
Mirogabalin for Neuropathic Pain: A Review of Non-Opioid Pharmacotherapy with Insights from Japan


Abstract
1. Introduction
2. Methods
3. The Clinical Significance of Neuropathic Pain as a Healthcare Burden
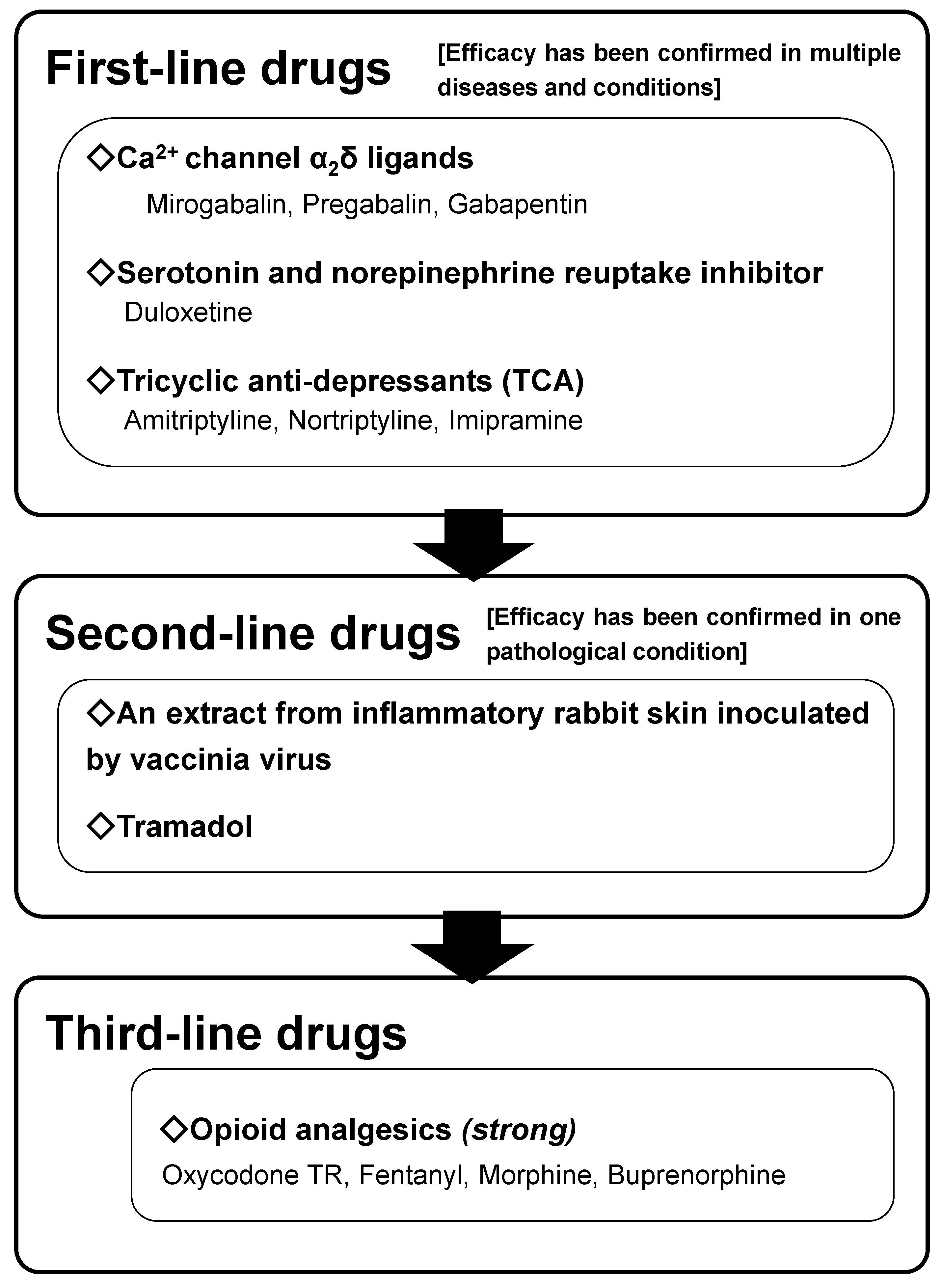
4. Pharmacotherapy for Neuropathic Pain in Japan
5. Mirogabalin: A Novel Calcium Channel α2δ Ligand
6. Expert Opinion
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Bauer, C.S.; Rahman, W.; Tran-Van-Minh, A.; Lujan, R.; Dickerson, A.H.; Dolphin, A.C. The anti-allodynic alpha-2-delta ligand, pregabalin inhibits the trafficking of the calcium channel alpha-2-delta subunit to presynaptic terminals in vivo. Biochem. Soc. Trans. 2010, 38, 525–528. [Google Scholar] [CrossRef] [PubMed]
- Bouhassira, D.; Lantéri-Minet, M.; Attal, N.; Laurent, B.; Touboul, C. Prevalence of chronic pain with neuropathic characteristics in the general population. Pain 2008, 136, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T.S. Pathophysiology of pain: From theory to clinical evidence. Eur. J. Pain 2008, 2, S13–S17. [Google Scholar] [CrossRef]
- Meisinger, C.; Bongaerts, B.W.C.; Heier, M.; Amann, U.; Kowall, B.; Herder, C.; Ruckert-Eheberg, I.M.; Rathmann, W.; Ziegler, D. Neuropathic pain is not adequately treated in the older general population: Results from the KORA F4 survey. Pharmacoepidemiol. Drug Saf. 2018, 27, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.; Sayer, A.A. Sarcopenia and frailty: New challenges for clinical practice. Clin. Med. 2015, 15 (Suppl. S6), s88–s891. [Google Scholar] [CrossRef]
- Nakamura, K.; Ogata, T. Locomotive syndrome: Definition and management. Clin. Rev. Bone Miner. Metab. 2016, 14, 56–67. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpaa, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef]
- Sumitani, M.; Sakai, T.; Matsuda, Y.; Abe, H.; Yamaguchi, S.; Hosokawa, T.; Fukui, S. Executive summary of the Clinical Guidelines of Pharmacotherapy for Neuropathic Pain: Second edition by the Japanese Society of Pain Clinicians. J. Anesth. 2018, 32, 463–478. [Google Scholar] [CrossRef]
- Martinez, V.; Attal, N.; Vanzo, B.; Vicaut, E.; Gautier, J.M.; Bouhassira, D.; Lanteri-Minet, M. Adherence of French GPs to chronic neuropathic pain clinical guidelines: Results of a cross-sectional, randomized, “e” case-vignette survey. PLoS ONE 2014, 9, e93855. [Google Scholar] [CrossRef]
- Imagama, S.; Hasegawa, Y.; Ando, K.; Kobayashi, K.; Hida, T.; Ito, K.; Tsushima, M.; Nishida, Y.; Ishiguro, N. Staged decrease of physical ability on the locomotive syndrome risk test is related to neuropathic pain, nociceptive pain, shoulder complaints, and quality of life in middle-aged and elderly people—The utility of the locomotive syndrome risk test. Mod. Rheumatol. 2017, 27, 1051–1056. [Google Scholar] [CrossRef]
- Hamacher, D.; Liebl, D.; Hödl, C.; HeBler, V.; Kniewasser, C.K.; Thonnessen, T.; Zech, A. Gait stability and its influencing factors in older adults. Front. Physiol. 2018, 9, 1955. [Google Scholar] [CrossRef]
