

Menstrual Cycle Tracking in Sports Research: Challenges, Progress, and Future Directions


Abstract
:1. Introduction
2. The Menstrual Cycle
3. Female Hormone Impact on Sport Physiology
3.1. Energy Metabolism
3.2. Hydration and Fluid Balance
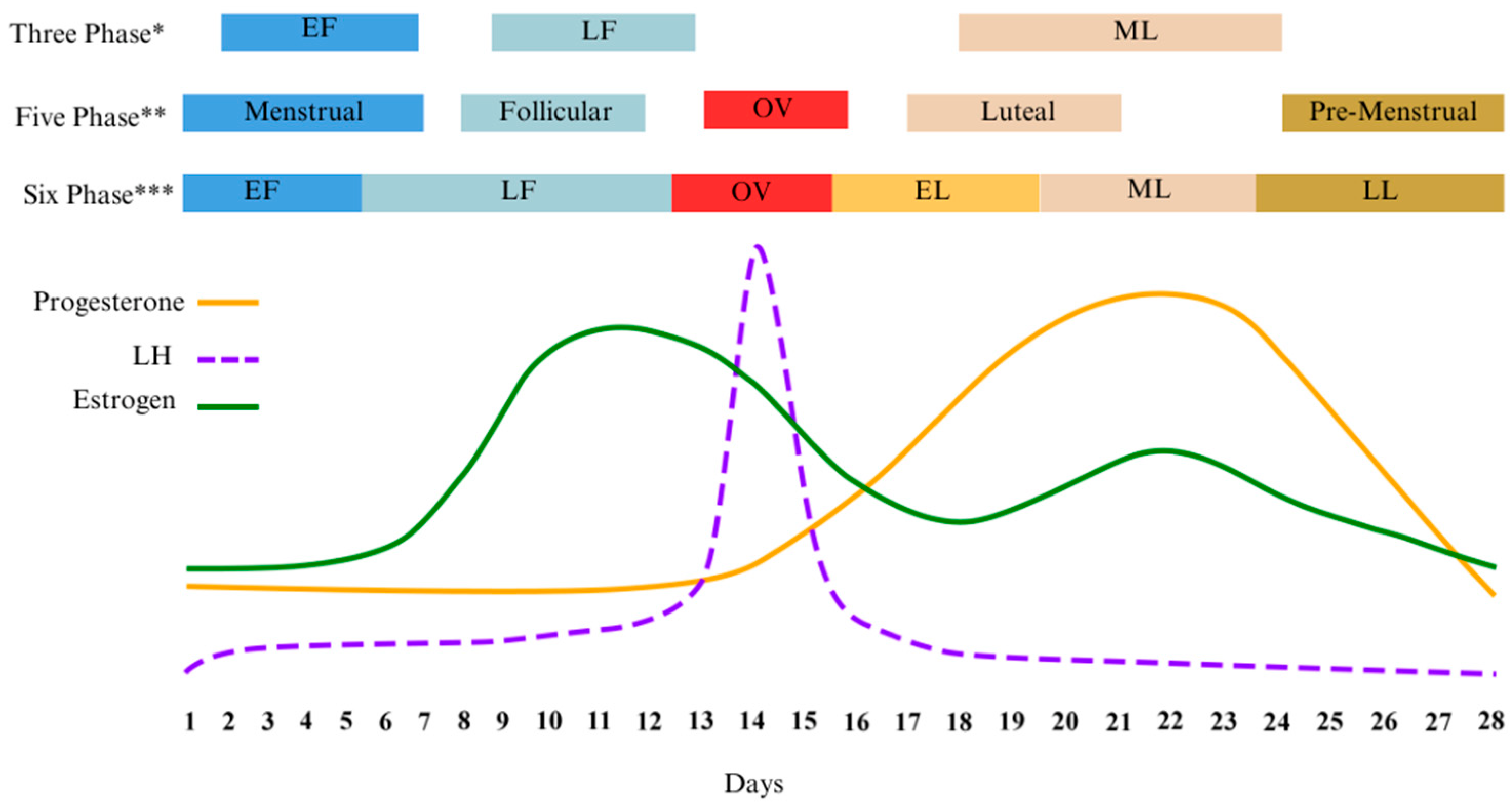
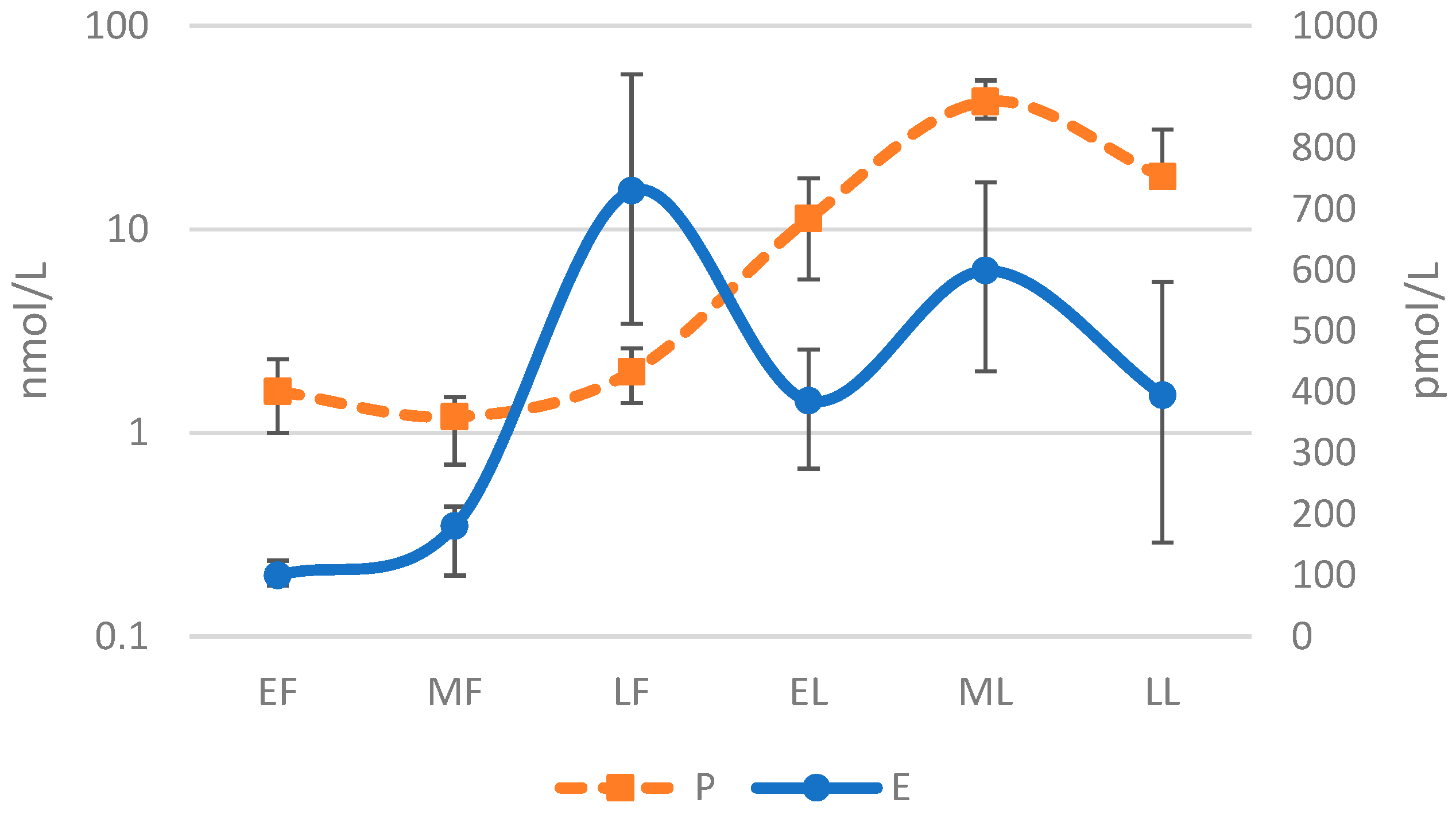
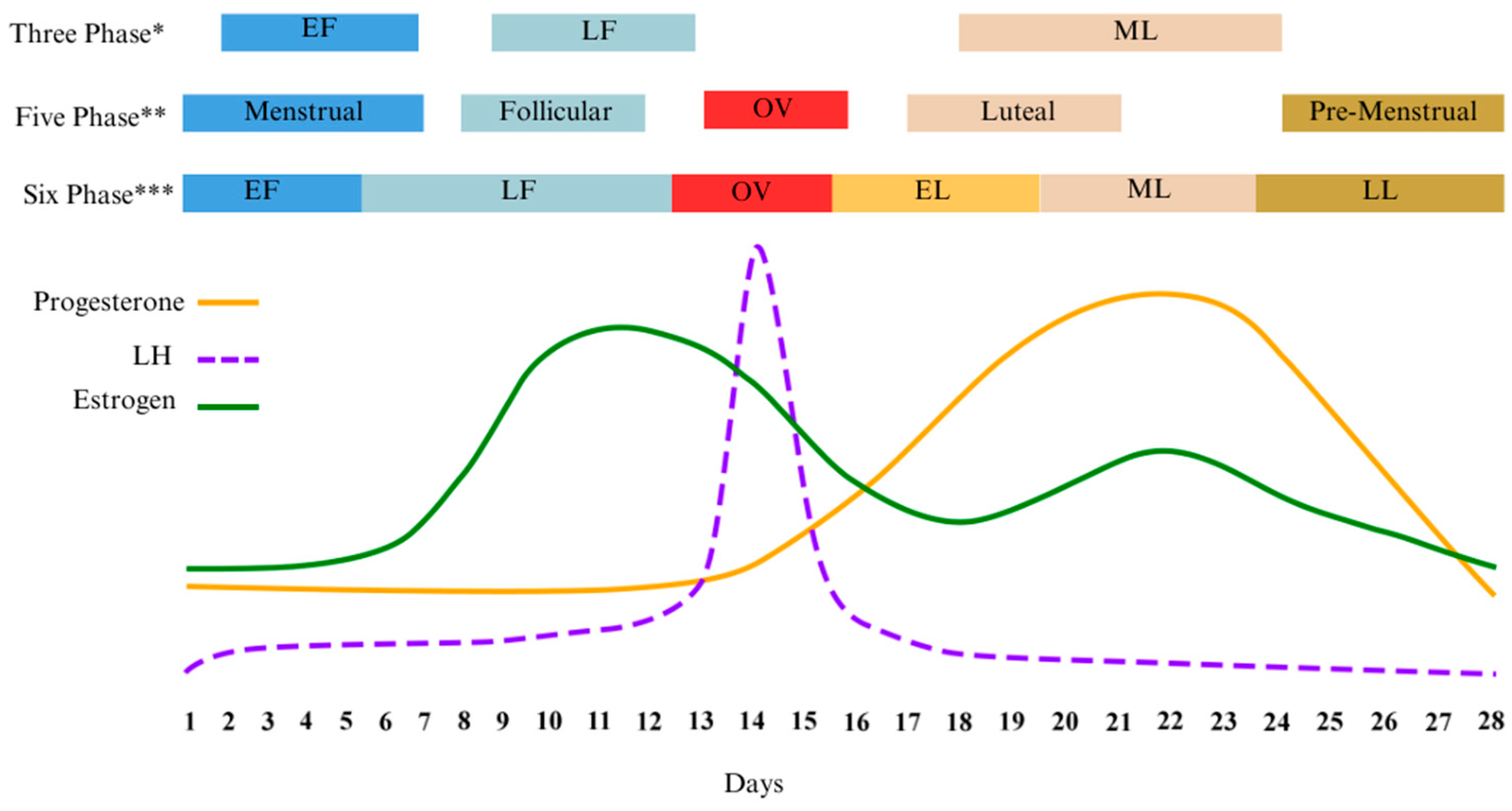
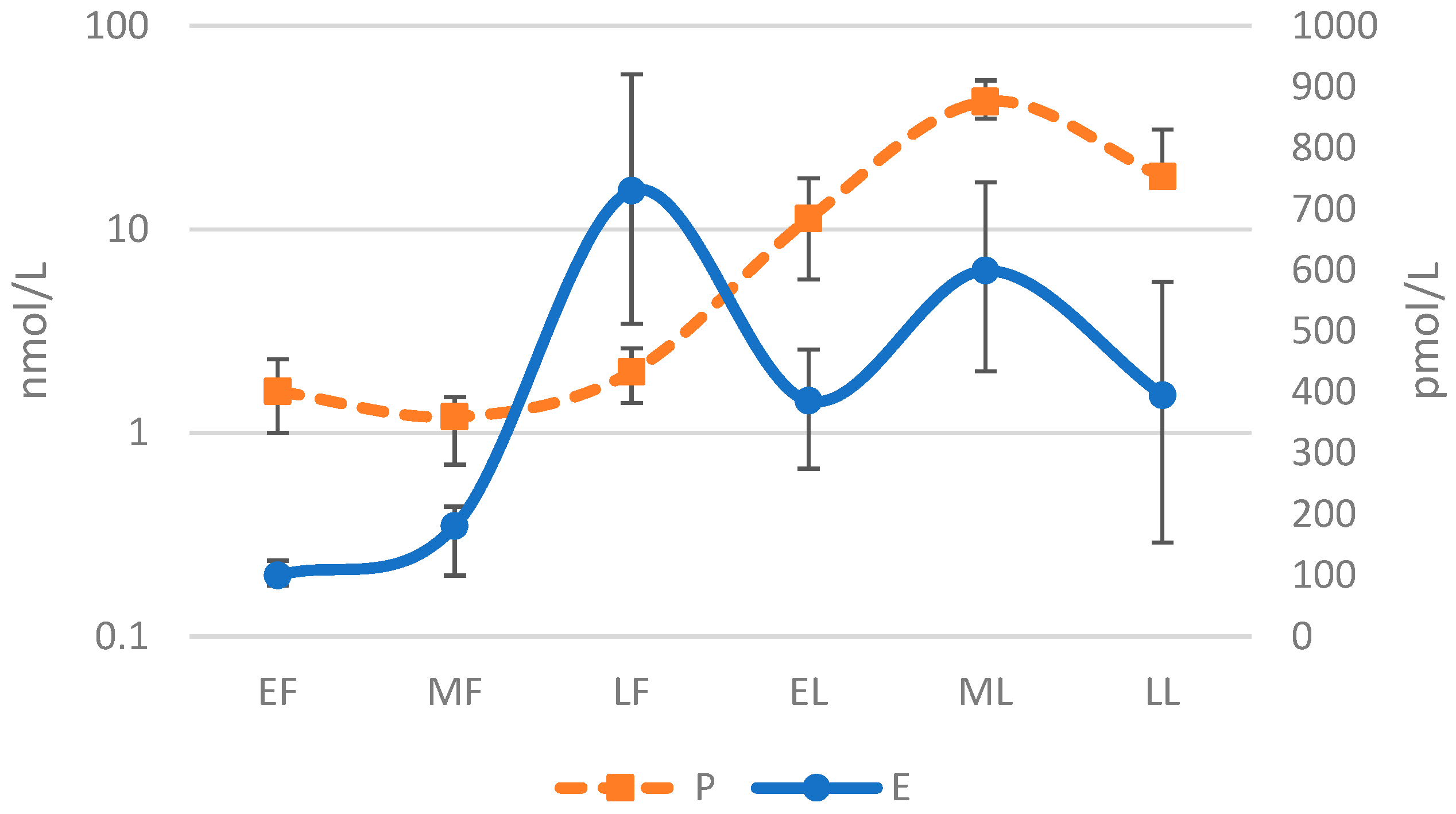
3.3. Menstrual Phase Terminology
4. Methodologies Past and Present
4.1. Hormone Profile Validation
4.2. Point of Ovulation Validation
4.2.1. Follicular Monitoring
4.2.2. Salivary Ferning
4.2.3. Counting Days
4.2.4. Menstrual Cycle Tracking Apps
4.2.5. Basal Body Temperature (BBT)
4.2.6. Urinary Luteinising Hormone (LH)
4.2.7. Cervical Mucus
4.3. Combined Methods
5. Obstacles to Phase Validation
6. Future of Menstrual Cycle Tracking
Author Contributions
Funding
Conflicts of Interest
References
- Hevener, A.L.; Ribas, V.; Moore, T.M.; Zhou, Z. The Impact of Skeletal Muscle ERα on Mitochondrial Function and Metabolic Health. Endocrinology 2020, 161, bqz017. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Seeley, R.J.; Clegg, D.J. Sexual Differences in the Control of Energy Homeostasis. Front. Neuroendocrinol. 2009, 30, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Cho, H.T.; Kim, Y.J. The Role of Estrogen in Adipose Tissue Metabolism: Insights into Glucose Homeostasis Regulation. Endocr. J. 2014, 61, 1055–1067. [Google Scholar] [CrossRef] [PubMed]
- Frank, A.; Brown, L.M.; Clegg, D.J. The Role of Hypothalamic Estrogen Receptors in Metabolic Regulation. Front. Neuroendocrinol. 2014, 35, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Hevener, A.L.; Zhou, Z.; Drew, B.G.; Ribas, V. The Role of Skeletal Muscle Estrogen Receptors in Metabolic Homeostasis and Insulin Sensitivity. In Advances in Experimental Medicine and Biology; Springer: Berlin/Heidelberg, Germany, 2017; Volume 1043, pp. 257–284. [Google Scholar]
- Hevener, A.L.; Zhou, Z.; Moore, T.M.; Drew, B.G.; Ribas, V. The Impact of ERα Action on Muscle Metabolism and Insulin Sensitivity—Strong Enough for a Man, Made for a Woman. Mol. Metab. 2018, 15, 20–34. [Google Scholar] [CrossRef] [PubMed]
- Ropero, A.B.; Alonso-Magdalena, P.; Quesada, I.; Nadal, A. The Role of Estrogen Receptors in the Control of Energy and Glucose Homeostasis. Steroids 2008, 73, 874–879. [Google Scholar] [CrossRef]
- Hevener, A.L.; Clegg, D.J.; Mauvais-Jarvis, F. Impaired Estrogen Receptor Action in the Pathogenesis of the Metabolic Syndrome. Mol. Cell. Endocrinol. 2015, 418, 306–321. [Google Scholar] [CrossRef]
- Chen, J.Q.; Brown, T.R.; Russo, J. Regulation of Energy Metabolism Pathways by Estrogens and Estrogenic Chemicals and Potential Implications in Obesity Associated with Increased Exposure to Endocrine Disruptors. Biochim. Biophys. Acta Mol. Cell Res. 2009, 1793, 1128–1143. [Google Scholar] [CrossRef]
- Howe, J.C.; Rumpler, W.V.; Seale, J.L. Energy Expenditure by Indirect Calorimetry in Premenopausal Women: Variation within One Menstrual Cycle. J. Nutr. Biochem. 1993, 4, 268–273. [Google Scholar] [CrossRef]
