Abstract
Objective: This study evaluated the systemic bioavailability of L-thyroxine (L-T4) in healthy women following repeated cutaneous application of a new gel formulation containing L-T4 and escin. Plasma concentrations of free triiodothyronine (FT3), reverse triiodothyronine (rT3), and thyroid-stimulating hormone (TSH) were also assessed, along with local and systemic tolerability. Methods: Thirty healthy women participated in a single-group, open-label trial. L-thyroxine gel was applied at 20 g/day for the first 2 days and 10 g/day for the following 26 days (equivalent to 20 mg/day and 10 mg/day of L-T4, respectively). Blood samples were collected at Baseline, 5 and 24 h after the first application, and on Days 14, 28 (End of Treatment, EOT), and 42 (End of Study, EOS). Tolerability and safety were monitored throughout. Results: Plasma FT4 concentrations remained stable throughout the study, with no clinically significant changes from Baseline (1.13 ± 0.15 ng/dL) to EOT (1.11 ± 0.13 ng/dL). FT3 and TSH levels also remained within physiological ranges, with only a transient, non-clinically relevant decrease observed 5 h after the first application. No changes in rT3 concentrations were detected at any time point. No serious adverse events were reported. Conclusions: This study confirms that repeated application of L-thyroxine/escin gel over 28 days (total exposure of 300 g) does not affect systemic thyroid hormone levels and is well tolerated in healthy women. These findings support the hypothesis that intact skin acts as an effective barrier to transdermal L-T4 absorption.
1. Introduction
Thyroid hormones exert a broad spectrum of physiological effects on the skin, including modulation of keratinocyte proliferation and differentiation, dermal matrix remodeling, and hair follicle cycling [1,2]. Both α and β isoforms of thyroid hormone receptors are widely expressed in cutaneous tissues [3,4,5]. In vitro, L-thyroxine (T4) stimulates keratin gene expression in human keratinocytes and modulates extracellular matrix homeostasis [2]. In vivo studies have demonstrated that T4 enhances wound healing and promotes hair growth [6,7].
Topical formulations containing supraphysiological concentrations of T4 have been used cosmetically to reduce localized fat deposits associated with cellulite. These effects are attributed to the hormone’s lipolytic activity and its ability to reduce dermal glycosaminoglycan accumulation and fibroblast elastase-like activity, which are linked to dermal laxity and fluid retention [8,9].
T4 itself is a prohormone with limited biological activity; it must undergo enzymatic conversion to the more active L-triiodothyronine (T3) via outer-ring deiodination by type 1 or type 2 deiodinases (D1, D2). Conversely, inner-ring deiodination by type 3 deiodinase (D3) inactivates T4 and T3, resulting in the production of reverse T3 (rT3) or T2, respectively. These enzymatic processes are known to occur in human skin, particularly within keratinocytes and fibroblasts [10].
Although T4-based creams have been marketed and applied topically for decades, clinical data on their systemic absorption remain limited. Previous investigations suggested minimal systemic bioavailability due to dermal metabolic inactivation and the skin’s barrier function [10,11]. Nonetheless, due to the supratherapeutic dose of L-T4 used in such formulations, the potential for drug-induced thyrotoxicosis cannot be excluded.
The primary objective of this study was to determine whether topical administration of a new gel formulation containing L-T4 and escin affects systemic thyroid hormone levels in healthy women. Secondary objectives included the evaluation of the gel’s local and systemic tolerability.
2. Materials and Methods
2.1. Study Design and Setting
This was a single-center, phase 1, single-group, open-label study conducted between January and November 2019 at the Clinical Pharmacology Centre for Drug Experimentation, Pisa University Hospital, Italy. The study was designed to evaluate the systemic bioavailability of L-T4 following repeated cutaneous application of an investigational gel formulation. Clinical trial was first entered in the EudraCT database on 4 November 2020 (EudraCT code: 2018-002380-26). The study was conducted in accordance with the Declaration of Helsinki and approved by the North-West Tuscany Area Ethics Committee—Italy (approval recorded on the regional platform with code n. 1364 on 13 September 2018) and by the Italian Competent Authority (Letter with official protocol number AIFA/SC/p/100984 on 12 September 2018). A completed TREND checklist (Transparent Reporting of Evaluations with Nonrandomized Designs) has been provided to ensure comprehensive and transparent reporting of the study.
2.2. Investigational Medicinal Product (IMP)
The IMP was a gel containing L-thyroxine and escin, marketed in Italy as Somatoline® gel (AIC n. 022816122). Each 10 g of gel contained 10 mg of L-T4 and 30 mg of escin. The gel was applied to both thighs daily: 10 g per thigh (20 g/day total) during the first 2 days, followed by 5 g per thigh (10 g/day total) for the remaining 26 days. The first application of the investigational product was performed under direct supervision at the clinical site by trained staff on Day 0. During this visit, participants were instructed on the correct technique for applying the gel to the thighs, including the appropriate amount, method, and duration of massage to ensure uniform distribution. Subjects were advised to wash and thoroughly dry both thighs, then apply the product to the target area (not exceeding 15 cm per side) using firm massage for several minutes until fully absorbed—defined as the absence of visible residue, stickiness, or film on the skin.
At discharge, each participant received a clinical diary with illustrated instructions for home administration and a daily log to record applications and report issues such as incomplete absorption or local reactions.
IMP use was monitored via the diary and by weighing the dispenser before each dispensation and upon return. Residual product was recorded in the IMP return log to objectively assess adherence.
This combination of supervised training, written instructions, self-reporting, and IMP dispenser weight monitoring was considered appropriate to support protocol compliance in the home setting.
2.3. Objectives and Endpoints
The primary objective was to assess the systemic bioavailability of L-T4 after repeated topical application. Secondary objectives included the evaluation of plasma levels of FT3, rT3, and TSH, as well as the assessment of local and systemic safety and tolerability. The primary endpoint was the change in plasma FT4 levels from Baseline to Day 28 and Day 42. Secondary endpoints included changes in FT3, rT3, and TSH levels at the same time points. Safety endpoints included adverse event reporting, vital signs, ECG, and local skin tolerability.
2.4. Participants and Biological Sample Management
Thirty Caucasian healthy women, aged 18–50 years, with a BMI between 18.5 and 30 kg/m², were enrolled. Inclusion criteria included no history of or ongoing relevant disorders, a normal physical examination, ECG, and laboratory values, including normal thyroid function. Use of medications or supplements containing iodine or interfering with thyroid metabolism was prohibited. Blood samples for thyroid hormone analysis were collected at Baseline, 5 h and 24 h post-first application, and on Days 14, 28 (EOT), and 42 (EOS). FT4, FT3, and TSH samples were analyzed on the same day. In particular, all subjects had to have normal baseline thyroid function (at screening visit −14), defined as serum levels of TSH between 0.4 and 4.0 µIU/mL; Free T4 (FT4) between 0.7 and 1.7 ng/dL; Free T3 (FT3) between 2.7 and 5.7 pg/mL. rT3 samples were stored at −80 °C and batch analyzed using ELISA (DBC Reverse T3 ELISA®, Diagnostics Biochem Canada Inc., 384 Neptune Crescent, London, ON, Canada).
2.5. Safety Assessment
Safety was monitored through adverse events (AEs), vital signs (including SBP, DBP, HR, respiratory rate, and temperature), ECGs, and laboratory tests. Local tolerability was assessed by both investigators and participants using a 0–3 scale for erythema, swelling, and itching, according to the Common Terminology Criteria for Adverse Events (CTCAE), Version 5.0 (U.S. Department of Health and Human Services, National Cancer Institute (NCI), Bethesda, MD, USA) [12].
2.6. Statistical and Analytical Plan
The sample size was estimated based on previous data obtained using a similar topical formulation (Certan et al., 2013) [11], where the mean T4 concentration was 11.0 ± 1.2 pg/mL. A minimum of 26 participants was calculated to ensure that changes in T4 levels could be detected within a 99% confidence interval (CI) of ±0.7 pg/mL. To account for a potential dropout rate of 15%, a total of 30 subjects were enrolled. The study database was managed using the electronic data capture system PheedIt, part of the SAS Clinical Data Management suite (SAS Institute Inc., Cary, NC, USA), provided and supported by DEDAGROUP Public Services S.r.l., Trento, Italy., Data analysis was performed using SAS® version 9.4 for Windows (SAS Institute Inc., Cary, NC, USA). Analyses were conducted on three predefined populations: the Safety Population, the Intention-to-Treat (ITT) Population, and the Per Protocol (PP) Population.
Quantitative data were summarized using descriptive statistics, including the mean, standard deviation (SD), median, minimum, and maximum values. Categorical data were expressed as counts and percentages. Where appropriate, changes from the Baseline were evaluated using a one-way analysis of variance (ANOVA) for repeated measures. The McNemar test was used for analyzing changes in frequency distributions.
Changes in plasma concentrations of FT4, FT3, rT3, and TSH were analyzed by time point relative to the Baseline. For each parameter, descriptive statistics and changes from the Baseline were calculated. Bioavailability assessments were based on the analysis of continuous variables by visit using ANOVA models.
2.7. Study Plan
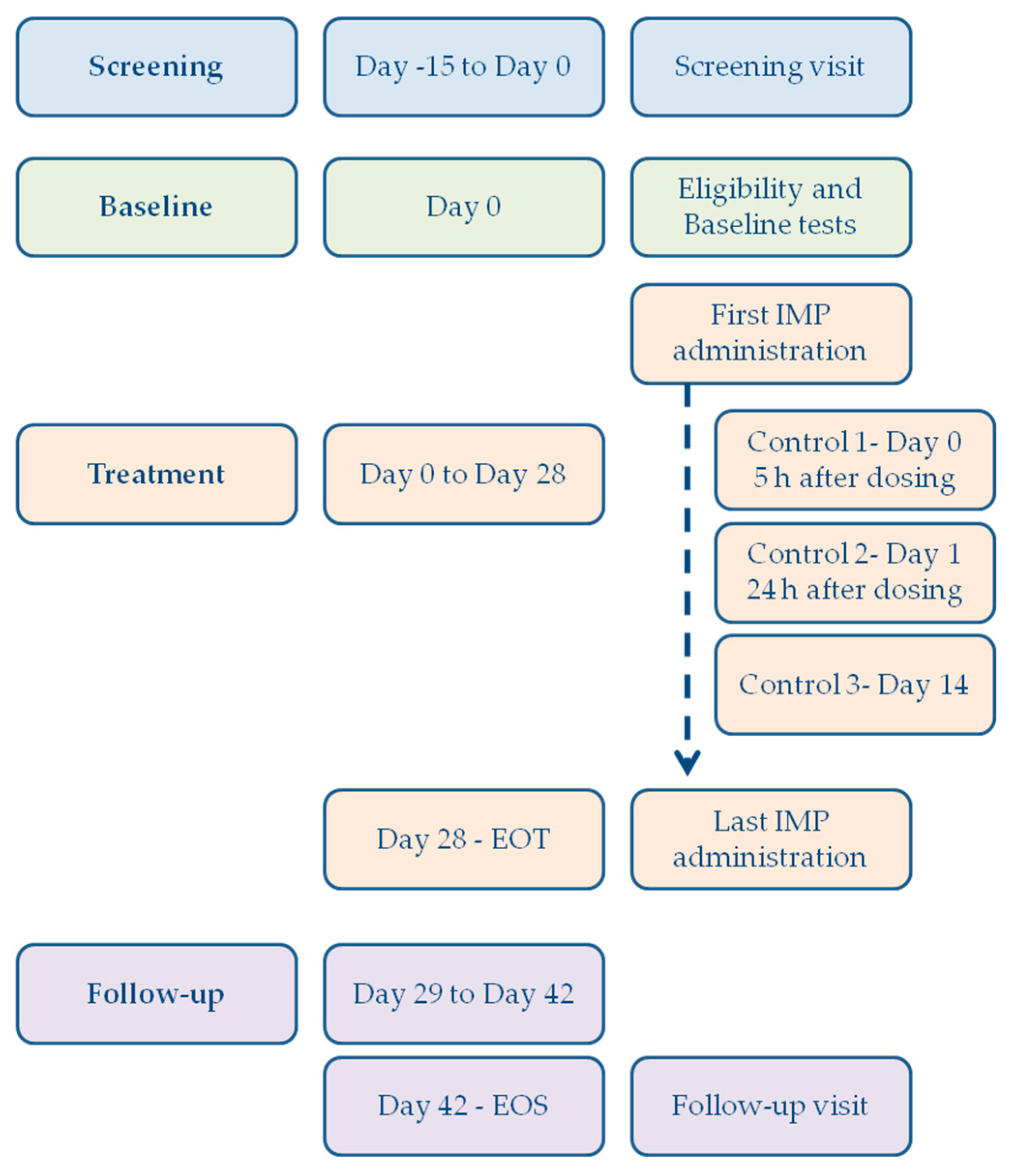
The overall conduct of the study, including the flow chart, the timing of assessments, procedures, and treatment schedule, is summarized in the study flow chart and detailed in Figure 1 and Table 1, respectively. The schedule outlines all key evaluations from screening through the end-of-study visit, including the timing of hormone measurements, safety assessments, and application of the investigational product.
