Abstract
Suicide is a leading cause of mortality and a recognized public health priority. In the last two decades, older adults (age 65 and older) saw the largest percentage increase in suicide rates. Despite these rising trends, geriatric suicide remains an understudied public health crisis. In this review, we summarize risk factors specific to geriatric suicide using a socioecological framework and the Interpersonal Theory of Suicide of burdensomeness and belongingness. Specifically, we categorize these risk factors into individual, interpersonal, organizational, and policy levels. For each type of risk factor, we review prevention and intervention programs that can help mitigate the risk of suicide among older adults. Some strategies we discuss include early detection, comprehensive healthcare approaches, community-based support systems, and legislative and policy solutions. The paper underscores the need for increased awareness and more targeted research to address the unique challenges faced by the aging population to provide more informed support and prevent suicide mortality.
1. Introduction
Suicide is recognized by the World Health Organization as a public health priority and remains one of the leading causes of death across all age groups [1]. In the United States, age-adjusted suicide rates rose from 10.4 per 100,000 in 2000 to 14.2 in 2023, a 37% increase over 23 years. This increase has been disproportionately higher among older individuals. Among women aged 65 and above, suicide rates increased by 44% between 2000 and 2021 [2]. From 2021 to 2022, there was an 8% increase in deaths by suicide among individuals 65 and above; in 2023, the rate remained nearly similar to 2022, declining by 0.01% [3]. In the years 2021 and 2022, individuals aged 75 and older had the highest suicide rate among all age groups. In 2019, older adults (individuals over the age of 65) formed 16.5% of the American population, but represented more than 19.4% of deaths by suicide [4]. This number may be an underestimation, due to a lack of appropriate reporting and the presence of silent suicides (including discontinuation of medications) [5]. Similarly, globally, suicide rates increase significantly with age, reaching nearly three times the age-standardized suicide mortality rate for all ages combined. At the same time, regional differences in these trends have also been observed. As an example, South Korea has seen a tripling in the rate of suicide among the elderly from 1990 to 2005, triggering economic reforms and restriction of access to lethal means to mitigate the rates. Sri Lanka, on the other hand, has seen a sharp fall in suicide mortality rate among the elderly following restriction of access to pesticides. Similarly, China has seen a reduction in suicide rates across all age groups, with the decline among the elderly being the smallest. In North Africa, the Middle East, and Latin America, suicide mortality rates continue to be low, likely secondary to religious beliefs and familial attitudes [5,6]. Over the next 20 years, it is anticipated that the population of older adults will increase by approximately 47% in the US [7] and double over the next 30 years globally. As the aging population continues to grow and social dynamics shift, the rising trend of suicide among the elderly becomes critical to understand.
To address this trend, it is vital to understand the underlying risk factors and to explore effective prevention strategies. In this review, we discuss some of these driving forces of suicide. Specifically, we use a socioecological framework to understand and contextualize underlying risk factors. We also build on the Interpersonal Theory of Suicide, to further examine the intersection of risk factors and concepts of perceived burdensomeness and thwarted belongingness. Finally, we build on this understanding and propose potential solutions to mitigate these risk factors and thus reduce suicidality among the elderly.
2. Method
Multiple theoretical models have been developed to explain suicidality, spanning a wide range of constructs. These include sociological models such as Durkheim’s social integration model [8]; psychological models by Freud and Menninger, which view suicide as aggression turned inward and as an escape from psychache [9]; cognitive models emphasizing hopelessness and escape [10]; interpersonal models that focus on belongingness and burdensomeness [11]; the stress–diathesis model which highlights vulnerability–stress interactions [12]; socioecological models that situate suicide within multilevel systems [13]; and Shneidman’s cubic model, which conceptualizes suicide as the intersection of psychache (intolerable psychological pain), press (life stress), and perturbation (cognitive or emotional disturbance) [14].
For this review, we chose to integrate Joiner’s Interpersonal Theory of Suicide and the Socioecological Model [11]. We specifically chose these two frameworks as they provide a complementary lens for understanding late-life suicide. The Interpersonal Theory offers a clinically useful explanation of the psychological drivers of suicidality (thwarted belongingness and perceived burdensomeness) from an individual perspective, while the socioecological model explains these individual experiences within broader social, organizational, and policy contexts. Taken together, the two models thus help bridge psychological mechanisms with overarching structural and public health determinants. This allows for a more holistic understanding of suicide in older adults, which in turn can help critically evaluate multilevel prevention strategies spanning clinical, community, and systemic domains. Furthermore, the “chrono” or time element in the socioecological model also allows for an understanding of the evolution of the factors over time, potentially providing some theories about the trend over time.
The socioecological framework is a widely used public health model that explains health outcomes under the umbrella of multiple nested systems—micro, meso, exo, macro and chrono—all of which interact with each other to influence individual health outcomes [13]. These systems encompass the individual’s immediate environment (micro) including interpersonal elements of family, neighborhoods and interaction between the various micro systems (meso) and spread out to include various components of the social environment such as community and other organizations and policy (exo), societal attitudes and culture (macro) and finally changes over time (chrono) thus providing a great depth of intersectional factors. This model allows for a deep understanding of each of the layers and also discusses a complex interplay between these nested layers, which is dynamic and changes over time.
A second widely used framework for understanding suicidality is Joiner’s Interpersonal Theory of Suicide. This theory posits that “an individual will not die by suicide, unless he (she) has both the desire to die as well as the ability to do so” [11,15]. The desire to die arises from two core psychological states: perceived burdensomeness and thwarted belongingness (a low sense of belonging or social alienation). Perceived burdensomeness may develop from distressing circumstances such as chronic illness, disability, or unemployment, where individuals come to view themselves as a liability to others, often accompanied by self-directed hostility. This belief can crystallize into the perception that one’s death would benefit loved ones more than one’s continued existence. Thwarted belongingness, in contrast, reflects a lack of meaningful connection or integration into social groups. It may manifest as loneliness, isolation, or the sense of having “no one to turn to”—all of which are robust predictors of suicidal behavior. These two psychological states interact to generate suicidal desire. However, desire alone is insufficient: suicide attempts become more likely when coupled with acquired capability, which involves habituation to pain, lowered fear of death, and access to lethal means. Together, these elements explain how the convergence of psychological distress and increased capability can culminate in suicide attempts.
In the following discussion, we will use the socioecological framework and discuss how the various nested systems can influence perceived burdensomeness and a sense of belongingness thus shaping the risk of suicide among the elderly. This review employed an integrative review approach with systematic elements to synthesize empirical and theoretical literature relevant to the socioecological model, which was subsequently integrated with the Interpersonal Theory. A comprehensive Google Scholar and PubMed search was conducted for articles published between January 2000 and March 2025. Eligible studies were peer-reviewed empirical or review articles published in English and focused on the elderly population. We specifically examined studies addressing predetermined risk factors informed by the socioecological model, including:
- Individual-level factors: sociodemographic characteristics, physical health conditions, and psychiatric/psychological conditions.
- External factors (micro, meso, exo, macro and chrono): interpersonal relationships, organizational influences, policy-related determinants, societal and cultural factors.
Our specific search terms included:
Population/Subject terms: “older adult”, “geriatric”, “elderly”, “aging”, “older population”, “late-life”, “age groups”;
Outcome and topic terms: “suicide”, “mental health”, “depression”, “late-life suicide prevention”, “interpersonal/community/societal interventions”, “prevention strategies”, “older adult mortality”, “protective factors”, “suicide rates”, “hopelessness”, “resilience”, “suicidal ideation”, “counseling”, “therapy”, “group activities”, Risk factor terms: “social isolation”, “loneliness”, “social support”, “isolation”, “burdensomeness”, “physical illness”, “physical comorbidity”, “chronic illness”, “cognitive”, “adverse life experience”, “substance use disorder”, “mental health”, “anxiety/depression/suicidality”, “psychiatric disorders”, “alcohol use”, “lethal means”, “access to lethal means”, “access to firearms”, “financial stress”, “food insecurity”, “autonomy”, “medication”, “access to healthcare”, “pandemic”, “COVID-19”, “systemic factors”, “socioeconomic status”, “means restriction”.
In addition, we reviewed prevention and intervention strategies targeting these categories. Articles were excluded if they were conference abstracts, editorials, or commentaries without empirical data.
Study Selection and Data Synthesis
Search results were screened in two stages. First, titles and abstracts were reviewed to determine relevance to suicide among the elderly. Second, full-text screening was performed to confirm eligibility. Data were then extracted on population characteristics, identified risk factors, and intervention/prevention strategies. Findings were then synthesized narratively, mapping risk and protective factors to the socioecological framework and finally insights from Interpersonal Theory were integrated to highlight intersectional themes.
3. Risk Factors
Figure 1 presents an integrated model of risk factors utilizing the Socioecological Model. At the center of the circle are individual characteristics associated with suicidal ideation among elderly individuals, including sociodemographic characteristics, physical health, psychiatric conditions and psychological determinants. The second (microsystem) level explores factors related to social isolation and loneliness, while the meso level is related to interactions between the various factors in the microsystem level. The exo level highlights policies and organizational issues, which macro or the cultural system reflects societal values and ageism. Finally, the most outward system, chrono highlights changes in these systems over time, which may all be associated with changes in perceived burdensomeness, feelings of belongingness and with the rising trends in suicide among the elderly.
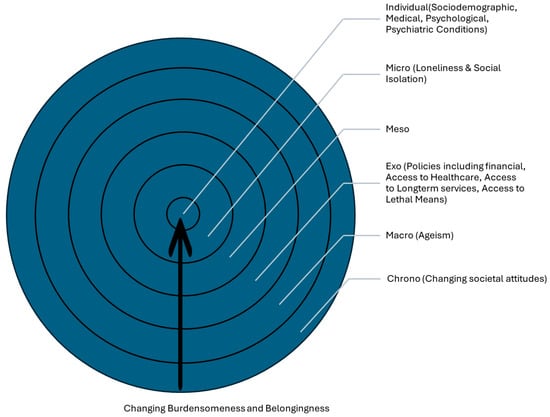
Figure 1.
Risk factors illustrated in Bronfenbrenner’s Socioecological Model.
3.1. Individual Factors
3.1.1. Sociodemographic Factors
Suicide risk among older adults is influenced by a range of individual factors—both static and dynamic. Among static risk factors, gender, and race play a significant role [10]. Among all age groups, men have a greater risk of death by suicide, while females have greater risk of suicide attempts. Among older adults, this gender disparity is heightened for suicide deaths, being approximately 2.5 times higher among males than females. This increased disparity may be driven by greater longevity among females, greater financial problems, informal caregiving role and traditional societal stereotypes all of which can worsen perceived burdensomeness. For suicide attempts, on the other hand, the disparity is reduced, with males having a similar risk of attempts as females [16]. Furthermore, white males have a significantly higher suicide rate as compared to their Hispanic or Latino, Asian or Pacific Islander, and African American or Black counterparts [17,18]. Variability in resilience and social support driven by racial and cultural differences may be associated with some of the observed disparities in suicide rates among older adults [19]. Living alone or recently widowed status heightens the risk of both suicide attempts and deaths by suicide, while residing with family lowers the risk [16].
Social status and income have been identified as important risk factors for suicide among the elderly [10]. Poor financial situations can exacerbate the experience of hopelessness and a sense of burdensomeness to others, a central component of the Interpersonal Theory of Suicide [11,15]. Among the elderly population, active income from employment falls, and financial security shifts to the safety net of retirement and Medicare. Studies have shown that these safety nets can be distressed when there are catastrophic health events, which in turn may be associated with feelings of high perceived burdensomeness. Indeed, more than half the older adults who went on to end their lives reported experiencing financial stressors in the six months leading to their deaths [20]. Particularly among older Asian adults, individuals in debt experienced greater depression and individuals with several debts reported more frequent suicide ideation [21]. Financial instability is also related to food insecurity; those experiencing food insecurity are more than five times more likely to attempt suicide than their food-secure counterparts [19,22].
3.1.2. Cognitive and Physical Health Issues
Aging is associated with a myriad of cognitive and physical health issues, all of which are associated with feelings of burdensomeness and loss of autonomy. Cognitive impairment, including dementia, has been identified as a potential risk factor for suicide among older adults, particularly in the early stages. Individuals with dementia have an approximately 53–54% higher risk for suicide compared to those without dementia (studies from Korea and USA), reflecting a global observation [23,24]. Furthermore, cognitive deficits in older adults are strongly associated with more lethal suicide attempts [25]. Risk of death by suicide is highest particularly in the early stages of Alzheimer’s, then decreases [24,26]. The early stages of cognitive decline may be associated with persistent hopelessness and heightened feelings of present or future burdensomeness. Furthermore, impulsive aggression and lack of cognitive flexibility with limited ability to identify alternative solutions can lead to increased vulnerability to suicidal behaviors during a suicidal crisis [26].
Similar to cognitive deficits, serious physical illnesses have been shown to predict suicide risk in older adults, with risk increasing in concert with the total number of medical comorbidities [27,28,29,30,31,32,33]. Older adults are more likely to have chronic medical conditions, including cardiovascular conditions, pulmonary conditions, gastrointestinal and renal disorders, neurological conditions, musculoskeletal conditions, vision- and hearing-loss, cancer, and pain [30]. Studies have noted that the risk of deaths by suicide is correlated with the number of health systems affected by a disease, with risk increasing as more health systems are involved [16]. Cardiovascular conditions such as congestive heart failure [31], respiratory conditions such as chronic obstructive pulmonary disease, neurological conditions such as seizure disorders and stroke, and urinary incontinence have been associated with an increased risk of suicide [10,31,32]. Beyond medical conditions, chronic pain plays a critical role in suicidality among older adults; the risk varying with type, and severity of pain, and presence of comorbid conditions including mental illnesses [33,34,35,36,37]. The relationship between physical pain and depression is bidirectional, leading to a vicious cycle [38]. Studies have found that painful conditions, such as arthritis, musculoskeletal issues, and headaches, are frequently reported among older adults who died by suicide [33,34,35,36,37]. Painful physical health conditions are likely to be associated with a more severe level of disability and loss of autonomy, which in turn is related to perceived burdensomeness. Furthermore, discomfort caused by the pain can moderate the association.
Cancer further elevates suicide risk in older adults, independent of other medical comorbidities and factors for suicide. Studies have consistently noted that males 65 years or older with lung, pancreatic, head and neck, or prostate cancer have a higher risk of suicide, with men with prostate cancer having a 4.24 times higher risk of suicide compared to their cohort [39]. The risk of death by suicide is greatest within a year after cancer diagnosis [40,41], highlighting a similar pattern of higher suicide death rates during the early stage of Alzheimer’s. The emotional impact and awareness of diagnosis, as well as perceived potential loss of autonomy and perceived burdensomeness likely act as underlying risk factors among these individuals [42].
3.1.3. Psychiatric Disorders
Psychiatric disorders, particularly depression and anxiety disorders have the strongest association with risk of suicide attempts and suicide deaths [20,43,44,45,46,47,48]. A recent suicide attempt or self-harm behavior is one of the strongest predictors of deaths by suicide, particularly among the elderly where the transition from suicidal behavior to attempt is frequent [48]. In the US, in 2021, approximately 11.5 percent of adults ages 65 and older were estimated to meet diagnostic criteria for any mental illness (AMI) in the past year [49]. Major depressive disorder, generalized anxiety disorder, and substance use disorder, including alcohol use, have been associated with a suicide mortality rate exceeding ten times that of individuals without these conditions [43]. Major depressive disorder is a significant risk factor for suicide across all age groups; however, older adults with major depressive disorder face unique vulnerabilities. Among older adults, symptoms of depression are often comorbid with cognitive decline or physical illness. Older adults often fail to express sadness or may present with more somatic complaints [50]. Thus, depression among the elderly is frequently underrecognized, and is often inadequately addressed, correlated with a high prevalence and severity of depression and in turn, suicidality [44]. Anxiety disorders frequently co-occur with depression and further compound suicide risk [45,46].
The use of certain medications, particularly benzodiazepines which are commonly prescribed for anxiety disorders, have been associated with an increased risk of suicide [45,51,52]. Similarly, substance use is a major concern in older adults [53,54]. Alcohol not only acts as an independent risk factor but can also be related to suicidality by worsening depression, physical illnesses, and emotional and social functioning, while heightening impulsivity [54,55]. While all these conditions have well-recognized and fairly well-studied treatments, including medication management and psychotherapy, they are often underrecognized among the elderly [50]. This could be secondary to lack of appropriate diagnostic understandings, and a myth that such non-cognitive psychiatric conditions do not start at a later age. Moreover, among older adults, depression may present with different levels of disability as compared to younger adults, thus warranting different levels of management [56]. Older individuals are also more susceptible to both physical and cognitive side effects associated with pharmacotherapy. Pharmacotherapy for psychiatric conditions may interact with medication management for medical conditions, and medications used for physical conditions can further exacerbate psychiatric conditions. Together, these unique requirements can affect adequate pharmacotherapeutic management of the psychiatric condition.
3.1.4. Psychological Determinants
Psychological determinants such as hopelessness, resilience, and life satisfaction influence the risk of suicide generally, but particularly among the elderly. Hopefulness is defined as a positive motivational state that is associated with one’s feeling of improvement [57]. In contrast, hopelessness is a pervasive negative and fatalistic view about the future and immutability of one’s situation [58]. Hopelessness has been shown to predict suicide better than depression in older adults and increases in the presence of physical illness [58]. Similar to hopefulness, resilience has been identified as an important protective factor in older adult suicide. Resilience is defined as positive adaptation in the face of adverse life experiences [59]. High resilience is associated with successful aging and less depression and helps attenuate the risk of suicidality [60]. On the contrary, low resilience is associated with poor perceptions of health, low energy levels, and increased hopelessness. Gooding et al. found that the association between loneliness and suicidal ideation was partially mediated by resilience [61].
Purpose in life and life satisfaction are two other well-known psychological protective factors against suicide ideation. Life satisfaction is positively associated with adjustment and negatively associated with depression and self-reported suicide attempts [62]. Life satisfaction is closely related to one’s perceived quality of life, and can be influenced by factors like social support, physical and mental health, access to healthcare, and economic stability. One study has found that even after controlling for the influence of depression and hopelessness, purpose in life and life satisfaction protected against suicidal ideation [63]. In the same study, purpose in life was strongly and inversely associated with suicidal ideation, mediating the relationship between life satisfaction and suicidal ideation and moderating the relationship between depression and suicidal ideation [64]. It was suggested that the experience of negative psychological factors such as depression and hopelessness may not be enough to cause suicidality, but rather it is both the presence of negative factors and absence of positive factors such as life satisfaction. In general, including among older adults, positive factors play a vital role in improving problem-solving and coping abilities and mental well-being, and therefore reduce suicide ideation.
3.2. External Factors
In addition to individual factors, as described by the socioecological model, suicide risk in the older adult population is influenced by a wide range of intersecting external factors, including interpersonal, institutional, or community-level factors such as social support and relationships, and policy-level determinants.
3.2.1. Interpersonal
Loneliness and social isolation are among the most widely discussed risk factors that affect the older adult population [58,59,60,61,65]. Both loneliness and social isolation are central to the construct of thwarted belongingness as outlined in the Interpersonal Theory of Suicide. Older adults are more at risk for loneliness and isolation due to living alone, bereavement and loss of family or social circles, or cognitive and physical issues leading to struggles with independent living. Loneliness, in turn, can further exacerbate many health risks including an increased risk of dementia, heart disease, and stroke, and is often associated with higher rates of depression, anxiety, and suicide [64,66,67,68,69,70]. Beyond its direct association with suicidal ideation, loneliness is also linked indirectly to physical illnesses that are frequently observed among individuals at elevated risk for suicide, as discussed earlier in this review [67,68]. The COVID-19 pandemic disproportionately affected older adults, especially among those with chronic diseases [69]. Older people with such illnesses were particularly susceptible to the negative health effects of COVID-19 infection, and thus, were advised to stay home and socially isolated; these influences are currently still being evaluated [71].
Among older adults, social support has shown to play a key role in improving the quality of life, mental health, and life satisfaction [72]. Social support is a multidimensional concept that refers to real or perceived assistance or resources provided by communities or social networks [73]. Social support systems can range from family and neighbors to social clubs, where elderly individuals can meet and spend time [74]. With age, also comes the loss of socialization at work, and potentially caregiver stress, particularly if a significant other is physically unwell. Social support among older adults also plays a crucial role in modifying risk factors associated with suicidal ideation. Social support has been found to be a moderating variable for depression and suicidal ideation [75]; compared to non-suicidal depressed and non-depressed older adults, suicidal depressed older adults reported the lowest levels of perceived social support [76].
3.2.2. Organizational
From an organizational perspective, in addition to these social factors, access to appropriate health services including physical health and behavioral health services is critical in identifying and treating underlying conditions. Access can include resources related to transportation, insurance, and health systems engaged in providing specialized care for older adults. The significant shortage in specialized geriatric care and adequate training in serving older adults, both for physical health and behavioral health conditions, is well-documented [77]. Adding to this shortage is lack of access related to insurance coverage for these specialized services. Furthermore, the COVID-19 pandemic severely disrupted access to another important service—formal long-term services and supports, which were already limited. Many home- and community-based services, including adult day health programs and assisted living facilities, were forced to close temporarily, with some later shutting down permanently [78,79]. This deficit continues and is likely associated with both caregiver stress and feelings of burdensomeness, all of which can in turn influence well-being and suicidality.
3.2.3. Policy
As with most public health issues, policy plays an important role in influencing the risk of suicide among older adults. Three particularly relevant policy-related risk factors include access to firearms and other lethal means, access to healthcare services, and adequate financial safety nets. In 2021, in the US, suicide by firearm was statistically more prevalent than all other mechanisms for death across all ethnicities in men aged 55 and older (29.6 deaths per 100,000 population for men) [80]. The suicide rate grew linearly as age increased among this population, from 26.6 (ages 55–64) and 26.1 (ages 65–74), to 38.2 (ages 75–84) and 55.7 (ages 85 and older) [2]. The most common lethal means of suicide for older adult men were firearms, poisoning, and suffocation. For poisoning-related deaths, including deaths from drug overdose, and suffocation-related deaths among women, rates generally declined with increasing age [2]. Aside from firearms, overdose from drugs constitutes a significant cause of many suicides in older adults [81]. Among deliberate drug overdoses, older patients have been found to more commonly use cardiovascular drugs and tricyclic antidepressants compared to their younger counterparts [82]. As discussed in earlier sections, two additional key policy-related elements are financial safety nets that can lower the perceived sense of burdensomeness related to financial security, and adequate insurance coverage that can improve access to timely and appropriate healthcare services.
3.2.4. Culture and Society (And Time)
Ageism, a term first introduced in 1969, refers to the prejudice and discrimination faced by older individuals [83,84]. Discriminatory behaviors can range from negative portrayal of the elderly individual to therapeutic failures in clinical settings, such as acceptance of depressive symptoms as normal aging and the adoption of a nihilistic attitude towards elderly individuals. These discriminatory behaviors may be particularly worse towards elderly individuals with physical health conditions and disabilities. They may also be compounded by gender stereotypes such as the need to be a stoic and self-reliant man, or a nurturing, self-sacrificing and silent woman. Unlike many other forms of discrimination, ageism is unfortunately often socially acceptable and frequently normalized in everyday interactions. Ageist attitudes have been gradually progressing over time. From a natural process that should be celebrated to a societal burden, discriminatory attitudes toward elderly individuals have been gradually increasing. These negative views have been reported worldwide, with one global survey indicating that over 60% of respondents had experienced or observed ageism, but may have a particularly greater influence among elderly in traditionally deferential Eastern cultures, where older adults were once respected as sources of wisdom and authority [85,86]. It has been proposed that the attitudinal shift may be driven by rapid population aging and changes in social dynamics, including urbanization, migration, and shifting family structures. In contrast, rates continue to be low in North Africa and the Middle East, and Latin America, likely secondary to sociocultural, continued collectivist attitudes and finally, religious attitudes [6]. The shift from cultural reverence to negative stereotyping likely erodes belongingness and increases perceived burdensomeness and loneliness—factors that may have particularly severe consequences in collectivist Eastern societies.
Ageism has both direct and indirect associations with late-life suicide. Ageism may heighten feelings of perceived burdensomeness (“I am a burden”) and thwarted belongingness (“I no longer belong”), especially when combined with age-related societal isolation and loneliness. Ageist stereotypes and discrimination directly reinforce both: by portraying older adults as dependent and costly, they amplify feelings of being a burden, while simultaneously undermining belongingness through exclusion, invisibility, or dismissal within families, communities, and healthcare systems. Many older individuals internalize these stereotypes, which can adversely affect psychological well-being, cognitive functioning, and physical health, thereby heightening suicide risk. Indeed, a meta-analysis of 422 studies from 45 countries found ageism negatively impacted health outcomes in 96% of cases—including increased risk for depression and suicidality [87]. A second U.S. study showed older adults with internalized ageism had significantly higher odds of recent suicidal ideation [88]. Age-related discrimination is not limited to stereotypes and societal and familial attitudes but have been well-documented in clinical settings as well. These behaviors can range from condescending communication (“elderspeak”) to decreased likelihood of being screened for depression and suicidality. Together, these experiences are associated with reduced access to care, and ultimately, higher vulnerability to suicide in late life.
4. Interventions to Reduce Suicide Risk
Successful aging is perhaps the strongest primary prevention intervention of suicide [89,90]. Successful aging has been defined as freedom from disease or disease-disability, high cognitive and physical functioning, and active engagement with life. The term successful aging not only implies longevity but also includes independence, functional ability, and quality of life or improved well-being [91]. Individuals who age successfully have been identified as having six broad themes: active engagement and independence; physical activity and well-being; resilience and acceptance; social-emotional connection and support; health promotion and maintenance; and mentally healthy/cognitively sound [92].
When planning and identifying interventions, it is important to recognize both the fluid nature of suicide and cultural context of the elderly individual. The underlying risk for suicide is also multicausal, with risk increasing as the number of underlying factors increases. Furthermore, as an individual ages, risk factors and their influence on risk of suicide vary, highlighting the importance of being dynamic and flexible in designing and evaluating interventions [93]. A population-based approach or public health approach aims to improve the health of the overall population and considers intervening at any level of disease from the personal or individual to the policy level. Targeted-approach interventions are similar to high-risk strategies but focus on subgroups with certain high-risk demographic or behavioral characteristics. In the context of geriatric suicide, this could look similar to a tailored intervention for older adults with early signs of Alzheimer’s disease. Lastly, screening could be thought of as an early preventive intervention, as early screening can identify people at risk, allowing practitioners to educate them and their families of the risks, and connect them to treatment services.
4.1. Individual
Table 1 discusses interventions at the various individual levels and their association with Interpersonal Theory. At the individual level, certain factors such as gender, race, and education level will be considered static risk factors, with limited ability to change through interventions. Nonetheless, recognizing the role of these static factors helps identify a vulnerable population. On the other hand, the individual dynamic risk factors related to financial, psychiatric and medical conditions can be addressed and mitigated through specific interventions. As an example, addressing financial distress and perhaps considering appropriate employment may help mitigate feelings of perceived burdensomeness [94].

Table 1.
Interventions for Individual Risk Factors and relationship with Interpersonal Theory constructs.
Risks stemming from psychiatric conditions can be alleviated through targeted treatments. These interventions begin with appropriate understanding and screening for depression and other psychiatric conditions among the elderly. The primary care settings are an important touchpoint in screening for suicidality among older adults. Studies have noted that approximately 70% of elderly people have reached out to their primary care physicians in the month before suicide [95]. Screening tools for depression such as the Geriatric Depression Scale (GDS) [96] can be used along with specialized screening tools for suicide [49]. Following screening and identification, appropriate treatment to mitigate risk from psychiatric conditions can help address suicidality. Treatment modalities for psychiatric conditions can range from pharmacotherapy such as antidepressants and anxiolytics to interventional methods such as electroconvulsive therapy to individual psychotherapy, including cognitive behavioral therapy, psychoeducation, psychodynamic therapy, and interpersonal psychotherapy focusing on changing roles [97,98,99,100,101,102]. Pharmacotherapy among the elderly needs to be cautiously addressed considering the risk of drug interactions and increased vulnerability to side effects. Medications such as sedatives, including benzodiazepines and medications that are associated with increased lethality such as tricyclic antidepressants, should be prescribed judiciously with careful monitoring. Psychotherapies, group and individual, aimed at addressing belongingness and burdensomeness, and strategies addressing loneliness, hopefulness, and resilience can be helpful in lowering suicidality.
Increasing awareness and education among primary care physicians about depressive symptoms, substance used disorders and the risk of suicide among the elderly is a critical intervention. Primary care physicians often form a trusting and enduring relationship with their patients, particularly the elderly patient, and education about risk factors including loss and loneliness with access to interventions can potentially help reduce suicide. Individuals seeking medical care and services for physical health issues, including cancer, medical conditions, and cognitive concerns are at high risk for suicide and should be screened for suicidality. Such screening should be followed with not just appropriate treatment with medications and therapy, but providing additional support such as ancillary services with social workers and other support team members can further enhance belongingness and lower burdensomeness. Management of suicidality should also include thoughtful and empathic discussions on limiting access to lethal means including firearms and monitoring medications. Increasing access to specialty geriatric care and settings with integrated behavioral health and utilizing digital health and telehealth services may help increase capacity to appropriately screen and address comorbid psychiatric and substance use disorders in a timely manner.
4.2. Interpersonal
Table 2 provides a list of interventions at the interpersonal level and their association with Interpersonal Theory. Among the elderly, addressing social support and caregiver burden play an important role in addressing suicidality. Community-based intervention programs can play an important role in lowering risks of suicide among the elderly [49,103]. Non-traditional settings such as libraries and churches may be used to both provide education and awareness about suicidality. Such interventions can take the form of mental-health workshops which provide education about depression to increase awareness and help-seeking, and group activities that promote social networks and relationships to reduce loneliness and isolation and build protective factors such as resilience. These social networks can also be used to provide support including transportation, and meal delivery programs [49]. A systematic review of suicide prevention programs through community intervention reported that long-term programs that utilized societal involvement at multiple levels succeeded in reducing suicide rates. While these networks improve awareness and encourage help-seeking behaviors, they also increase feelings of belongingness. Elderly individuals often also serve as informal caregivers for their significant others, which in turn can increase fatigue and isolation. Studies evaluating the roles of formal and informal caregiving, long-term residential services, nursing homes and in-home services and therapeutic aides on feelings of burdensomeness among elderly and belongingness among their caregivers will be critical from a preventive perspective.
Table 2.
Interventions for Interpersonal (Micro) Risk Factors and relationship with Interpersonal Theory constructs.
4.3. Organizational and Policy
Table 3 lists interventions at the organizational and policy levels and their association with Interpersonal Theory. Access to appropriate healthcare is not only important to ensure the health and well-being of older individuals but is also critical for the early identification and prevention of suicide. Older adults face several barriers to care, including insurance and transportation [104]. These barriers were further heightened during the COVID-19 pandemic [105]. Older adults with Medicaid or who are uninsured have higher rates of suicide ideation and suicide attempts compared to those on private insurance [106]. The Affordable Care Act (ACA) addressed some of these barriers by including several provisions that improved healthcare access for older adults, including improved mental healthcare access, and was associated with a significantly decreased risk of suicide in older adults with Medicaid [106].
Table 3.
Interventions for Organizational & Policy (Exo) Risk Factors and relationship with Interpersonal Theory constructs.
Means-restriction policies—particularly those addressing firearm access—are among the most strongly evidence-based strategies for reducing suicide risk among all age groups, including elderly individuals. In addition to state policies with regard to firearm access, risk management and targeted training for healthcare professionals to screen and evaluate patients for suicidality and lethal-means safety may also be effective [107]. For those with a gun in the home, keeping the weapon unloaded and in a locked safe decreases the likelihood of suicide [81]. However, restricting other commonly used lethal means amongst older adults, such as medication accessibility using medication lockboxes, may infringe on personal autonomy and will need to be balanced from an ethical perspective. Further research is warranted to examine the feasibility and effectiveness of means reduction, including firearm restriction strategies and medication lockboxes, tailored to the specific suicide risks of older adults. Finally, increasing awareness and knowledge about suicidality and safety strategies among older individuals and their social support networks, using appropriately designed and targeted suicide prevention campaigns, particularly through simple Google searches, may help address disparities associated with rising trends in suicide among the elderly [108].
Most current interventions are heavily weighted towards addressing individual depressive symptoms and suicidality by lowering access to means, few have focused on societal and organizational influences on perceived burdensomeness and thwarted belongingness. And even fewer have focused on the need to address ageism. Perhaps the most important intervention that transcends all levels will be to address the changing attitudes toward elderly individuals. Acknowledging and addressing ageism and discriminatory behaviors toward elderly individuals will help enhance all proposed interventions at all levels and thus help address both perceived burdensomeness and thwarted belongingness. These changes can range from media portrayal of elderly individuals to awareness, linguistic education and awareness (“elderspeak”) and education about discriminatory behaviors across the multiple socioecological systems, including family members, organizations (employers and healthcare organizations) and policy-making bodies [109].
5. Conclusions
To summarize, the rising trend of suicide among older adults represents a pressing and complex public health challenge. Late-life suicide is not the result of a single cause, but rather a complex interplay of layered influences across individual, interpersonal, cultural, and structural domains. In this review, we integrated the socioecological framework with Joiner’s interpersonal theory to illustrate how broader social and systemic risk factors shape individual-level vulnerabilities—specifically perceived burdensomeness, thwarted belongingness, and the acquired capability for suicide. Addressing this challenge requires a multifaceted strategy. Key priorities include integrating routine psychosocial and suicide risk screening into primary care; investing in aging-sensitive and accessible mental health services; expanding community initiatives that strengthen social connectedness; enacting policies to reduce access to lethal means; and ensuring adequate financial, caregiving, and health system safety nets. Finally, while these strategies target critical drivers, a transcending imperative lies in tackling ageism—the pervasive negative stereotypes and discriminatory practices that diminish older adults’ sense of value and belonging. Promoting narratives of intergenerational solidarity, and successful aging will not only improve help-seeking but is also a cornerstone in suicide prevention. By reframing societal attitudes toward aging, we can support environments where older adults enjoy improved belongingness and less burdensomeness—ultimately not just curbing the rising trend of suicide but improving overall health and well-being among the elderly population.
Author Contributions
Conceptualization, S.R. and S.J.G.; methodology, S.X. and S.R.; investigation, S.X. and S.J.G.; data curation, S.X., S.R., and M.U.; writing—original draft preparation, S.X., S.R., and M.U.; writing—review and editing, S.R., S.J.G., and M.U.; supervision, S.R.; funding acquisition, S.R. All authors have read and agreed to the published version of the manuscript.
Funding
Ramanathan receives funding support from Substance Abuse and Mental Health Services Administration (1H79FG000986-01).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Suicide; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- Garnett, M.F.; Spencer, M.R.; Weeks, J.D. Suicide Among Adults Age 55 and Older, 2021; NCHS Data Brief. No. 483; National Center for Health Statistics: Hyattsville, MD, USA, 2023.
- Centers for Disease Control and Prevention. Suicide Data and Statistics. Available online: https://www.cdc.gov/suicide/suicide-data-statistics.html (accessed on 22 June 2025).
- Choi, N.G.; DiNitto, D.M.; Marti, C.N.; Kaplan, M.S. Older Suicide Decedents: Intent Disclosure, Mental and Physical Health, and Suicide Means. Am. J. Prev. Med. 2017, 53, 772–780. [Google Scholar] [CrossRef]
- De Leo, D. Late-life suicide in an aging world. Nat. Aging 2022, 2, 7–12. [Google Scholar] [CrossRef]
- He, J.; Ouyang, F.; Qiu, D.; Li, L.; Li, Y.; Xiao, S. Time Trends and Predictions of Suicide Mortality for People Aged 70 Years and Over From 1990 to 2030 Based on the Global Burden of Disease Study 2017. Front. Psychiatry 2021, 12, 721343. [Google Scholar] [CrossRef]
- United States Census Bureau. 2023 National Population Projections Tables: Main Series; United States Census Bureau: Suitland, MA, USA, 2023. Available online: https://www.census.gov/data/tables/2023/demo/popproj/2023-summary-tables.html (accessed on 18 May 2025).
- Kushner, H.I.; Sterk, C.E. The Limits of Social Capital: Durkheim, Suicide, and Social Cohesion. Am. J. Public Health 2005, 95, 1139–1143. [Google Scholar] [CrossRef] [PubMed]
- Shira, B.; Lawrence, O.C. Psychological Models of Suicide. In The Suicidal Crisis: Clinical Guide to the Assessment of Imminent Suicide Risk, 2nd ed.; Oxford Academic: New York, NY, USA, 2023. [Google Scholar]
- Wenzel, A.; Beck, A.T. A cognitive model of suicidal behavior: Theory and treatment. Appl. Prev. Psychol. 2008, 12, 189–201. [Google Scholar] [CrossRef]
- Joiner, T.E.; Van Orden, K.A.; Witte, T.K.; Selby, E.A.; Ribeiro, J.D.; Lewis, R.; Rudd, M.D. Main predictions of the interpersonal–psychological theory of suicidal behavior: Empirical tests in two samples of young adults. J. Abnorm. Psychol. 2009, 118, 634–646. [Google Scholar] [CrossRef]
- Rubinstein, D.H. A stress-diathesis theory of suicide. Suicide Life-Threat. Behav. 1986, 16, 182–197. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Toward an experimental ecology of human development. Am. Psychol. 1977, 32, 513–531. [Google Scholar] [CrossRef]
- Shneidman, E.S. A psychological approach to suicide. In Cataclysms, Crises, and Catastrophes: Psychology in Action; VandenBos, G.R., Bryant, B.K., Eds.; American Psychological Association: Washington, DC, USA, 1987; pp. 147–183. [Google Scholar]
- Chu, C.; Buchman-Schmitt, J.M.; Stanley, I.H.; Hom, M.A.; Tucker, R.P.; Hagan, C.R.; Rogers, M.L.; Podlogar, M.C.; Chiurliza, B.; Ringer, F.B.; et al. The interpersonal theory of suicide: A systematic review and meta-analysis of a decade of cross-national research. Psychol. Bull. 2017, 143, 1313–1345. [Google Scholar] [CrossRef]
- Beghi, M.; