Evaluation of a New Concept of Myofunctional Therapy in Children

Abstract
:INTRODUCTION
PATIENTS AND METHODS
Criteria
- Breathing: Organically induced mouth breathing, allergies and/or asthma were ruled out at baseline in all children with the finding “mouth breathing“. Before each clinical examination the mode of breathing was assessed. The children were unaware of being observed. Signs of habitual mouth breathing such as a continuously open mouth and cracks at the corners of the mouth were also recorded on the diagnostic sheet. The findings were supplemented by questioning both the parents and the children on the mode of breathing during the day and at night.
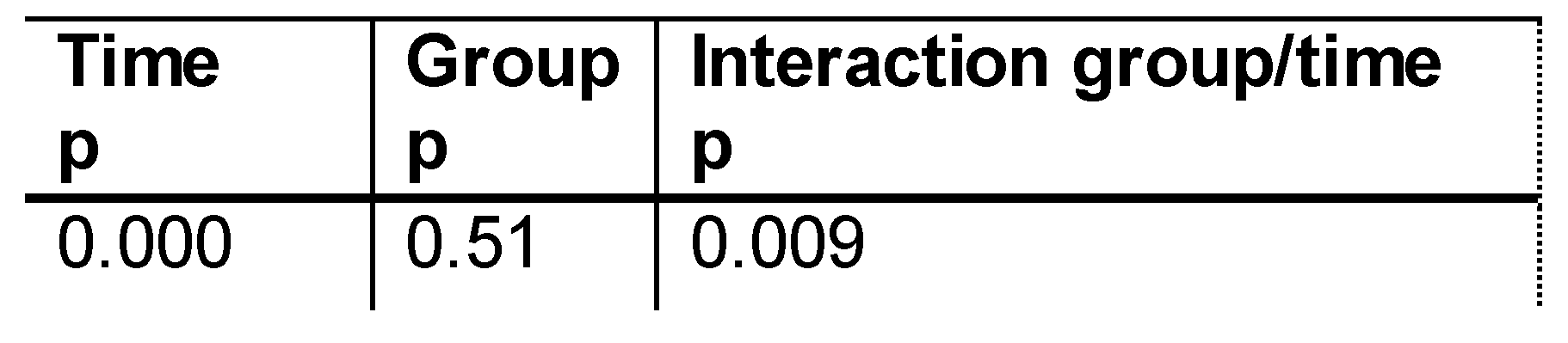
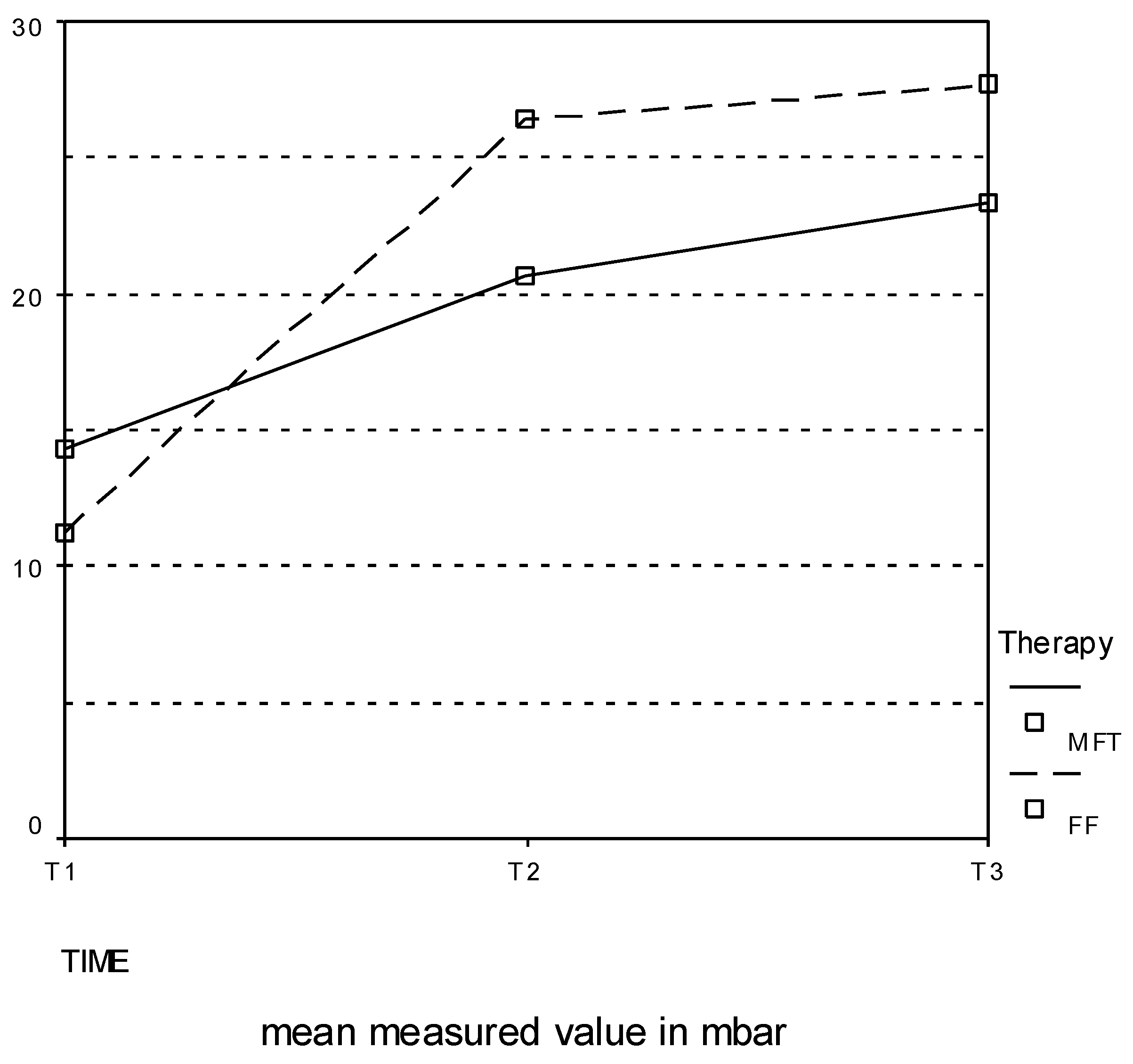
- Lip strength: Lip strength was measured with a Myo-Bar-Meter® (Akkuphon, Unna, Germany), a digital precision pressure gauge with a piezoresistive relative-pressure sensor. The measuring principle is based on overpressure measurement. The measured values provide information on the development of lip strength and thus on lip competence. Three measurements per patient were made at each examination time point, with lip competence being clinically rated.
- Swallowing pattern: Within the scope of the initial diagnosis, morphological factors impairing proper tongue position, e.g. a shortened frenulum or enlarged tonsils, were ruled out in all children. The existing swallowing pattern was assessed by clinical examination during mastication and speech and by means of palatography (Engelke, Engelke and Schwestka, 1990). After application of a paste to the tip and lateral edges of the tongue, the patient was asked to swallow. The color impressions were rated visually and documented by means of photos taken immediately thereafter.
- Sigmatism: This examination unit was performed exclusively by the speech/language pathologist. Within the scope of a conventional diagnosis by the speech/language pathologist (visual rating of the movement pattern during /s/ sound formation and acoustic rating), irregular /s/ sound formation was rated, followed by the movement pattern during articulation of the phonemes l, n, t, and d.
