
The Landscape of IgA Nephropathy Treatment Strategy: A Pharmacological Overview

 and
and
Abstract
1. Introduction
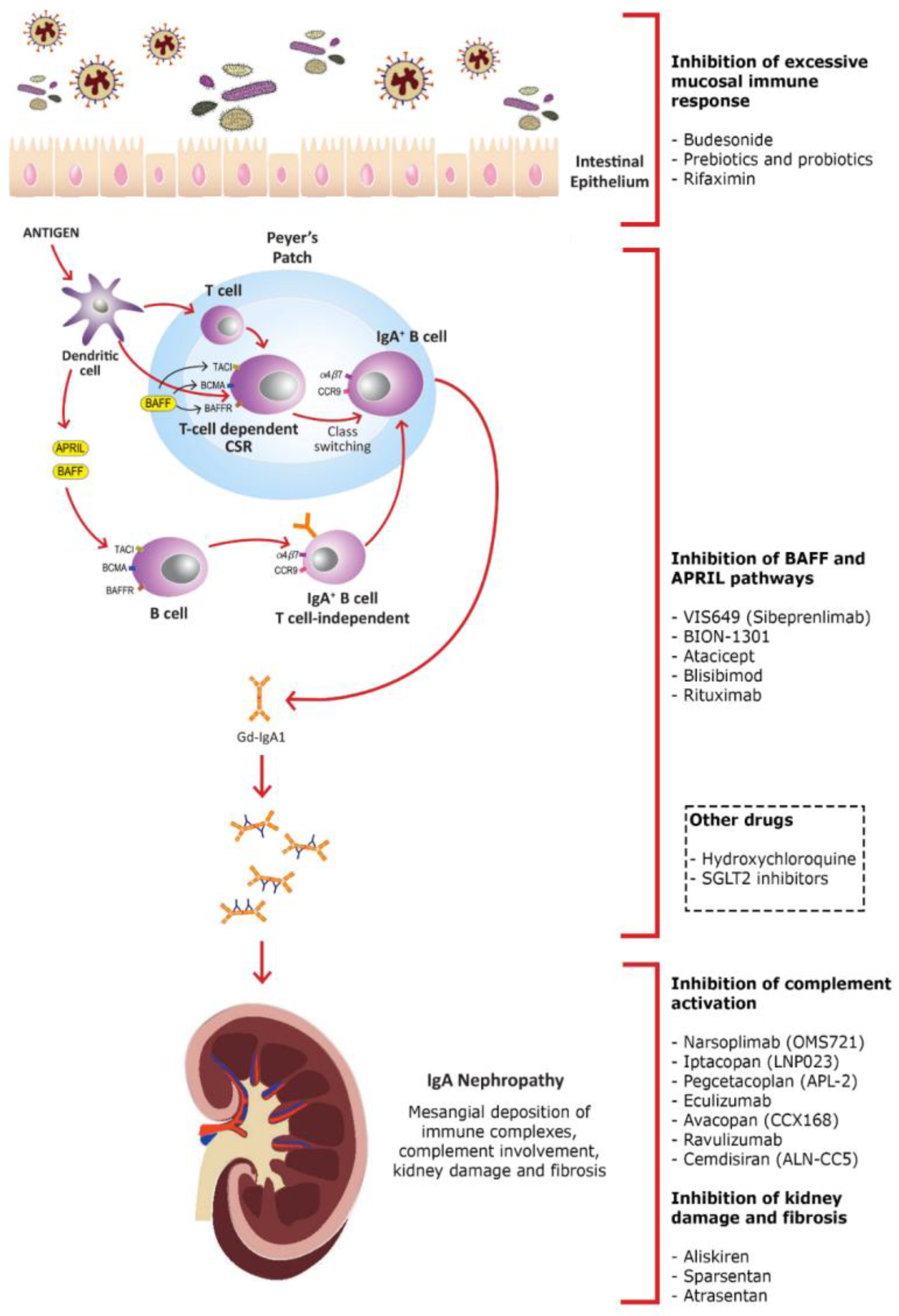
2. Inhibition of Excessive Mucosal Immune Response
2.1. Budesonide
2.2. Prebiotics and Probiotics
2.3. Rifaximin
3. Inhibition of B Cell-Activating Factor (BAFF) and a Proliferation-Inducing Ligand (APRIL) Pathways
3.1. VIS649 (Sibeprenlimab)
3.2. BION-1301
3.3. Atacicept
3.4. Blisibimod
3.5. Rituximab
4. Inhibition of Complement Activation
4.1. Narsoplimab (OMS721)
4.2. Iptacopan (LNP023)
4.3. Pegcetacoplan (APL-2)
4.4. Eculizumab
4.5. Avacopan (CCX168)
4.6. Ravulizumab
4.7. Cemdisiran (ALN-CC5)
5. Inhibition of Kidney Damage and Fibrosis
5.1. Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Antagonists
5.2. Aliskiren
5.3. Sparsentan
5.4. Atrasentan
6. Other Drugs
6.1. Hydroxychloroquine (HCQ)
6.2. Sodium-Glucose Cotransporter 2 Inhibitors (SGLT2i)
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sallustio, F.; Curci, C.; Di Leo, V.; Gallone, A.; Pesce, F.; Gesualdo, L. A New Vision of IgA Nephropathy: The Missing Link. Int. J. Mol. Sci. 2019, 21, 189. [Google Scholar] [CrossRef]
- Fabio, S.; Curci, C.; Cimmarusti, M.T.; Picerno, A.; De Palma, G.; Sivo, C.; Annese, F.; Fontò, G.; Stasi, A.; Pesce, F.; et al. Elevated levels of IL-6 in IgA nephropathy patients are induced by an epigenetically driven mechanism triggered by viral and bacterial RNA. medRxiv 2022. [Google Scholar] [CrossRef]
- Cheung, C.K.; Rajasekaran, A.; Barratt, J.; Rizk, D.V. An Update on the Current State of Management and Clinical Trials for IgA Nephropathy. J. Clin. Med. 2021, 10, 2493. [Google Scholar] [CrossRef]
- He, J.W.; Zhou, X.J.; Lv, J.C.; Zhang, H. Perspectives on how mucosal immune responses, infections and gut microbiome shape IgA nephropathy and future therapies. Theranostics 2020, 10, 11462–11478. [Google Scholar] [CrossRef]
- Wu, L.; Liu, D.; Xia, M.; Chen, G.; Liu, Y.; Zhu, X.; Liu, H. Immunofluorescence deposits in the mesangial area and glomerular capillary loops did not affect the prognosis of immunoglobulin a nephropathy except C1q:a single-center retrospective study. BMC Nephrol. 2021, 22, 43. [Google Scholar] [CrossRef]
- Knoppova, B.; Reily, C.; King, R.G.; Julian, B.A.; Novak, J.; Green, T.J. Pathogenesis of IgA Nephropathy: Current Understanding and Implications for Development of Disease-Specific Treatment. J. Clin. Med. 2021, 10, 4501. [Google Scholar] [CrossRef]
- Eitner, F.; Floege, J. In search of a better understanding of IgA nephropathy-associated hematuria. Kidney Int. 2012, 82, 513–515. [Google Scholar] [CrossRef]
- Perse, M.; Veceric-Haler, Z. The Role of IgA in the Pathogenesis of IgA Nephropathy. Int. J. Mol. Sci. 2019, 20, 6199. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int. 2021, 100, S1–S276. [Google Scholar] [CrossRef]
- Maixnerova, D.; Tesar, V. Emerging Modes of Treatment of IgA Nephropathy. Int. J. Mol. Sci. 2020, 21, 9064. [Google Scholar] [CrossRef]
- Suzuki, H. Biomarkers for IgA nephropathy on the basis of multi-hit pathogenesis. Clin. Exp. Nephrol. 2019, 23, 26–31. [Google Scholar] [CrossRef]
- Samy, E.; Wax, S.; Huard, B.; Hess, H.; Schneider, P. Targeting BAFF and APRIL in systemic lupus erythematosus and other antibody-associated diseases. Int. Rev. Immunol. 2017, 36, 3–19. [Google Scholar] [CrossRef]
- Gesualdo, L.; Di Leo, V.; Coppo, R. The mucosal immune system and IgA nephropathy. Semin. Immunopathol. 2021, 43, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.; Li, X.K. The Role of Immune Modulation in Pathogenesis of IgA Nephropathy. Front. Med. 2020, 7, 92. [Google Scholar] [CrossRef] [PubMed]
