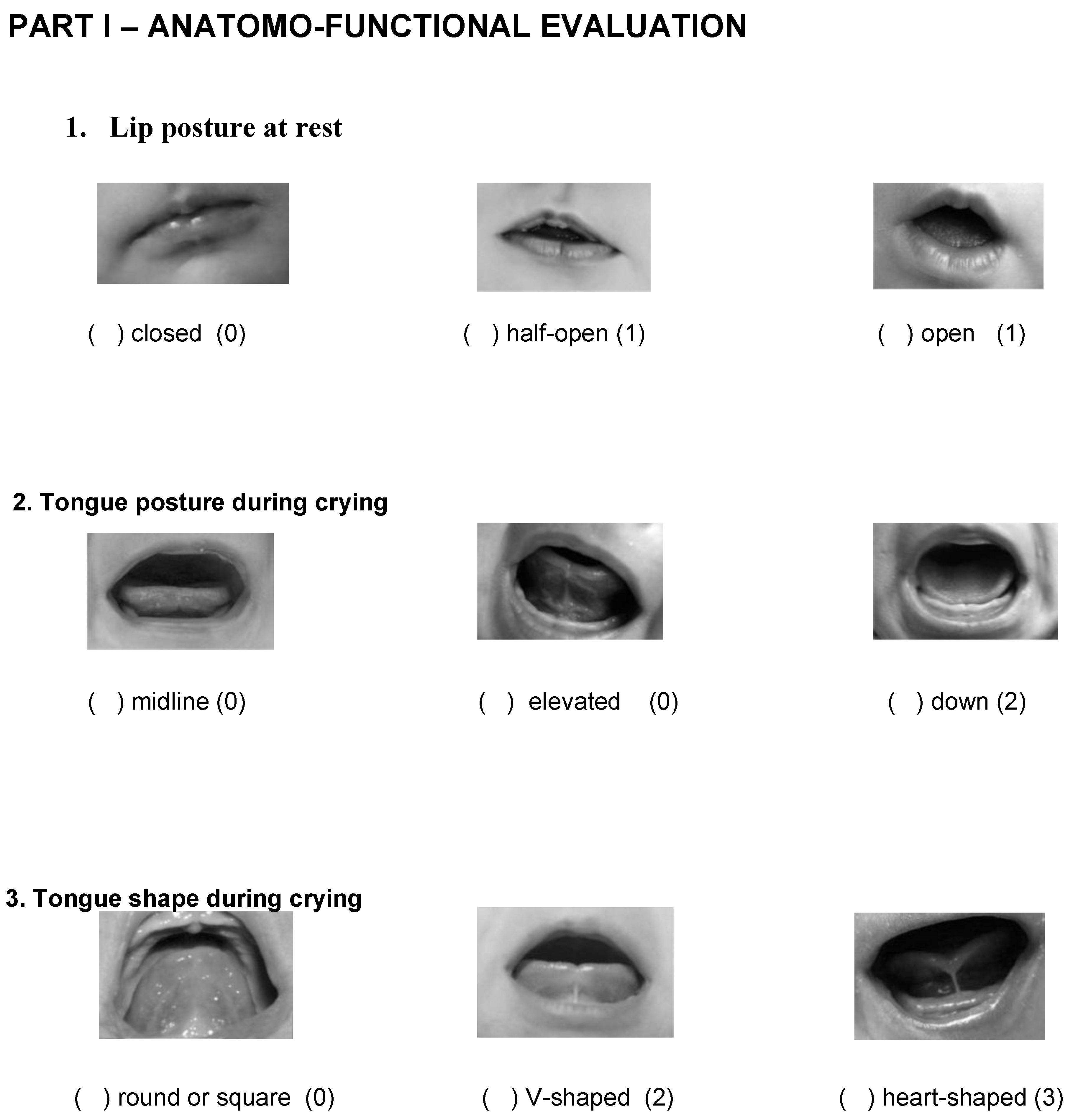
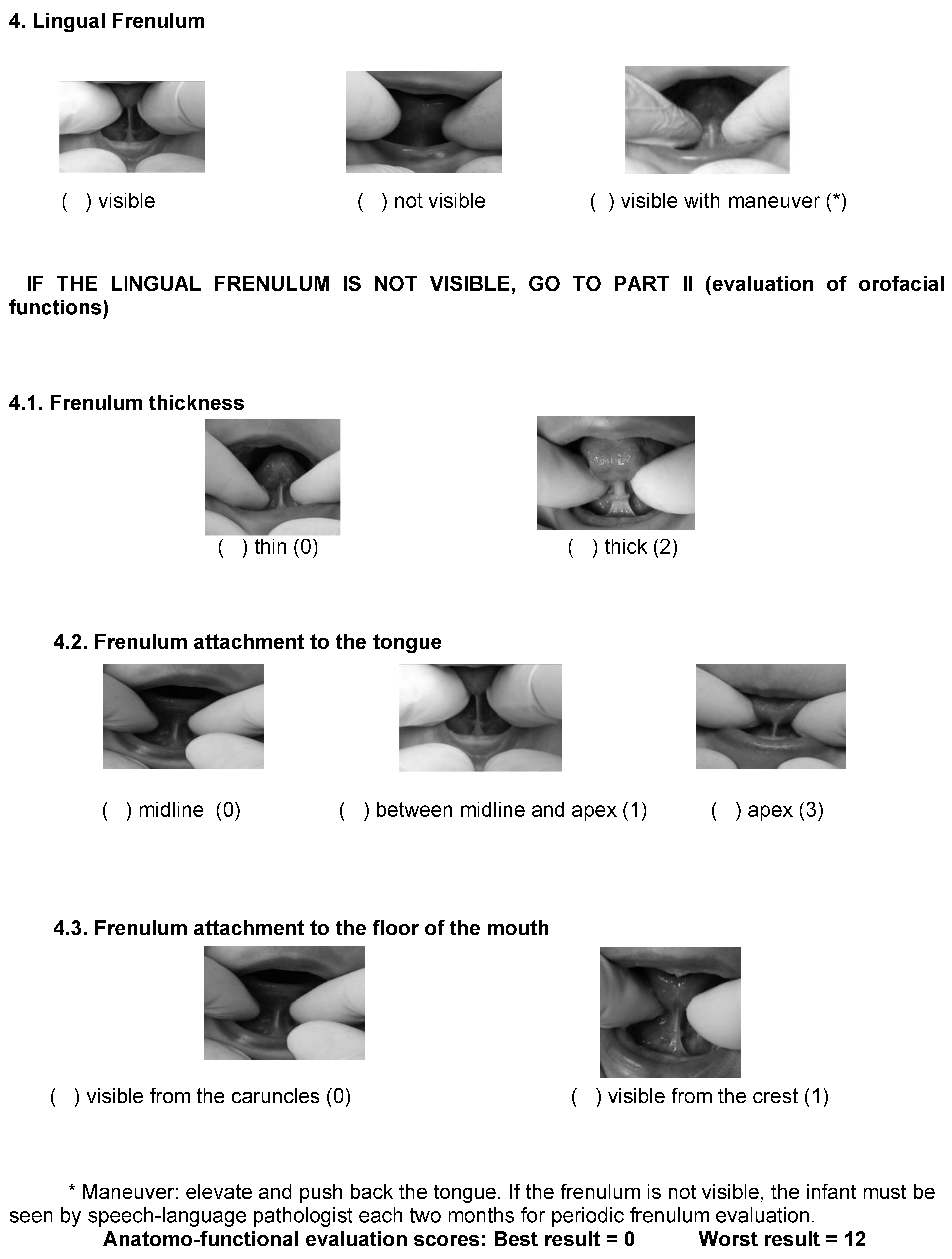
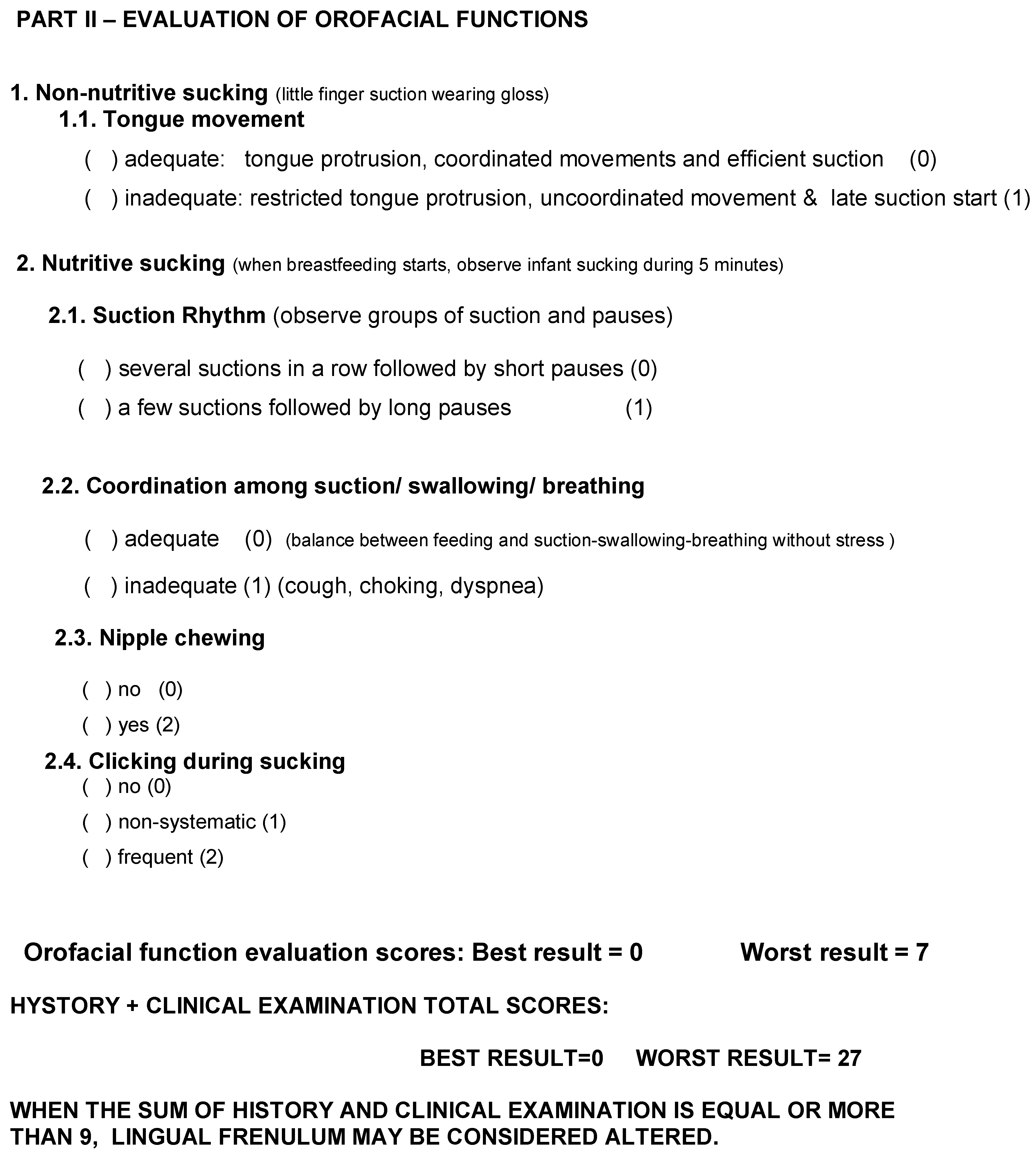
Lingual Frenulum Protocol With Scores for Infants

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:INTRODUCTION
METHODS
RESULTS
DISCUSSION
CONCLUSION
SPECIAL NOTE
Appendix A
References
- Ballard, J. L., C. E. Auer, and J. C. Khoury. 2002. Ankyloglossia: Assessment, incidence, and effect of frenuloplasty on the breastfeeding dyad. Journal of Pediatrics 110, 5: 1–6. [Google Scholar]
- Coryllos, E., C. W. Genna, and A. C. Salloum. 2004. Congenital tongue-tie and its impact in breastfeeding. Breastfeeding Newsletter, 1–6. [Google Scholar]
- Edmunds, J., S. Miles, and P. Fullbrook. 2011. Tongue-tie and breastfeeding: A review of the literature. Australian Breastfeeding 19, 1: 19–26. [Google Scholar]
- Geddes, D. T., J. C. Kent, H. L. McClellan, C. P. Garbin, L. M. Chadwick, and P. E. Hartmann. 2010. Sucking characteristics of successfully breastfeeding infants with ankyloglossia: A case series. Acta Pædiatrica 99: 301–303. [Google Scholar] [CrossRef]
- Geddes, D. T., D. B. Langton, I. Gollow, L. A. Jacobs, P. E. Hartmann, and K. Simmer. 2008. Frenulotomy for breastfeeding infants with ankyloglossia: Effect on milk removal and sucking mechanism as imaged by ultrasound. Pediatrics 122: e188–e194. [Google Scholar] [PubMed]
- Griffiths, D. M. 2004. Do tongue ties affect breastfeeding? Journal of Human Lactation 20, 4: 409–414. [Google Scholar] [PubMed]
- Hall, D. M. B., and M. J. Renfrew. 2005. Tongue-tie: Common problem or old wives tale. Archives Disability Childhood 90: 1211–1215. [Google Scholar]
- Hazelbaker, A. K. 1993. The assessment tool for lingual frenulum function (ATLFF): Use in a lactation consultant private practice. Thesis, Pacific Oaks College, Pasadena, CA. [Google Scholar]
- Hogan, M., C. Westcott, and M. Griffiths. 2005. Randomized, controlled trial of division of tongue-tie in infants with feeding problems. Journal of Paediatric Childhood Health 41: 246–250. [Google Scholar]
- Knox, I. 2010. Tongue tie and frenotomy in the breastfeeding newborn. NeoReviews 11, 9: 513–519. [Google Scholar] [CrossRef]
- Kotlow, L. A. 1999. Ankiloglossia (tongue-tie): A diagnostic and treatment quandary. Quintessence International 31: 276–278. [Google Scholar]
- Kotlow, L. A. 2011. Diagnosis and treatment of ankyloglossia and tied maxillary fraenum in infants using Er:YAG and 1064 diode lasers. European Archives of Paediatric Dentistry 12, 2. [Google Scholar] [CrossRef]
