Abstract
The aim of this study was to investigate the effect of ingestion of ice slurry before bedtime on the sleep quality of rugby union players in the summer season. Thirteen healthy male university rugby union players volunteered for this study. The participants ingested either ice slurry or a room-temperature beverage (control) 30 min before bedtime. A wearable activity-based sleep monitor was used to analyze objective sleep parameters, and the subjective sleep scores were assessed using the Oguri–Shirakawa–Azumi Sleep Inventory, middle-aged and aged version (OSA-MA). No differences in the amount or efficiency of sleep were observed between the ice slurry/control beverage conditions. Significant shortening of the sleep latency was observed in the ice slurry condition as compared with the control beverage condition. Moreover, significant improvement of the subjective sleep score for “feeling refreshed” on the OSA-MA was observed in the ice slurry condition. There were no significant differences in the other subjective sleep scores between the two conditions. The results suggest that ice slurry ingestion before bedtime may improve the latency of sleep onset, accelerate recovery from fatigue, and be useful as a sleep improvement strategy in rugby union players engaging in exercises during the summer season.
1. Introduction
In order to alleviate the fatigue caused by match-playing and high training loads in athletes, a variety of recovery strategies have been attempted [1]. A number of studies have investigated the effects of various strategies for accelerating the rate of recovery, including sleep [2,3], stretching, active rest, compression garments, and massage [4]. Among these, sleep is considered as being one of the most important post-exercise recovery strategies, but it is known to be influenced by irregular training and environmental factors. For example, it is known that hot environments increase wakefulness and decrease slow-wave and rapid eye movement sleep [5], while early-morning training and late-night matches decrease the sleep quality [6].
Sleep quality (e.g., sleep latency, wake time after sleep onset, and sleep efficiency) is known to be influenced by the circadian rhythm and is reported to be closely correlated with the body temperature [7,8]. Sleep is typically initiated at a time when the body temperature declines rapidly [9]. The core body temperature is higher in the daytime and lower at night, and disturbances in this temperature rhythm are known to worsen the sleep quality [10]. Factors that affect the body temperature rhythm in athletes include nighttime training and games, especially during the summer season. Skein et al. [11] reported that 5 days of training in the heat is associated with a decrease in the sleep quality (sleep latency and wake after sleep onset) in athletes. This result underscores the importance of lowering the core body temperature before sleep to improve the quality of sleep (and obtain good recovery) in athletes. In studies aimed at improving sleep in athletes, immersion in cold water after training has been reported to shorten the sleep latency [12], but not improve the sleep quality [13,14]; therefore, the effects of external cooling on sleep are not clear. On the other hand, internal cooling, e.g., by ingestion of ice slurry, is attracting attention as a method for lowering the core body temperature. Ingestion of ice slurry, which is a mixture of ice and a liquid carrier, has recently attracted attention as a cooling strategy for athletes. Changing the physical state of water from the solid state to the liquid state requires a large transfer of heat energy. Accordingly, ice slurry provides a greater cooling effect than liquid water alone [15,16]. It has been reported that ingestion of 2 to 7.5 g/kg body mass of ice slurry attenuated the rise in the core body temperature during exercise [17,18,19]. However, until date, no studies have examined the effects of ingestion of ice slurry at bedtime on the sleep quality.
As described above, ensuring an adequate duration of sleep is necessary to achieve high performance in athletes [20]. However, in practice, it is difficult to ensure adequate sleep duration due to the heat in the summer and demanding training and game schedules; therefore, recovery strategies, such as improving the sleep quality, are important [21]. In particular, tackle- and collision-based activities, which occur during match play and rugby union training, have a high energy cost and can lead to excessive increase in the core body temperature in hot environments [22,23]. Furthermore, Swinbourne et al. [24] reported that professional rugby players are at risk of poor sleep during preseason training due to physical stress. We investigated the effect of ice slurry ingestion at bedtime on the sleep quality in the summer season in rugby union players, to verify the hypothesis that internal cooling would shorten the sleep latency.