- Zhang, S.; Osumi, H.; Uchizawa, A.; Hamada, H.; Park, I.; Suzuki, Y.; Tanaka, Y.; Ishihara, A.; Yajima, K.; Seol, J.; et al. Changes in Sleeping Energy Metabolism and Thermoregulation during Menstrual Cycle. Physiol. Rep. 2020, 8, e14353. [Google Scholar] [CrossRef]
- Benton, M.J.; Hutchins, A.M.; Dawes, J.J. Effect of Menstrual Cycle on Resting Metabolism: A Systematic Review and Metaanalysis. PLoS ONE 2020, 15, e0236025. [Google Scholar] [CrossRef]
- Chapman, A.B.; Zamudio, S.; Woodmansee, W.; Merouani, A.; Osorio, F.; Johnson, A.; Moore, L.G.; Dahms, T.; Coffin, C.; Abraham, W.T.; et al. Systemic and Renal Hemodynamic Changes in the Luteal Phase of the Menstrual Cycle Mimic Early Pregnancy. Am. J. Physiol. Ren. Physiol. 1997, 273, F777–F782. [Google Scholar] [CrossRef]
- Szmuilowicz, E.D.; Adler, G.K.; Williams, J.S.; Green, D.E.; Yao, T.M.; Hopkins, P.N.; Seely, E.W. Relationship between Aldosterone and Progesterone in the Human Menstrual Cycle. J. Clin. Endocrinol. Metab. 2006, 91, 3981–3987. [Google Scholar] [CrossRef]
- Pechère-Bertschi, A.; Maillard, M.; Stalder, H.; Brunner, H.R.; Burnier, M. Renal Segmental Tubular Response to Salt during the Normal Menstrual Cycle. Kidney Int. 2002, 61, 425–431. [Google Scholar] [CrossRef]
- Olson, B.R.; Forman, M.R.; Lanza, E.; McAdam, P.A.; Beecher, G.; Kimzey, L.M.; Campbell, W.S.; Raymond, E.G.; Brentzel, S.L.; Güttsches-Ebeling, B. Relation between Sodium Balance and Menstrual Cycle Symptoms in Normal Women. Ann. Intern. Med. 1996, 125, 564–567. [Google Scholar] [CrossRef]
- Landau, R.L.; Lugibihl, K. The Effect of Progesterone on Amino Acid Metabolism. J. Clin. Endocrinol. Metab. 1961, 21, 1355–1363. [Google Scholar] [CrossRef]
- Draper, C.F.; Duisters, K.; Weger, B.; Chakrabarti, A.; Harms, A.C.; Brennan, L.; Hankemeier, T.; Goulet, L.; Konz, T.; Martin, F.P.; et al. Menstrual Cycle Rhythmicity: Metabolic Patterns in Healthy Women. Sci. Rep. 2018, 8, e14568. [Google Scholar] [CrossRef]
- Faustmann, G.; Meinitzer, A.; Magnes, C.; Tiran, B.; Obermayer-Pietsch, B.; Gruber, H.J.; Ribalta, J.; Rock, E.; Roob, J.M.; Winklhofer-Roob, B.M. Progesterone-Associated Arginine Decline at Luteal Phase of Menstrual Cycle and Associations with Related Amino Acids and Nuclear Factor KB Activation. PLoS ONE 2018, 13, e0200489. [Google Scholar] [CrossRef] [PubMed]
- Kriengsinyos, W.; Wykes, L.J.; Goonewardene, L.A.; Ball, R.O.; Pencharz, P.B. Phase of Menstrual Cycle Affects Lysine Requirement in Healthy Women. Am. J. Physiol. Endocrinol. Metab. 2004, 287, E489–E496. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.E.; Febbraio, M.A. Effect of the Ovarian Hormones on GLUT4 Expression and Contraction-Stimulated Glucose Uptake. Am. J. Physiol. Endocrinol. Metab. 2002, 282, E1139–E1146. [Google Scholar] [CrossRef] [PubMed]
- Flannery, C.A.; Choe, G.H.; Cooke, K.M.; Fleming, A.G.; Radford, C.C.; Kodaman, P.H.; Jurczak, M.J.; Kibbey, R.G.; Taylor, H.S. Insulin Regulates Glycogen Synthesis in Human Endometrial Glands through Increased GYS2. J. Clin. Endocrinol. Metab. 2018, 103, 2843–2850. [Google Scholar] [CrossRef]