- Toth, C.; Brady, S.; Hatfield, M. The importance of catastrophizing for successful pharmacological treatment of peripheral neuropathic pain. J. Pain Res. 2014, 7, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.P.; Mao, J. Neuropathic pain: Mechanisms and their clinical implications. BMJ 2014, 348, f7656. [Google Scholar] [CrossRef]
- Bras, M.; Dordevic, V.; Gregurek, R.; Blajic, M. Neurobiological and clinical relationship between psychiatric disorders and chronic pain. Psychiatr. Danub. 2010, 22, 221–226. [Google Scholar] [PubMed]
- Andersen, M.L.; Araujo, P.; Frange, C.; Tufik, S. Sleep disturbance and pain—A tale of two common problems. Chest 2018, 154, 1249–1259. [Google Scholar] [CrossRef] [PubMed]
- Ushio, M.; Sumitani, M.; Abe, H.; Mietani, K.; Hozumi, J.; Inoue, R.; Tsuchida, R.; Ushida, T.; Yamada, Y. Characteristics of locomotive syndrome in Japanese patients with chronic pain and results of a path analysis confirming the relevance of a vicious cycle involving locomotive syndrome, musculoskeletal pain and its psychological factors. JMA J. 2019, 2, 184–189. [Google Scholar] [CrossRef]
- Meyer-Rosberg, K.; Kvarnström, A.; Kinnman, E.; Gordh, T.; Nordfors, L.O.; Kristofferson, A. Peripheral neuropathic pain—A multidimensional burden for patients. Eur. J. Pain 2001, 5, 379–389. [Google Scholar] [CrossRef]
- Azuma, K.; Abe, H.; Hozumi, J.; Inoue, R.; Konishi, M.; Tsuchida, R.; Ando, M.; Saita, K.; Sumitani, M. Prefectural adequacy of opioid availability for cancer pain and its determinants in Japan: A preliminary study. JMA J. 2020, 3, 340–346. [Google Scholar]
- Hasegawa-Moriyama, M.; Morioka, Y.; Hiroi, S.; Naya, N.; Suzuki, Y.; Koretaka, Y.; Hara, E.; Abe, H.; Uchida, K.; Sumitani, M. High prevalence of severe pain is associated with low opioid availability in patients with advanced cancer: Combinated database study and nationwide questionnaire survey in Japan. Neuropsychopharmacol. Rep. 2024, 44, 502–511. [Google Scholar] [CrossRef]
- Marchetti Calônego, M.A.; Sikandar, S.; Ferris, F.D.; de Barros, G.A.M. Spread the Word: There are two opioid crises! Drugs 2020, 80, 1147–1154. [Google Scholar] [CrossRef]
- World Health Organization. WHO Health Organization Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents; World Health Organization: Geneve, Switzerland, 2018. [Google Scholar]
- Kozai, D.; Numoto, N.; Nishikawa, K.; Kamegawa, A.; Kawasaki, S.; Hiroaki, Y.; Irie, K.; Oshima, A.; Hanzawa, H.; Shimada, K.; et al. Recognition mechanism of a novel gabapentinoid drug, mirogabalin, for recombinant human α2δ1, a voltage-gated calcium channels subunit. J. Mol. Biol. 2023, 435, 168049. [Google Scholar] [CrossRef]
- Yang, F.; Wang, Y.; Zhang, M.; Yu, S. Mirogabalin as a novel calcium channel alpha-2-delta ligand for the treatment of neuropathic pain: A review of clinical update. Front. Pharmacol. 2024, 15, 1491570. [Google Scholar] [CrossRef]