- Davin, J.C.; Forget, P.; Mahieu, P.R. Increased intestinal permeability to (51 Cr) EDTA is correlated with IgA immune complex-plasma levels in children with IgA-associated nephropathies. Acta Paediatr. Scand. 1988, 77, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Coppo, R. The intestine-renal connection in IgA nephropathy. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2015, 30, 360–366. [Google Scholar] [CrossRef]
- Sallustio, F.; Picerno, A.; Montenegro, F.; Cimmarusti, M.T.; Di Leo, V.; Gesualdo, L. The Human Virome and Its Crosslink with Glomerulonephritis and IgA Nephropathy. Int. J. Mol. Sci. 2023, 24, 3897. [Google Scholar] [CrossRef] [PubMed]
- Rauen, T.; Fitzner, C.; Eitner, F.; Sommerer, C.; Zeier, M.; Otte, B.; Panzer, U.; Peters, H.; Benck, U.; Mertens, P.R.; et al. Effects of Two Immunosuppressive Treatment Protocols for IgA Nephropathy. J. Am. Soc. Nephrol. JASN 2018, 29, 317–325. [Google Scholar] [CrossRef]
- Schimpf, J.I.; Klein, T.; Fitzner, C.; Eitner, F.; Porubsky, S.; Hilgers, R.D.; Floege, J.; Groene, H.J.; Rauen, T. Renal outcomes of STOP-IgAN trial patients in relation to baseline histology (MEST-C scores). BMC Nephrol. 2018, 19, 328. [Google Scholar] [CrossRef]
- Lv, J.; Zhang, H.; Wong, M.G.; Jardine, M.J.; Hladunewich, M.; Jha, V.; Monaghan, H.; Zhao, M.; Barbour, S.; Reich, H.; et al. Effect of Oral Methylprednisolone on Clinical Outcomes in Patients with IgA Nephropathy: The TESTING Randomized Clinical Trial. Jama 2017, 318, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Fellstrom, B.C.; Barratt, J.; Cook, H.; Coppo, R.; Feehally, J.; de Fijter, J.W.; Floege, J.; Hetzel, G.; Jardine, A.G.; Locatelli, F.; et al. Targeted-release budesonide versus placebo in patients with IgA nephropathy (NEFIGAN): A double-blind, randomised, placebo-controlled phase 2b trial. Lancet 2017, 389, 2117–2127. [Google Scholar] [CrossRef]
- Smerud, H.K.; Barany, P.; Lindstrom, K.; Fernstrom, A.; Sandell, A.; Pahlsson, P.; Fellstrom, B. New treatment for IgA nephropathy: Enteric budesonide targeted to the ileocecal region ameliorates proteinuria. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2011, 26, 3237–3242. [Google Scholar] [CrossRef] [PubMed]
- Barratt, J.; Lafayette, R.; Kristensen, J.; Stone, A.; Cattran, D.; Floege, J.; Tesar, V.; Trimarchi, H.; Zhang, H.; Eren, N.; et al. Results from part A of the multi-center, double-blind, randomized, placebo-controlled NefIgArd trial, which evaluated targeted-release formulation of budesonide for the treatment of primary immunoglobulin A nephropathy. Kidney Int. 2023, 103, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Floege, J.; Feehally, J. The mucosa-kidney axis in IgA nephropathy. Nat. Rev. Nephrol. 2016, 12, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Caggiano, G.; Cosola, C.; Di Leo, V.; Gesualdo, M.; Gesualdo, L. Microbiome modulation to correct uremic toxins and to preserve kidney functions. Curr. Opin. Nephrol. Hypertens. 2020, 29, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Bunker, J.J.; Bendelac, A. IgA Responses to Microbiota. Immunity 2018, 49, 211–224. [Google Scholar] [CrossRef] [PubMed]
- Shreiner, A.B.; Kao, J.Y.; Young, V.B. The gut microbiome in health and in disease. Curr. Opin. Gastroenterol. 2015, 31, 69–75. [Google Scholar] [CrossRef]
- Martin, R.; Langella, P. Emerging Health Concepts in the Probiotics Field: Streamlining the Definitions. Front. Microbiol. 2019, 10, 1047. [Google Scholar] [CrossRef]
- Morrison, D.J.; Preston, T. Formation of short chain fatty acids by the gut microbiota and their impact on human metabolism. Gut Microbes 2016, 7, 189–200. [Google Scholar] [CrossRef]