- Zhang, H.; Qi, J.; Wang, Y.; Sun, J.; Li, Z.; Sui, L.; Fan, J.; Liu, C.; Shang, Y.; Kong, L.; et al. Progesterone Regulates Glucose Metabolism Through Glucose Transporter 1 to Promote Endometrial Receptivity. Front. Physiol. 2020, 11, 543148. [Google Scholar] [CrossRef]
- Han, H.S.; Kang, G.; Kim, J.S.; Choi, B.H.; Koo, S.H. Regulation of Glucose Metabolism from a Liver-Centric Perspective. Exp. Mol. Med. 2016, 48, e218. [Google Scholar] [CrossRef]
- Oosthuyse, T.; Bosch, A.N. The Effect of the Menstrual Cycle on Exercise Metabolism: Implications for Exercise Performance in Eumenorrhoeic Women. Sports Med. 2010, 40, 207–227. [Google Scholar] [CrossRef]
- Elliott-Sale, K.J.; Minahan, C.L.; de Jonge, X.A.K.J.; Ackerman, K.E.; Sipilä, S.; Constantini, N.W.; Lebrun, C.M.; Hackney, A.C. Methodological Considerations for Studies in Sport and Exercise Science with Women as Participants: A Working Guide for Standards of Practice for Research on Women. Sports Med. 2021, 51, 843–861. [Google Scholar] [CrossRef]
- Janse De Jonge, X.A.K. Effects of the Menstrual Cycle on Exercise Performance. Sports Med. 2003, 33, 833–851. [Google Scholar] [CrossRef]
- Paul, R.W.; Sonnier, J.H.; Johnson, E.E.; Hall, A.T.; Osman, A.; Connors, G.M.; Freedman, K.B.; Bishop, M.E. Inequalities in the Evaluation of Male Versus Female Athletes in Sports Medicine Research: A Systematic Review. Am. J. Sports Med. 2023, 51, 3335–3342. [Google Scholar] [CrossRef]
- Deldicque, L. Editorial: Women in Elite Sports and Performance Enhancement: 2021. Front. Sports Act. Living 2022, 4, 999969. [Google Scholar] [CrossRef]
- Sims, S.T.; Heather, A.K. Myths and Methodologies: Reducing Scientific Design Ambiguity in Studies Comparing Sexes and/or Menstrual Cycle Phases. Exp. Physiol. 2018, 103, 1309–1317. [Google Scholar] [CrossRef] [PubMed]
- Tarnopolsky, L.J.; MacDougall, J.D.; Atkinson, S.A.; Tarnopolsky, M.A.; Sutton, J.R. Gender Differences in Substrate for Endurance Exercise. J. Appl. Physiol. 1990, 68, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Hackney, A.C.; McCracken-Compton, M.A.; Ainsworth, B. Substrate Responses to Submaximal Exercise in the Midfollicular and Midluteal Phases of the Menstrual Cycle. Int. J. Sport Nutr. 1994, 4, 299–308. [Google Scholar] [CrossRef]
- Tarnopolsky, M.A.; Atkinson, S.A.; Phillips, S.M.; MacDougall, J.D. Carbohydrate Loading and Metabolism during Exercise in Men and Women. J. Appl. Physiol. 1995, 78, 1360–1368. [Google Scholar] [CrossRef] [PubMed]
- Horton, T.J.; Pagliassotti, M.J.; Hobbs, K.; Hill, J.O. Fuel Metabolism in Men and Women during and after Long-Duration Exercise. J. Appl. Physiol. 1998, 85, 1823–1832. [Google Scholar] [CrossRef]
- Hackney, A.C. Influence of Oestrogen on Muscle Glycogen Utilization during Exercise. Acta Physiol. Scand. 1999, 167, 273–274. [Google Scholar] [CrossRef]
- Carter, S.L.; Rennie, C.; Tarnopolsky, M.A. Substrate Utilization during Endurance Exercise in Men and Women after Endurance Training. Am. J. Physiol. Endocrinol. Metab. 2001, 280, 898–907. [Google Scholar] [CrossRef]
- Zderic, T.W.; Coggan, A.R.; Ruby, B.C. Glucose Kinetics and Substrate Oxidation during Exercise in the Follicular and Luteal Phases. J. Appl. Physiol. 2001, 90, 447–453. [Google Scholar] [CrossRef]