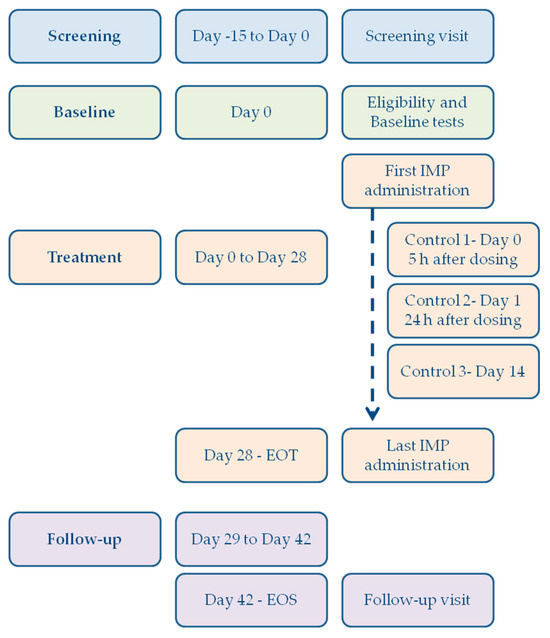
Figure 1.
Study flow chart. Overview of the study design, including screening period (Day −15 to Day 0), baseline assessments, and treatment phase with first and last application of the investigational medicinal product (IMP). Control visits were conducted on Day 0 (5 h post-dosing), Day 1 (24 h post-dosing), and Day 14, with the End of Treatment (EOT) visit on Day 28 and the End of Study (EOS) on Day 42.

Table 1.
Schedule of assessments. SBP: systolic blood pressure; SDB: diastolic blood pressure; HR: heart rate; RF: respiratory rate; BT: body temperature; EOT: End of Treatment; EOS: End of Study.
3. Results
3.1. Study Population
A total of 34 healthy female volunteers were screened. Four subjects did not meet the inclusion criteria and were excluded. Thirty participants were enrolled and completed the study, with no major or critical protocol deviations recorded; the entire study population was included in the Safety Population, the ITT, and the PP analyses. Demographic and anthropometric characteristics are summarized in Table 2.
Table 2.
Demographic and anthropometric characteristics of the study population.
3.2. Systemic Bioavailability of FT4
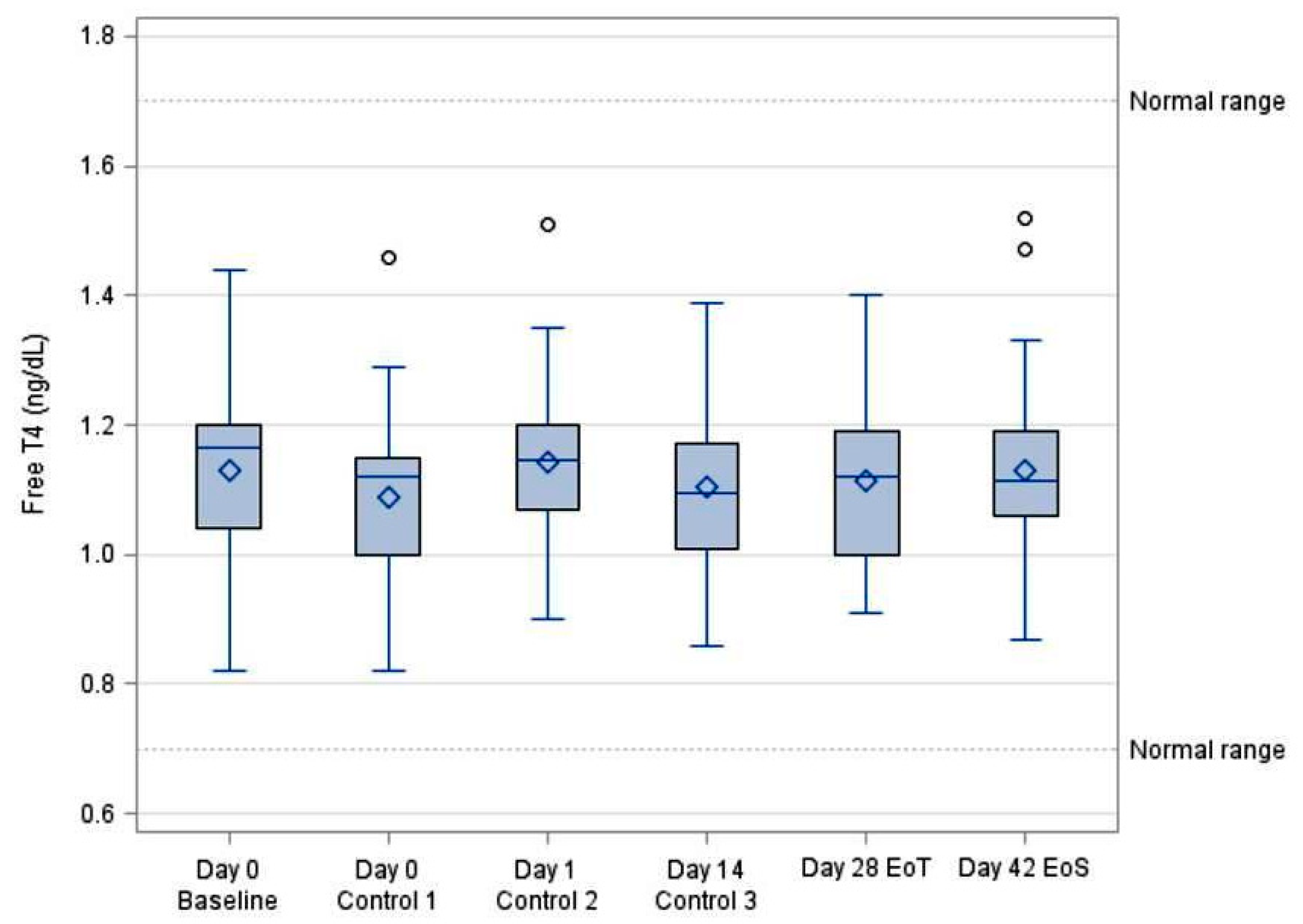
Plasma concentrations of FT4 were measured at Baseline, 5 h and 24 h post-first application, and on Days 14, 28 (EOT), and 42 (EOS). FT4 levels remained stable throughout the study, with no statistically or clinically significant changes from Baseline (1.13 ± 0.15 ng/dL) to EOT (1.11 ± 0.13 ng/dL). The maximum observed variation was a minor decrease at 5 h (−3.7%), which was not statistically significant (p > 0.05, ANOVA). Detailed values are reported in Table 3 and depicted in Figure 2.
Table 3.
Plasma FT4 concentrations (ng/dL) measured in the full study population (N = 30).
