Abstract
In the present study, a Google Forms survey open questionnaire was applied to identify variables in hygiene habits that influence the contamination of toothbrushes in Mexican homes. A total of 275 questionnaires were validated, and 18 samples were analyzed to determine microbiology indicator groups (Mesophilic Aerobic Bacteria [MAB], Coliform Organisms [CO], and Yeast and Molds [Y/M]) with dilution and plate casting methods. Results were compared with data obtained from surveys, which were encoded to construct conglomerates. Interestingly, a higher microbial count was found in toothbrushes stored in cases (4.9 × 109 CFU/mL for MAB, 4.43 × 109 CFU/mL for CO, and 4.38 × 109 CFU/mL for Y/M), while the use and disposal of toothbrushes following recommendations of life expectancy limited bacterial growth (<10 CFU/mL for CO and Y/M), reducing the possible growth of pathogens such as Klebsiella pneumoniae, Streptococcus pyogenes, and Pseudomonas, among others. Finally, most people do not have the habit of disinfecting their toothbrushes periodically. Further, the survey revealed that disinfection techniques applied by a limited group (14% of the respondents) are improvised and are not standardized with the objective of disinfection.
1. Introduction
In the XIX century, toothbrushing was popularized since the promulgation of the Louis Pasteur germ theory, for which dental brushes were widely used to reduce harmful bacterial growth for oral health, eliminate food residues, maintain a fresh breath, and prevent gingival inflammation. Nevertheless, a risk associated with toothbrush contamination has been recorded since 1920, and in 1992, it was observed that contaminated brushes may cause bacteremia and septicemia. Also, this contamination can be linked to opportunistic microorganisms and even respiratory viruses such as SARS-CoV-2 or influenza, which may be lethal for humans [1,2,3].
Contamination is the retention and survival of infectious organisms that occur in living and non-living things. In healthy adults, toothbrush contamination takes place soon after initial use and increases with repeated use. Contamination can be direct or indirect and is affected by microorganisms such as enterobacterium found in the storage environment and others that can be present in oral cavities, like opportunistic bacteria. Those microorganisms reach toothbrushes through different mechanisms, like contact with user hands, aerosols expelled from toilets without cover, extended use of brushes, storage, and use of cases [3,4,5]. Contamination of toothbrushes can be related to humidity or toilet sitting, while the use of disinfectants such as chlorhexidine after toothbrushing or even the use brushes made of activated carbon helps reduce the bacterial count [6].
Bad hygiene practices and dental cavity presence have been related to high counts of Gram-negative facultative anaerobic microorganisms, where the yeast Candida albicans can be found [7]. Also, factors such as smoking and the use and abuse of antibiotics may create an imbalance of the oral microbiome and, eventually, lead to dental cavities and periodontitis, which are diseases caused by acidogenic and acid-tolerant microorganisms like Streptococcus mutants, or inflammation due to cariogenic bacteria [8]. It has been reported that many pathogens can induce bacteremia when they invade the body through poor oral hygiene practices [9]. Unfortunately, Alzheimer’s disease and pneumonia development have been correlated with anaerobic bacteria, causing periodontal disease and modifying oral cavity bacteria. Even though toothbrushing favors the removal of these bacteria, humidity and food leftovers may remain in toothbrushes, turning into pathogen reservoirs that can become potential risks for oral diseases [2].
Indicator microorganisms (IM) behave similarly to pathogens regarding concentrations and reactions to environmental factors; the difference lies in that IM are easier, quicker, and cheaper to identify. Once the presence of IM is identified, it can be inferred that among them, pathogens may be present, reacting in the same manner to pH, temperature, the presence of nutrients, hydraulic retention time, and disinfection systems. Among IM, mesophilic aerobic bacteria have high significance since they grow at temperatures of 35 ± 2 °C. Coliforms are non-sporulated aerobic or facultative anaerobic Gram-negative bacilli that ferment lactose, while yeast and molds are relevant due to toxin production and are easily transferred through aerosols [10,11,12].
Thus, it is vital to conduct different studies that allow the correlation of activities practiced in homes that are not adequate and that expose directly or indirectly the quality and innocuity of the toothbrush, influencing the contamination with IM in samples, such as the handling and storage localization of toothbrushes. On the other hand, it is also important to put this information within reach for the population, which complements the correct practice of brushing teeth. This study aimed to identify the practices and hygiene habits that influence the level of contamination of toothbrushes in Mexican homes using a survey and the quantification of colony-forming units (CFU) for indicator microorganisms in the samples selected from the survey.
2. Materials and Methods
2.1. Questionnaire
A convenient sampling of the snowball type via WhatsApp and e-mail was conducted following the guidelines of the Helsinki Declaration through informed consent. A Google Forms questionnaire was provided to people living in the Metropolitan Zone of Guadalajara, Jalisco, about routines, oral hygiene habits, and toothbrush handling in homes. Results were compiled in an Excel database with a total of 275 questionnaires received.
2.2. Sample Selection
Toothbrushes with at least 1 month of use from individuals that previously answered the survey “Oral hygiene habits: Handling and maintenance of toothbrush at home”, preferably belonging to distinct sex and age groups, and that were willing to donate their toothbrushes for use in the exploratory study were selected. A total of 23 samples were collected, and 18 were processed after exclusion criteria were applied.
2.3. Sample Collection and Processing
Owners of the toothbrushes could receive the results obtained in this study. The results will be available to the public, and to ensure patient privacy and personal data confidentiality, samples were coded as M1, M2, and so on.
Donated toothbrushes were processed on the day of collection. In the laboratory, data on sex and age were registered, and each brush was given a code. Each sample was put in a sterile bag with a hermetic seal (WhirlPack, S-19793, Kenosha, WI, USA), and 30 mL of nutrient broth were added. While closed, bags were finger massaged in order for the broth to penetrate all surfaces of the brushes. Finally, bags were incubated (Novatech, HS45-AIA, Guadalajara, Mexico) at 37 °C for 18–24 h.
2.4. Microbial Assessment
Previously coded samples were diluted in accordance with NOM-110-SSA1-1994 [13]. Calculations and corresponding mesophilic aerobic bacteria, coliforms, yeast, and mold colony counts were conducted according to the Mexican norms [14,15,16], respectively. Briefly, serial dilutions were made from sample bags in buffered peptone water (BPW), and 1 mL of each dilution was seeded by plate casting in different mediums: plate count agar (PCA) for mesophilic aerobic bacteria (MAC), violet red bile agar (VRBA) for total coliforms (TC), and potato dextrose agar (PDA) for yeast and molds (YM). Plates for MCA and TC were incubated at 36 °C and YM plates at 25 °C for 24–48 h (Novatech, HS45-AIA, Mexico), and colonies were counted on a colony counter (SOLBAR Q-20, Beracah médica, Guadalajara, Mexico). Plates were prepared in triplicate, and results were expressed as CFU/mL.
2.5. Statistical Analysis
Data obtained through the survey (a cross-sectional study from May–June 2021) were alphabetically coded in Excel in order to analyze the data statistically using Origin Pro 2020, utilizing the Ward and Manhattan methods to generate four conglomerates, each where samples were classified and correlated with hygiene practices. The chi-square test was applied to determine significant statistical differences in microorganism count (p < 0.05).
3. Results