- Dropout rate28 patients attended all three scheduled examinations, 10 attended only the baseline diagnostic examination, and 17 failed to attend at least one examination. The loss of data within the individual groups is shown in Table 2. The most frequent reason given for absence was illness, holidays or lack of time on the part of the parents.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean age (months) | Minimum age (months) | Maximum age (months) | Standard deviation (± months) | |
| Control group | 101 | 55 | 203 | 35 |
| Study group | 100 | 47 | 190 | 38 |
Therapy Concepts
| Group | N = | Missing | |
|---|---|---|---|
| T0 | control | 19 | 0 |
| study | 26 | 0 | |
| total | 45 | 0 | |
| T1 | control | 14 | 5 |
| study | 19 | 7 | |
| total | 33 | 12 | |
| T2 | control | 13 | 6 |
| study | 17 | 9 | |
| total | 30 | 15 |
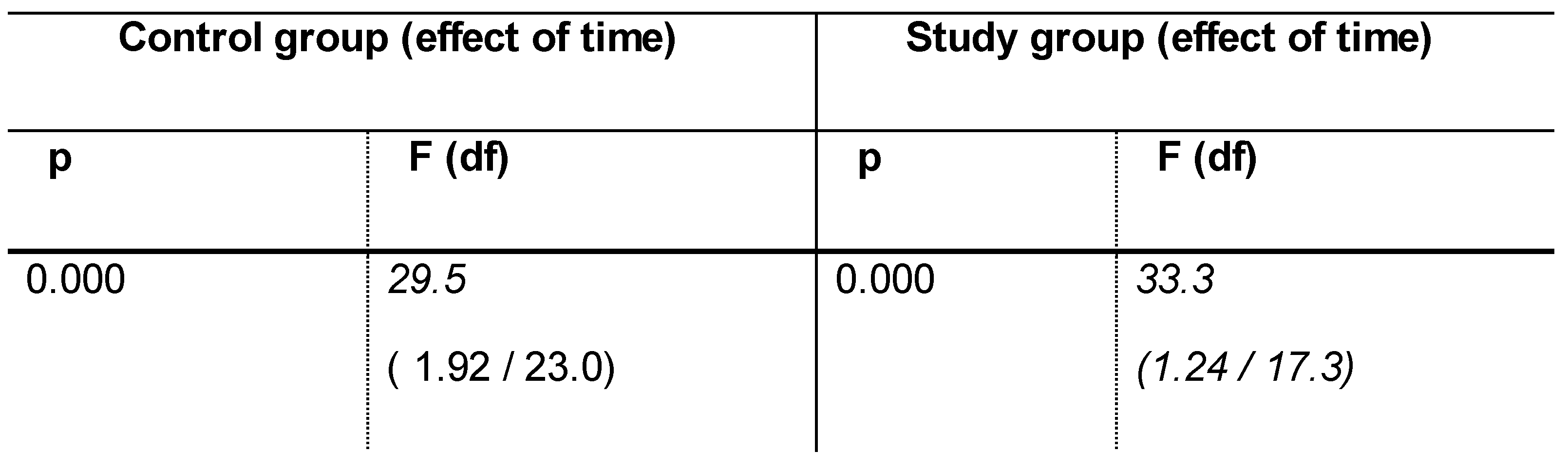
Statistical Analysis
- 2-way ANOVA with repeat
- measurement Friedman test
- Wilcoxon test
- Mann-Whitney U test
- Chi-square test
RESULTS
Breathing
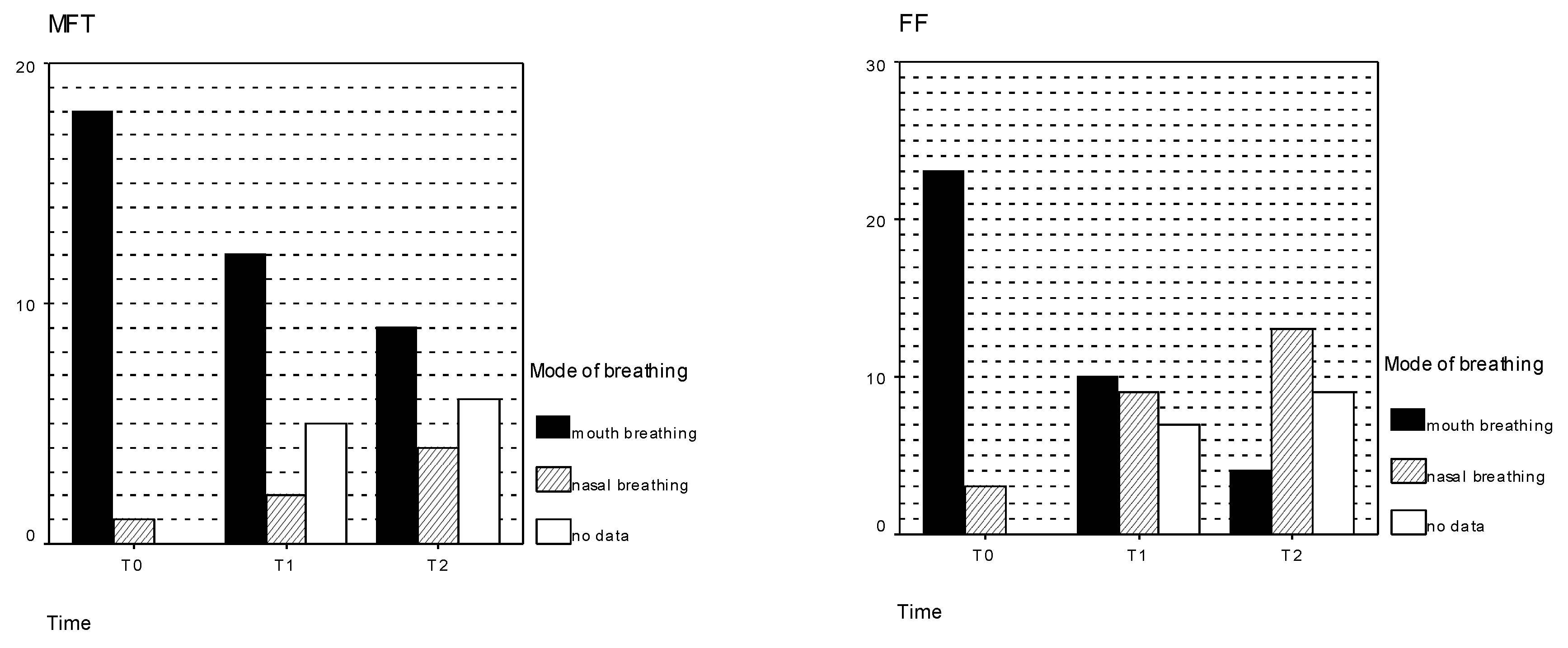
- At time point T0, 91.1% (41/45) of all examined children were habitual mouth breathers. This habit was observed in 94.7% (18/19) of the children in the control group [Figure 2a] and in 88.5% (23/26) of those in the study group [Figure 2b]. The significance value of p= 0.627 confirms that the two treatment groups were statistically comparable with each other at time point T0 [Table 3].
- At time point T1, 33.3% (11/33) of all children were already breathing through their nose, meaning that mouth breathing was still observed in 66.7% (22/33). The habitual mouth breathing had not been changed in 85.7% (n=12) of children in the control group and in 52.6% (n=10) of those in the study group. In the comparison of the two patient collectives at time point T1, the chi-square test revealed a statistical trend with a significance value of p=0.051.
- At time point T2, 43.3% (13/30) of the patients were still observed to be habitual mouth breathers. At this time point the intergroup difference was statistically significant (p=0.016): Continued habitual mouth breathing was recorded in 69.2% (9/13) of those in the control group and in 23.5% (4/17) of those in the study group.
| Control group | Study group | Total | ||
|---|---|---|---|---|
| T0 | 94.7% | 88.5% | 0.627 | 91.1% |
| T1 | 85.7% | 52.6% | 0.051 | 66.7% |
| T2 | 69.2% | 23.5% | 0.016* | 43.3% |
| p=0.097 | p=0.001** | p=0.000** |
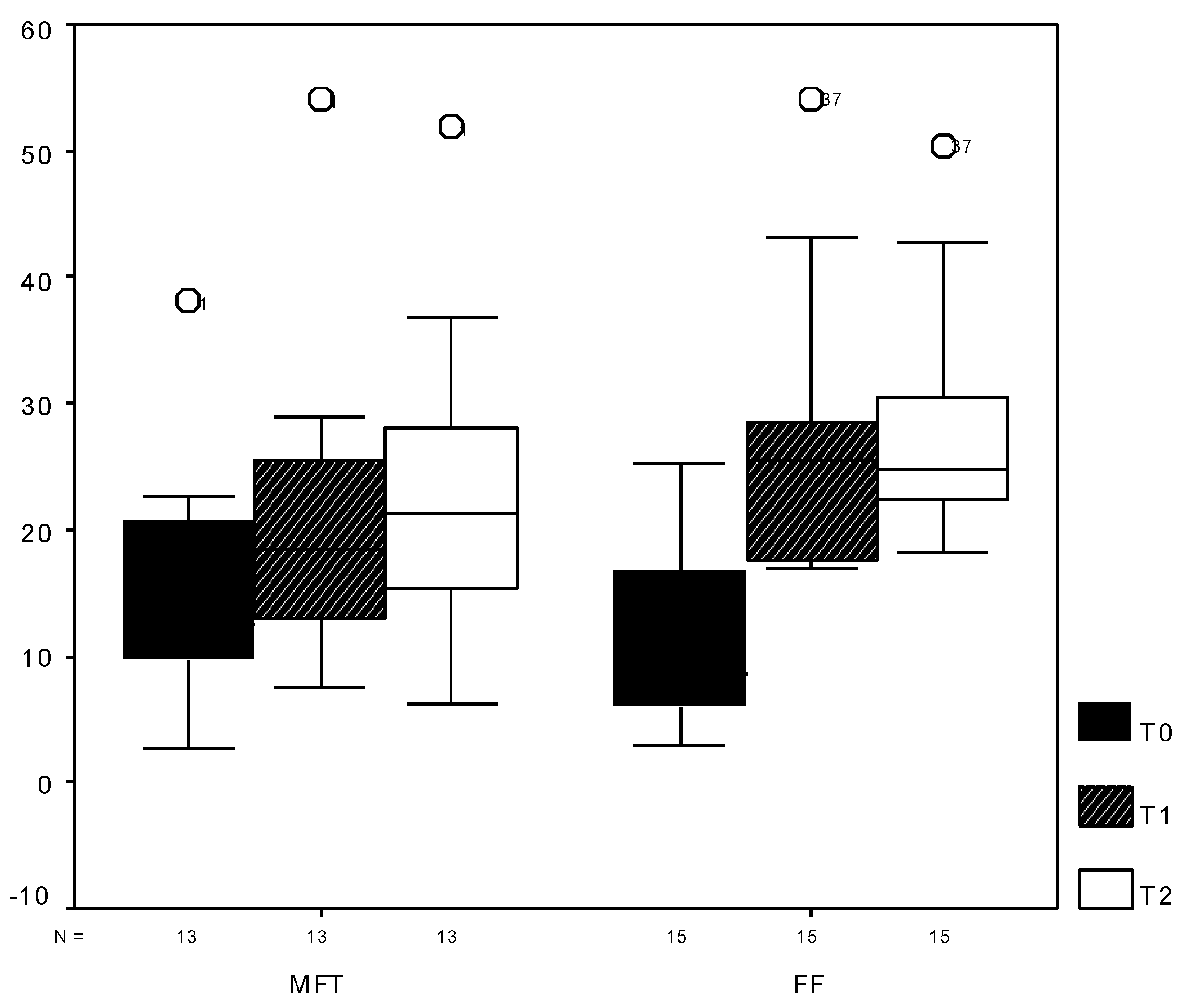
Development of Lip Strength
Swallowing Pattern
Sigmatism
DISCUSSION
| Control group | Study group | Total | ||
|---|---|---|---|---|
| T0 | 100% | 100% | 100% | |
| T1 | 92.9% | 73.7% | 0.171 | 81.8% |
| T2 | 76.9% | 35.3% | 0.028* | 53.3% |
| 0.097 | 0.000** | 0.000** |
| Control group | Study group | Total | ||
|---|---|---|---|---|
| T0 | 100% | 96.2% | 0.578 | 97.8% |
| T1 | 100% | 94.7% | 0.576 | 97% |
| T2 | 92.3% | 88.2% | 0.603 | 90% |
| 0.368 | 0.368 | 0.135 |
CONCLUSIONS AND RECOMMENDATIONS
References
- Bacha, S. M., and C. F. Rispoli. 1999. Myofunctional therapy: brief intervention. International Journal of Orofacial Myology 25: 37–47. [Google Scholar] [CrossRef]
- Benkert, K. K. 1997. The effectiveness of orofacial myofunctional therapy in improving dental occlusion. International Journal of Orofacial Myology 23: 35–46. [Google Scholar] [CrossRef]
- Bertolini, M. M., and J. Z. Paschoal. 2001. Prevalence of adapted swallowing in a population of school children. International Journal of Orofacial Myology 27: 33–43. [Google Scholar] [CrossRef]
- Biegenzahn, W., L. Fischman, and U. Mayrhofer-Krammel. 1992. Myofunctional therapy in patients with orofacial dysfunctions affecting speech. Folia Phoniatrica et Logopaedica 44, 5: 238–44. [Google Scholar] [CrossRef]
- Engelke, W., D. Engelke, and R. Schwestka. 1990. Zur klinischen und instrumentellen Untersuchung motorischer Zungenfunktionen. Deutsche Zahnärztliche Zeitschrift 45, 7: 11–6. [Google Scholar]
- Freiesleben, D., and V. Hahn. 1995. Grundlagen und Praxis der myofunktionellen Therapie unter besonderer Berücksichtigung des Einsatzes in der pädagogischen Sprachtherapie. Sprache Stimme Gehör 19: 118–25. [Google Scholar]
- Garretto, L. 2001. Orofacial myofunctional disorders related to malocclusion. International Journal of Orofacial Myology 27: 44–54. [Google Scholar] [CrossRef]
- Hubermann-Krakauer, L., and A. Guilherme. 2000. Relationship between mouth breathing and postural alterations of children: a descriptive analysis. International Journal of Orofacial Myology 26: 13–23. [Google Scholar] [CrossRef]
- Josell, S. D. 1995. Habits affecting dental and maxillofacial growth and development. Dental Clinics of North America 39, 4: 851–60. [Google Scholar] [CrossRef]
- Khinda, V., and N. Grewal. 1999. Relationship of tongue-thrust swallowing and anterior open bite with articulation disorders: a clinical study. Journal of the Indian Society of Pedodontics and Preventive Dentistry 17, 2: 33–9. [Google Scholar]
- Klocke, A., H. Korbmacher, and B. Kahl-Nieke. 2000. Der Status der myofunktionellen Therapie im Rahmen der interdisziplinären Zusammenarbeit aus der Sicht des Muskelfunktionstherapeuten. Sprache Stimme Gehör 24, 1: 38–43. [Google Scholar] [CrossRef]
- Korbmacher, H., and B. Kahl-Nieke. 2001. Optimizing interdisciplinary cooperation for patients with orofacial dysfunctions. Journal of Orofacial Orthopedics 62, 3: 246–50. [Google Scholar] [CrossRef]
- Krüger, M., and J. Tränkmann. 1997. Myofunktionelle Therapie. Sprache Stimme Gehör, 173–84. [Google Scholar]
- Landis, C. F. 1994. Applications of orofacial myofunctional techniques to speech therapy. International Journal of Orofacial Myology, 40–51. [Google Scholar] [CrossRef]
- Marchesan, I. Q., and L. R. Hubermann-Krakauer. 1996. The importance of respiratory activity in myofunctional therapy. International Journal of Orofacial Myology, 23–7. [Google Scholar] [CrossRef]
- Marchesan, I. Q. 2000. The speech pathology treatment with alterations of the stomatognathic system. International Journal of Orofacial Myology, 5–12. [Google Scholar] [CrossRef]
- Meyer, P. G. 2000. Tongue, lip and jaw differentiation and its relationship to orofacial myofunctional treatment. International Journal of Orofacial Myology, 44–52. [Google Scholar] [CrossRef]
- Pierce, R. B. 1983. The relationship between mouth breathing and tongue thrusting. International Journal of Orofacial Myology 9, 2: 4–5. [Google Scholar] [CrossRef]