- Kupietzky, A., and E. Botzer. 2005. Ankyloglossia in the infant and young child: Clinical suggestions for diagnosis and management. Pediatric Dentistry 27, 1. [Google Scholar]
- Lalakea, M. L., and A. H. Messner. 2002. Ankyloglossia: The adolescent and adult perspective. Journal of Otolaryngology Head and Neck Surgery 127: 539–545. [Google Scholar]
- Marchesan, I. Q. 2005. Lingual frenulum: Quantitative evaluation proposal. International Journal of Orofacial Myology 31: 39–48. [Google Scholar] [CrossRef]
- Marchesan, I. Q. 2010. Protocolo de avaliação do frênulo da língua. Revista de Atualização Científica CEFAC 12, 6: 977–989. [Google Scholar] [CrossRef]
- Messner, A. H., M. L. Lalakea, J. Aby, J. MacMahon, and E. Bair. 2000. Ankyloglossia incidence and associated feeding difficulties. Archives of Otolaryngology Head and Neck Surgery 126: 36–39. [Google Scholar] [CrossRef] [PubMed]
- Messner, A. H., and M. L. Lalakea. 2002. The effect of ankyloglossia on speech in children. Archives of Otolaryngology Head and Neck Surgery 127: 539–545. [Google Scholar] [CrossRef]
- Miranda, B. H., and C. J. Milroy. 2010. A quick snip-A study of the impact of outpatient tongue-tie release on neonatal growth and breastfeeding. Journal Plastic Reconstruction Aesthetic Surgery 63, 9: e683–e685. [Google Scholar] [CrossRef]