- Devries, M.C.; Hamadeh, M.J.; Phillips, S.M.; Tarnopolsky, M.A. Menstrual Cycle Phase and Sex Influence Muscle Glycogen Utilization and Glucose Turnover during Moderate-Intensity Endurance Exercise. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2006, 291, 1120–1128. [Google Scholar] [CrossRef]
- Stannard, S.R.; Buckley, A.J.; Edge, J.A.; Thompson, M.W. Adaptations to Skeletal Muscle with Endurance Exercise Training in the Acutely Fed versus Overnight-Fasted State. J. Sci. Med. Sport 2010, 13, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Miotto, P.M.; McGlory, C.; Holloway, T.M.; Phillips, S.M.; Holloway, G.P. Sex Differences in Mitochondrial Respiratory Function in Human Skeletal Muscle. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2018, 314, R909–R915. [Google Scholar] [CrossRef] [PubMed]
- Fink, J.S. Female Athletes, Women’s Sport, and the Sport Media Commercial Complex: Have We Really “Come a Long Way, Baby”? Sport Manag. Rev. 2015, 18, 331–342. [Google Scholar] [CrossRef]
- Schaumberg, M.A.; Jenkins, D.G.; Janse de Jonge, X.A.K.; Emmerton, L.M.; Skinner, T.L. Three-Step Method for Menstrual and Oral Contraceptive Cycle Verification. J. Sci. Med. Sport 2017, 20, 965–969. [Google Scholar] [CrossRef]
- Ansdell, P.; Thomas, K.; Hicks, K.M.; Hunter, S.K.; Howatson, G.; Goodall, S. Physiological Sex Differences Affect the Integrative Response to Exercise: Acute and Chronic Implications. Exp. Physiol. 2020, 105, 2007–2021. [Google Scholar] [CrossRef] [PubMed]
- Oydanich, M.; Babici, D.; Zhang, J.; Rynecki, N.; Vatner, D.E.; Vatner, S.F. Mechanisms of Sex Differences in Exercise Capacity. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2019, 316, R832–R838. [Google Scholar] [CrossRef] [PubMed]
- Sims, S.T.; Ware, L.; Capodilupo, E.R. Patterns of Endogenous and Exogenous Ovarian Hormone Modulation on Recovery Metrics across the Menstrual Cycle. BMJ Open Sport Exerc. Med. 2021, 7, e001047. [Google Scholar] [CrossRef]
- Fehring, R.J.; Schneider, M.; Raviele, K. Variability in the Phases of the Menstrual Cycle. JOGNN—J. Obstet. Gynecol. Neonatal Nurs. 2006, 35, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Bruinvels, G.; Hackney, A.C.; Pedlar, C.R. Menstrual Cycle: The Importance of Both the Phases and the Transitions Between Phases on Training and Performance. Sports Med. 2022, 52, 1457–1460. [Google Scholar] [CrossRef] [PubMed]
- Bruinvels, G.; Goldsmith, E.; Blagrove, R.; Simpkin, A.; Lewis, N.; Morton, K.; Suppiah, A.; Rogers, J.P.; Ackerman, K.E.; Newell, J.; et al. Prevalence and Frequency of Menstrual Cycle Symptoms Are Associated with Availability to Train and Compete: A Study of 6812 Exercising Women Recruited Using the Strava Exercise App. Br. J. Sports Med. 2021, 55, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, T.K.; Braunstein, G.D. Physiological Effects of Androgens in Women. In Androgen Excess Disorders in Women; Humana Press: Totowa, NJ, USA, 2007; pp. 49–62. [Google Scholar]
- Farage, M.A.; Neill, S.; MacLean, A.B. Physiological Changes Associated with the Menstrual Cycle a Review. Obstet. Gynecol. Surv. 2009, 64, 58–72. [Google Scholar] [CrossRef]
- Gimunová, M.; Paulínyová, A.; Bernaciková, M.; Paludo, A.C. The Prevalence of Menstrual Cycle Disorders in Female Athletes from Different Sports Disciplines: A Rapid Review. Int. J. Environ. Res. Public Health 2022, 19, 14243. [Google Scholar] [CrossRef]
- de Jonge, X.J.; Thompson, B.; Ahreum, H.A.N. Methodological Recommendations for Menstrual Cycle Research in Sports and Exercise. Med. Sci. Sports Exerc. 2019, 51, 2610–2617. [Google Scholar] [CrossRef]
- Kendrick, Z.V.; Ellis, G.S. Effect of Estradiol on Tissue Glycogen Metabolism and Lipid Availability in Exercised Male Rats. J. Appl. Physiol. 1991, 71, 1694–1699. [Google Scholar] [CrossRef]
- Devries, M.C. Sex-Based Differences in Endurance Exercise Muscle Metabolism: Impact on Exercise and Nutritional Strategies to Optimize Health and Performance in Women. Exp. Physiol. 2016, 101, 243–249. [Google Scholar] [CrossRef]
- Campbell, S.E.; Angus, D.J.; Febbraio, M.A. Glucose Kinetics and Exercise Performance during Phases of the Menstrual Cycle: Effect of Glucose Ingestion. Am. J. Physiol. Endocrinol. Metab. 2001, 281, 817–825. [Google Scholar] [CrossRef]
- D’Eon, T.M.; Sharoff, C.; Chipkin, S.R.; Grow, D.; Ruby, B.C.; Braun, B. Regulation of Exercise Carbohydrate Metabolism by Estrogen and Progesterone in Women. Am. J. Physiol. Endocrinol. Metab. 2002, 283, 1046–1055. [Google Scholar] [CrossRef]
- Stricker, R.; Eberhart, R.; Chevailler, M.C.; Quinn, F.A.; Bischof, P.; Stricker, R. Establishment of Detailed Reference Values for Luteinizing Hormone, Follicle Stimulating Hormone, Estradiol, and Progesterone during Different Phases of the Menstrual Cycle on the Abbott ARCHITECT® Analyzer. Clin. Chem. Lab. Med. 2006, 44, 883–887. [Google Scholar] [CrossRef]
- Casazza, G.A.; Jacobs, K.A.; Suh, S.H.; Miller, B.F.; Horning, M.A.; Brooks, G.A. Menstrual Cycle Phase and Oral Contraceptive Effects on Triglyceride Mobilization during Exercise. J. Appl. Physiol. 2004, 97, 302–309. [Google Scholar] [CrossRef]
- Suh, S.H.; Casazza, G.A.; Horning, M.A.; Miller, B.F.; Brooks, G.A. Luteal and Follicular Glucose Fluxes during Rest and Exercise in 3-h Postabsorptive Women. J. Appl. Physiol. 2002, 93, 42–50. [Google Scholar] [CrossRef]
- Boisseau, N.; Isacco, L. Substrate Metabolism during Exercise: Sexual Dimorphism and Women’s Specificities. Eur. J. Sport Sci. 2022, 22, 672–683. [Google Scholar] [CrossRef] [PubMed]
- Wenner, M.M.; Stachenfeld, N.S. Sex Hormones and Environmental Factors Affecting Exercise. In Sex Hormones, Exercise and Women: Scientific and Clinical Aspects; Springer International Publishing: Berlin/Heidelberg, Germany, 2016; pp. 151–170. ISBN 9783319445588. [Google Scholar]
- Stachenfeld, N.S. Sex Hormone Effects on Body Fluid Regulation. Exerc. Sport Sci. Rev. 2008, 36, 152. [Google Scholar] [CrossRef] [PubMed]
- Tollan, A.; Kvenild, K.; Strand, H.; Øian, P.; Maltau, J.M. Increased Capillary Permeability for Plasma Proteins in Oral Contraceptive Users. Contraception 1992, 45, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Øian, P.; Tollan, A.; Fadnes, H.O.; Noddeland, H.; Maltau, J.M. Transcapillary Fluid Dynamics during the Menstrual Cycle. Am. J. Obstet. Gynecol. 1987, 156, 952–955. [Google Scholar] [CrossRef]
