
Effect of Ingestion of Ice Slurry on the Sleep Quality of Rugby Union Players in the Summer Season

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
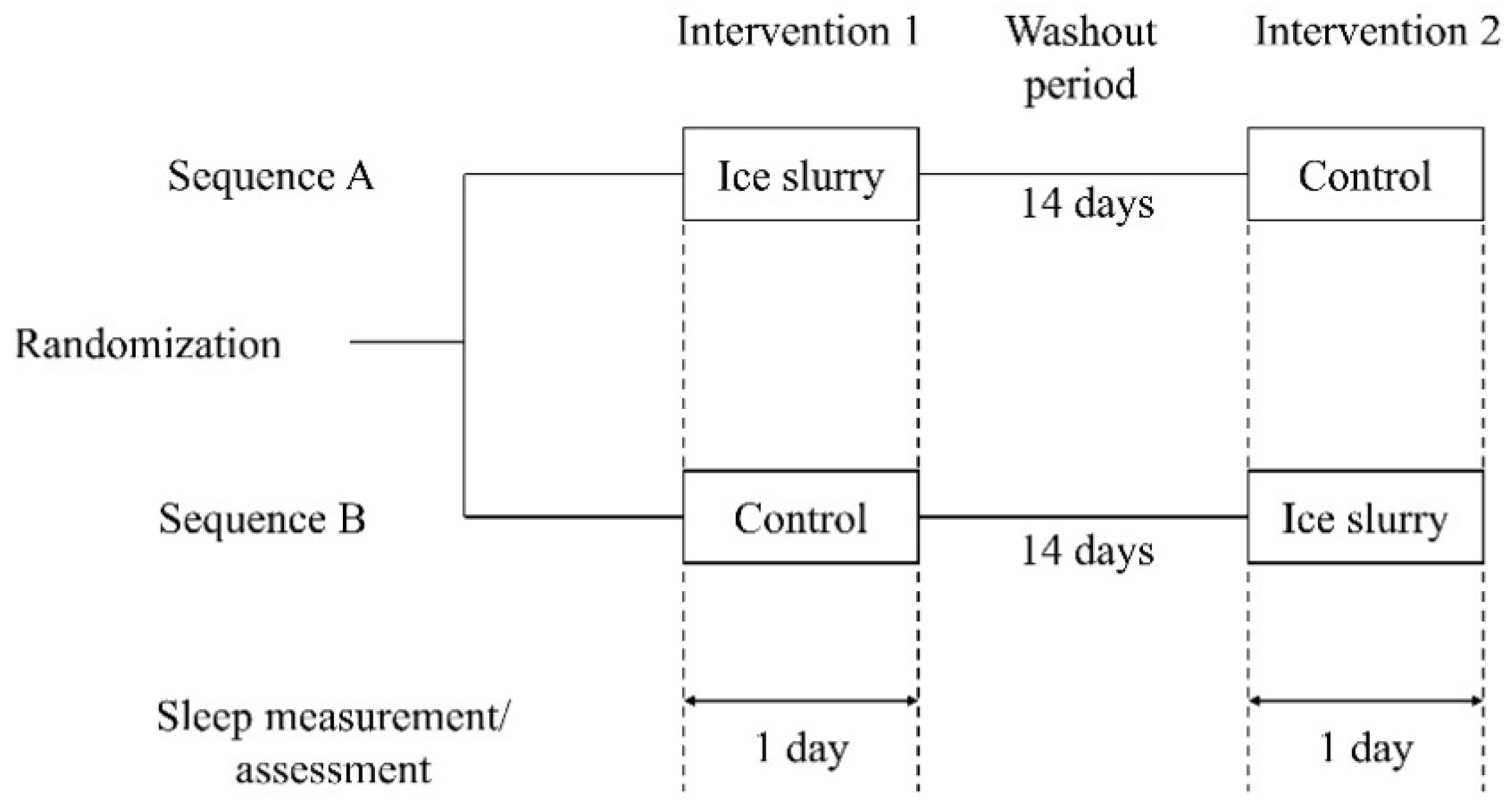
2.2. Study Design
2.3. Intervention
2.4. Rating of Perceived Exertion and Total Physical Activity Count
2.5. Measurements and Analysis of Objective Sleep Parameters
2.6. Assessment of Subjective Sleep Parameters
2.7. Statistical Analysis
3. Results
3.1. Training Status of the Test Day
3.2. Objective Sleep Parameters
3.3. Subjective Sleep Parameters
3.4. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kellmann, M.; Bertollo, M.; Bosquet, L.; Brink, M.; Coutts, A.J.; Duffield, R.; Erlacher, D.; Halson, S.L.; Hecksteden, A.; Heidari, J.; et al. Recovery and Performance in Sport: Consensus Statement. Int. J. Sports Physiol. Perform. 2018, 13, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Claudino, J.G.; Gabbet, T.J.; De Sá Souza, H.; Simim, M.; Fowler, P.; De Alcantara Borba, D.; Melo, M.; Bottino, A.; Loturco, I.; D’Almeida, V.; et al. Which Parameters to Use for Sleep Quality Monitoring in Team Sport Athletes? A Systematic Review and Meta-Analysis. BMJ Open Sport Exerc. Med. 2019, 5, e000475. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.S.H.; Teo, W.P.; Warmington, S.A. Effects of Training and Competition on the Sleep of Elite Athletes: A Systematic Review and Meta-Analysis. Br. J. Sports Med. 2019, 53, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, O.; Douzi, W.; Theurot, D.; Bosquet, L.; Dugué, B. An Evidence-Based Approach for Choosing Post-Exercise Recovery Techniques to Reduce Markers of Muscle Damage, Soreness, Fatigue, and Inflammation: A Systematic Review With Meta-Analysis. Front. Physiol. 2018, 9, 403. [Google Scholar] [CrossRef]
- Karacan, I.; Thornby, J.I.; Anch, A.M.; Williams, R.L.; Perkins, H.M. Effects of High Ambient Temperature on Sleep in Young Men. Aviat. Space Environ. Med. 1978, 49, 855–860. [Google Scholar] [PubMed]
- Conlan, G.; McLean, B.; Kemp, J.; Duffield, R. Effect of Training/Competition Load and Scheduling on Sleep Characteristics in Professional Rugby League Athletes. J. Strength Cond. Res. 2021. [Google Scholar] [CrossRef]
- Reid, K. Assessment of Circadian Rhythms. Neurol. Clin. 2019, 37, 505–526. [Google Scholar] [CrossRef]
- Gilbert, S.S.; Van Den Heuvel, C.J.; Dawson, D. Daytime Melatonin and Temazepam in Young Adult Humans: Equivalent Effects on Sleep Latency and Body Temperatures. J. Physiol. 1999, 514, 905–914. [Google Scholar] [CrossRef]