- Baba, M.; Matsui, N.; Kuroha, M.; Wasaki, Y.; Ohwada, S. Mirogabalin for the treatment of diabetic peripheral neuropathic pain: A randomized, double-blind, placebo-controlled phase III study in Asia patients. J. Diabet. Investig. 2019, 10, 1299–1306. [Google Scholar] [CrossRef]
- Kato, J.; Matsui, N.; Kakehi, Y.; Murayama, E.; Ohwada, S.; Sugihara, M. Mirogabalin for the management of postherpetic neuralgia: A randomized, double-blind, placebo-controlled phase 3 study in Asian patients. Pain 2019, 160, 1175–1185. [Google Scholar] [CrossRef]
- Ushida, T.; Katayama, Y.; Hiasa, Y.; Nishihara, M.; Tajima, F.; Katoh, S.; Tanaka, H.; Maeda, T.; Furusawa, K.; Richardson, M.; et al. Mirogabalin for central neuropathic pain after spinal cord injury: A randomized, double-blind, placebo-controlled, phase 3 study in Asia. Neurology 2023, 100, e1193–e1206. [Google Scholar] [CrossRef] [PubMed]
- Ushida, T.; Yokoyama, M.; Shiosakai, K.; Saito, K.; Ibe, S.; Okuizumi, K. A large-scale database study for the prescription status of a new voltage-gated calcium channel α2δ ligand, mirogabalin, in Japan. Exp. Opin. Pharmacother. 2022, 23, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Farrar, J.T.; Young JPJr LaMoreaux, L.; Werth, J.L.; Poole, M.R. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Sadegh, A.A.; Gehr, N.L.; Finnerup, N.B. A systematic review and meta-analysis of randomized controlled head-to-head trials of recommended drugs for neuropathic pain. Pain Rep. 2024, 982, e1138. [Google Scholar] [CrossRef]
- Kato, J.; Matsui, N.; Kakehi, Y.; Murayama, E.; Ohwada, S. Long-term safety and efficacy of mirogabalin in Asian patients with postherpetic neuralgia. Medicine 2020, 99, e21976. [Google Scholar] [CrossRef]
- Kimura, Y.; Yamaguchi, S.; Suzuki, T.; Kato, J.; Chiba, S.; Hirakawa, N.; Yamaguchi, K.; Tanabe, Y.; Takatsuna, H.; Kenyoshi, Y.; et al. Switching from pregabalin to mirogabalin in patients with peripheral neuropathic pain: A multi-center, prospective, single-arm, open-label study (MIROP study). Pain Ther. 2021, 10, 711–727. [Google Scholar] [CrossRef]
- Li, C.Y.; Zhang, X.L.; Matthews, E.A.; Li, K.W.; Kurwa, A. Calcium channel α2δ1 subunit mediates spinal hyperexcitability in pain modulation. Pain 2006, 125, 20–34. [Google Scholar] [CrossRef] [PubMed]
- Barclay, J.; Balaguero, N.; Minone, M.; Ackerman, S.L.; Brodbeck, V.A.L.J.; Canti, C.; Meir, A.; Page, K.M.; Kusumi, K.; Perez-Reyes, E.; et al. Ducky mouse phenotype of epilepsy and ataxia is associated with mutations in the Cacna2d2 gene and decreased calcium channel current in cerebellar Purkinje cells. J. Neurosci. 2001, 21, 6095–6104. [Google Scholar] [CrossRef]
- Domon, Y.; Arakawa, N.; Inoue, T.; Matsuda, F.; Takahashi, M.; Yamamura, N.; Kai, K.; Kitano, Y. Binding characteristics and analgesic effects of mirogabalin, a novel ligand for the α2δ subunit of voltage-gated calcium channels. J. Pharmacol. Exp. Ther. 2018, 365, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Kodama, S.; Shiosakai, K.; Kimura, T. Relationship between the dose titration and adherence of mirogabalin in patients with peripheral neuropathic pain depending on renal function: A nationwide electronic medical record database study. Exp. Opin. Pharmacother. 2023, 24, 267–282. [Google Scholar] [CrossRef]
- Mathieson, S.; Maher, C.G.; McLachlan, A.J.; Latimer, J.; Koes, B.W.; Hancock, M.J.; Harris, I.; Day, R.O.; Billot, L.; Pik, J.; et al. Trial of pregabalin for acute and chronic sciatica. N. Engl. J. Med. 2017, 376, 1111–1120. [Google Scholar] [CrossRef] [PubMed]
- Nikaido, T.; Takatsuna, H.; Tabata, S.; Shiosakai, K.; Nakatani, T.; Konno, S. Efficacy and safety of add-on mirogabalin to NSAIDs in lumbar spinal canal stenosis with peripheral neuropathic pain: A randomized, open-label study. Pain Ther. 2022, 11, 1195–1214. [Google Scholar] [CrossRef]
- Attal, N.; Fermanian, C.; Fermanian, J.; Lanteri-Minet, M.; Alchaar, H.; Bouhassira, D. Neuropathic pain: Are there distinct subtypes depending on the aetiology or anatomical lesion? Pain 2008, 138, 343–353. [Google Scholar] [CrossRef]
- Sumitani, M.; Miyauchi, S.; McCabe, C.S.; Shibata, M.; Maeda, L.; Saitoh, Y.; Tashiro, T.; Mashimo, T. Mirror visual feedback alleviates deafferentation pain, depending on qualitative aspects of the pain: A preliminary report. Rheumatology 2008, 47, 1038–1043. [Google Scholar] [CrossRef]
- World Health Organization. International Perspectives on Spinal Cord Injury; World Health Organization: Geneve, Switzerland, 2013. [Google Scholar]
- OSCIS investigators; Chikuda, H.; Koyama, Y.; Matsubayashi, Y.; Ogata, T.; Ohtsu, H.; Sugita, S.; Sumitani, M.; Kadono, Y.; Miura, T.; et al. Effect of early vs. delayed surgical treatment on motor recovery in incomplete cervical spinal cord injury with preexisting cervical stenosis: A randomized clinical trial. JAMA Netw. Open 2021, 4, e2133604. [Google Scholar] [CrossRef]
- Misawa, S.; Denda, T.; Kodama, S.; Suzuki, T.; Naito, Y.; Kogawa, T.; Takada, M.; Suichi, T.; Shiosakai, K.; Kuwabara, S.; et al. Efficacy and safety of mirogabalin for chemotherapy-induced peripheral neuropathy: A prospective single-arm trial (MiroCIP study). BMC Cancer 2023, 23, 1098. [Google Scholar] [CrossRef]
- Sumitani, M.; Nishizawa, D.; Hozumi, J.; Ikeda, K. Genetic implications in quality palliative care and preventing opioid crisis in cancer-related pain management. J. Neurosci. Res. 2022, 100, 362–372. [Google Scholar] [CrossRef] [PubMed]
- Sumitani, M. Time to act for reappraising the educational system for universal access to opioid analgesics, for quality palliative care and cancer-related pain relief in East Asian countries. Lancet Reg. Health West. Pac. 2021, 16, 100270. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Subjects | Goals | Pharmacotherapy Strategy | ||
|---|---|---|---|---|