- Monteiro, R.C.; Rafeh, D.; Gleeson, P.J. Is There a Role for Gut Microbiome Dysbiosis in IgA Nephropathy? Microorganisms 2022, 10, 683. [Google Scholar] [CrossRef]
- Soylu, A.; Berktas, S.; Sarioglu, S.; Erbil, G.; Yilmaz, O.; Demir, B.K.; Tufan, Y.; Yesilirmak, D.; Turkmen, M.; Kavukcu, S. Saccharomyces boulardii prevents oral-poliovirus vaccine-induced IgA nephropathy in mice. Pediatr. Nephrol. 2008, 23, 1287–1291. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Dong, L.; Jiang, Z.; Tan, L.; Luo, X.; Pei, G.; Qin, A.; Zhong, Z.; Liu, X.; Tang, Y.; et al. Probiotics ameliorate IgA nephropathy by improving gut dysbiosis and blunting NLRP3 signaling. J. Transl. Med. 2022, 20, 382. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Jin, Y.; Zhou, W.; Xiao, T.; Wu, Z.; Su, J.; Gao, H.; Shen, P.; Zheng, B.; Luo, Q.; et al. Rifaximin Modulates the Gut Microbiota to Prevent Hepatic Encephalopathy in Liver Cirrhosis without Impacting the Resistome. Front. Cell. Infect. Microbiol. 2021, 11, 761192. [Google Scholar] [CrossRef]
- Jin, Y.; Ren, X.; Li, G.; Li, Y.; Zhang, L.; Wang, H.; Qian, W.; Hou, X. Beneficial effects of Rifaximin in post-infectious irritable bowel syndrome mouse model beyond gut microbiota. J. Gastroenterol. Hepatol. 2018, 33, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Pagliari, D.; Gambassi, G.; Piccirillo, C.A.; Cianci, R. The Intricate Link among Gut “Immunological Niche”, Microbiota, and Xenobiotics in Intestinal Pathology. Mediat. Inflamm 2017, 2017, 8390595. [Google Scholar] [CrossRef]
- Yang, L.; Liu, B.; Zheng, J.; Huang, J.; Zhao, Q.; Liu, J.; Su, Z.; Wang, M.; Cui, Z.; Wang, T.; et al. Rifaximin Alters Intestinal Microbiota and Prevents Progression of Ankylosing Spondylitis in Mice. Front. Cell Infect. Microbiol. 2019, 9, 44. [Google Scholar] [CrossRef]
- Di Leo, V.; Gleeson, P.J.; Sallustio, F.; Bounaix, C.; Da Silva, J.; Loreto, G.; Ben Mkaddem, S.; Monteiro, R.C. Rifaximin as a Potential Treatment for IgA Nephropathy in a Humanized Mice Model. J. Pers. Med. 2021, 11, 309. [Google Scholar] [CrossRef]
- Mohandas, S.; Vairappan, B. Role of pregnane X-receptor in regulating bacterial translocation in chronic liver diseases. World J. Hepatol. 2017, 9, 1210–1226. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Barbara, G.; DuPont, H.L.; Mearin, F.; Gasbarrini, A.; Tack, J. New concepts on intestinal microbiota and the role of the non-absorbable antibiotics with special reference to rifaximin in digestive diseases. Dig. Liver Dis. 2018, 50, 741–749. [Google Scholar] [CrossRef]
- Ponziani, F.R.; Zocco, M.A.; D’Aversa, F.; Pompili, M.; Gasbarrini, A. Eubiotic properties of rifaximin: Disruption of the traditional concepts in gut microbiota modulation. World J. Gastroenterol. 2017, 23, 4491–4499. [Google Scholar] [CrossRef]
- Lopetuso, L.R.; Napoli, M.; Rizzatti, G.; Gasbarrini, A. The intriguing role of Rifaximin in gut barrier chronic inflammation and in the treatment of Crohn’s disease. Expert Opin Investig. Drugs 2018, 27, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Cerutti, A.; Cols, M.; Gentile, M.; Cassis, L.; Barra, C.M.; He, B.; Puga, I.; Chen, K. Regulation of mucosal IgA responses: Lessons from primary immunodeficiencies. Ann. N. Y. Acad. Sci. 2011, 1238, 132–144. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, B.; Belvedere, O.; Roschke, V.; Moore, P.A.; Olsen, H.S.; Migone, T.S.; Sosnovtseva, S.; Carrell, J.A.; Feng, P.; Giri, J.G.; et al. Synthesis and release of B-lymphocyte stimulator from myeloid cells. Blood 2001, 97, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Vincent, F.B.; Saulep-Easton, D.; Figgett, W.A.; Fairfax, K.A.; Mackay, F. The BAFF/APRIL system: Emerging functions beyond B cell biology and autoimmunity. Cytokine Growth Factor Rev. 2013, 24, 203–215. [Google Scholar] [CrossRef]
