
Fluid Replacement Strategies and Heart Rate Variability Recovery Following Prolonged Exercise in the Heat and Mild Dehydration

 , , , ,
, , , , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.2.1. Participants
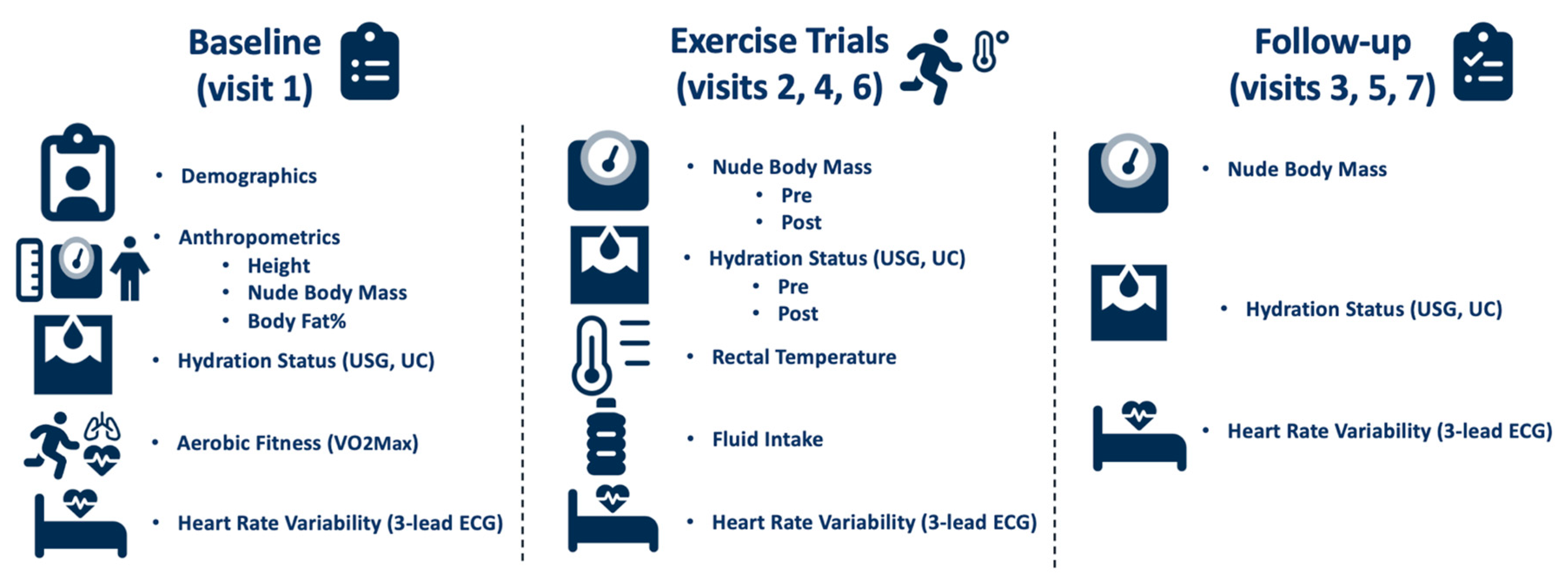
2.2.2. Baseline and Familiarization (Visit 1)
2.2.3. Exercise Trials (Visits 2, 4, and 6)
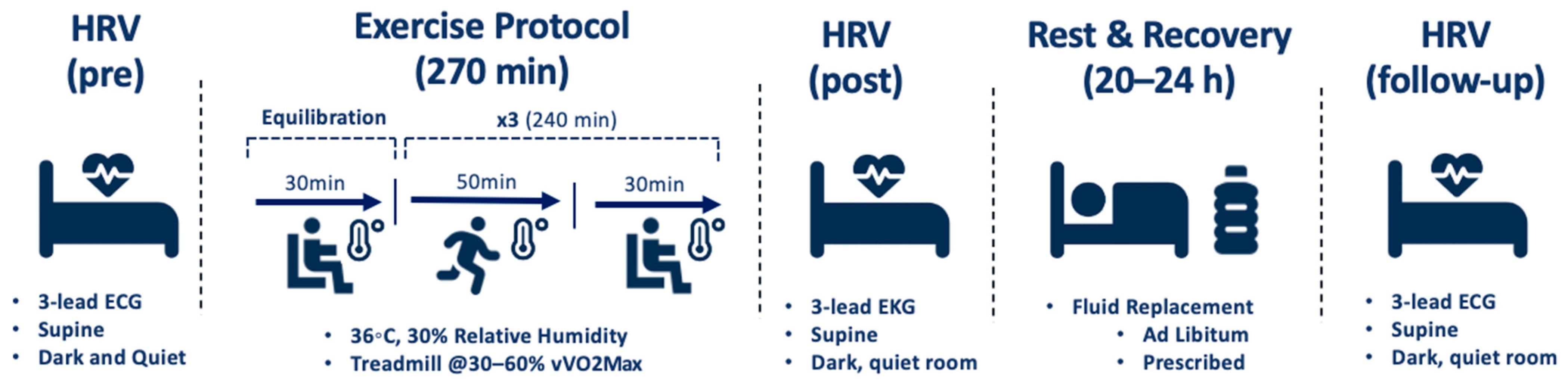
2.2.4. Exercise Protocol
2.2.5. Fluid Replacement Strategies
2.2.6. Follow-Up Visits (Visits 3, 5, and 7)
2.2.7. Measurements
3. Statistical Analyses
4. Results
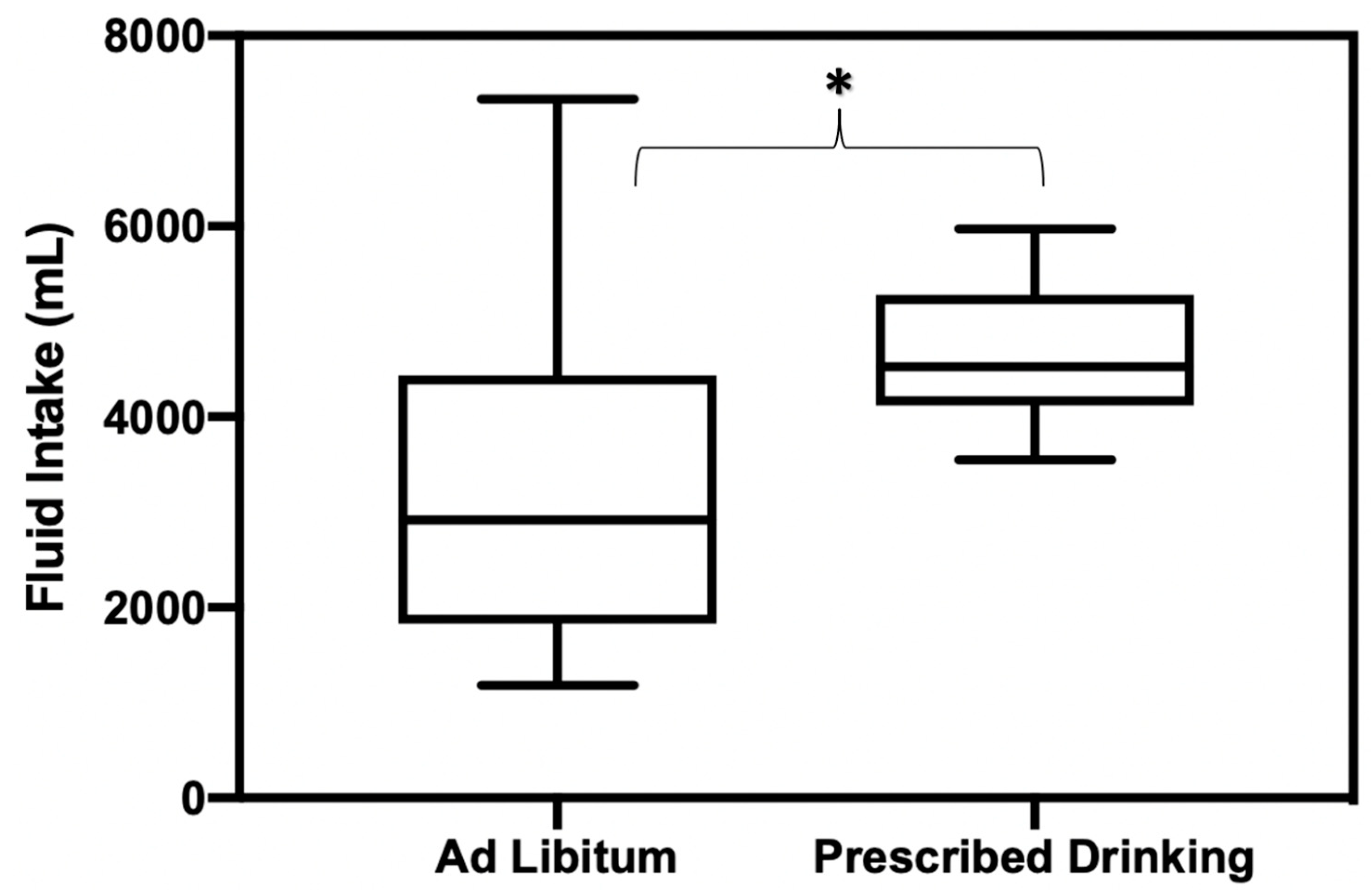
4.1. Fluid Replacement Protocol
4.2. Body Mass Loss and Hydration Status
4.3. Physiological and Behavioral Variables
4.4. HRV Time Domains
4.4.1. RMSSD
4.4.2. pNN50
4.5. HRV Frequency Domains
4.5.1. Low Frequency
4.5.2. High Frequency
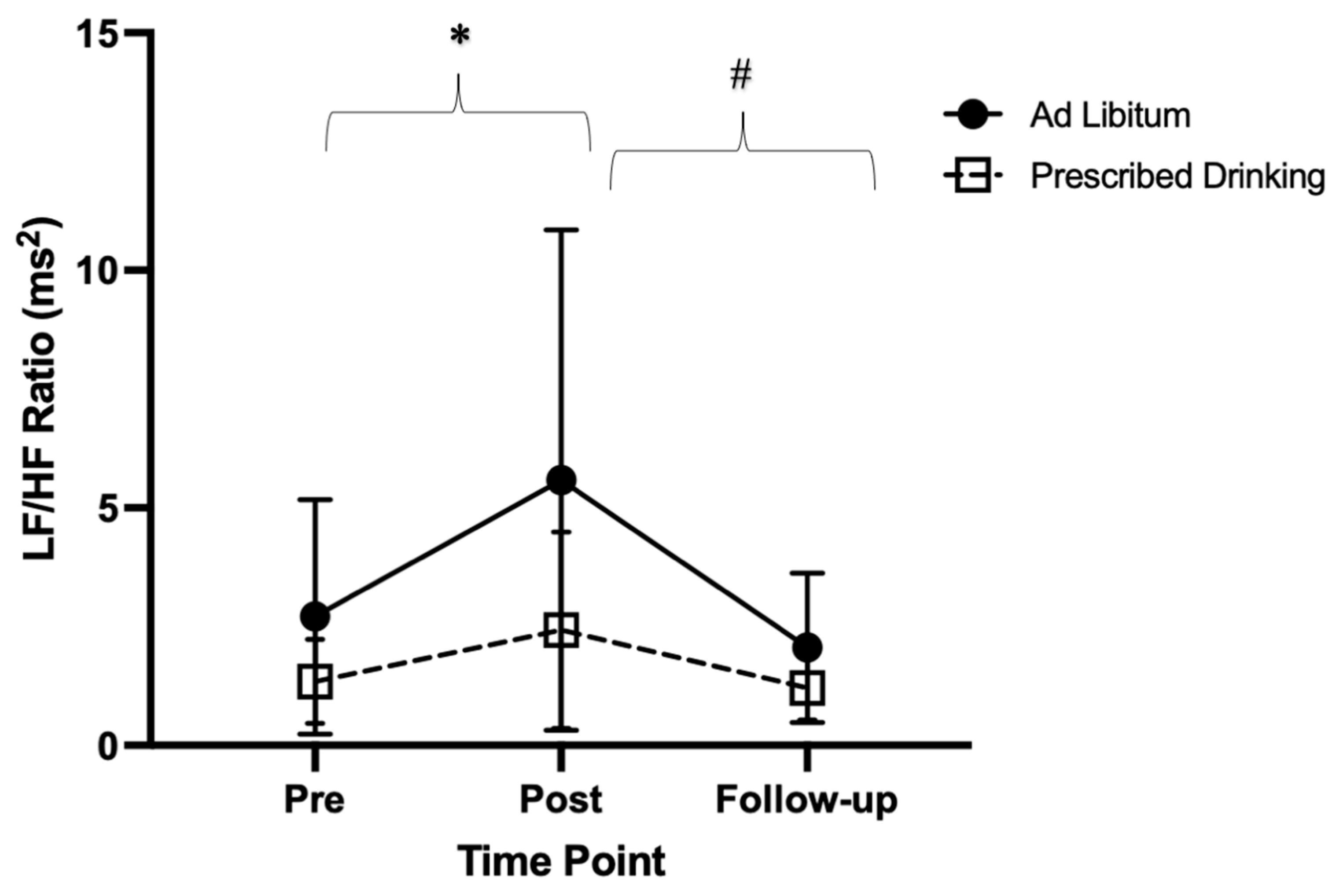
4.5.3. Low Frequency: High Frequency Ratio
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kenny, G.P.; Journeay, W.S. Human thermoregulation: Separating thermal and nonthermal effects on heat loss. Front. Biosci. 2010, 15, 259–290. [Google Scholar] [CrossRef] [PubMed]
- Flouris, A.D.; Schlader, Z.J. Human behavioral thermoregulation during exercise in the heat. Scand. J. Med. Sci. Sport. 2015, 25, 52–64. [Google Scholar] [CrossRef] [PubMed]
- Carter, R.; Cheuvront, S.N.; Wray, D.W.; Kolka, M.A.; Stephenson, L.A.; Sawka, M.N. The influence of hydration status on heart rate variability after exercise heat stress. J. Therm. Biol. 2005, 30, 495–502. [Google Scholar] [CrossRef]
- Macartney, M.J.; Meade, R.D.; Notley, S.R.; Herry, C.L.; Seely, A.J.E.; Kenny, G.P. Fluid Loss during Exercise-Heat Stress Reduces Cardiac Vagal Autonomic Modulation. Med. Sci. Sport. Exerc. 2020, 52, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Convertino, V.A.; Armstrong, L.E.; Edward, C.F.; Mack, G.W.; Sawaka, M.N.; Senay, L.C.; Scherman, M. Exercise and Fluid Replacement. Medicine & Science in Sports & Exercise. Available online: https://www.researchgate.net/profile/Michael_Sawka/publication/13917600_Exercise_and_fluid_replacement_Position_stand_American_College_of_Sports_Medicine/links/558a8ad808aee1fc9174f2f1.pdf (accessed on 20 August 2020).
- Casa, D.J.; Csillan, D.; Armstrong, L.E.; Baker, L.B.; Bergeron, M.F.; Buchanan, V.M.; Carroll, M.J.; Cleary, M.A.; Eichner, E.R.; Ferrara, M.S.; et al. Preseason Heat-Acclimatization Guidelines for Secondary School Athletics. J. Athl. Train. 2009, 44, 332–333. [Google Scholar] [CrossRef] [PubMed]
- Casa, D.J. Sport and Physical Activity in the Heat: Maximizing Performance and Safety; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Brenner, I.K.M.; Thomas, S.; Shephard, R.J. Spectral analysis of heart rate variability during heat exposure and repeated exercise. Eur. J. Appl. Physiol. 1997, 76, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Pryor, R.; Pryor, J.L.; Vandermark, L.W.; Adams, E.L.; Brodeur, R.M.; Armstrong, L.E.; Lee, E.C.; Maresh, C.M.; Anderson, J.M.; Casa, D.J. Exacerbated heat strain during consecutive days of repeated exercise sessions in heat. J. Sci. Med. Sport 2019, 22, 1084–1089. [Google Scholar] [CrossRef]
- Macartney, M.J.; Notley, S.R.; Meade, R.D.; Herry, C.L.; Kenny, G.P. Heart rate variability in older men on the day following prolonged work in the heat. J. Occup. Environ. Hyg. 2020, 17, 383–389. [Google Scholar] [CrossRef]
- Schlader, Z.J.; Colburn, D.; Hostler, D. Heat Strain Is Exacerbated on the Second of Consecutive Days of Fire Suppression. Med. Sci. Sport. Exerc. 2017, 49, 999–1005. [Google Scholar] [CrossRef]
- Michael, S.; Graham, K.S.; Davis, G.M.O. Cardiac Autonomic Responses during Exercise and Post-exercise Recovery Using Heart Rate Variability and Systolic Time Intervals—A Review. Front. Physiol. 2017, 8, 301. [Google Scholar] [CrossRef]
- Abellán-Aynés, O.; López-Plaza, D.; Alacid, F.; Naranjo-Orellana, J.; Manonelles, P. Recovery of Heart Rate Variability After Exercise Under Hot Conditions: The Effect of Relative Humidity. Wilderness Environ. Med. 2019, 30, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Kaltsatou, A.; Flouris, A.D.; Herry, C.L.; Notley, S.R.; Macartney, M.J.; Seely, A.J.E.; Kenny, G.P.; E Seely, A.J. Heart rate variability in older workers during work under the Threshold Limit Values for heat exposure. Am. J. Ind. Med. 2020, 63, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, R.G.; Ahmad, S.; Seely, A.J.; Kenny, G.P. Heart rate variability and baroreceptor sensitivity following exercise-induced hyperthermia in endurance trained men. Eur. J. Appl. Physiol. 2012, 112, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Papelier, Y.; Laursen, P.B.; Ahmaidi, S. Noninvasive assessment of cardiac parasympathetic function: Postexercise heart rate recovery or heart rate variability? Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H8–H10. [Google Scholar] [CrossRef] [PubMed]
- Flouris, A.D.; Friesen, B.J.; Herry, C.L.; Seely, A.J.E.; Notley, S.R.; Kenny, G.P. Heart rate variability dynamics during treatment for exertional heat strain when immediate response is not possible. Exp. Physiol. 2019, 104, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Stacey, M.M.J.; Delves, S.K.; Woods, D.R.; Britland, S.E.; Macconnachie, L.; Allsopp, A.J.; Brett, S.J.; Fallowfield, J.L.; Boos, C.J. Heart rate variability and plasma nephrines in the evaluation of heat acclimatisation status. Eur. J. Appl. Physiol. 2018, 118, 165–174. [Google Scholar] [CrossRef]
- García Iglesias, D.; Roqueñi Gutiérrez, N.; De Cos, F.J.; Calvo, D. Analysis of the High-Frequency Content in Human QRS Complexes by the Continuous Wavelet Transform: An Automatized Analysis for the Prediction of Sudden Cardiac Death. Sensors 2018, 18, 560. [Google Scholar] [CrossRef]
- Ebrahimzadeh, E.; Pooyan, M.; Bijar, A. A Novel Approach to Predict Sudden Cardiac Death (SCD) Using Nonlinear and Time-Frequency Analyses from HRV Signals. PLoS ONE 2014, 9, e81896. [Google Scholar] [CrossRef]
- Laurent, C.M.; Green, J.M.; A Bishop, P.; Sjökvist, J.; E Schumacker, R.; Richardson, M.T.; Curtner-Smith, M. A Practical Approach to Monitoring Recovery: Development of a Perceived Recovery Status Scale. J. Strength Cond. Res. 2011, 25, 620–628. [Google Scholar] [CrossRef]
- Harmon Kimberly, G.; Asif Irfan, M.; Maleszewski Joseph, J.; Owens, D.; Prutkin, J.; Salerno, J.; Zigman, M.; Ellenbogen, R.; Rao, A.; Ackerman, M.; et al. Incidence, Cause, and Comparative Frequency of Sudden Cardiac Death in National Collegiate Athletic Association Athletes. Circulation 2015, 132, 10–19. [Google Scholar] [CrossRef]
- Adams, W.M.; Hosokawa, Y.; Casa, D.J. Body-Cooling Paradigm in Sport: Maximizing Safety and Performance During Competition. J. Sport Rehabil. 2016, 25, 382–394. [Google Scholar] [CrossRef] [PubMed]
- McDermott, B.P.; Anderson, S.A.; Armstrong, L.E.; Casa, D.J.; Cheuvront, S.N.; Cooper, L.; Kenney, W.L.; O’Connor, F.G.; Roberts, W.O. National Athletic Trainers’ Association Position Statement: Fluid Replacement for the Physically Active. J Athl. Train. 2017, 52, 877–895. [Google Scholar] [CrossRef] [PubMed]
- Casa, D.J.; Guskiewicz, K.M.; Anderson, S.A.; Courson, R.W.; Heck, J.F.; Jimenez, C.C.; McDermott, B.P.; Miller, M.G.; Stearns, R.L.; Swartz, E.E.; et al. National Athletic Trainers’ Association Position Statement: Preventing Sudden Death in Sports. J. Athl. Train. 2012, 47, 96–118. [Google Scholar] [CrossRef] [PubMed]
- Casa, D.J.; Curtis, R.M.; Stearns, R.L. Heart rate variability offers additional applications in heat-stressed. Exp. Physiol. 2019, 104, 991–992. [Google Scholar] [CrossRef] [PubMed]
- Casa, D.J.; Almquist, J.; Anderson, S.A.; Baker, L.; Bergeron, M.F.; Biagioli, B.; Boden, B.; Brenner, J.S.; Carroll, M.; Colgate, B.; et al. The Inter-Association Task Force for Preventing Sudden Death in Secondary School Athletics Programs: Best-Practices Recommendations. J. Athl. Train. 2013, 48, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Hostler, D.; Bednez, J.C.; Kerin, S.; Reis, S.; Kong, P.W.; Morley, J.; Gallagher, M., Jr.; Suyama, J. Comparison of Rehydration Regimens for Rehabilitation of Firefighters Performing Heavy Exercise in Thermal Protective Clothing: A Report from the Fireground Rehab Evaluation (FIRE) Trial. Prehospital Emerg. Care 2010, 14, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Langan, S.P.; Manning, C.N.; Morrissey, M.C.; Gulati, T.; Laxminarayan, S.; Reifman, J.; Casa, D.J. Efficacy of two intermittent cooling strategies during prolonged work-rest intervals in the heat with personal protective gear compared with a control condition. Eur. J. Appl. Physiol. 2023, 1–10. [Google Scholar] [CrossRef]
- Miller, K.C.; Hughes, L.E.; Long, B.C.; Adams, W.M.; Casa, D.J. Validity of Core Temperature Measurements at 3 Rectal Depths During Rest, Exercise, Cold-Water Immersion, and Recovery. J. Athl. Train. 2017, 52, 332–338. [Google Scholar] [CrossRef]
- Hernando, D.; Garatachea, N.; Almeida, R.; Casajús, J.A.; Bailón, R. Validation of Heart Rate Monitor Polar RS800 for Heart Rate Variability Analysis During Exercise. J. Strength Cond. Res. 2018, 32, 716–725. [Google Scholar] [CrossRef]
- Georgiou, K.; Larentzakis, A.V.; Khamis, N.N.; Alsuhaibani, G.I.; Alaska, Y.A.; Giallafos, E.J. Can Wearable Devices Accurately Measure Heart Rate Variability? A Systematic Review. Folia Med. 2018, 60, 7–20. [Google Scholar] [CrossRef]
- Manual | BIOPAC. BIOPAC Systems, Inc. Available online: https://www.biopac.com/manual/ (accessed on 22 January 2021).
- Frontiers | HRVanalysis: A Free Software for Analyzing Cardiac Autonomic Activity | Physiology. Available online: https://www.frontiersin.org/articles/10.3389/fphys.2016.00557/full (accessed on 5 March 2021).
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- About—Jamovi. Available online: https://www.jamovi.org/about.html (accessed on 16 January 2021).
- Early, K.S.; Earnest, C.P.; Theall, B.; Lemoine, N.P.; Harrell, B.; Johannsen, N.M. Free-living, continuous hypo-hydration, and cardiovascular response to exercise in a heated environment. Physiol. Rep. 2018, 6, e13672. [Google Scholar] [CrossRef] [PubMed]
- Nolte, H.W.; Noakes, T.D.; Nolte, K. Ad Libitum vs. Restricted Fluid Replacement on Hydration and Performance of Military Tasks. Aviat. Space Environ. Med. 2013, 84, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Lopez, R.; Casa, D.J.; Jensen, K.A.; Stearns, R.L.; DeMartini, J.K.; Pagnotta, K.D.; Roti, M.W.; Armstrong, L.E.; Maresh, C.M. Comparison of Two Fluid Replacement Protocols During a 20-km Trail Running Race in the Heat. J. Strength Cond. Res. 2016, 30, 2609–2616. [Google Scholar] [CrossRef]
- Lopez, R.M.; Casa, D.J.; A Jensen, K.; DeMartini, J.K.; Pagnotta, K.D.; Ruiz, R.C.; Roti, M.W.; Stearns, R.L.; E Armstrong, L.; Maresh, C.M. Examining the Influence of Hydration Status on Physiological Responses and Running Speed During Trail Running in the Heat With Controlled Exercise Intensity. J. Strength Cond. Res. 2011, 25, 2944–2954. [Google Scholar] [CrossRef]
- Casa, D.J.; Armstrong, L.E.; Hillman, S.K.; Montain, S.J.; Reiff, R.V.; Rich, B.S.E.; Roberts, W.O.; Stone, J.A. National Athletic Trainers’ Association Position Statement: Fluid Replacement for Athletes. J. Athl. Train. 2000, 35, 212–224. [Google Scholar]
- Convertino, V.A.; Armstrong, L.E.; Coyle, E.F.; Mack, G.W.; Sawka, M.N.; Senay, L.C.; Sherman, W.M. ACSM Position Stand: Exercise and Fluid Replacement. Med. Sci. Sports Exerc. 1996, 28, 1–9. [Google Scholar] [CrossRef]
- Adams, W.M. Rehydration on Subsequent Performance and Recovery Following Exercise-Induced Dehydration: Ad Libitum Versus Prescribed Fluid Replacement. Ph.D. Thesis, University of Connecticut, Stamford, CT, USA, 2016; p. 109. [Google Scholar]
- Yamamoto, Y.; Hughson, R.L.; Peterson, J.C. Autonomic control of heart rate during exercise studied by heart rate variability spectral analysis. J. Appl. Physiol. 1991, 71, 1136–1142. [Google Scholar] [CrossRef]
- Bernardi, L.; Passino, C.; Robergs, R.; Appenzeller, O. Acute and persistent effects of a 46-kilometre wilderness trail run at altitude: Cardiovascular autonomic modulation and baroreflexes. Cardiovasc. Res. 1997, 34, 273–280. [Google Scholar] [CrossRef]
- Evidence for an Intrinsic Mechanism Regulating Heart Rate Variability in the Transplanted and the Intact Heart During Submaximal Dynamic Exercise? | Cardiovascular Research | Oxford Academic. Available online: https://academic.oup.com/cardiovascres/article/24/12/969/493866?login=true (accessed on 4 March 2021).
- Perini, R.; Veicsteinas, A. Heart rate variability and autonomic activity at rest and during exercise in various physiological conditions. Eur. J. Appl. Physiol. 2003, 90, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Rimoldi, O.; Furlan, R.; Pagani, M.R.; Piazza, S.; Guazzi, M.; Pagani, M.; Malliani, A. Analysis of Neural Mechanisms Accompanying Different Intensities of Dynamic Exercise. Chest 1992, 101 (Suppl. 5), 226S–230S. [Google Scholar] [CrossRef] [PubMed]
- González-Alonso, J. Separate and Combined Influences of Dehydration and Hyperthermia on Cardiovascular Responses to Exercise. Int. J. Sports Med. 1998, 19 (Suppl. 2), S111–S114. [Google Scholar] [CrossRef] [PubMed]
- Charkoudian, N.; Halliwill, J.R.; Morgan, B.J.; Eisenach, J.H.; Joyner, M.J. Influences of hydration on post-exercise cardiovascular control in humans. J. Physiol. 2003, 552, 635–644. [Google Scholar] [CrossRef] [PubMed]
- Binkley, H.M.; Beckett, J.; Casa, D.J.; Kleiner, D.M.; Plummer, P.E. National Athletic Trainers’ Association Position Statement: Exertional Heat Illnesses. J. Athl. Train. 2002, 37, 329–343. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ad Libitum (n = 6) | Prescribed Drinking (n = 6) | Overall (n = 12) | |
|---|---|---|---|
| Age (years) | 27 ± 5 | 25 ± 5 | 26 ± 5 |
| VO2max (mL/kg/min) | 58.93 ± 7.61 | 57.95 ± 7.14 | 58.44 ± 7.05 |
| Velocity at VO2max (vVO2) (mph) | 9.42 ± 0.92 | 9.25 ± 0.94 | 9.33 ± 0.89 |
| Stature (cm) | 179.75 ± 4.92 | 186.50 ± 7.97 | 183.13 ± 7.23 |
| Body Mass (kg) | 75.99 ± 4.67 | 80.61 ± 10.40 | 78.30 ± 8.06 |
| Body Fat (%) | 11.35 ± 1.91 | 8.13 ± 1.76 | 9.74 ± 2.43 |
| a | ||
| Prescribed Drinking | Ad Libitum | |
| AVG Trec (°C) | 38.02 ± 0.32 | 37.97 ± 0.30 |
| Peak Trec (°C) | 38.92 ± 0.46 | 38.77 ± 0.42 |
| AVG HR (bpm) | 136 ± 10 | 136 ± 13 |
| Peak HR (bpm) | 175 ± 8 | 172 ± 12 |
| Nude Body Mass (kg) (pre-trial) | 81.60 ± 9.47 | 78.43 ± 3.60 |
| Nude Body Mass (kg) (post-trial) | 79.00 ± 9.16 | 76.27 ± 2.51 |
| BML (%) | 2.78 ± 1.00 | 2.97 ± 1.36 |
| Fluid Intake (L) | 1.7 ± 1.2 | 2.3 ± 1.1 |
| USG (pre-trial) | 1.009 ± 0.007 | 1.010 ± 0.006 |
| UC (pre-trial) | 3 ± 2 | 3 ± 1 |
| USG (post-trial) | 1.020 ± 0.008 | 1.016 ± 0.009 |
| UC (post-trial) | 6 ± 2 | 5 ± 2 |
| b | ||
| Prescribed Drinking | Ad Libitum | |
| HR (bpm) | 55 ± 7 | 50 ± 4 |
| Nude Body Mass (kg) (follow-up) | 80.92 ± 9.38 | 77.62 ± 2.81 |
| BML (%) | 0.83 ± 0.77 | 1.05 ± 1.30 |
| Fluid Intake (L) | 4.6 ± 7.1 * | 3.4 ± 1.9 |
| USG | 1.019 ± 0.010 | 1.015 ± 0.006 |
| UC | 4 ± 2 | 5 ± 2 |
| Ad Libitum | Prescribed Drinking | |||||
|---|---|---|---|---|---|---|
| Pre-Trial | Post-Trial | Follow-Up | Pre-Trial | Post-Trial | Follow-Up | |
| RMSSD (ms2) | 4.17 ± 0.87 | 3.69 ± 0.89 | 4.22 ± 0.54 | 4.59 ± 0.92 | 3.53 ± 0.71 | 4.52 ± 0.50 |
| pNN50 (%) | 30.13 ± 22.95 | 13.20 ± 11.18 | 39.04 ± 20.48 | 47.99 ± 21.70 | 16.46 ± 18.36 | 54.85 ± 20.30 |
| LF (ms2) | 1141.94 ± 803.97 | 1384.87 ± 1178.15 | 1680.14 ± 1277.60 | 13,546.17 ± 48,834.52 | 625.47 ± 617.34 | 2220.77 ± 1517.20 |
| HF (ms2) | 951.53 ± 1026.03 | 471.99 ± 497.52 | 1162.49 ± 984.31 | 8333.46 ± 27,592.16 | 516.58 ± 774.87 | 2414.07 ± 1813.98 |
| LF:HF Ratio (ms2) | 2.71 ± 2.47 | 5.58 ± 5.26 | 2.05 ± 1.57 | 1.34 ± 0.88 | 2.42 ± 2.07 | 1.20 ± 0.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manning, C.N.; Morrissey, M.C.; Langan, S.P.; Stearns, R.L.; Huggins, R.A.; Curtis, R.M.; Sekiguchi, Y.; Laxminarayan, S.; Reifman, J.; Casa, D.J. Fluid Replacement Strategies and Heart Rate Variability Recovery Following Prolonged Exercise in the Heat and Mild Dehydration. Physiologia 2023, 3, 98-112. https://doi.org/10.3390/physiologia3010008
Manning CN, Morrissey MC, Langan SP, Stearns RL, Huggins RA, Curtis RM, Sekiguchi Y, Laxminarayan S, Reifman J, Casa DJ. Fluid Replacement Strategies and Heart Rate Variability Recovery Following Prolonged Exercise in the Heat and Mild Dehydration. Physiologia. 2023; 3(1):98-112. https://doi.org/10.3390/physiologia3010008
Chicago/Turabian StyleManning, Ciara N., Margaret C. Morrissey, Sean P. Langan, Rebecca L. Stearns, Robert A. Huggins, Ryan M. Curtis, Yasuki Sekiguchi, Srinivas Laxminarayan, Jaques Reifman, and Douglas J. Casa. 2023. "Fluid Replacement Strategies and Heart Rate Variability Recovery Following Prolonged Exercise in the Heat and Mild Dehydration" Physiologia 3, no. 1: 98-112. https://doi.org/10.3390/physiologia3010008
APA StyleManning, C. N., Morrissey, M. C., Langan, S. P., Stearns, R. L., Huggins, R. A., Curtis, R. M., Sekiguchi, Y., Laxminarayan, S., Reifman, J., & Casa, D. J. (2023). Fluid Replacement Strategies and Heart Rate Variability Recovery Following Prolonged Exercise in the Heat and Mild Dehydration. Physiologia, 3(1), 98-112. https://doi.org/10.3390/physiologia3010008