- Navarro, N. P., and M. López. 2002. Anquiloglossia en niños de 5 a 11 años de edad. Diagnóstico y tratamiento. Revista Cubana Estomatologia 39, 3: 3–7. [Google Scholar]
- Ricke, L. A., N. J. Baker, D. J. Madlon-Kay, and T. A. DeFor. 2005. Newborn tongue-tie: Prevalence and effect on breast-feeding. Journal of the American Board Family Medicine 18, 1: 1–7. [Google Scholar] [CrossRef]
- Segal, L. M., R. Stephenso, M. Dawes, and P. Feldman. 2007. Prevalence, diagnosis, and treatment of ankyloglossia. Canadian Family Physician 53: 1027–1033. [Google Scholar] [PubMed]
- Singh, S., and R. D. Kent. 2000. Dictionary of speech-language pathology. San Diego, California: Singular’s. [Google Scholar]
- Suter, V. G., and M. M. Bornstein. 2009. Ankyloglossia: Facts and myths in diagnosis and treatment. Journal of Periodontology 80, 8: 1204–1219. [Google Scholar] [CrossRef] [PubMed]
- Tuli, A., and A. Singh. 2010. Monopolar diathermy used for correction of ankyloglossia. Journal of Indian Society of Pedodontics and Preventive Dentistry 28: 130–133. [Google Scholar] [PubMed]
- Voros-Balog, T., N. Vincze, and J. Banoczy. 2003. Prevalence of tongue lesions in Hungarian children. Journal of Oral Disease 9: 84–87. [Google Scholar]