- Lopez-Fraga, M.; Fernandez, R.; Albar, J.P.; Hahne, M. Biologically active APRIL is secreted following intracellular processing in the Golgi apparatus by furin convertase. EMBO Rep. 2001, 2, 945–951. [Google Scholar] [CrossRef]
- Day, E.S.; Cachero, T.G.; Qian, F.; Sun, Y.; Wen, D.; Pelletier, M.; Hsu, Y.M.; Whitty, A. Selectivity of BAFF/BLyS and APRIL for binding to the TNF family receptors BAFFR/BR3 and BCMA. Biochemistry 2005, 44, 1919–1931. [Google Scholar] [CrossRef]
- Takahara, M.; Nagato, T.; Nozaki, Y.; Kumai, T.; Katada, A.; Hayashi, T.; Harabuchi, Y. A proliferation-inducing ligand (APRIL) induced hyper-production of IgA from tonsillar mononuclear cells in patients with IgA nephropathy. Cell. Immunol. 2019, 341, 103925. [Google Scholar] [CrossRef]
- Myette, J.R.; Kano, T.; Suzuki, H.; Sloan, S.E.; Szretter, K.J.; Ramakrishnan, B.; Adari, H.; Deotale, K.D.; Engler, F.; Shriver, Z.; et al. A Proliferation Inducing Ligand (APRIL) targeted antibody is a safe and effective treatment of murine IgA nephropathy. Kidney Int. 2019, 96, 104–116. [Google Scholar] [CrossRef]
- Cao, Y.; Lu, G.; Chen, X.; Chen, X.; Guo, N.; Li, W. BAFF is involved in the pathogenesis of IgA nephropathy by activating the TRAF6/NF-kappaB signaling pathway in glomerular mesangial cells. Mol. Med. Rep. 2020, 21, 795–805. [Google Scholar] [CrossRef]
- Barratt, J.; Tumlin, J.; Suzuki, Y.; Kao, A.; Aydemir, A.; Pudota, K.; Jin, H.; Guhring, H.; Appel, G.; JANUS study investigators. Randomized Phase II JANUS Study of Atacicept in Patients with IgA Nephropathy and Persistent Proteinuria. Kidney Int. Rep. 2022, 7, 1831–1841. [Google Scholar] [CrossRef]
- Stohl, W.; Merrill, J.T.; Looney, R.J.; Buyon, J.; Wallace, D.J.; Weisman, M.H.; Ginzler, E.M.; Cooke, B.; Holloway, D.; Kaliyaperumal, A.; et al. Treatment of systemic lupus erythematosus patients with the BAFF antagonist “peptibody” blisibimod (AMG 623/A-623): Results from randomized, double-blind phase 1a and phase 1b trials. Arthritis Res. Ther. 2015, 17, 215. [Google Scholar] [CrossRef]
- Yeo, S.C.; Liew, A.; Barratt, J. Emerging therapies in immunoglobulin A nephropathy. Nephrology 2015, 20, 788–800. [Google Scholar] [CrossRef]
- Lenert, A.; Niewold, T.B.; Lenert, P. Spotlight on blisibimod and its potential in the treatment of systemic lupus erythematosus: Evidence to date. Drug Des. Dev. Ther. 2017, 11, 747–757. [Google Scholar] [CrossRef]
- Huang, X.; Xu, G. An Update on Targeted Treatment of IgA Nephropathy: An Autoimmune Perspective. Front. Pharmacol. 2021, 12, 715253. [Google Scholar] [CrossRef]
- Jayne, D. Role of rituximab therapy in glomerulonephritis. J. Am. Soc. Nephrol. JASN 2010, 21, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Jarrick, S.; Lundberg, S.; Welander, A.; Carrero, J.J.; Hoijer, J.; Bottai, M.; Ludvigsson, J.F. Mortality in IgA Nephropathy: A Nationwide Population-Based Cohort Study. J. Am. Soc. Nephrol. JASN 2019, 30, 866–876. [Google Scholar] [CrossRef] [PubMed]