| Rapid Response Program | Patients with advanced cancer and/or terminally-ill condition | Adequate pain relief as the central goal and improving and maintaining QOL to the greatest extent | Necessary and sufficient doses of opioids should be recommended without any dose-limits. Adding opioids promptly on an as-needed basis without any time limits. To balance the analgesic and adverse effects of opioids, the administration of multimodal analgesia with adjuvant analgesics and opioids is recommended. | |
| Bridge-to-Recovery Program | Patients receiving anti-cancer treatment | In case of cancer treatment-related pain, interfering with continuation of the anti-cancer treatment(s) | Moderate control of pain to reduce it to an endurable level and ensure the continuation of anti-cancer treatment(s) and the maintenance of QOL as high as possible | Necessary and sufficient doses of opioids are prioritized (high-dose opioids are acceptable if required). Augmenting daily dosage of opioids promptly on an as-needed basis. To balance the analgesic and adverse effects of opioids, administering multimodal analgesia in combination with adjuvant analgesics is recommended. |
| Temporal Maintenance Program | Mild-to-moderate pain that does not interfere with the continuation of anti-cancer treatment(s) (endurable intensity of cancer treatment-related pain) | Maintaining QOL as high as possible and maintaining cancer treatment-related pain without interfering with anti-cancer treatment(s) | Multimodal analgesia achieved primarily with non-opioid analgesics is recommended. Concurrent opioids within moderate doses can be administered if required. Adding opioids promptly on an as-needed basis is acceptable a few times per day. | |
| Destination Program | Cancer survivors | Maintaining QOL as high as possible while balancing the favorable and adverse effects of long-term analgesics | Prioritizing non-opioid analgesics alone. Multimodal analgesia with bare-minimum doses of opioids might be acceptable if required. Strict prohibition of adding opioids on an as-needed basis. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sumitani, M.; Kogure, T.; Abe, H.; Tsuchida, R.; Inoue, R.; Sumitani, M. Mirogabalin for Neuropathic Pain: A Review of Non-Opioid Pharmacotherapy with Insights from Japan. Future Pharmacol. 2025, 5, 31. https://doi.org/10.3390/futurepharmacol5030031
Sumitani M, Kogure T, Abe H, Tsuchida R, Inoue R, Sumitani M. Mirogabalin for Neuropathic Pain: A Review of Non-Opioid Pharmacotherapy with Insights from Japan. Future Pharmacology. 2025; 5(3):31. https://doi.org/10.3390/futurepharmacol5030031
Chicago/Turabian StyleSumitani, Mizuho, Takamichi Kogure, Hiroaki Abe, Rikuhei Tsuchida, Reo Inoue, and Masahiko Sumitani. 2025. "Mirogabalin for Neuropathic Pain: A Review of Non-Opioid Pharmacotherapy with Insights from Japan" Future Pharmacology 5, no. 3: 31. https://doi.org/10.3390/futurepharmacol5030031
APA StyleSumitani, M., Kogure, T., Abe, H., Tsuchida, R., Inoue, R., & Sumitani, M. (2025). Mirogabalin for Neuropathic Pain: A Review of Non-Opioid Pharmacotherapy with Insights from Japan. Future Pharmacology, 5(3), 31. https://doi.org/10.3390/futurepharmacol5030031