- Kräuchi, K. The Human Sleep-Wake Cycle Reconsidered from a Thermoregulatory Point of View. Physiol. Behav. 2007, 90, 236–245. [Google Scholar] [CrossRef]
- Kimura, S.; Takaoka, Y.; Toyoura, M.; Kohira, S.; Ohta, M. Core Body Temperature Changes in School-Age Children with Circadian Rhythm Sleep-Wake Disorder. Sleep Med. 2021, 87, 97–104. [Google Scholar] [CrossRef]
- Skein, M.; Wingfield, G.; Gale, R.; Washington, T.; Minett, G. Sleep Quantity and Quality during Consecutive Day Heat Training with the Inclusion of Cold-Water Immersion Recovery. J. Therm. Biol. 2018, 74, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Lastella, M.; Roach, G.D.; Halson, S.L.; Sargent, C. The Effects of Cold Water Immersion on the Amount and Quality of Sleep Obtained by Elite Cyclists during a Simulated Hill Climbing Tour. Sport Sci. Health 2019, 15, 223–228. [Google Scholar] [CrossRef]
- Robey, E.; Dawson, B.; Halson, S.; Gregson, W.; King, S.; Goodman, C.; Eastwood, P. Effect of Evening Postexercise Cold Water Immersion on Subsequent Sleep. Med. Sci. Sports Exerc. 2013, 45, 1394–1402. [Google Scholar] [CrossRef] [PubMed]
- Krueger, M.; Costello, J.T.; Stenzel, M.; Mester, J.; Wahl, P. The Physiological Effects of Daily Cold-Water Immersion on 5-Day Tournament Performance in International Standard Youth Field-Hockey Players. Eur. J. Appl. Physiol. 2020, 120, 295–305. [Google Scholar] [CrossRef]
- Douzi, W.; Dugué, B.; Vinches, L.; Al Sayed, C.; Hallé, S.; Bosquet, L.; Dupuy, O. Cooling during Exercise Enhances Performances, but the Cooled Body Areas Matter: A Systematic Review with Meta-Analyses. Scand. J. Med. Sci. Sports 2019, 29, 1660–1676. [Google Scholar] [CrossRef]
- Osakabe, J.; Matsumoto, T.; Umemura, Y. Ice Slurry Ingestion as a Cooling Strategy in the Heat. J. Phys. Fit. Sports Med. 2019, 8, 73–78. [Google Scholar] [CrossRef]
- Levels, K.; Teunissen, L.P.J.; De Haan, A.; De Koning, J.J.; Van Os, B.; Daanen, H.A.M. Effect of Warm-up and Precooling on Pacing during a 15-Km Cycling Time Trial in the Heat. Int. J. Sports Physiol. Perform. 2013, 8, 307–311. [Google Scholar] [CrossRef][Green Version]
- Nakamura, M.; Nakamura, D.; Yasumatsu, M.; Takahashi, H. Effect of Ice Slurry Ingestion on Core Temperature and Blood Pressure Response after Exercise in a Hot Environment. J. Therm. Biol. 2021, 98, 102922. [Google Scholar] [CrossRef]
- Siegel, R.; Maté, J.; Brearley, M.B.; Watson, G.; Nosaka, K.; Laursen, P.B. Ice Slurry Ingestion Increases Core Temperature Capacity and Running Time in the Heat. Med. Sci. Sports Exerc. 2010, 42, 717–725. [Google Scholar] [CrossRef]