- Fervenza, F.C.; Appel, G.B.; Barbour, S.J.; Rovin, B.H.; Lafayette, R.A.; Aslam, N.; Jefferson, J.A.; Gipson, P.E.; Rizk, D.V.; Sedor, J.R.; et al. Rituximab or Cyclosporine in the Treatment of Membranous Nephropathy. N. Engl. J. Med. 2019, 381, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Medjeral-Thomas, N.R.; Cook, H.T.; Pickering, M.C. Complement activation in IgA nephropathy. Semin. Immunopathol. 2021, 43, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Stangou, M.; Alexopoulos, E.; Pantzaki, A.; Leonstini, M.; Memmos, D. C5b-9 glomerular deposition and tubular alpha3beta1-integrin expression are implicated in the development of chronic lesions and predict renal function outcome in immunoglobulin A nephropathy. Scand. J. Urol. Nephrol. 2008, 42, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Zhang, Y.; Duan, X.; Peng, Q.; Liu, Q.; Zhou, Y.; Quan, S.; Xing, G. C3a, C5a renal expression and their receptors are correlated to severity of IgA nephropathy. J. Clin. Immunol. 2014, 34, 224–232. [Google Scholar] [CrossRef]
- Ring, T.; Pedersen, B.B.; Salkus, G.; Goodship, T.H. Use of eculizumab in crescentic IgA nephropathy: Proof of principle and conundrum? Clin. Kidney J. 2015, 8, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Rosenblad, T.; Rebetz, J.; Johansson, M.; Bekassy, Z.; Sartz, L.; Karpman, D. Eculizumab treatment for rescue of renal function in IgA nephropathy. Pediatr. Nephrol. 2014, 29, 2225–2228. [Google Scholar] [CrossRef] [PubMed]
- Herzog, A.L.; Wanner, C.; Amann, K.; Lopau, K. First Treatment of Relapsing Rapidly Progressive IgA Nephropathy with Eculizumab after Living Kidney Donation: A Case Report. Transplant. Proc. 2017, 49, 1574–1577. [Google Scholar] [CrossRef]
- Komers, R.; Plotkin, H. Dual inhibition of renin-angiotensin-aldosterone system and endothelin-1 in treatment of chronic kidney disease. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2016, 310, R877–R884. [Google Scholar] [CrossRef] [PubMed]
- Woo, K.T.; Lau, Y.K.; Wong, K.S.; Chiang, G.S. ACEI/ATRA therapy decreases proteinuria by improving glomerular permselectivity in IgA nephritis. Kidney Int. 2000, 58, 2485–2491. [Google Scholar] [CrossRef] [PubMed]
- Szeto, C.C.; Kwan, B.C.; Chow, K.M.; Leung, C.B.; Li, P.K. The safety and short-term efficacy of aliskiren in the treatment of immunoglobulin a nephropathy--a randomized cross-over study. PLoS ONE 2013, 8, e62736. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Radhakrishnan, J.; Alpers, C.E.; Barratt, J.; Bieler, S.; Diva, U.; Inrig, J.; Komers, R.; Mercer, A.; Noronha, I.L.; et al. Sparsentan in patients with IgA nephropathy: A prespecified interim analysis from a randomised, double-blind, active-controlled clinical trial. Lancet 2023, 401, 1584–1594. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Stefansson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef]
- Smeijer, J.D.; Kohan, D.E.; Webb, D.J.; Dhaun, N.; Heerspink, H.J.L. Endothelin receptor antagonists for the treatment of diabetic and nondiabetic chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2021, 30, 456–465. [Google Scholar] [CrossRef]
- Rajasekaran, A.; Julian, B.A.; Rizk, D.V. IgA Nephropathy: An Interesting Autoimmune Kidney Disease. Am. J. Med. Sci. 2021, 361, 176–194. [Google Scholar] [CrossRef]
- Liu, L.J.; Yang, Y.Z.; Shi, S.F.; Bao, Y.F.; Yang, C.; Zhu, S.N.; Sui, G.L.; Chen, Y.Q.; Lv, J.C.; Zhang, H. Effects of Hydroxychloroquine on Proteinuria in IgA Nephropathy: A Randomized Controlled Trial. Am. J. Kidney Dis. 2019, 74, 15–22. [Google Scholar] [CrossRef]
- Wanner, C.; Inzucchi, S.E.; Lachin, J.M.; Fitchett, D.; von Eynatten, M.; Mattheus, M.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Zinman, B.; et al. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 323–334. [Google Scholar] [CrossRef]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef]
- Wheeler, D.C.; Toto, R.D.; Stefansson, B.V.; Jongs, N.; Chertow, G.M.; Greene, T.; Hou, F.F.; McMurray, J.J.V.; Pecoits-Filho, R.; Correa-Rotter, R.; et al. A pre-specified analysis of the DAPA-CKD trial demonstrates the effects of dapagliflozin on major adverse kidney events in patients with IgA nephropathy. Kidney Int. 2021, 100, 215–224. [Google Scholar] [CrossRef]