- Steinach, M.; Lichti, J.; Maggioni, M.A.; Fähling, M. A Fluid Shift for Endurance Exercise-Why Hydration Matters. Acta Physiol. 2019, 227, e13347. [Google Scholar] [CrossRef]
- Stachenfeld, N.S.; Keefe, D.L. Estrogen Effects on Osmotic Regulation of AVP and Fluid Balance. Am. J. Physiol. Endocrinol. Metab. 2002, 283, E711–E721. [Google Scholar] [CrossRef]
- McCracken, M.; Ainsworth, B.; Hackney, A.C. Effects of the Menstrual Cycle Phase on the Blood Lactate Responses to Exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1994, 69, 174–175. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Giustiniani, P.; Rodriguez-Sanchez, N.; Galloway, S.D.R. Fluid and Electrolyte Balance Considerations for Female Athletes. Eur. J. Sport Sci. 2021, 22, 697–708. [Google Scholar] [CrossRef]
- Sims, S.T.; Rehrer, N.J.; Bell, M.L.; Cotter, J.D. Preexercise Sodium Loading Aids Fluid Balance and Endurance for Women Exercising in the Heat. J. Appl. Physiol. 2007, 103, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Darwish, A.; Lui, F. Physiology, Colloid Osmotic Pressure. In StatPearls; StatPearls Publishing: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Retzlaff, J.A.; Tauxe, W.N.; Kiely, J.M.; Stroebel, C.F. Erythrocyte Volume, Plasma Volume, and Lean Body Mass in Adult Men and Women. Blood 1969, 33, 649–667. [Google Scholar] [CrossRef] [PubMed]
- Cable, N.T.; Elliott, K.J. The Influence of Reproductive Hormones on Muscle Strength. Biol. Rhythm Res. 2010, 35, 235–244. [Google Scholar] [CrossRef]
- McNulty, K.L.; Elliott-Sale, K.J.; Dolan, E.; Swinton, P.A.; Ansdell, P.; Goodall, S.; Thomas, K.; Hicks, K.M. The Effects of Menstrual Cycle Phase on Exercise Performance in Eumenorrheic Women: A Systematic Review and Meta-Analysis. Sports Med. 2020, 50, 1813–1827. [Google Scholar] [CrossRef]
- Bull, J.R.; Rowland, S.P.; Scherwitzl, E.B.; Scherwitzl, R.; Danielsson, K.G.; Harper, J. Real-World Menstrual Cycle Characteristics of More than 600,000 Menstrual Cycles. NPJ Digit. Med. 2019, 2, 83. [Google Scholar] [CrossRef]
- Dam, T.V.; Dalgaard, L.B.; Sevdalis, V.; Bibby, B.M.; Janse De Jonge, X.; Gravholt, C.H.; Hansen, M. Muscle Performance during the Menstrual Cycle Correlates with Psychological Well-Being, but Not Fluctuations in Sex Hormones. Med. Sci. Sports Exerc. 2022, 54, 1678–1689. [Google Scholar] [CrossRef]
- De Souza, M.J.; Miller, B.E.; Loucks, A.B.; Luciano, A.A.; Pescatello, L.S.; Campbell, C.G.; Lasley, B.L. High Frequency of Luteal Phase Deficiency and Anovulation in Recreational Women Runners: Blunted Elevation in Follicle-Stimulating Hormone Observed during Luteal-Follicular Transition1. J. Clin. Endocrinol. Metab. 1998, 83, 4220–4232. [Google Scholar] [CrossRef]
- Wideman, L.; Montgomery, M.M.; Levine, B.J.; Beynnon, B.D.; Shultz, S.J. Accuracy of Calendar-Based Methods for Assigning Menstrual Cycle Phase in Women. Sports Health 2013, 5, 143–149. [Google Scholar] [CrossRef]
- Kyei-Mensah, A.; Maconochie, N.; Zaidi, J.; Pittrof, R.; Campbell, S.; Tan, S.L. Transvaginal Three-Dimensional Ultrasound: Reproducibility of Ovarian and Endometrial Volume Measurements. Fertil. Steril. 1996, 66, 718–722. [Google Scholar] [CrossRef]
- Su, H.; Yi, Y.; Wei, T.; Chang, T.; Cheng, C. Detection of Ovulation, a Review of Currently Available Methods. Bioeng. Transl. Med. 2017, 2, 238–246. [Google Scholar] [CrossRef]
- Ecochard, R.; Boehringer, H.; Rabilloud, M.; Marret, H. Chronological Aspects of Ultrasonic, Hormonal, and Other Indirect Indices of Ovulation. BJOG 2001, 108, 822–829. [Google Scholar] [CrossRef]
- Queenan, J.T.; O’Brien, G.D.; Bains, L.M.; Simpson, J.; Collins, W.P.; Campbell, S. Ultrasound Scanning of Ovaries to Detect Ovulation in Women. Fertil. Steril. 1980, 34, 99–105. [Google Scholar] [CrossRef]
- Sruthi Priya, B.; Pushpaja, M.; Siva Kumar, A.V.; Maruthy, K.N. Does the Salivary Fern Pattern Determine Fertile Period in Reproductive Female? Clin. Epidemiol. Glob. Health 2020, 8, 698–701. [Google Scholar] [CrossRef]
- Johnson, S.; Marriott, L.; Zinaman, M. Can Apps and Calendar Methods Predict Ovulation with Accuracy? Curr. Med. Res. Opin. 2018, 34, 1587–1594. [Google Scholar] [CrossRef] [PubMed]
- Barron, M.L.; Fehring, R.J. Basal Body Temperature Assessment: Is It Useful to Couples Seeking Pregnancy? MCN Am. J. Matern./Child Nurs. 2005, 30, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Berglund Scherwitzl, E.; Lindén Hirschberg, A.; Scherwitzl, R. Identification and Prediction of the Fertile Window Using NaturalCycles. Eur. J. Contracept. Reprod. Health Care 2015, 20, 403–408. [Google Scholar] [CrossRef]
- Killick, S.; Elstein, M. Pharmacologic Production of Luteinized Unruptured Follicles by Prostaglandin Synthetase Inhibitors. Fertil. Steril. 1987, 47, 773–777. [Google Scholar] [CrossRef]
- Blake, K.R.; Dixson, B.J.W.; O’Dean, S.M.; Denson, T.F. Standardized Protocols for Characterizing Women’s Fertility: A Data-Driven Approach. Horm. Behav. 2016, 81, 74–83. [Google Scholar] [CrossRef]
- Guida, M.; Tommaselli, G.A.; Palomba, S.; Pellicano, M.; Moccia, G.; Di Carlo, C.; Nappi, C. Efficacy of Methods for Determining Ovulation in a Natural Family Planning Program. Fertil. Steril. 1999, 72, 900–904. [Google Scholar] [CrossRef]
- Najmabadi, S.; Schliep, K.C.; Simonsen, S.E.; Porucznik, C.A.; Egger, M.J.; Stanford, J.B. Cervical Mucus Patterns and the Fertile Window in Women without Known Subfertility: A Pooled Analysis of Three Cohorts. Hum. Reprod. 2021, 36, 1784–1795. [Google Scholar] [CrossRef]
- Rogan, M.M.; Black, K.E. Dietary Energy Intake across the Menstrual Cycle: A Narrative Review. Nutr. Rev. 2023, 81, 869–886. [Google Scholar] [CrossRef]
- Francis, G.; Keay, N. Analysis of the Variability in the Timing of Physiological Events in the Menstrual Cycle. Researchgate 2023, 1–13, in press. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Alignment Days to Phase Method | |||||
|---|---|---|---|---|---|
| Three Phase * | Five Phase ** | Six Phase *** | * | ** | *** |
| Early Follicular | Menstrual | Early Follicular | 2–7 | 1–7 | 1–5 |
| Late Follicular | Follicular | Late Follicular | 9–13 | 8–12 | 6–12 |
| Ovulation | Ovulation | 13–16 | 13–15 | ||
| Early Luteal | 16–19 | ||||
| Mid Luteal | Luteal | Mid Luteal | 18–24 | 17–21 | 20–23 |
| Pre-Menstrual | Late Luteal | 22–28 | 24–28 | ||
| Method | Verifies | Data Collected | Process | Accuracy | Limitations | Benefits |
|---|---|---|---|---|---|---|
| Point of Ovulation | ||||||
| Cervical Mucus | Point of ovulation | changes in vaginal mucus consistency | physical inspection of fluids | 48–76% moderate | wide range of accuracy | low cost, no expertise required, may benefit from pairing with BBT |
| Counting Days | Point of ovulation | start and end of mense | record keeping, estimation | low to moderate 18–59% | excludes anovulatory cycles, human error in recall | free, convenient access, benefits from pairing with additional methods |
| Menstrual Cycle Tracking Apps | Point of ovulation | start and end of mense | record keeping, predictive algorithm | low 21% | no secondary verification used for markers of ovulation | free, convenient access, may benefit from pairing with additional methods |
| Ultrasonography | Point of ovulation | tracks growth of follicles in ovary | transvaginal ultrasound | high 80% (gold standard) | 5–6 scans over 3–8 days, expensive, high level of expertise required, costly equipment | high level of accuracy |
| Basal Body Temperature | End of ovulation/start of LUT phase | changes in resting body temperature | daily recording of oral, vaginal or rectal body temperature | low 22% | low accuracy in detecting ovulation window | low cost, may benefit from pairing with additional methods |
| Salivary Ferning | Point of ovulation | saliva | viewing of crystalized saliva patterns | moderate 42–53% | requires equipment, moderate accuracy | low cost may benefit from pairing with additional methods |
| Urinary Luteinizing Hormone | Point of ovulation | LH levels from urine | urine applied to test strips | high 80% based on 100% correlation with Ultrasonography | excludes LUT deficiency disorders, false positives | low cost, convenient, no technical expertise, reliably with high accuracy |
| Hormone | ||||||
| Serum Progesterone | hormone level | serum Progesterone | blood draw | high 89% (gold standard) | cost, expertise, infection risk in field | high accuracy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dole, A.; Beaven, M.; Sims, S.T. Menstrual Cycle Tracking in Sports Research: Challenges, Progress, and Future Directions. Physiologia 2023, 3, 598-610. https://doi.org/10.3390/physiologia3040044
Dole A, Beaven M, Sims ST. Menstrual Cycle Tracking in Sports Research: Challenges, Progress, and Future Directions. Physiologia. 2023; 3(4):598-610. https://doi.org/10.3390/physiologia3040044
Chicago/Turabian StyleDole, Andrew, Martyn Beaven, and Stacy T. Sims. 2023. "Menstrual Cycle Tracking in Sports Research: Challenges, Progress, and Future Directions" Physiologia 3, no. 4: 598-610. https://doi.org/10.3390/physiologia3040044
APA StyleDole, A., Beaven, M., & Sims, S. T. (2023). Menstrual Cycle Tracking in Sports Research: Challenges, Progress, and Future Directions. Physiologia, 3(4), 598-610. https://doi.org/10.3390/physiologia3040044