- Creado, S.; Advani, S. Sleep Disorders in the Athlete. Psychiatr. Clin. N. Am. 2021, 44, 393–403. [Google Scholar] [CrossRef]
- Nelson, K.; Davis, J.; Corbett, C. Sleep Quality: An Evolutionary Concept Analysis. Nurs. Forum 2022, 57, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.R.; King, R.F.G.J.; Duckworth, L.C.; Sutton, L.; Preston, T.; O’Hara, J.P.; Jones, B. Energy Expenditure of Rugby Players during a 14-Day in-Season Period, Measured Using Doubly Labelled Water. Eur. J. Appl. Physiol. 2018, 118, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Meir, R.; Brooks, L.; Shield, T. Body Weight and Tympanic Temperature Change in Professional Rugby League Players during Night and Day Games: A Study in the Field. J. Strength Cond. Res. 2003, 17, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Swinbourne, R.; Miller, J.; Smart, D.; Dulson, D.K.; Gill, N. The Effects of Sleep Extension on Sleep, Performance, Immunity and Physical Stress in Rugby Players. Sports 2018, 6, 42. [Google Scholar] [CrossRef]
- Borg, G. Psychophysical Bases of Perceived Exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Matsuo, M.; Masuda, F.; Sumi, Y.; Takahashi, M.; Yamada, N.; Ohira, M.H.; Fujiwara, K.; Kanemura, T.; Kadotani, H. Comparisons of Portable Sleep Monitors of Different Modalities: Potential as Naturalistic Sleep Recorders. Front. Neurol. 2016, 7, 110. [Google Scholar] [CrossRef]
- Nakada, Y.; Sugimoto, A.; Kadotani, H.; Yamada, N. Verification of Effect of Sleep Health Education Program in Workplace: A Quasi-Randomized Controlled Trial. Ind. Health 2018, 56, 20–29. [Google Scholar] [CrossRef]
- Nakazaki, K.; Kitamura, S.; Motomura, Y.; Hida, A.; Kamei, Y.; Miura, N.; Mishima, K. Validity of an Algorithm for Determining Sleep/Wake States Using a New Actigraph. J. Physiol. Anthropol. 2014, 33, 31. [Google Scholar] [CrossRef]
- Shrivastava, D.; Jung, S.; Saadat, M.; Sirohi, R.; Crewson, K. How to Interpret the Results of a Sleep Study. J. Community Hosp. Intern. Med. Perspect. 2014, 4, 24983. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Takase, M.; Yamazaki, K.; Shirakawa, S.; Azumi, K. Standardization of Revised Version of OSA Sleep Inventory for Middle Age and Aged. Brain Sci. Ment. Disord. 1999, 10, 401–409. [Google Scholar]
- Umigai, N.; Takeda, R.; Mori, A. Effect of Crocetin on Quality of Sleep: A Randomized, Double-Blind, Placebo-Controlled, Crossover Study. Complementary Ther. Med. 2018, 41, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 2013. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Nakamura, T.; Hayano, J.; Yamamoto, Y. Seasonal Sleep Variations and Their Association With Meteorological Factors: A Japanese Population Study Using Large-Scale Body Acceleration Data. Front. Digit. Health 2021, 3, 677043. [Google Scholar] [CrossRef] [PubMed]
- Okamoto-Mizuno, K.; Tsuzuki, K. Effects of Season on Sleep and Skin Temperature in the Elderly. Int. J. Biometeorol. 2010, 54, 401–409. [Google Scholar] [CrossRef]
- Bannai, M.; Kawai, N. New Therapeutic Strategy for Amino Acid Medicine: Glycine Improves the Quality of Sleep. J. Pharmacol. Sci. 2012, 118, 145–148. [Google Scholar] [CrossRef]
- Hashizaki, M.; Nakajima, H.; Shiga, T.; Tsutsumi, M.; Kume, K. A Longitudinal Large-Scale Objective Sleep Data Analysis Revealed a Seasonal Sleep Variation in the Japanese Population. Chronobiol. Int. 2018, 35, 933–945. [Google Scholar] [CrossRef]
- Hu, X.; Wei, W.; Huang, D.; Lin, C.; Lu, F.; Li, X.; Liao, H.; Yu, Z.; Weng, X.; Wang, S.; et al. The Assessment of Sleep Quality in Patients Following Valve Repair and Valve Replacement for Infective Endocarditis: A Retrospective Study at a Single Center. Med. Sci. Monit. 2021, 27, e930596. [Google Scholar] [CrossRef]
- Leduc, C.; Tee, J.; Phibbs, P.; Read, D.; Ramirez, C.; Thomas, S.; Weaving, D.; Jones, B. Objective Sleep Patterns and Validity of Self-Reported Sleep Monitoring across Different Playing Levels in Rugby Union. S. Afr. J. Sport. Med. 2020, 32, 1–6. [Google Scholar] [CrossRef]
- Youngstedt, S.D.; O’Connor, P.J.; Dishman, R.K. The Effects of Acute Exercise on Sleep: A Quantitative Synthesis. Sleep 1997, 20, 203–214. [Google Scholar] [CrossRef]
- Onitsuka, S.; Nakamura, D.; Onishi, T.; Arimitsu, T.; Takahashi, H.; Hasegawa, H. Ice Slurry Ingestion Reduces Human Brain Temperature Measured Using Non-Invasive Magnetic Resonance Spectroscopy. Sci. Rep. 2018, 8, 2757. [Google Scholar] [CrossRef]
- Haghayegh, S.; Khoshnevis, S.; Smolensky, M.H.; Diller, K.R.; Castriotta, R.J. Before-Bedtime Passive Body Heating by Warm Shower or Bath to Improve Sleep: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2019, 46, 124–135. [Google Scholar] [CrossRef] [PubMed]
- Sivertsen, B.; Omvik, S.; Havik, O.E.; Pallesen, S.; Bjorvatn, B.; Nielsen, G.H.; Straume, S.; Nordhus, I.H. A Comparison of Actigraphy and Polysomnography in Older Adults Treated for Chronic Primary Insomnia. Sleep 2006, 29, 1353–1358. [Google Scholar] [CrossRef] [PubMed]
- Herbst, E.; Metzler, T.J.; Lenoci, M.; Mc Caslin, S.E.; Inslicht, S.; Marmar, C.R.; Neylan, T.C. Adaptation Effects to Sleep Studies in Participants with and without Chronic Posttraumatic Stress Disorder. Psychophysiology 2010, 47, 1127–1133. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Control | Ice Slurry | p-Value | Cohen’s d | |