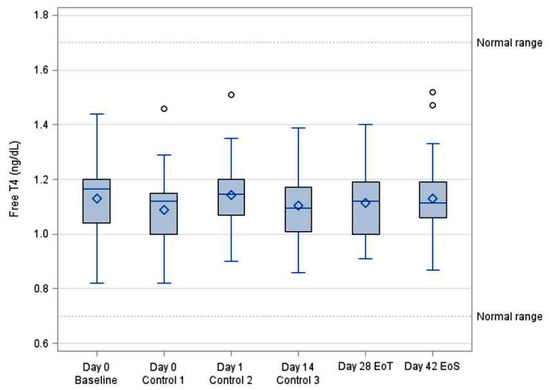
Figure 2.
Trend of free FT4 over time (Boxplot).
3.3. Systemic Bioavailability of FT3
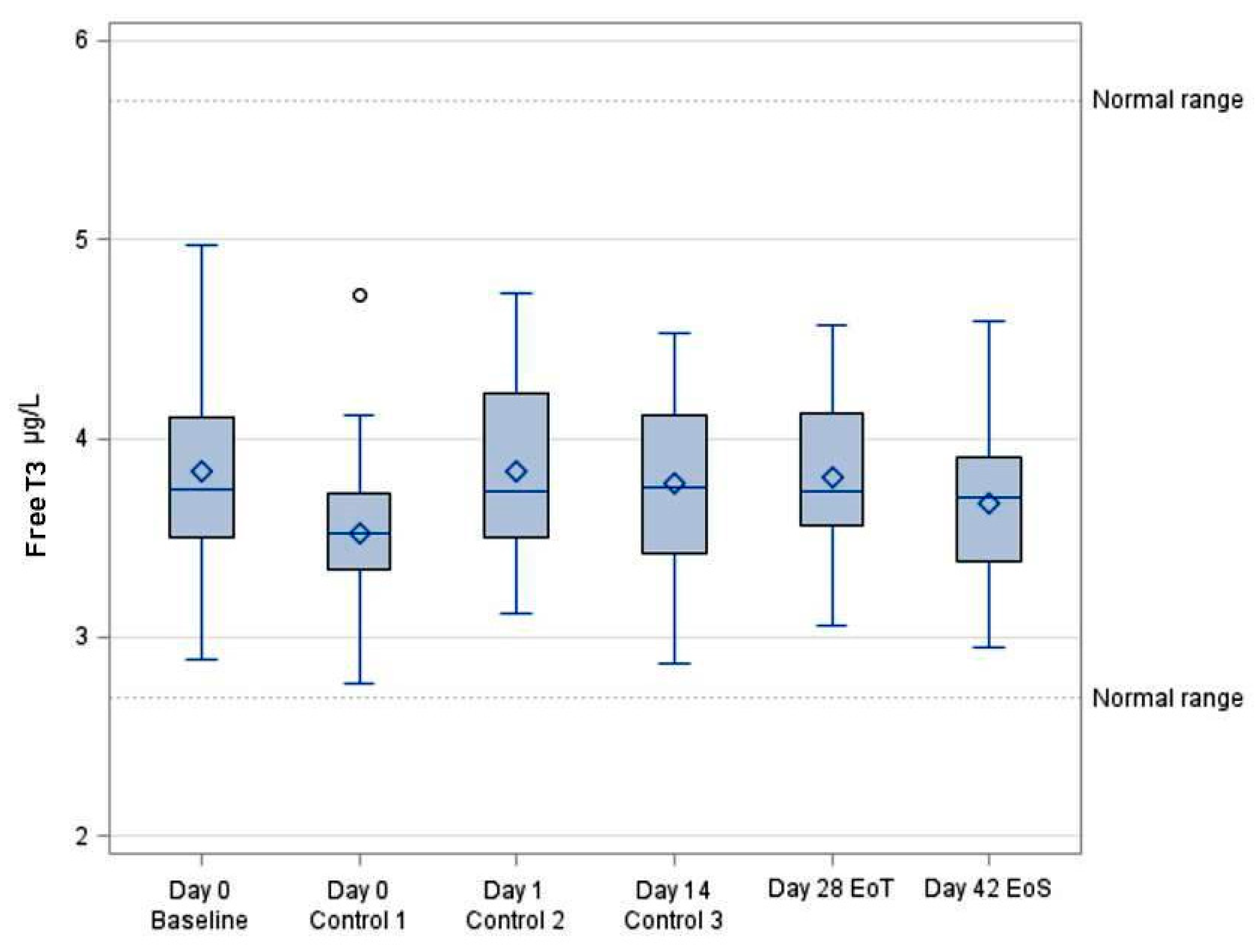
FT3 levels showed a slight but statistically significant decrease at 5 h post-application (3.83 ± 0.52 to 3.52 ± 0.44 ng/dL, p < 0.05), consistent with known circadian fluctuations. No significant changes were observed at subsequent time points. The temporal trend is reported in Table 4 and visualized in Figure 3.
Table 4.
Plasma concentrations of FT3 (ng/dL) measured in the full study population (N = 30).
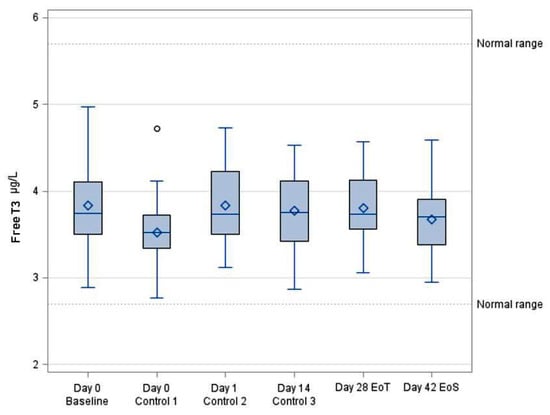
Figure 3.
Trend of FT3 over time (Boxplot).