- Wallace, H., and S. Clarke. 2006. Tongue tie-division in infants with breast-feeding difficulties. International Journal of Pediatric Otolaryngology 70, 7: 1257–1261. [Google Scholar]
© 2012 by the authors. 2012 Roberta Lopes de Castro Martinelli, Irene Queiroz Marchesan, Giédre Berretin-Felix.
Share and Cite
Martinelli, R.L.d.C.; Marachesan, I.Q.; Berretin-Felix, G. Lingual Frenulum Protocol With Scores for Infants. Int. J. Orofac. Myol. Myofunct. Ther. 2012, 38, 104-112. https://doi.org/10.52010/ijom.2012.38.1.8
Martinelli RLdC, Marachesan IQ, Berretin-Felix G. Lingual Frenulum Protocol With Scores for Infants. International Journal of Orofacial Myology and Myofunctional Therapy. 2012; 38(1):104-112. https://doi.org/10.52010/ijom.2012.38.1.8
Chicago/Turabian StyleMartinelli, Roberta Lopes de Castro, Irene Queiroz Marachesan, and Giedre Berretin-Felix. 2012. "Lingual Frenulum Protocol With Scores for Infants" International Journal of Orofacial Myology and Myofunctional Therapy 38, no. 1: 104-112. https://doi.org/10.52010/ijom.2012.38.1.8
APA StyleMartinelli, R. L. d. C., Marachesan, I. Q., & Berretin-Felix, G. (2012). Lingual Frenulum Protocol With Scores for Infants. International Journal of Orofacial Myology and Myofunctional Therapy, 38(1), 104-112. https://doi.org/10.52010/ijom.2012.38.1.8