|---|---|---|---|---|---|
| RPE | Before exercise for 60 min | 10.7 ± 1.3 | 10.6 ± 1.6 | 0.705 | 0.19 |
| After exercise for 60 min | 18.1 ± 1.6 | 18.0 ± 1.7 | 0.828 | 0.17 | |
| Total physical activity count | 1487.8 ± 121.3 | 1444.3 ± 122.6 | 0.348 | 1.29 | |
| Sleep Parameters | Control | Ice Slurry | p-Value | Cohen’s d |
|---|---|---|---|---|
| Bedtime (hh:mm) | 23:28 ± 00:43 | 23:49 ± 01:14 | 0.451 | 0.35 |
| Wake time (hh:mm) | 07:09 ± 00:59 | 07:04 ± 00:33 | 0.755 | 0.11 |
| Time in bed (min) | 461.2 ± 65.5 | 434.8 ± 69.8 | 0.351 | 0.39 |
| Total sleep time (min) | 259.5 ± 60.1 | 255.4 ± 64.5 | 0.867 | 0.07 |
| Sleep latency (min) | 72.3 ± 60.2 | 34.3 ± 23.6 * | 0.026 | 0.83 |
| Wake time after sleep onset (min) | 117.2 ± 54.0 | 133.8 ± 45.2 | 0.290 | 0.33 |
| Sleep efficiency (%) | 56.4 ± 11.4 | 58.8 ± 11.7 | 0.535 | 0.21 |
| Sleep Parameters | Control | Ice Slurry | p-Value | Cohen’s d |
|---|---|---|---|---|
| Factor I Sleepiness upon rising | 42.9 ± 6.0 | 46.2 ± 7.7 | 0.165 | 0.48 |
| Factor II Initiation and maintenance of sleep | 38.6 ± 9.7 | 41.8 ± 9.4 | 0.350 | 0.34 |
| Factor III Frequent dreaming | 50.1 ± 10.0 | 50.7 ± 8.2 | 0.875 | 0.07 |
| Factor IV Feeling refreshed (recovery from fatigue) | 40.1 ± 6.9 | 46.8 ± 6.5 * | 0.030 | 1.00 |
| Factor V Sleep length | 45.5 ± 9.1 | 46.2 ± 8.3 | 0.781 | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morito, A.; Inami, T.; Hirata, A.; Yamada, S.; Shimomasuda, M.; Kato, K.; Tahara, S.; Kohtake, N. Effect of Ingestion of Ice Slurry on the Sleep Quality of Rugby Union Players in the Summer Season. Physiologia 2022, 2, 46-54. https://doi.org/10.3390/physiologia2030005
Morito A, Inami T, Hirata A, Yamada S, Shimomasuda M, Kato K, Tahara S, Kohtake N. Effect of Ingestion of Ice Slurry on the Sleep Quality of Rugby Union Players in the Summer Season. Physiologia. 2022; 2(3):46-54. https://doi.org/10.3390/physiologia2030005
Chicago/Turabian StyleMorito, Akihisa, Takayuki Inami, Akihiro Hirata, Satoshi Yamada, Masatsugu Shimomasuda, Keita Kato, Shigeyuki Tahara, and Naohiko Kohtake. 2022. "Effect of Ingestion of Ice Slurry on the Sleep Quality of Rugby Union Players in the Summer Season" Physiologia 2, no. 3: 46-54. https://doi.org/10.3390/physiologia2030005
APA StyleMorito, A., Inami, T., Hirata, A., Yamada, S., Shimomasuda, M., Kato, K., Tahara, S., & Kohtake, N. (2022). Effect of Ingestion of Ice Slurry on the Sleep Quality of Rugby Union Players in the Summer Season. Physiologia, 2(3), 46-54. https://doi.org/10.3390/physiologia2030005