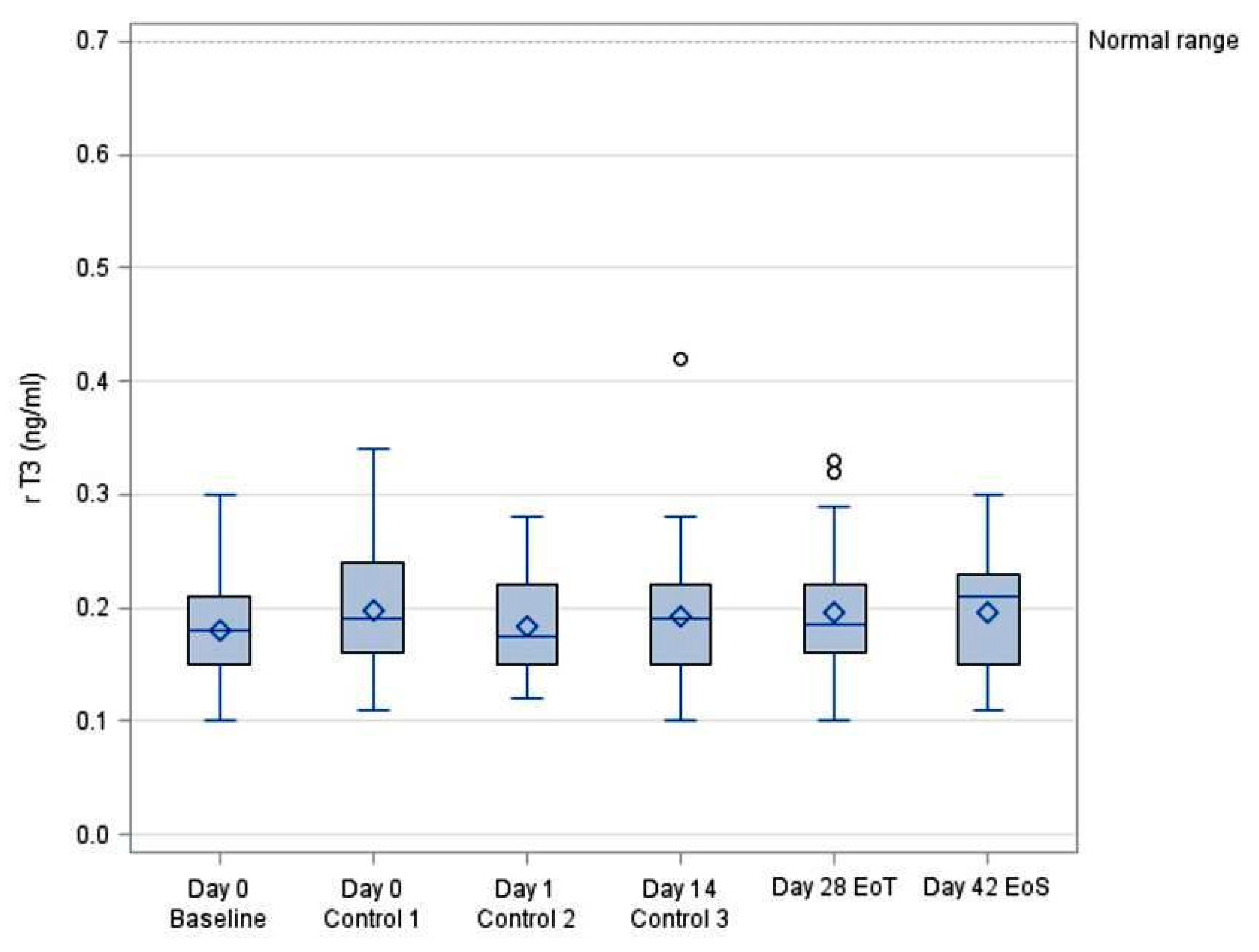
3.4. Systemic Bioavailability of rT3
rT3 concentrations remained unchanged across all study visits. A minor, non-significant increase was observed at 5 h and Day 28; however, these fluctuations were within the expected physiological range. Results are summarized in Table 5 and Figure 4.
Table 5.
Plasma concentrations of rT3 (ng/dL) measured in the full study population (N = 30).
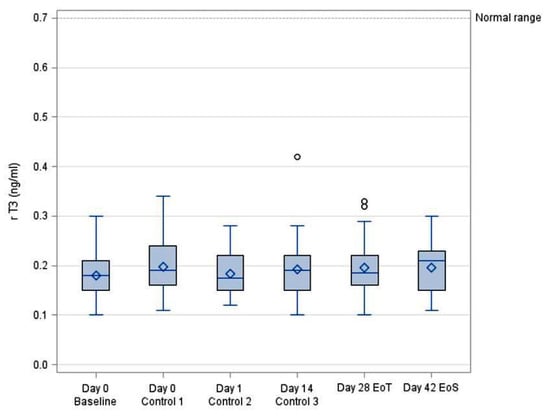
Figure 4.
Trend of rT3 over time (Boxplot).
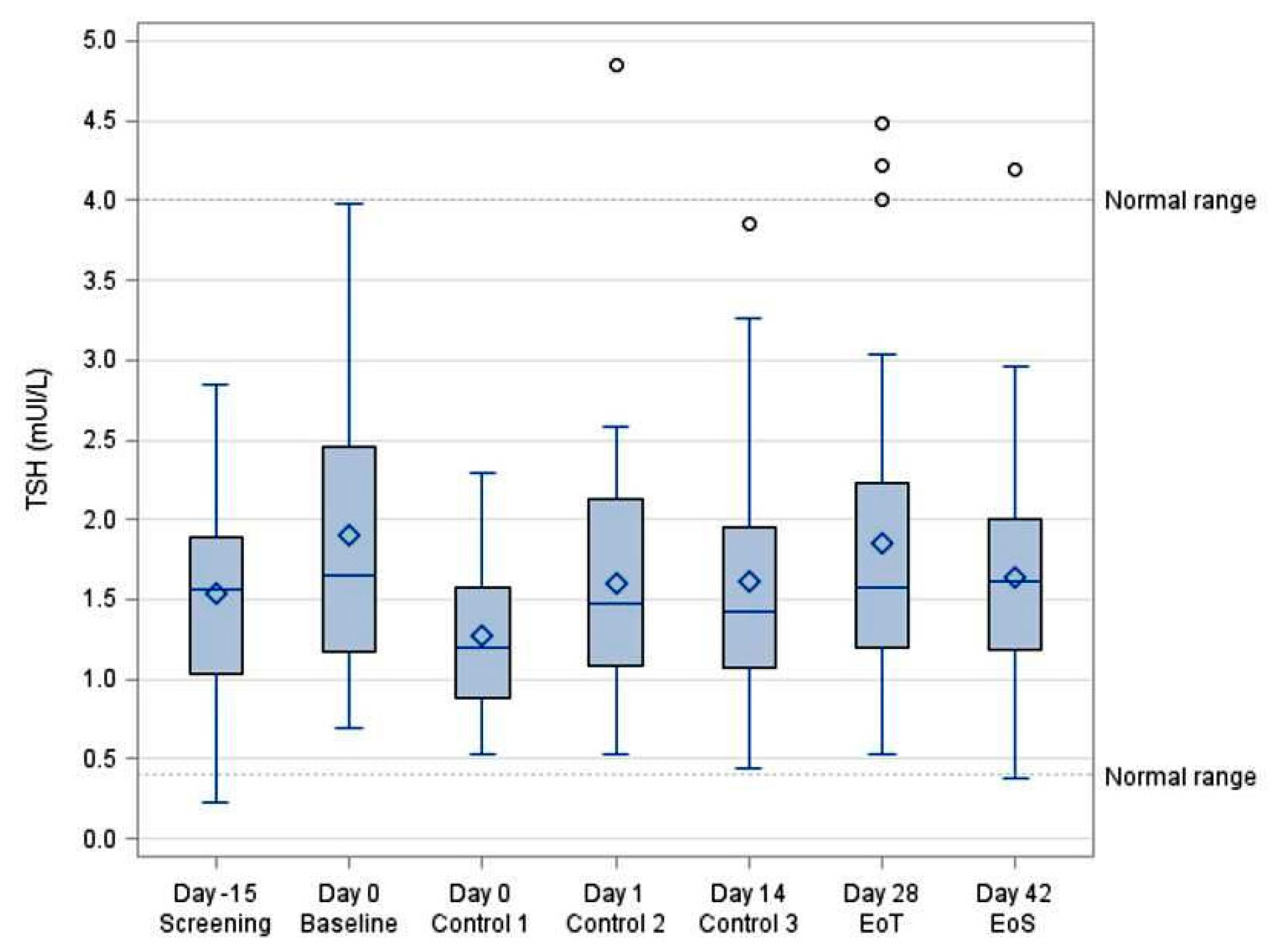
3.5. TSH Concentrations
TSH levels exhibited a transient decrease at 5 h post-application (from 1.90 ± 0.91 to 1.27 ± 0.48 mUI/L, p < 0.05), likely reflecting circadian variation. No significant differences were observed at subsequent time points (Table 6, Figure 5).