A total of 275 questionnaires collected over 2 months were validated (188 women, 87 men), with ages ranging from 11–20 (47.6%), 21–30 (37.8%), 31–40 (1.5%), 41–50 (5.8%), 51–60 (4%), and >60 years old (2.5%). Table 1 compiles the general characteristics of participants’ knowledge about their buccal health and toothbrushing practices. Most of the population considers having a good buccal health state (61.5%), 24% stated that their medical visits are only once a year, and 33.1% mentioned that they only undergo in medical checks when feeling pain. Practices like the use of dental floss were not included since its use is low worldwide [17]. The guidelines of the American Dental Association (ADA) recommend that, for prevention and buccal disease control, doctor’s visits should total at least one per year.

Table 1.
Knowledge about health and toothbrushing practices.
Regarding the general overview of toothbrushing routines (Table 2), 41.8% of participants assure completing a routine in 2 min, while 38.9% mention that it should take more time. The ADA recommends using soft to medium bristles, which corresponds to most of the population when buying a toothbrush (medium 16.7% and soft 58.2%). Also, brush appearance is considered when acquiring a new toothbrush by 41.1% of participants, while 35.6% make purchases on the basis lf a professional prescription (35.6%); some participants buy considering brands (32.7%) or while others based on price (33.8). Finally, 44.4% of the people who participated in the survey replaced a toothbrush after three or more months, which impacts the innocuity and safety of this tool.
Table 2.
Knowledge about brushing routines and the types of toothbrushes.
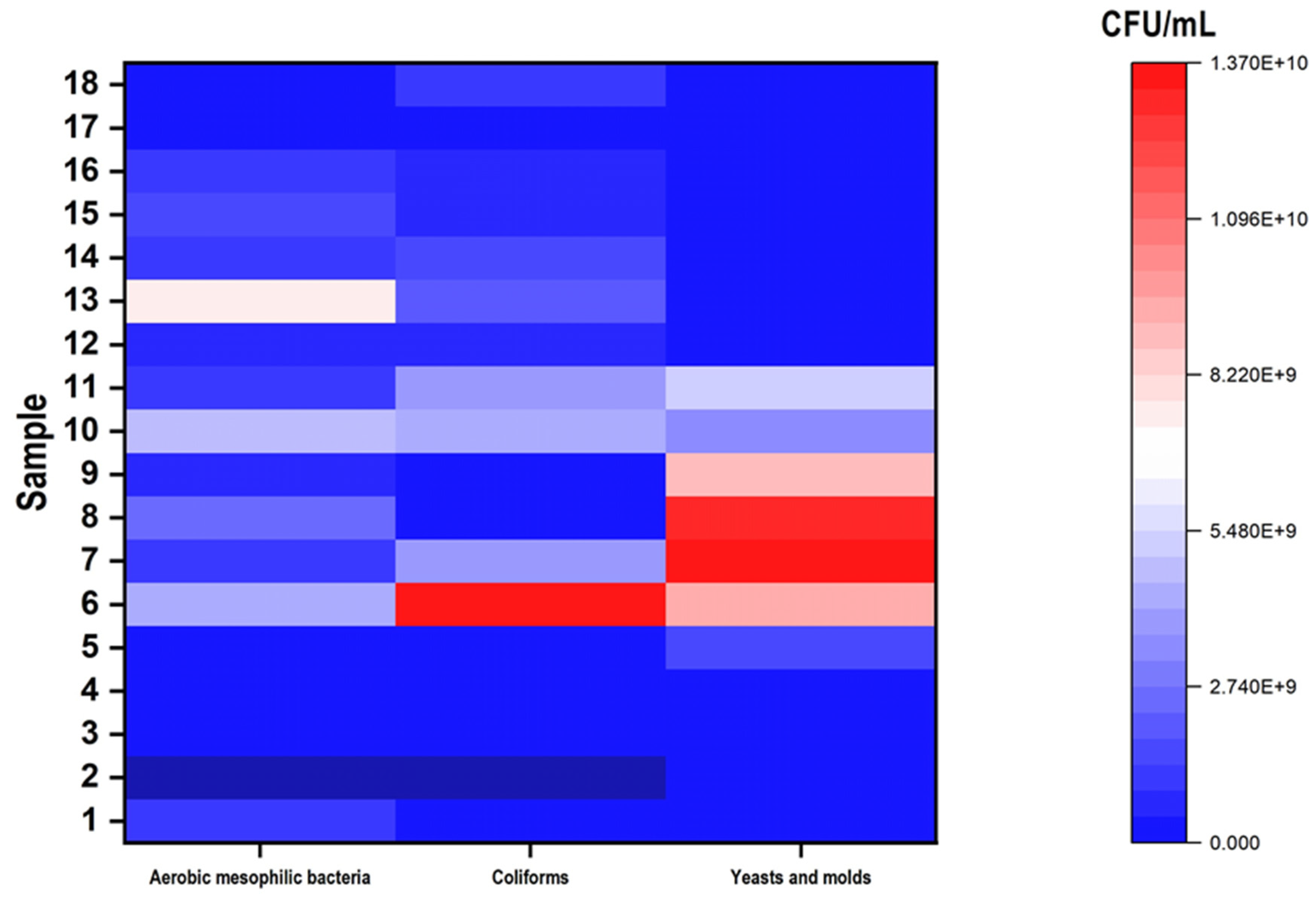
Among the surveyed individuals, 23 confirmed their donation, from which 18 toothbrushes were processed following the exclusion and inclusion criteria established for the study. When processing, dilutions were determined depending on the turbidity of the enrichment medium, which ranged from 4 to 8 dilutions. In Figure 1, samples 6–9 stand out with higher microbial counts compared to others (p < 0.05); samples 8 and 9 presented mesophilic aerobic bacteria of 4 × 108 and 2.7 × 109 CFU/mL, respectively, while total coliforms in sample 7 were of 4 × 109 CFU/mL, and yeast and molds for sample 6 were 9.2 × 109 CFU/mL. These counts were correlated with the answers to the survey for storage in cases, storage within at least 1 m from the toilet, and use for three months. Some studies suggest that following these recommendations helps reduce the development of microorganisms on toothbrushes.