- Pierce, R. B., and P Taylor. 2001. Rationale for including orofacial myofunctional therapy in university training programs. International Journal of Orofacial Myology, 24–32. [Google Scholar] [CrossRef]
- Satomi, M. 2001. The relationship of lip strength and lip sealing in MFT. International Journal of Orofacial Myology, 18–23. [Google Scholar] [CrossRef]
- Schopf, P. 1988. Myofunktionelle Übungen/ Myofunktionelle Therapie Wissenschaftliche Stellungnahme der Deutschen Gesellschaft für Zahn-, Mund-und Kieferheilkunde. Deutsche Zahnärztliche Zeitschrift. [Google Scholar]
- Sergl, H. G. 1988. 15 Thesen zur aktuellen Situation der myofunktionellen Therapie. Fortschritte der Kieferorthopädie 49: 312–314. [Google Scholar] [CrossRef] [PubMed]
- Umberger, F. G., and R. G. Johnston. 1997. The efficacy of oral myofunctional and coarticulation therapy. International Journal of Orofacial Myology, 3–9. [Google Scholar] [CrossRef]
- Wadsworth, S. D., C. A. Maul, and E. J. Stevens. 1998. The prevalence of orofacial myofunctional disorders among children identified with speech and language disorders in grades kindergarten through six. International Journal of Orofacial Myology 24: 1–19. [Google Scholar] [CrossRef]
© 2004 by the author. 2004 Korbmacher, H.M., Schwan, M., Berndsen, S., Bull, J., Kahl-Nieke, B.
Share and Cite
Korbmacher, H.M.; Schwan, M.; Berndsen, S.; Bull, J.; Kahl-Nieke, B. Evaluation of a New Concept of Myofunctional Therapy in Children. Int. J. Orofac. Myol. Myofunct. Ther. 2004, 30, 40-52. https://doi.org/10.52010/ijom.2004.30.1.4
Korbmacher HM, Schwan M, Berndsen S, Bull J, Kahl-Nieke B. Evaluation of a New Concept of Myofunctional Therapy in Children. International Journal of Orofacial Myology and Myofunctional Therapy. 2004; 30(1):40-52. https://doi.org/10.52010/ijom.2004.30.1.4
Chicago/Turabian StyleKorbmacher, Heike M., Marco Schwan, Sabine Berndsen, Julia Bull, and Bärbel Kahl-Nieke. 2004. "Evaluation of a New Concept of Myofunctional Therapy in Children" International Journal of Orofacial Myology and Myofunctional Therapy 30, no. 1: 40-52. https://doi.org/10.52010/ijom.2004.30.1.4
APA StyleKorbmacher, H. M., Schwan, M., Berndsen, S., Bull, J., & Kahl-Nieke, B. (2004). Evaluation of a New Concept of Myofunctional Therapy in Children. International Journal of Orofacial Myology and Myofunctional Therapy, 30(1), 40-52. https://doi.org/10.52010/ijom.2004.30.1.4