Table 6.
Plasma concentrations of TSH (mUI/L) measured in the full study population (N = 30).
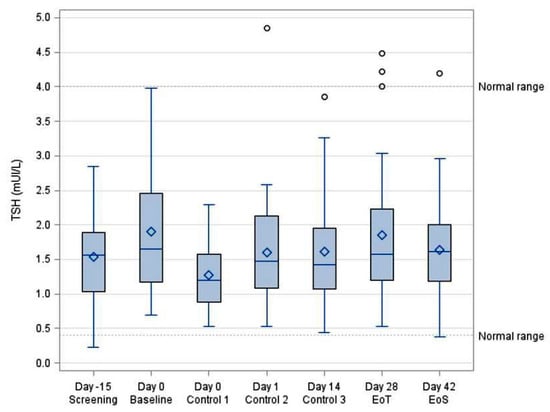
Figure 5.
Trend of TSH over time (Boxplot).
3.6. Extent of Exposure and Compliance
All 30 participants completed the 28-day treatment regimen. Overall compliance was 99.5%, with only four missed applications across 840 treatment days. Total exposure corresponded to 300 g of L-thyroxine gel (equivalent to 3 g L-T4 and 9 g escin).
3.7. Adverse Events
Eighteen AEs were reported during treatment and one during follow-up. No serious adverse events (SAEs) or deaths occurred. Most AEs were mild and unrelated to the investigational product. Events were distributed across various SOCs, with headache and skin reactions (erythema, pruritus) being the most frequently reported (Table 7).
Table 7.
Summary of all AEs by SOC and their IMP relationship (related/Not related). Adverse events were coded using the MedDRA version 22.0 (Medical Dictionary for Regulatory Activities), developed by the International Council for Harmonisation (ICH) and maintained by the MedDRA MSSO (Maintenance and Support Services Organization, McLean, VA, USA). SOC: System Organ Class; IMP: Investigational Medicinal Product.
3.8. Vital Signs and Safety Parameters
No clinically relevant changes were observed in systolic or diastolic blood pressure, heart rate, respiratory rate, or body temperature. Transient, non-significant reductions in SBP (−4.1 mmHg), DBP (−2.7 mmHg), and HR (−6.8 bpm) were noted at 5 h post-application. No abnormalities were found in ECG or clinical laboratory evaluations (Table 8).
Table 8.
Change from Baseline in vital signs measured in the full study population (N = 30). SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure; HR: Heart Rate.
4. Discussion
L-T4/escin topic formulation has been employed in the last fifty years for the treatment of localized adiposity associated with cellulite. It can be applied in both cosmetic [13] and therapeutic [14,15] treatments, with the potential for its adoption to expand due to its benefits for various dermatological conditions [2].
Over time, several studies have been conducted to assess the safety of the treatment and to rule out significant systemic absorption of the active ingredient (L-T4) that could affect the blood concentration of thyroid hormones. The primary endpoint of the study was the change in plasma FT4 levels. FT4 was selected over other thyroid-related hormones as it provides a direct, sensitive, and reliable marker of systemic exposure to exogenous L-thyroxine in healthy subjects. This choice is supported by both pharmacological rationale—given FT4’s immediacy and specificity compared to TSH and FT3—and regulatory guidance, as outlined in the EMA’s product-specific bioequivalence guideline for levothyroxine tablets (EMA/CHMP/176098/2020) [16]. Moreover, the use of FT4 as the primary endpoint is consistent with prior studies evaluating dermal absorption of L-T4 formulations [10,11]. In such studies, no significant changes in thyroid hormones were observed at any time point during treatment with L-T4/escin cream [11,17,18,19].
The development of a new gel formulation necessitated an investigation into its bioavailability and safety; therefore, this study was designed to evaluate plasma levels of FT4, FT3, rT3, and TSH in order to exclude any transcutaneous absorption of L-T4 and potential interference with systemic thyroid homeostasis.
The inclusion of women aged 18–50 years was guided by both regulatory [20] and physiological considerations. This age range ensured a homogeneous population with stable endocrine function and skin characteristics, minimizing confounding factors related to perimenopause. It also reflects the likely target demographic for topical L-T4/escin-based products, enhancing the external validity of bioavailability and safety findings. While age-related differences in dermal absorption cannot be excluded, broader age ranges may be explored in future studies.
No changes in fT3 were detected in any subject. Furthermore, plasma rT3 levels were also unaffected by the application of L-T4/escin gel at all time points, in contrast to a study by Santini et al., who reported an increase in rT3 levels at 6 and 12 h after cream application [10]. This discrepancy could be attributed to differences in the absorption profiles of the two tested formulations. Keratinocytes and fibroblasts both express deiodinase 3 (D3), which converts T4 and T3 into rT3 [4,21].
A possible explanation for the observed difference may be a decreased penetration of the gel into the deep layers of the dermis, resulting in a lower contribution of D3 to T3-to-rT3 conversion.
Another possible explanation for the lack of increase in rT3 could be the difference in the time points selected for thyroid hormone measurements. In the present study, blood samples were collected 5 h after administration, which occurred on average at 8:30 a.m., whereas in the study by Santini et al., hormone levels were measured at 6 and 12 h after administration, with dosing occurring at 8:00 a.m., and the greatest increase in rT3 observed at 12 h after administration [10].