- Keener, A.B. SGLT2 inhibitors breathe life into kidney-disease care. Nature 2023, 615, S2–S4. [Google Scholar] [CrossRef] [PubMed]
- Neuen, B.L.; Young, T.; Heerspink, H.J.L.; Neal, B.; Perkovic, V.; Billot, L.; Mahaffey, K.W.; Charytan, D.M.; Wheeler, D.C.; Arnott, C.; et al. SGLT2 inhibitors for the prevention of kidney failure in patients with type 2 diabetes: A systematic review and meta-analysis. Lancet. Diabetes Endocrinol. 2019, 7, 845–854. [Google Scholar] [CrossRef] [PubMed]
- The, E.-K.C.G.; Herrington, W.G.; Staplin, N.; Wanner, C.; Green, J.B.; Hauske, S.J.; Emberson, J.R.; Preiss, D.; Judge, P.; Mayne, K.J.; et al. Empagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2023, 388, 117–127. [Google Scholar] [CrossRef]
- Herrington, W.G.; Frankel, A.H.; Wonnacott, A.; Webb, D.; Watt, A.; Watson, M.; Roberts, J.; Staplin, N.; Roddick, A.; Riding, A.; et al. UK Kidney Association Clinical Practice Guideline: Sodium-Glucose Co-Transporter-2 (SGLT-2) Inhibition in Adults with Kidney Disease; UK Kidney Association: Bristol, UK, 2021. [Google Scholar]
- Dave, C.V.; Schneeweiss, S.; Patorno, E. Comparative risk of genital infections associated with sodium-glucose co-transporter-2 inhibitors. Diabetes Obes. Metab. 2019, 21, 434–438. [Google Scholar] [CrossRef]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R.; et al. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Petrykiv, S.I.; Laverman, G.D.; de Zeeuw, D.; Heerspink, H.J.L. The albuminuria-lowering response to dapagliflozin is variable and reproducible among individual patients. Diabetes Obes. Metab. 2017, 19, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Bersoff-Matcha, S.J.; Chamberlain, C.; Cao, C.; Kortepeter, C.; Chong, W.H. Fournier Gangrene Associated with Sodium-Glucose Cotransporter-2 Inhibitors: A Review of Spontaneous Postmarketing Cases. Ann. Intern. Med. 2019, 170, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Mathur, M.; Barratt, J.; Suzuki, Y.; Engler, F.; Pasetti, M.F.; Yarbrough, J.; Sloan, S.; Oldach, D. Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of VIS649 (Sibeprenlimab), an APRIL-Neutralizing IgG(2) Monoclonal Antibody, in Healthy Volunteers. Kidney Int. Rep. 2022, 7, 993–1003. [Google Scholar] [CrossRef] [PubMed]
- Bruchfeld, A.; Magin, H.; Nachman, P.; Parikh, S.; Lafayette, R.; Potarca, A.; Miao, S.; Bekker, P. C5a receptor inhibitor avacopan in immunoglobulin A nephropathy-an open-label pilot study. Clin. Kidney J. 2022, 15, 922–928. [Google Scholar] [CrossRef] [PubMed]
- de Zeeuw, D.; Coll, B.; Andress, D.; Brennan, J.J.; Tang, H.; Houser, M.; Correa-Rotter, R.; Kohan, D.; Lambers Heerspink, H.J.; Makino, H.; et al. The endothelin antagonist atrasentan lowers residual albuminuria in patients with type 2 diabetic nephropathy. J. Am. Soc. Nephrol. JASN 2014, 25, 1083–1093. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Drug | Site of Action | Clinical Research Trial/Study on Mouse Models of IgAN | Possible Outcomes | Possible Adverse Effects (AE) |
|---|---|---|---|---|
| Inhibition of Excessive Mucosal Immune Response | ||||
| TRF Budesonide | Peyer’s patches in the distal ileum | Randomized, double-blind, placebo-controlled study Phase III clinical trial (NefIgArd) NCT03643965 Active, not recruiting | Reduction in UPCR and GFR preservation | Hypertension, peripheral oedema, muscle spasms, and acne [23] |
| Prebiotics and probiotics | Inhibition of NLRP3/ASC/ Caspase 1 signaling pathway [32] | 35 patients with IgAN and C57BL/6 mice | Alleviation of gut dysbiosis and attenuation of IgAN clinicopathological manifestations | |