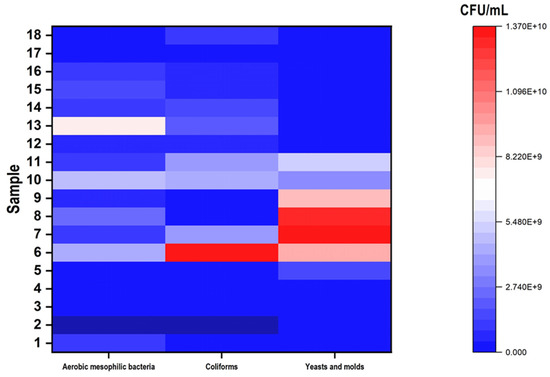
Figure 1.
Heat map of the CFU/mL plate count of indicator microorganisms in toothbrush samples.
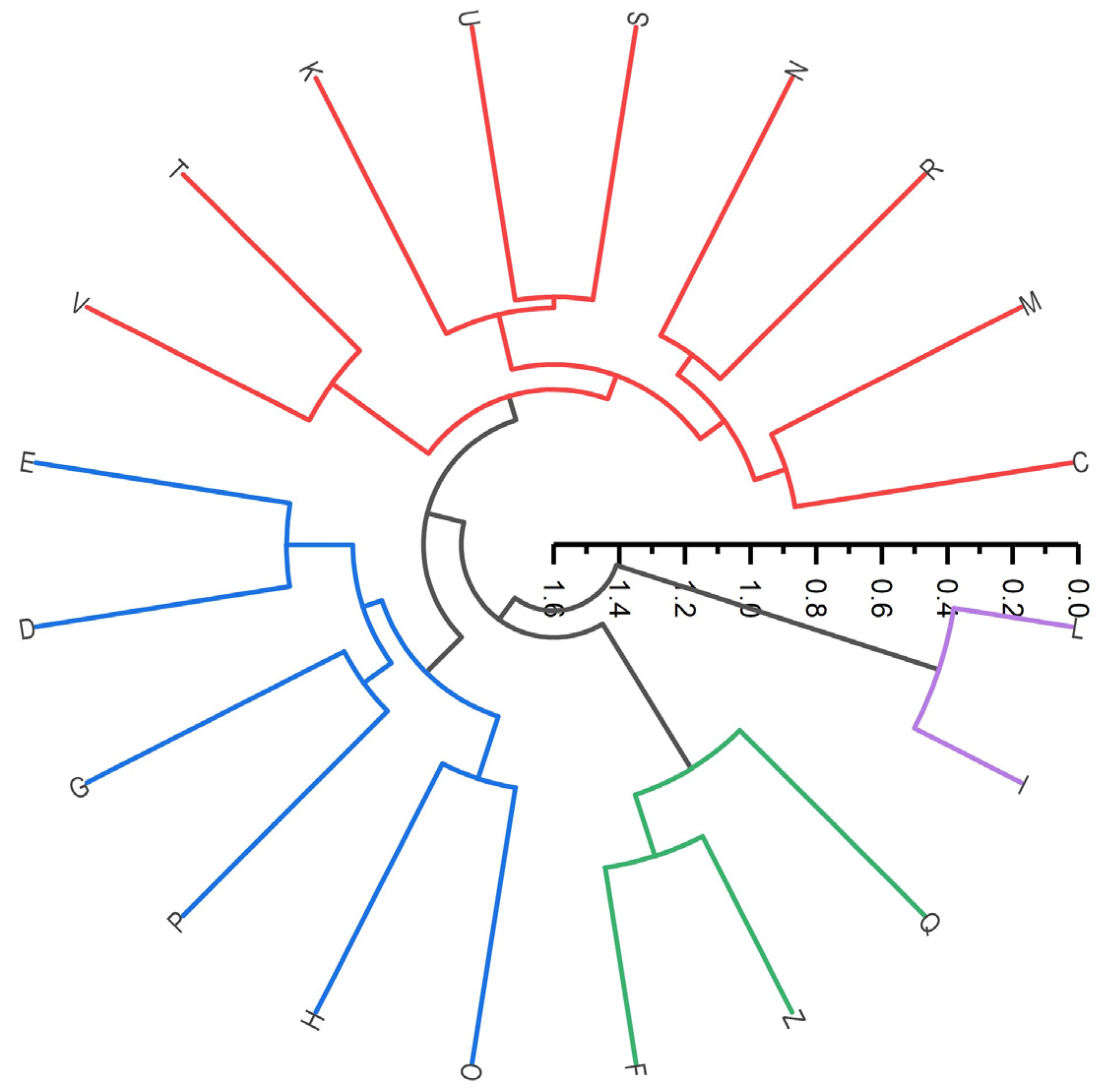
In order to establish a statistical analysis between people surveyed and toothbrushes analyzed, the Ward method and a cluster dendrogram were applied (Figure 2). The objective was to group surveyed in their corresponding conglomerate to relate the CFU count and determine the habits that significantly impact indicator microorganism counts in toothbrushes.
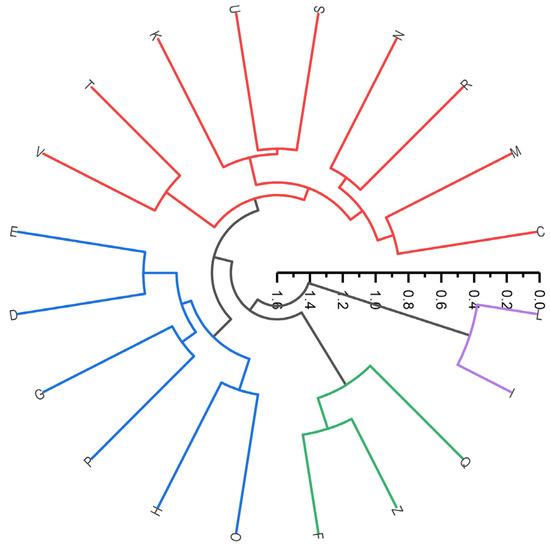
Figure 2.
Dendrogram-predicted samples using the Ward and Manhattan methods. Different colors represent different storage habits of toothbrushes.
Among samples in conglomerate 1, it is worth mentioning sample 12 (blue cluster in Figure 2) since it was the only one in the cluster that mentioned the storage of its toothbrush inside a protective case, developing a higher count of coliforms compared to the other samples in the cluster. In the second group, the green cluster, sample 3, did not present a coliform, yeast, or mold count, which could be attributed to the fact that the participant was the only one to change his toothbrush before the recommended three months, while the rest of the group exceeded this time. For the red cluster (third conglomerate), samples 4 and 17 presented a lower CFU/mL count; this could be because the toothbrushes were stored inside a drawer in the bathroom, which avoids exposure to microorganism contamination. Samples 5, 8, and 9 (Figure 1) exhibited a high yeast and mold count, probably related to the use of protective cases. Lastly, samples 4, 9, and 17 mentioned a process to disinfect their brushes; for example, sample 17 applied sodium bicarbonate and vinegar after every use. Despite the low microbial count of coliforms, yeast, and molds, the mesophilic bacteria count was high. In the last conglomerate (purple), one main contributing factor was age since the sample was declared to be older than 60 years, and the coliform count was high.