This could suggest a progressive absorption of L-T4, meaning that the 5 h time point may not have been sufficient to detect a statistically significant change from Baseline, as the active ingredient had not yet been fully absorbed. Additionally, the different excipients in the new formulation could also have delayed absorption, making it impossible to detect changes in rT3 at 5 h post-dose.
Finally, it cannot be excluded that the excipients in the new gel formulation could interfere with the binding of L-T4 to D3.
In the present study, statistically significant decreases from Baseline in T3 and TSH were observed five hours after the first application of L-thyroxine gel. This finding can likely be attributed to the physiological circadian fluctuations in thyroid hormone levels, particularly TSH and T3 [22,23]. To minimize intra-individual variability and potential confounding, Baseline and 5 h blood samples were collected at standardized time points for all participants (approximately 08:30 and 13:45, respectively). Additionally, in-clinic procedures were standardized: participants remained seated at rest under continuous medical supervision, thereby limiting the impact of external factors such as physical activity or stress. These precautions strengthen the interpretation that the transient decline in FT3 and TSH reflects normal circadian variation rather than a pharmacodynamic effect of the investigational product. Notably, TSH and T3 levels typically peak between 2:00 and 4:00 a.m.—with the T3 peak lagging behind TSH by approximately 90 min—and reach their lowest values between 2:00 and 4:00 p.m. The sampling time, at five hours post-dose (around early afternoon), may, therefore, have coincided with this circadian nadir, contributing to the statistically significant differences observed compared to the Baseline. In contrast, T4 fluctuations, as reported by Russel et al. [24], are less influenced by TSH variations, which may explain why no significant differences in T4 levels from Baseline were detected. Although a slight decrease in FT4 was observed 5 h post-application, this variation remained well within the normal physiological range and is likely attributable to circadian fluctuation rather than systemic absorption. Moreover, the magnitude of change was below the typical inter-assay variability reported for FT4 measurements, reinforcing its lack of clinical significance. The absence of any consistent downward trend in subsequent time points further supports the conclusion that this minor variation does not reflect the systemic bioavailability of L-T4 under the study conditions.
Despite its strengths, this study has some limitations. The single-group, open-label design without a comparator arm limits the ability to fully exclude subtle systemic or local effects unrelated to the investigational product. Although objective hormonal endpoints and standardized tolerability assessments helped reduce bias, future studies should consider randomized controlled designs with vehicle-only or active comparators. The inclusion of only healthy women aged 18–50 with intact skin also narrows generalizability to broader populations, such as older adults, men, or individuals with dermatological conditions. Furthermore, reverse T3 (rT3) levels were batch-analyzed, consistent with early-phase practices, but this approach may introduce some variability compared to real-time assessments. The study was not intended to compare the topical formulation with oral L-T4 nor to evaluate pharmacodynamic outcomes in patients with thyreopathic conditions.
Further research is warranted to explore the safety and therapeutic potential of L-T4 gel in target populations, including bioavailability comparisons, studies on compromised skin, and trials assessing long-term efficacy and tolerability.
5. Conclusions
In conclusion, these results confirm the safety and lack of systemic effects of the new gel formulation in healthy women, with no significant changes in plasma levels of L-T4, T3, rT3, or TSH after total exposure to 300 g over 28 days. This evidence also supports the hypothesis that the skin acts as an effective barrier to the absorption of thyroxine. However, these conclusions are only valid when the skin barrier is intact and do not exclude the possibility of transcutaneous absorption in cases of barrier dysfunction. Further studies may be warranted to investigate the potential impact of skin alterations on the pharmacokinetics and systemic effects of L-thyroxine gel.
Author Contributions
Conceptualization and supervision: G.G., F.D.N. and E.F.; investigation: G.G., F.D.N., A.F. and C.C.; data curation: G.G. and F.D.N.; writing—original draft preparation: G.G.; writing—review and editing: G.G., F.D.N. and E.F.; project administration and review and editing: F.D.F. All authors have read and agreed to the published version of the manuscript.
Funding
This study was sponsored by Manetti & Roberts S.p.A. Società Italo Britannica. as a commercial clinical trial submitted to the Azienda Ospedaliero Universitaria Pisana. No additional funding was provided for independent research activities.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the North-West Tuscany Area Ethics Committee—Italy (approval recorded on the regional platform with code n. 1364 on 13 September 2018) and by the Italian Competent Authority (Letter with official protocol number AIFA/SC/p/100984 on 12 September 2018).
Informed Consent Statement
Informed consent was obtained from all individual participants included in the study both for trial participation and research publication purposes.
Data Availability Statement
The raw data generated during this study are the property of Manetti & Roberts S.p.A. Società Italo Britannica, as established in the agreement with the Azienda Ospedaliero-Universitaria Pisana (AOUP). Access to these data may be granted upon reasonable request and subject to sponsor approval. Requests should be addressed to the corresponding author, who will coordinate with the sponsor.
Acknowledgments
The authors would like to acknowledge Maria Rita Sessa and Caterina Pelosini for their valuable technical support in the laboratory analysis of blood samples.
Conflicts of Interest
This study was sponsored by Manetti & Roberts S.p.A. Società Italo Britannicaand conducted at the Azienda Ospedaliero-Universitaria Pisana, on behalf of which the authors were part of the clinical investigation team. The company had role in the design of the study, in the collection and analyses of data and no role in the interpretation of data, in the writing of the manuscript or in the decision to publish the results. For the writing of this manuscript, G.G. and F.D.N. declare having received a writing fee from Manetti & Roberts S.p.A. Società Italo Britannica. The remaining authors declare that they have no competing interests.