| Rifaximin | Inhibition of microbe-induced immune response and has a direct anti-inflammatory property through binding to the pregnane X receptor (PXR) and modulating gut microbiota [37] | α1KI-CD89Tg mice | Reduction in UPCR, serum levels of hIgA1–sCD89 and mIgG–hIgA1 complexes, hIgA1 glomerular deposition, and CD11b+ cell infiltration | Nausea, stomach pain, dizziness, tiredness, headache, and joint pain |
| Inhibition of BAFF and APRIL Pathways | ||||
| VIS649 (Sibeprenlimab) | Humanized IgG2 monoclonal antibody that inhibits APRIL | Multicenter, randomized, double-blind, placebo-controlled study Phase III trial (Visionary Study) NCT05248646 [83] Recruiting | Reduction in serum APRIL, IgA, Gd-IgA1, IgG, and IgM | No serious Aes or Aes leading to study discontinuation |
| BION-1301 | Novel humanized blocking antibody targeting APRIL | Part 1: randomized, placebo-controlled single ascending dose design in healthy volunteers; Part 2: randomized, placebo-controlled, multiple ascending dose design in HVs; Part 3 (MD-IgAN): open-label multiple dose design in subjects with IgAN NCT03945318 Active, not recruiting | Reduction in serum levels of APRIL, of immunoglobulins, and in proteinuria | Well-tolerated with no serious adverse events |
| Atacicept | Inhibits BlyS and APRIL [50] | Phase Iib randomized, double-blind, placebo-controlled, dose-ranging study (ORIGIN 3) NCT04716231 Recruiting | Reduction in IgA, IgG, IgM, and Gd-IgA in proteinuria | Aes of special interest included cardiac failure, ischemic heart disease, cardiac arrhythmia, infections, hypersensitivity reactions, and injection-site reactions |
| Blisibimod | Inhibits both soluble and membrane BAFF | Randomized, double-blind, placebo-controlled Phase 2/3 study (BRIGHT-SC) NCT02062684 Completed | Reduction in level of peripheral B cells, immunoglobulins, and UPCR | Upper respiratory tract infection, urinary tract infection, injection site erythema/reaction, and diarrhea |
| Rituximab | Anti-CD20 monoclonal antibody | Multicenter, randomized, prospective, open-label trial NCT00498368 Completed | Changes in proteinuria levels | Fever; cold symptoms, such as runny nose or sore throat; flu symptoms, such as cough, tiredness, and body aches; headache; and cold sores in the mouth or throat |
| Inhibition of Complement Activation | ||||
| Narsoplimab (OMS721) | Anti-mannan-associated lectin-binding serine protease-2 (MASP-2) | Randomized, double-blind, placebo-controlled Phase 3 study (ARTEMIS-IGAN) NCT03608033 Recruiting | Change from baseline in UPE and proteinuria reduction, rate of change in GFR, and safety and tolerability | Headache, upper respiratory infection, and fatigue |
| Iptacopan (LNP023) | Inhibits factor B inhibitor of the alternative complement pathway | Randomized, double-blind, dose-ranging, parallel-group Phase 3 study (APPLAUSE-IgAN) NCT03373461 Completed | Reduction in UPCR | Headache, abdominal discomfort, blood alkaline phosphatase increase, cough, oropharyngeal pain, pyrexia, and upper respiratory infection |
| Pegcetacoplan (APL-2) | Inhibits C3 protein | Phase 2 study NCT03453619 Active, not recruiting | Proteinuria reduction changes in disease-specific biomarkers (serum C3 levels, AH50 and C3a concentrations, and serum albumin levels) Stabilization or improvement in estimated GFR | No serious or severe AE were reported; stomach pain, vomiting, diarrhea, cold sores, cold symptoms, and tiredness |
| Eculizumab | Inhibits C5 convertase | Case reports [61,62,63] | Temporary stabilization, but not improvement, of GFR | No AEs were described in the cited case reports |