2. Materials and Methods
2.1. Participants
Thirteen healthy male university rugby union players (mean age 19.1 ± 0.9 years; age range, 18–21 years; body mass 84.5 ± 8.4 kg; height 1.71 ± 0.05 m; VO2 max 61.7 ± 4.8 mL/kg/min) belonging to the same team participated in this study. Participants had at least 3 years of rugby union training experience. The average self-reported sleep duration in the previous week was 7.8 ± 0.7 h; the participants had no disorders of sleep or circadian rhythm, and no history of use of medications that could affect sleep or circadian rhythm. The participants were provided a thorough explanation about the risks and benefits of participating in the study, and written informed consent was obtained from each of them prior to the commencement of this study. The participants were randomized by their body mass and allocated to one of two sequences. This study was conducted with the approval of the Ethics Committee of Keio University Graduate School of System Design (approval number: SDM-2020-E017), in accordance with the principles laid down in the latest version of the Declaration of Helsinki.
2.2. Study Design
This study had an open-label, randomized, crossover design, and consisted of two crossover 1 day intervention periods separated by a 14 day washout period (Figure 1). Throughout the study period, the participants were asked to maintain their normal lifestyles, including their physical activity and nutritional habits. For the 16 day study period, the participants were enrolled in a regular fitness conditioning program and field-based rugby union-specific training (total 10 h per week) at their training facility (Kanagawa, Japan); no cup matches or competitions were held during the study period. The participants did not take part in any other structured recovery methods during this period. On the test day and the day before the test day, they were instructed to avoid consuming alcohol, caffeine, nonsteroidal anti-inflammatory drugs, and nutritional supplements. This study was conducted from August to September 2020 (Kanagawa, Japan). The highest temperatures and average relative humidity (RH) on each test day were 34.3 °C and 73% RH and 33.0 °C and 86% RH, respectively. The average highest temperature and RH during the study period were 33.0 ± 2.2 °C and 77.3% ± 4.5%, respectively. The participants underwent field-based rugby union-specific training for 60 min during the daytime on the test day. During the study period, the participants consumed three meals per day (providing a total of approximately 5000 kcal). On the test day, the participants had a typical dinner 5 h before bedtime with a macronutrient composition of approximately 1900 kcal (235.2 g of carbohydrates, 63.1 g of fat, and 77.2 g of protein).
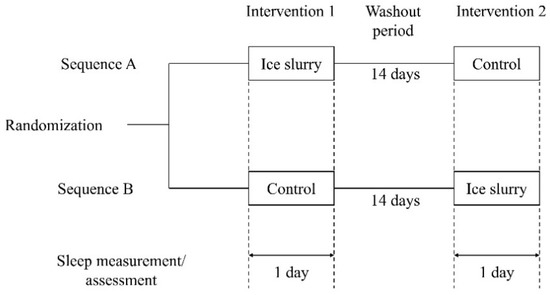
Figure 1.
Overview of the study design.
2.3. Intervention
The participants ingested 2 g/kg body mass of −2 °C ice slurry (ice slurry) or room-temperature beverage (control) 30 min before bedtime. The compositions of the ice slurry and control beverage were the same: 56 kcal/100 g carbohydrate, 94.0 mg/100 g Na, and 20.3 mg/100 g K. The participants ingested the ice slurry or control beverage from aluminum foil-based pouches; for the ice slurry, the pouch was rubbed thoroughly until soft.
2.4. Rating of Perceived Exertion and Total Physical Activity Count
The rating of perceived exertion (RPE) was measured before and after the 60 min field-based rugby union-specific training (exercise). The RPE was measured using a 6–20-point Borg Scale [25]. The total physical activity during exercise was measured using an actigraphy device (MTN-220, Acos Co., Ltd., Nagano, Japan) [26,27]. The MTN-220 is a small and lightweight coin-shaped device (external dimensions: 27 mm in diameter and 10 mm in depth; weight 9 g) that records the amount of physical activity using an internal three-axis accelerometer. The participants fixed the MTN-220 to the front side of their bodies during exercise, by clipping it to the edge of their pants.
2.5. Measurements and Analysis of Objective Sleep Parameters
The sleep measurements were conducted in the participants’ own rooms at the university dormitory with the temperature set to approximately 25 °C from 30 min before bedtime to wake time, using the actigraphy device (MTN-220) [26,27]. The reported agreement rate between the results of sleep/wake states calculated with the MTN-220 and those calculated with polysomnography was 85% [28]. The participants were required to fix the MTN-220 to the front side of their bodies by clipping it to the edge of their pants 30 min before bedtime. Data were collected overnight, extracted from the MTN-220 through an NFC interface (RC-S380, Sony Corporation, Tokyo, Japan) using the SleepSignAct ver. 2.0 software (Kissei Comtec, Nagano, Japan), and analyzed using the algorithm described in a previous study [28]. The objective sleep parameters obtained from the software were the bedtime, wake time, time in bed, total sleep time, sleep latency, wake time after sleep onset, and sleep efficiency. The time in bed was defined as the total time spent lying in bed during the night, total sleep time was defined as the total time classified as sleep during the time in bed, sleep latency was defined as the length of time a participant took to fall asleep, wake time after sleep onset was defined as the total time during which the participant was awake during time in bed, and sleep efficiency was defined as the total sleep time in relation to the time in bed [29].
2.6. Assessment of Subjective Sleep Parameters
Subjective sleep scores were assessed using the Oguri–Shirakawa–Azumi Sleep Inventory, middle-aged and aged version (OSA-MA), at wake up time [30,31]. The OSA-MA is a self-reported questionnaire composed of 16 items, with the response to each of the items graded on a four-point scale. The items are consolidated into five factors: sleepiness on rising, initiation and maintenance of sleep, frequent dreaming, “feeling refreshed (recovery from fatigue)”, and sleep length. The OSA-MA scores were calculated as the corrected (Zc) scores, using a Microsoft Excel sheet provided by the creators of the inventory. The Zc score was created by replacing the mean of the standard score of the population at the time of the intervention with 50 points, with higher scores indicating a better quality of sleep.
2.7. Statistical Analysis
Descriptive data are presented as means ± standard deviation (SD), unless stated otherwise. All statistical analyses were performed using the SAS software package version 9.4 (SAS Institute Japan Ltd., Tokyo, Japan). All data were assessed for normal distribution using the Shapiro–Wilk test. A paired t-test was performed to compare the mean values of the objective and subjective sleep parameters (control vs. ice slurry conditions). Data that were not normally distributed were analyzed by the Wilcoxon signed-rank test. The significance level was set at p < 0.05. Cohen’s d was used to measure the effect size for paired samples [32]. Cohen’s d values between 0.2 and 0.5 were considered as small, values between 0.5 and 0.8 were considered as intermediate, and values greater than 0.8 were considered as high. The sample size was calculated using the software G*Power 3.1 [33], considering the sleep latency in a previous study [8]. To calculate the sample size, the effect size (0.90), two tails, α error probability (0.05), and power (0.8) were considered, and the appropriate sample size was determined to be 12.
3. Results
3.1. Training Status of the Test Day
The RPE and total physical activity during exercise are shown in Table 1. No significant differences between the two conditions were found in the RPE before and after 60 min exercise. Moreover, the total physical activity during exercise was not different between the two conditions.

Table 1.
Rating of perceived exertion and total physical activity during exercise.
3.2. Objective Sleep Parameters
Table 2 shows the values of the activity-based sleep parameters obtained from the MTN-220 data. No significant differences between the two conditions were found in the bedtime, wake time, time in bed, total sleep time, wake time after sleep onset, or sleep efficiency. The sleep latency was significantly shortened in the ice slurry condition as compared with the control condition.
Table 2.
Objective sleep parameters obtained from the MTN-220 data.
3.3. Subjective Sleep Parameters
The mean OSA-MA scores are shown in Table 3. There were no differences between the conditions in the scores for the following factors: “sleepiness upon rising”, “initiation and maintenance of sleep”, “frequent dreaming”, and “sleep length”. The score for “feeling refreshed (recovery from fatigue)” was significantly higher under the ice slurry condition than under the control condition.
Table 3.
Subjective sleep parameters assessed by the OSA-MA.
3.4. Adverse Events
No adverse events associated with ice slurry ingestion were observed during the study period.
4. Discussion
This study is the first to evaluate the effect of ingestion of ice slurry at bedtime on the nighttime sleep quality during the summer season in university rugby union players. Although ingestion of ice slurry 30 min before bedtime did not affect the wake time after sleep onset or sleep efficiency, ice slurry ingestion shortened the sleep latency and improved the subjective OSA-MA score for “feeling refreshed (recovery from fatigue)”. Significant seasonal variations are known to exist in sleep quality parameters such as the sleep latency, sleep efficiency, and wake time after sleep onset, and the sleep quality is known to be often worse in the summer season than in other seasons [34]. One of the reported causes of poor sleep quality in the summer season is the change in body and skin temperature in hot environments [35,36,37]. The time in bed, total sleep time, sleep latency, and wake time after sleep onset, measured as the objective sleep parameters using the MTN-220, were 461.2 ± 65.5 min, 259.5 ± 60.1 min, 72.3 ± 60.2 min, and 117.2 ± 54.0 min, respectively, under the control condition. The sleep efficiency was 56.4% ± 11.4%, indicating that the sleep quality was also poor in the participants of this study; a widely accepted normal range for sleep efficiency is >85% [38]. In addition, the low scores (<50) on OSA-MA, a subjective assessment scale for the sleep quality, other than the score for frequent dreaming, also suggested that the sleep quality was still poor [30]. As compared with other studies examining the sleep measures of rugby union players, in the present study, the total sleep time and sleep efficiency were lower [24,39]. The major plausible reason for the poor sleep quality and quantity is that the participants in this study underwent field-based rugby union-specific training in hot environments. As shown in Table 1, the total physical activity and RPE after exercise did not differ between the two study conditions, suggesting that the intensity of exercise on the day of the experiment was not different between the two conditions. In addition to the exercise intensity, the timing of the exercise and exercise duration are thought to be important parameters that could have acute effects on sleep. In the present study, the participants performed exercise for 60 min at least 6 h before bedtime. In a previous study, no reliable effects of exercise on sleep were seen when the duration of exercise was 60 min [40]. Another previous study showed the absence of any differences in the rectal temperature at bedtime or throughout the sleep period following exercise for 1 h at 60% VO2 max performed 5–6 h before bedtime, as compared with the non-exercise control condition [40]. Therefore, the sleep quality decrement observed in this study is likely to be due to the hot environment.
As reported from previous studies on the effects of external cooling, no differences were observed between the study conditions in sleep measures such as bedtime, wake time, time in bed, total sleep time, wake time after sleep onset, or sleep efficiency [12,13]. In these latter studies, the effect of cold-water immersion after exercise to shorten the sleep latency could be explained in part by the reduced muscle discomfort. However, since ice slurry ingestion has been shown to have no direct effect on the muscle temperature, it is possible that a different mechanism could exist to explain the beneficial effects of ice slurry ingestion on the sleep latency and subjective fatigue in this study. One such example is the brain cooling effect via conductive cooling. It was recently reported using magnetic resonance spectroscopy that ingestion of ice slurry lowers the temperature of the frontal lobe [41]. The effect of ice slurry ingestion in the present study on the brain temperature could explain its effects on the sleep latency and subjective fatigue.
In particular, the sleep latency has been reported to be associated with the core body temperature [8]. The core body temperature of the participants may have been affected by the ambient temperature, but ingestion of ice slurry may have caused a rapid decrease in the core body temperature, contributing to the improved sleep latency [42]. In a previous study, ingestion of 2 g/kg body mass of ice slurry 30 min prior to exercise reduced the core body temperature [17]. Therefore, in this study, the participants ingested 2 g/kg body mass of ice slurry 30 min before bedtime. Because the room temperature was controlled at 25 °C, and not higher, the amount of ice slurry ingested was sufficient to improve the sleep quality.
No adverse events associated with the ingestion of ice slurry were observed during the study period, indicating the safety of ice slurry ingestion. Ice slurry ingestion at bedtime could be a useful alternative for improving the sleep quality in hot environments, with no side-effects such as habituation or dependence on hypnotics.
This study had some limitations. Firstly, in this study, we used an actigraphy device, MTN-220, which can be attached to the waist to monitor the sleep quality, because all participants were not familiar with portable polysomnography. Actigraphy underestimates the sleep latency and total wake time, and consequently overestimates the total sleep time and sleep efficiency [43]. Although the abovementioned systematic differences between polysomnography and actigraphy exist, actigraphy is thought to be able to detect treatment effects of sleep parameters [43]. Furthermore, since the MTN-220 cannot measure sleep stages, further studies using portable polysomnography are needed to clarify the effect of ingestion of ice slurry on the sleep stages. Secondly, the sample size for this study was small and the sleep quality measurement period was only 1 day. There is a well-known phenomenon called the “first night effect”, which is characterized by a decrease in sleep quality on the first night of testing [44]. Therefore, in order to clarify the effects of ingestion of ice slurry at bedtime on the sleep quality, a larger, randomized controlled trial with a longer period of measurement of the sleep quality is warranted. Thirdly, ingestion of ice slurry did not improve variables of sleep quality in hot environments other than the sleep latency as an objective sleep parameter and “feeling refreshed (recovery from fatigue)” as a subjective parameter. Further research on the sleep quality is, therefore, required among rugby union players, involving comprehensive indices of sleep quality, recovery from fatigue, and exercise performance over longer periods of time. Lastly, in this study, we were not able to monitor the brain and core body temperature during sleep. Because these measurements interfere with the sleep quality of the participants, a noncontact and continuous method of measurement is necessary to clarify the detailed mechanism of the effect of ingestion of ice slurry at bedtime on the sleep quality. Moreover, we did not measure thermal sensation or thermal comfort at the time of ingestion. The cold sensations experienced by the participants in the ice slurry condition might have affected the sleep parameters. To clarify the potential biases arising from the differences in subjective comfort, future studies should examine the effect of cold sensation on the sleep parameters.
5. Conclusions
The results showed that ice slurry ingestion at bedtime did not affect the sleep duration, but suggested the possibility that it improved the latency of sleep onset and accelerated recovery from subjective fatigue. Ice slurry ingestion at bedtime might be useful as a sleep improvement strategy in rugby union players engaging in exercises during the summer season. Further research is, therefore, required on the comprehensive sleep architecture and objective recovery status of rugby union players.
Author Contributions
Conceptualization, A.M., S.Y. and K.K.; methodology, A.M., S.Y. and M.S.; formal analysis, T.I.; investigation, A.H. and S.T.; data curation, T.I.; writing—original draft preparation, A.M.; writing—review and editing, all authors; supervision, A.M. and N.K.; funding acquisition, A.M. All authors read and agreed to the published version of the manuscript.
Funding
This research was funded by Taisho Pharmaceutical Co., Ltd.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Keio University Graduate School of System Design (approval number: SDM-2020-E017).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to thank staff and members of the Keio University Rugby Football Club who participated in this study.
Conflicts of Interest
A.M., S.Y., M.S. and K.K. are employees of Taisho Pharmaceutical Co., Ltd., which supported the present study in part. However, the funders had no role in the recruitment of the participants or data collection and analysis.
References
- Kellmann, M.; Bertollo, M.; Bosquet, L.; Brink, M.; Coutts, A.J.; Duffield, R.; Erlacher, D.; Halson, S.L.; Hecksteden, A.; Heidari, J.; et al. Recovery and Performance in Sport: Consensus Statement. Int. J. Sports Physiol. Perform. 2018, 13, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Claudino, J.G.; Gabbet, T.J.; De Sá Souza, H.; Simim, M.; Fowler, P.; De Alcantara Borba, D.; Melo, M.; Bottino, A.; Loturco, I.; D’Almeida, V.; et al. Which Parameters to Use for Sleep Quality Monitoring in Team Sport Athletes? A Systematic Review and Meta-Analysis. BMJ Open Sport Exerc. Med. 2019, 5, e000475. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.S.H.; Teo, W.P.; Warmington, S.A. Effects of Training and Competition on the Sleep of Elite Athletes: A Systematic Review and Meta-Analysis. Br. J. Sports Med. 2019, 53, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, O.; Douzi, W.; Theurot, D.; Bosquet, L.; Dugué, B. An Evidence-Based Approach for Choosing Post-Exercise Recovery Techniques to Reduce Markers of Muscle Damage, Soreness, Fatigue, and Inflammation: A Systematic Review With Meta-Analysis. Front. Physiol. 2018, 9, 403. [Google Scholar] [CrossRef]
- Karacan, I.; Thornby, J.I.; Anch, A.M.; Williams, R.L.; Perkins, H.M. Effects of High Ambient Temperature on Sleep in Young Men. Aviat. Space Environ. Med. 1978, 49, 855–860. [Google Scholar] [PubMed]
- Conlan, G.; McLean, B.; Kemp, J.; Duffield, R. Effect of Training/Competition Load and Scheduling on Sleep Characteristics in Professional Rugby League Athletes. J. Strength Cond. Res. 2021. [Google Scholar] [CrossRef]
- Reid, K. Assessment of Circadian Rhythms. Neurol. Clin. 2019, 37, 505–526. [Google Scholar] [CrossRef]
- Gilbert, S.S.; Van Den Heuvel, C.J.; Dawson, D. Daytime Melatonin and Temazepam in Young Adult Humans: Equivalent Effects on Sleep Latency and Body Temperatures. J. Physiol. 1999, 514, 905–914. [Google Scholar] [CrossRef]
- Kräuchi, K. The Human Sleep-Wake Cycle Reconsidered from a Thermoregulatory Point of View. Physiol. Behav. 2007, 90, 236–245. [Google Scholar] [CrossRef]
- Kimura, S.; Takaoka, Y.; Toyoura, M.; Kohira, S.; Ohta, M. Core Body Temperature Changes in School-Age Children with Circadian Rhythm Sleep-Wake Disorder. Sleep Med. 2021, 87, 97–104. [Google Scholar] [CrossRef]
- Skein, M.; Wingfield, G.; Gale, R.; Washington, T.; Minett, G. Sleep Quantity and Quality during Consecutive Day Heat Training with the Inclusion of Cold-Water Immersion Recovery. J. Therm. Biol. 2018, 74, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Lastella, M.; Roach, G.D.; Halson, S.L.; Sargent, C. The Effects of Cold Water Immersion on the Amount and Quality of Sleep Obtained by Elite Cyclists during a Simulated Hill Climbing Tour. Sport Sci. Health 2019, 15, 223–228. [Google Scholar] [CrossRef]
- Robey, E.; Dawson, B.; Halson, S.; Gregson, W.; King, S.; Goodman, C.; Eastwood, P. Effect of Evening Postexercise Cold Water Immersion on Subsequent Sleep. Med. Sci. Sports Exerc. 2013, 45, 1394–1402. [Google Scholar] [CrossRef] [PubMed]
- Krueger, M.; Costello, J.T.; Stenzel, M.; Mester, J.; Wahl, P. The Physiological Effects of Daily Cold-Water Immersion on 5-Day Tournament Performance in International Standard Youth Field-Hockey Players. Eur. J. Appl. Physiol. 2020, 120, 295–305. [Google Scholar] [CrossRef]
- Douzi, W.; Dugué, B.; Vinches, L.; Al Sayed, C.; Hallé, S.; Bosquet, L.; Dupuy, O. Cooling during Exercise Enhances Performances, but the Cooled Body Areas Matter: A Systematic Review with Meta-Analyses. Scand. J. Med. Sci. Sports 2019, 29, 1660–1676. [Google Scholar] [CrossRef]
- Osakabe, J.; Matsumoto, T.; Umemura, Y. Ice Slurry Ingestion as a Cooling Strategy in the Heat. J. Phys. Fit. Sports Med. 2019, 8, 73–78. [Google Scholar] [CrossRef]
- Levels, K.; Teunissen, L.P.J.; De Haan, A.; De Koning, J.J.; Van Os, B.; Daanen, H.A.M. Effect of Warm-up and Precooling on Pacing during a 15-Km Cycling Time Trial in the Heat. Int. J. Sports Physiol. Perform. 2013, 8, 307–311. [Google Scholar] [CrossRef][Green Version]
- Nakamura, M.; Nakamura, D.; Yasumatsu, M.; Takahashi, H. Effect of Ice Slurry Ingestion on Core Temperature and Blood Pressure Response after Exercise in a Hot Environment. J. Therm. Biol. 2021, 98, 102922. [Google Scholar] [CrossRef]
- Siegel, R.; Maté, J.; Brearley, M.B.; Watson, G.; Nosaka, K.; Laursen, P.B. Ice Slurry Ingestion Increases Core Temperature Capacity and Running Time in the Heat. Med. Sci. Sports Exerc. 2010, 42, 717–725. [Google Scholar] [CrossRef]
- Creado, S.; Advani, S. Sleep Disorders in the Athlete. Psychiatr. Clin. N. Am. 2021, 44, 393–403. [Google Scholar] [CrossRef]
- Nelson, K.; Davis, J.; Corbett, C. Sleep Quality: An Evolutionary Concept Analysis. Nurs. Forum 2022, 57, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.R.; King, R.F.G.J.; Duckworth, L.C.; Sutton, L.; Preston, T.; O’Hara, J.P.; Jones, B. Energy Expenditure of Rugby Players during a 14-Day in-Season Period, Measured Using Doubly Labelled Water. Eur. J. Appl. Physiol. 2018, 118, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Meir, R.; Brooks, L.; Shield, T. Body Weight and Tympanic Temperature Change in Professional Rugby League Players during Night and Day Games: A Study in the Field. J. Strength Cond. Res. 2003, 17, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Swinbourne, R.; Miller, J.; Smart, D.; Dulson, D.K.; Gill, N. The Effects of Sleep Extension on Sleep, Performance, Immunity and Physical Stress in Rugby Players. Sports 2018, 6, 42. [Google Scholar] [CrossRef]
- Borg, G. Psychophysical Bases of Perceived Exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Matsuo, M.; Masuda, F.; Sumi, Y.; Takahashi, M.; Yamada, N.; Ohira, M.H.; Fujiwara, K.; Kanemura, T.; Kadotani, H. Comparisons of Portable Sleep Monitors of Different Modalities: Potential as Naturalistic Sleep Recorders. Front. Neurol. 2016, 7, 110. [Google Scholar] [CrossRef]
- Nakada, Y.; Sugimoto, A.; Kadotani, H.; Yamada, N. Verification of Effect of Sleep Health Education Program in Workplace: A Quasi-Randomized Controlled Trial. Ind. Health 2018, 56, 20–29. [Google Scholar] [CrossRef]
- Nakazaki, K.; Kitamura, S.; Motomura, Y.; Hida, A.; Kamei, Y.; Miura, N.; Mishima, K. Validity of an Algorithm for Determining Sleep/Wake States Using a New Actigraph. J. Physiol. Anthropol. 2014, 33, 31. [Google Scholar] [CrossRef]
- Shrivastava, D.; Jung, S.; Saadat, M.; Sirohi, R.; Crewson, K. How to Interpret the Results of a Sleep Study. J. Community Hosp. Intern. Med. Perspect. 2014, 4, 24983. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Takase, M.; Yamazaki, K.; Shirakawa, S.; Azumi, K. Standardization of Revised Version of OSA Sleep Inventory for Middle Age and Aged. Brain Sci. Ment. Disord. 1999, 10, 401–409. [Google Scholar]
- Umigai, N.; Takeda, R.; Mori, A. Effect of Crocetin on Quality of Sleep: A Randomized, Double-Blind, Placebo-Controlled, Crossover Study. Complementary Ther. Med. 2018, 41, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 2013. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Nakamura, T.; Hayano, J.; Yamamoto, Y. Seasonal Sleep Variations and Their Association With Meteorological Factors: A Japanese Population Study Using Large-Scale Body Acceleration Data. Front. Digit. Health 2021, 3, 677043. [Google Scholar] [CrossRef] [PubMed]
- Okamoto-Mizuno, K.; Tsuzuki, K. Effects of Season on Sleep and Skin Temperature in the Elderly. Int. J. Biometeorol. 2010, 54, 401–409. [Google Scholar] [CrossRef]
- Bannai, M.; Kawai, N. New Therapeutic Strategy for Amino Acid Medicine: Glycine Improves the Quality of Sleep. J. Pharmacol. Sci. 2012, 118, 145–148. [Google Scholar] [CrossRef]
- Hashizaki, M.; Nakajima, H.; Shiga, T.; Tsutsumi, M.; Kume, K. A Longitudinal Large-Scale Objective Sleep Data Analysis Revealed a Seasonal Sleep Variation in the Japanese Population. Chronobiol. Int. 2018, 35, 933–945. [Google Scholar] [CrossRef]
- Hu, X.; Wei, W.; Huang, D.; Lin, C.; Lu, F.; Li, X.; Liao, H.; Yu, Z.; Weng, X.; Wang, S.; et al. The Assessment of Sleep Quality in Patients Following Valve Repair and Valve Replacement for Infective Endocarditis: A Retrospective Study at a Single Center. Med. Sci. Monit. 2021, 27, e930596. [Google Scholar] [CrossRef]
- Leduc, C.; Tee, J.; Phibbs, P.; Read, D.; Ramirez, C.; Thomas, S.; Weaving, D.; Jones, B. Objective Sleep Patterns and Validity of Self-Reported Sleep Monitoring across Different Playing Levels in Rugby Union. S. Afr. J. Sport. Med. 2020, 32, 1–6. [Google Scholar] [CrossRef]
- Youngstedt, S.D.; O’Connor, P.J.; Dishman, R.K. The Effects of Acute Exercise on Sleep: A Quantitative Synthesis. Sleep 1997, 20, 203–214. [Google Scholar] [CrossRef]
- Onitsuka, S.; Nakamura, D.; Onishi, T.; Arimitsu, T.; Takahashi, H.; Hasegawa, H. Ice Slurry Ingestion Reduces Human Brain Temperature Measured Using Non-Invasive Magnetic Resonance Spectroscopy. Sci. Rep. 2018, 8, 2757. [Google Scholar] [CrossRef]
- Haghayegh, S.; Khoshnevis, S.; Smolensky, M.H.; Diller, K.R.; Castriotta, R.J. Before-Bedtime Passive Body Heating by Warm Shower or Bath to Improve Sleep: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2019, 46, 124–135. [Google Scholar] [CrossRef] [PubMed]
- Sivertsen, B.; Omvik, S.; Havik, O.E.; Pallesen, S.; Bjorvatn, B.; Nielsen, G.H.; Straume, S.; Nordhus, I.H. A Comparison of Actigraphy and Polysomnography in Older Adults Treated for Chronic Primary Insomnia. Sleep 2006, 29, 1353–1358. [Google Scholar] [CrossRef] [PubMed]
- Herbst, E.; Metzler, T.J.; Lenoci, M.; Mc Caslin, S.E.; Inslicht, S.; Marmar, C.R.; Neylan, T.C. Adaptation Effects to Sleep Studies in Participants with and without Chronic Posttraumatic Stress Disorder. Psychophysiology 2010, 47, 1127–1133. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).