Abbreviations
The following abbreviations are used in this manuscript:
| AIC | Autorizzazione all’Immissione in Commercio |
| AIFA | Agenzia Italiana del Farmaco |
| ECG | Electrocardiogram |
| EoS | End of Study |
| EoT | End of Treatment |
| FT3 | Free Triiodothyronine |
| FT4 | Free Thyroxine |
| GCP | Good Clinical Practice |
| IMP | Investigational Medicinal Product |
| ITT | Intention-to-Treat |
| L-T3 | Levotriiodothyronine |
| L-T4 | Levothyroxine |
| PP | Per Protocol |
| rT3 | Reverse Triiodothyronine |
| TSH | Thyroid-Stimulating Hormone |
References
- Safer, J.D. Thyroid hormone action on skin. Dermato-Endocrinology 2011, 3, 211–215. [Google Scholar] [CrossRef]
- Paus, R.; Ramot, Y.; Kirsner, R.S.; Tomic-Canic, M. Topical L-thyroxine: The Cinderella among hormones waiting to dance on the floor of dermatological therapy? Exp. Dermatol. 2020, 29, 910–923. [Google Scholar] [CrossRef]
- Törmä, H.; Rollman, O.; Vahlquist, A. Detection of mRNA transcripts for retinoic acid, vitamin D3, and thyroid hormone (c-erb-A) nuclear receptors in human skin using reverse transcription and polymerase chain reaction. Acta Derm. Venereol. 1993, 73, 102–107. [Google Scholar] [CrossRef]
- Slominski, A.; Wortsman, J.; Kohn, L.; Ain, K.B.; Venkataraman, G.M.; Pisarchik, A.; Chung, J.H.; Giuliani, C.; Thornton, M.; Slugocki, G.; et al. Expression of hypothalamic-pituitary-thyroid axis related genes in the human skin. J. Investig. Dermatol. 2002, 119, 1449–1455. [Google Scholar] [CrossRef] [PubMed]
- Cianfarani, F.; Baldini, E.; Cavalli, A.; Marchioni, E.; Lembo, L.; Teson, M.; Persechino, S.; Zambruno, G.; Ulisse, S.; Odorisio, T.; et al. TSH receptor and thyroid-specific gene expression in human skin. J. Investig. Dermatol. 2010, 130, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.Y.; Langan, E.A.; Meier, N.T.; Funk, W.; Siemers, F.; Paus, R. Thyroxine (T4) may promote re-epithelialisation and angiogenesis in wounded human skin ex vivo. PLoS ONE 2019, 14, e0212659. [Google Scholar] [CrossRef] [PubMed]
- Post, H.; Hundt, J.E.; Zhang, G.; Depping, R.; Rose, C.; Langan, E.A.; Paus, R. Thyroxine restores severely impaired cutaneous re-epithelialisation and angiogenesis in a novel preclinical assay for studying human skin wound healing under “pathological” conditions ex vivo. Arch. Dermatol. Res. 2021, 313, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Shishido, M.; Kuroda, K.; Tsukifuji, R.; Fujita, M.; Shinkai, H. A case of pretibial myxedema associated with Graves’ disease: An immunohistochemical study of serum-derived hyaluronan-associated protein. J. Dermatol. 1995, 22, 948–952. [Google Scholar] [CrossRef] [PubMed]
- Kronick, P.L.; Sacks, M.S. Matrix macromolecules that affect the viscoelasticity of calfskin. J. Biomech. Eng. 1994, 116, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Santini, F.; Vitti, P.; Chiovato, L.; Ceccarini, G.; Macchia, M.; Montanelli, L.; Gatti, G.; Rosellini, V.; Mammoli, C.; Martino, E.; et al. Role for inner ring deiodination preventing transcutaneous passage of thyroxine. J. Clin. Endocrinol. Metab. 2003, 88, 2825–2830. [Google Scholar] [CrossRef] [PubMed]
- Certan, D.; Righini, V.; Oliva, M.; Fioravanti, P.; Bevilacqua, M. Bioavailability of L-thyroxine and its metabolites after topical treatment with an emulsion containing 0.1% micronised L-thyroxine. G. Ital. Dermatol. Venereol. 2013, 148, 287–292. [Google Scholar] [PubMed]
- U.S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. National Cancer Institute, NIH. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm (accessed on 27 November 2017).
- Comi, R.; Bertolotti, M. La Somatoline nel trattamento degli inestetismi da accumulo adiposo sottocutaneo. Il Policlin. Sez. Medica 1994, 101, 1–21. [Google Scholar]
- Lisi, P. Sperimentazione clinica di una crema contenente levo-tiroxina ed escina. G. Ital. Dermatol. Venereol. 1973, 108, 1–7. [Google Scholar]
- Dini, D.; Bianchini, M.; Massa, T.; Fassio, T. Trattamento del linfedema dell’arto superiore conseguente a mastectomia con escina e levo-tiroxina. Minerva Med. 1981, 72, 2319–2322. [Google Scholar] [PubMed]
- European Medicines Agency (EMA). Guideline on the Bioequivalence of Levothyroxine Oral Products. EMA/CHMP/176098/2020, Committee for Medicinal Products for Human Use (CHMP). Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/levothyroxine-tablets-125-mcg-25-mcg-50-mcg-75-mcg-100-mcg-and-200-mcg-and-additional-strengths-within-range-product-specific-bioequivalence-guidance_en.pdf (accessed on 10 December 2020).
- Norbiato, G.; Endocrinology Service, “L. Sacco” Hospital, Milan, Italy. Valutazione dell’eventuale biodisponibilità sistemica di l-T4 esogena dopo ripetuta applicazione topica di Somatoline bustine nel volontario sano—Confronto cross-over tra due formulazioni di emulsione, Final Report, Study SOMA 001.98. 1998; Unpublished internal document.
- Buraglio, M.; LCG Bioscience Clinical Pharmacology Unit, Bourn Hall Clinic, Bourn, Cambridge, UK. Somatoline Cream Repeat Topical Application in Women. Evaluation of Absorption, Study Report, Protocol No. LCGCPU 0197 E. 1997; Unpublished internal document.
- Righini, V.; Renzetti, D.; Bevilacqua, M. Studio sulla biodisponibilità sistemica di L-tiroxina4 dopo ripetuta applicazione cutanea di un farmaco topico in commercio. G. Ital. Dermatol. Venereol. 2003, 138, 333–340. [Google Scholar]
- European Medicines Agency (EMA). Guideline on the Investigation of Bioequivalence. EMA/CPMP/EWP/QWP/1401/98 Rev. 1. Committee for Medicinal Products for Human Use (CHMP); London, 20 January 2010, Effective from 1 August 2010. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-investigation-bioequivalence-rev1_en.pdf (accessed on 16 June 2025).
- Köhrle, J.; Frädrich, C. Deiodinases control local cellular and systemic thyroid hormone availability. Free Radic. Biol. Med. 2022, 193 Pt 1, 59–79. [Google Scholar] [CrossRef] [PubMed]
- Haus, E. Chronobiology in the endocrine system. Adv. Drug Deliv. Rev. 2007, 59, 985–1014. [Google Scholar] [CrossRef] [PubMed]
- Philippe, J.; Dibner, C. Thyroid circadian timing: Roles in physiology and thyroid malignancies. J. Biol. Rhythms 2015, 30, 76–83. [Google Scholar] [CrossRef]
- Russell, W.; Harrison, R.F.; Smith, N.; Darzy, K.; Shalet, S.; Weetman, A.P.; Ross, R.J. Free triiodothyronine has a distinct circadian rhythm that is delayed but parallels thyrotropin levels. J. Clin. Endocrinol. Metab. 2008, 93, 2300–2306. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).