| Avacopan (CCX168) | Selective C5a receptor inhibitor | Open-label pilot study [84] | Improvement in UPCR | One serious AE of unstable angina, which was deemed to be unrelated to avacopan |
| Ravulizumab | Monoclonal antibody against C5 | Phase 2, double-blind, randomized, placebo-controlled study (SANCTUARY) NCT04564339 Recruiting | Reduction in UPCR and improvement in GFR | Upper respiratory tract infection, diarrhea, nausea, vomiting, headache, high blood pressure, and fever |
| Cemdisiran (ALN-CC5) | Suppresses liver production of C5 protein | Phase 2, randomized, double-blind, placebo-controlled study NCT03841448 Active, not recruiting | Reduction in UPCR | No serious or severe AEs |
| Inhibition of Kidney Damage and Fibrosis | ||||
| Aliskiren | Direct renin inhibitor | Randomized crossover study NCT00870493 Completed | Anti-proteinuric effect [66] | Hyperkalemia |
| Sparsentan | Selective antagonist of angiotensin II receptor and endothelin A receptor | Randomized, multicenter, double-blind, parallel-group, active-controlled study (PROTECT) NCT03762850 [67] Active, not recruiting | Reduction in proteinuria | Well-tolerated with a clearly defined safety profile |
| Atrasentan | Antagonist of endothelin A receptor | Phase 3, randomized, double-blind, placebo-controlled study (ALIGN) NCT04573478 Active, not recruiting Phase 2, open-label, basket study (AFFINITY) NCT04573920 Recruiting | Effect on proteinuria | Increase in weight and a reduction in hemoglobin [85] |
| Other drugs | ||||
| Hydroxychloroquine (HCQ) | Inhibits mucosal and intrarenal toll-like receptor signaling | Randomized, double-blind, placebo-controlled study NCT02942381 Completed | Reduction in proteinuria and GFR preservation | HCQ was well-tolerated, and no serious AEs were recorded [71] |
| Sodium-glucose cotransporter 2 inhibitors (SGLT2i) | Modulation of inflammatory and profibrotic mediators and regulation of toxic intracellular compounds (i.e., advanced glycation end products) | International, multicenter, event-driven, randomized, double-blind, parallel group, placebo-controlled study (Dapa-CKD) NCT03036150 Completed Multicenter international randomized parallel-froup double-blind placebo-controlled clinical trial (EMPA-KIDNEY) NCT03594110 Active, not recruiting | Preservation of GFR Reduction in end-stage kidney disease, in death from renal causes, in death from cardiovascular causes, or inhospitalization for heart failure | Genital infections Changes in urination, including urgent need to urinate more often, in larger amounts, or at night [79] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Leo, V.; Annese, F.; Papadia, F.; Cara, I.; Giliberti, M.; Sallustio, F.; Gesualdo, L. The Landscape of IgA Nephropathy Treatment Strategy: A Pharmacological Overview. Future Pharmacol. 2023, 3, 517-534. https://doi.org/10.3390/futurepharmacol3020033
Di Leo V, Annese F, Papadia F, Cara I, Giliberti M, Sallustio F, Gesualdo L. The Landscape of IgA Nephropathy Treatment Strategy: A Pharmacological Overview. Future Pharmacology. 2023; 3(2):517-534. https://doi.org/10.3390/futurepharmacol3020033
Chicago/Turabian StyleDi Leo, Vincenzo, Francesca Annese, Federica Papadia, Iris Cara, Marica Giliberti, Fabio Sallustio, and Loreto Gesualdo. 2023. "The Landscape of IgA Nephropathy Treatment Strategy: A Pharmacological Overview" Future Pharmacology 3, no. 2: 517-534. https://doi.org/10.3390/futurepharmacol3020033
APA StyleDi Leo, V., Annese, F., Papadia, F., Cara, I., Giliberti, M., Sallustio, F., & Gesualdo, L. (2023). The Landscape of IgA Nephropathy Treatment Strategy: A Pharmacological Overview. Future Pharmacology, 3(2), 517-534. https://doi.org/10.3390/futurepharmacol3020033