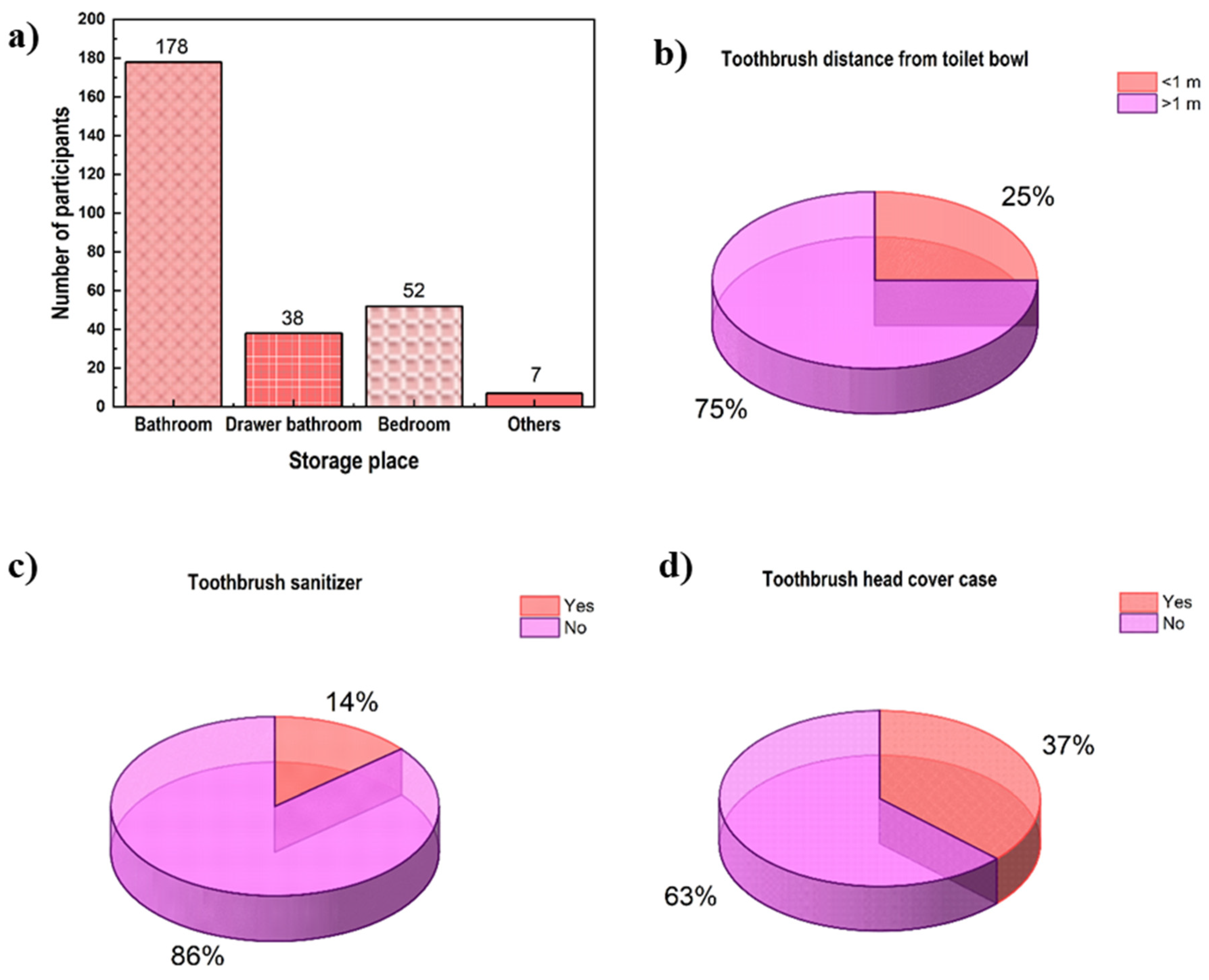
The environment where the toothbrush is located has a direct impact on bacterial counts. Considering this, among the surveys, 178 participants stored their toothbrushes in the bathroom near the sink (Figure 3a) and 75% of these at a distance lower than 1 m from the toilet (Figure 3b). On the other hand, 37% of the total population also mentioned that they keep their brushes in cases both near and far from the toilet (Figure 3d), and a small sample indicated that they disinfect their toothbrushes (14%), as seen in Figure 3c. There is a major concern about microorganisms in toothbrush storage in protective cases, while a lower count is related to use for the recommended life expectancy of three months compared with prolonged use.
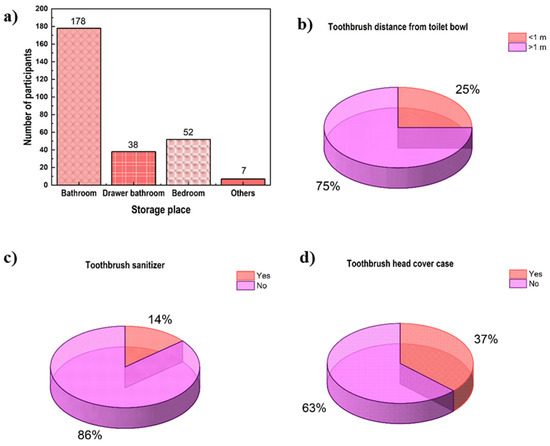
Figure 3.
Hygiene practices from the Mexican population: (a) storage place of toothbrushes, (b) toothbrush distance from toilet, (c) use of toothbrush sanitizer, and (d) use of a head cover case.
In this study, it was highlighted that most people do not have the habit of disinfecting their toothbrushes (86%, Figure 3c). Surveys revealed that disinfection techniques are improvised and not standardized to completely disinfect the brush.
4. Discussion
Toothbrushing is a common activity used to prevent buccal infections, and different recommendations include replacing toothbrushes within a maximum period of three months. Some of the pathogens that can be found in toothbrushes used for more than 3 months include Klebsiella pneumoniae, Streptococcus pyogenes, Pseudomonas, Candida, Escherichia coli, and Staphylococcus aureus [18,19]. Other microorganisms found in toothbrushes include Micrococcaceae, Actinomycetaceae, and Streptococcaceae, whose occurrence depends on the period of use [20]. Not only may these pathogens be present, but it has been recorded that poor oral hygiene procedures may induce cardiovascular disease since periodontal pathogens can infiltrate the circulatory system through injuries in the mouth [21]. Other chronic pathologies associated with poor oral hygiene include cystic fibrosis [22]. Also, it has been reported that some pathogens that colonize toothbrushes may express antimicrobial resistance genes, which can lead to health complications if those microorganisms infiltrate the circulatory system [23].
Confirmed etiologic agents of adults (age > 40 years) that are responsible for the microbial charge, among others, are Actinobacillus, Campylobacter, Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola [24], which can be related to illness, nutritional habits, or the use of prostheses and dental implants. It should be noted that a hazard associated with contamination is the relationship between periodontal disease and cancer, where typical microorganisms include Fusobacterium nucleatum, Prevtella intermedia, Campylobacter rectus, Porphyromonas gingivalis, and Tannerella forsythia. Fusobacterium has been found in the oral cavity, estimating high concentrations in colorectal tumors and being associated with carcinogenesis [25]. Such is the case of patients with pancreatic cancer where elevated oral cavity bacterial counts were found. These pathogens could travel through the circulatory system when the periodontium is weakened, facilitated during chewing, or with bad toothbrushing.
It has been reported that the increase in the count of mesophilic bacteria, coliforms, and S. aureus is time-dependent on toothbrushes. Over a 3-month period, S. aureus can grow 10-fold/month on toothbrush bristles [26]. Contamination of toothbrushes is mainly associated with oral hygiene and the environment, whether or not users follow specific instructions on how to use and store toothbrushes [27].
Dayoub et al. [28] found that toothbrushes in cases exposed to contaminated surfaces have higher counts than those exposed without cases. A wet environment favors yeast development, like Candida species, responsible for candidiasis disease. Most studies focus mainly on bacteria, and overlook yeast and molds, which are likely to grow in toothbrush cases. Being a favorable environment for the growth of C. albicans, toothbrush cases may be considered a risk for immunocompromised patients [29,30]. Environmental and human microbiomes can interact at a common site, such as toothbrushes, which, in combination with bathroom features, personal health, and dental hygiene, can lead to antimicrobial resistance development [23].
Karibasappa et al. [31] mentioned that it is impossible to completely decontaminate toothbrushes in this type of environment, where it is recommended to submerge them in antibacterial solutions after each use. In this study, homemade disinfection practices like a combination of vinegar and sodium bicarbonate were applied; even though it is a process that is gaining popularity, the neutralization of the ingredients should be considered. Cooking vinegar alone can only inhibit some bacteria, while pathogens and parasites, like Taenia solium, are probably not affected [32]. Other solutions applied are formulations of activated carbon or chlorhexidine, which have been demonstrated to reduce bacterial counts in toothbrush samples [6]. Some microorganisms can secrete polysaccharides to form a biofilm that protects them from harmful agents, and thus, it is necessary to address not only microorganism inhibition but also biofilm inhibition. Chemical-based products with chloroxylenol can inhibit 95% of bacterial counts like Escherichia coli [27] and Streptococcus mutans [33], while plant essential oils of clove, oregano, and thyme have been tested against bacteria and biofilm, proving to be effective in both cases [34]. Other procedures for toothbrush disinfection include steam disinfection, which has proven to completely eradicate cystic fibrosis pathogens [22]. In this sense, the use of disinfectant products that contain essential oils should be encouraged to prevent pathogen growth and protect toothbrushes, since natural products are of great interest nowadays. For this, it is necessary to bring about collective education regarding storage practices and disinfection processes, emphasizing the importance of the use and sanitization of toothbrushes for public health. Finally, it is essential to conduct studies that include more subjects to better determine the relationships between toothbrushes and their contaminants.
5. Conclusions
Indicator microorganism counts from toothbrushes are higher when kept in a cover case. Use and disposal following life expectancy recommendations limits microorganism growth. Also, most people do not have the habit of periodically disinfecting their toothbrushes. The survey revealed that disinfection techniques applied by this section of the population are typically improvised and unstandardized. Higher counts may lead to bacteremia and even cardiovascular disease, for which it is recommended to follow specialist indications to avoid the contraction of these microorganisms. For these, a further study using different natural antibacterial solutions, such as polyphenols or monoterpenes, and comparing them with traditional antiseptic substances in order to promote a safe disinfection alternative should be conducted. Other new prospects may include elaborating toothbrushes with intelligent materials that provide innocuity and, at the same time, are environmentally friendly. Lastly, it is important to promote a hygiene habit culture focused on toothbrush use and handling to limit the growth of microorganisms that indicate contamination and can be harmful to people’s health. With this, the periodic disinfection of toothbrushes is a procedure that should be implemented, considering correct application, in order to minimize systemic diseases that impair the quality of life. So far, this is the first study that correlates oral hygiene practices in Latin American homes, mainly in Mexico, and microorganism counts, for which it is recommended to provide more insight on the topic.
Author Contributions
Conceptualization, L.E.G.-M.; methodology, A.O.B.-C., A.L.R.-C. and S.G.U.-P.; software, J.M.S.-J., C.A.V.-C.; validation, A.O.B.-C., A.L.R.-C., S.G.U.-P. and L.E.G.-M.; formal analysis, L.E.G.-M., C.A.V.-C. and J.M.S.-J.; investigation, C.A.V.-C. and J.M.S.-J.; resources, L.E.G.-M., B.V.-R. and J.M.S.-J.; data curation, L.E.G.-M. and J.M.S.-J.; writing—original draft preparation, L.E.G.-M. and J.M.S.-J.; writing—review and editing, C.A.V.-C. and B.V.-R.; visualization, J.M.S.-J.; supervision, L.E.G.-M., C.A.V.-C. and B.V.-R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of CUValles/UDG.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Acknowledgments
The authors acknowledge the support from the Universidad de Guadalajara for the technical assistance during the completion of this work.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Shang, Q.; Gao, Y.; Qin, T.; Wang, S.; Shi, Y.; Chen, T. Interaction of oral and toothbrush microbiota affects oral cavity health. Front. Cell Infect. Microbiol. 2020, 10, 17. [Google Scholar] [CrossRef] [PubMed]
- Schmalz, G.; Feindt, L.; Tanneberger, F.; Haak, R.; El Wahed, A.A.; Truyen, U.; Ziebolz, D. The role of toothbrush in the transmission of corona-and influenza viruses—Results of an in vitro study. Clin. Oral Investig. 2022, 26, 5741–5749. [Google Scholar] [CrossRef] [PubMed]
- Potlia, I.; Singh, P.; Chauhan, H.; Malhotra, S.; Tandon, P.; Srivastava, A.P. Knowledge attitude and practice of dentists regarding toothbrush hygiene and disinfection in private cental colleges of Lucknow City India: A Cross-sectional Study. Int. J. Clin. Pediatr. Dent. 2022, 15, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Frazelle, M.R.; Munro, C.L. Toothbrush contamination: A review of the literature. Nurs. Res. Pract. 2012, 2012, 420630. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Baptist, J.; Bhat, S.; Ongole, R.; Natarajan, S. Assessment of tooth brush microbial contamination in dental health care providers: An investigative cross-sectional study. J. Indian Acad. Oral Med. Radiol. 2023, 35, 226–230. [Google Scholar] [CrossRef]
- Khan, S.A.; Syed, F.A.; Khalid, T.; Farheen, N.; Javed, F.; Kazmi, S.M.R. An updated systematic review on toothbrush contamination: An overlooked oral health concern among general population. Int. J. Dent. Hyg. 2024, 22, 95–105. [Google Scholar] [CrossRef]
- Patel, M. Oral cavity and Candida albicans: Colonisation to the development of infection. Pathogens 2022, 11, 335. [Google Scholar] [CrossRef] [PubMed]
- Benn, A.M.; Heng, N.C.; Thomson, W.M.; Sissons, C.H.; Gellen, L.S.; Gray, A.R.; Broadbent, J.M. Associations of sex, oral hygiene and smoking with oral species in distinct habitats at age 32 years. Eur. J. Oral Sci. 2022, 130, e12829. [Google Scholar] [CrossRef]
- Martins, C.C.; Lockhart, P.B.; Firmino, R.T.; Kilmartin, C.; Cahill, T.J.; Dayer, M.; Occhi-Alexandre, I.G.P.; Lai, H.; Ge, L.; Thornhill, M.H. Bacteremia following different oral procedures: Systematic review and meta-analysis. Oral Dis. 2023. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Arcos-Pulido, M.D.P.; Ávila-de Navia, M.S.C.; Lilia, S.; Torres, E.; Mónica, S.; Gómez-Prieto, A.C. Microbiological Indicators of Contamination of the Water Sources; Universidad Colegio Mayor de Cundinamarca: Bogotá, Colombia, 2005; Volume 3. [Google Scholar] [CrossRef]
- Fout, G.S.; Borchardt, M.A.; Kieke, B.A., Jr.; Karim, M.R. Human virus and microbial indicator occurrence in public-supply groundwater systems: Meta-analysis of 12 international studies. Hydrogeol. J. 2017, 25, 903–919. [Google Scholar] [CrossRef]
- Richiardi, L.; Pignata, C.; Fea, E.; Bonetta, S.; Carraro, E. Are indicator microorganisms predictive of pathogens in water? Water 2023, 15, 2964. [Google Scholar] [CrossRef]
- NORMA Oficial Mexicana. NOM-110-SSA1-1994. Bienes y Servicios. Preparación y Dilución de Muestras de Alimentos Para su Análisis Microbiológico; Diario Oficial de la Federación DV: Ciudad de México, Mexico, 1994; Volume 11, p. 16. Available online: https://www.dof.gob.mx/nota_detalle.php?codigo=4728921&fecha=15/08/1994#gsc.tab=0 (accessed on 5 November 2023).
- NORMA Oficial Mexicana. NOM-092-SSA1-1994. Bienes y Servicios. Método Para la Cuenta de Bacterias Aerobias en Placa; Diario Oficial de la Federación: Ciudad de México, Mexico, 1994; Volume 12, Available online: https://dof.gob.mx/nota_detalle.php?codigo=4886029&fecha=12/12/1995#gsc.tab=0 (accessed on 5 November 2023).
- NORMA Oficial Mexicana. NOM-113-SSA1-1994, Bienes y Servicios. Método Para la Cuenta de Microorganismos Coliformes Totales en Placa; Diario Oficial de la Federación: Ciudad de México, Mexico, 1995; Available online: https://www.fao.org/faolex/results/details/es/c/LEX-FAOC013519/ (accessed on 5 November 2023).
- NORMA Oficial Mexicana. NOM-111-SSA1-1994, Bienes y Servicios. Método Para la Cuenta de Mohos y Levaduras en Alimentos; Diario Oficial de la Federación: Ciudad de México, Mexico, 1994; Available online: https://dof.gob.mx/nota_detalle.php?codigo=4881226&fecha=13/09/1995#gsc.tab=0. (accessed on 5 November 2023).
- Luo, T.; Beiter, K.; Tseng, T.S. Association between acculturation, dental floss use, dental visits and unmet dental needs among Asians in the United States: Findings from National Health and Nutrition Examination Survey (NHANES) 2011–2018. Community Dent. Oral Epidemiol. 2024, 52, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Raiyani, C.M.; Arora, R.; Bhayya, D.P.; Dogra, S.; Katageri, A.A.; Singh, V. Assessment of microbial contamination on twice a day used toothbrush head after 1-month and 3 months: An in vitro study. J. Nat. Sci. Biol. Med. 2015, 6 (Suppl. S1), S44–S48. [Google Scholar] [CrossRef] [PubMed]
- Ralephenya, T.R.; Molepo, J.; Molaudzi, M.; Volchansky, A.; Shangase, S.L. Contamination of used toothbrushes and their decontamination with disinfecting agents. S. Afr. Dent. J. 2020, 75, 478–484. [Google Scholar] [CrossRef]
- Zinn, M.K.; Schages, L.; Bockmühl, D. The toothbrush microbiome: Impact of user age, period of use and bristle material on the microbial communities of toothbrushes. Microorganisms 2020, 8, 1379. [Google Scholar] [CrossRef] [PubMed]
- Pardo, A.; Signoriello, A.; Signoretto, C.; Messina, E.; Carelli, M.; Tessari, M.; De Manna, N.D.; Rossetti, C.; Albanese, M.; Lombardo, G.; et al. Detection of periodontal pathogens in oral samples and cardiac specimens in patients undergoing aortic valve replacement: A pilot study. J. Clin. Med. 2021, 10, 3874. [Google Scholar] [CrossRef]
- Millar, B.C.; Maguire, M.; Moore, R.E.; Murphy, A.; McCaughan, J.; Stirling, J.; Moore, J.E. Steam disinfection of toothbrushes from patients with cystic fibrosis: Evidence-based recommendations. Pediatr. Pulmonol. 2020, 55, 3012–3020. [Google Scholar] [CrossRef]
- Blastein, R.A.; Michelitsch, L.M.; Glawe, A.J.; Lee, H.; Huttelmaier, S.; Hellgeth, N.; Maamar, S.B.; Hartmann, E.M. Toothbrush microbiomes feature a meeting ground for human oral and environmental microbiota. Microbiome 2021, 9, 1–14. [Google Scholar] [CrossRef]
- Zawadzki, P.J.; Perkowski, K.; Padzik, M.; Mierzwińska-Nastalska, E.; Szaflik, J.P.; Conn, D.B.; Chomicz, L. Examination of oral microbiota diversity in adults and older adults as an approach to prevent spread of risk factors for human infections. Biomed. Res. Int. 2017, 8106491. [Google Scholar] [CrossRef]
- Mai, X.; Genco, R.J.; LaMonte, M.J.; Hovey, K.M.; Freudenheim, J.L.; Andrews, C.A.; Wactawski-Wende, J. Periodontal pathogens and risk of incident cancer in postmenopausal females: The buffalo osteoperio study. J. Periodontol. 2016, 87, 257–267. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, D.; Kim, H.S.; Baik, J.Y.; Ju, S.H.; Kim, S.H. Analysis of microbial contamination and antibacterial effect associated with toothbrushes. J. Dent. Hyg. Sci. 2018, 18, 296–304. [Google Scholar] [CrossRef]
- Joy, T.; Venugopal, S.; Sadanandan, S.; Mathew, M. Evaluation of microbial contamination of toothbrushes and their decontamination using various disinfectants: An in vitro study. J. Indian Assoc. Public Health Dent. 2022, 20, 200–205. [Google Scholar] [CrossRef]
- Dayoub, M.B.; Rusilko, D.; Gross, A. Microbial contamination of toothbrushes. J. Dent. Res. 1977, 56, 706. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, A.P.; Watanabe, E.; Ito, I.Y. Toothbrush contamination by Candida spp. and efficacy of mouthrinse spray for their disinfection. Mycopathologia 2010, 169, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Mobin, M.; Borba, C.D.M.; Tapety, F.I.; Noleto, I.D.; Teles, J. Analysis of fungal contamination and disinfection of toothbrushes. Acta Odontol. Latinoam. 2011, 24, 86–91. [Google Scholar] [PubMed]
- Karibasappa, G.N.; Nagesh, L.; Sujatha, B.K. Assessment of microbial contamination of toothbrush head: An in vitro study. Indian J. Dent. Res. 2011, 22, 2. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Mohanty, S.; Kadanthode, M.; Kumar, P. Review of cysticercosis of maxillofacial region and report of two cases. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e760–e769. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Kunte, S.; Jagtap, C.; Jajoo, S.; Patel, A.; Shah, P. Efficacy of two different mouth rinses in inhibition of the growth of Streptococcus mutans on toothbrush bristles. J. Dental Res. Rev. 2021, 8, 261–266. [Google Scholar]
- Aires, A.; Barreto, A.S.; Semedo-Lemsaddek, T. Antimicrobial effects of essential oils on oral microbiota biofilms: The toothbrush in vitro model. Antibiotics 2021, 10, 21. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).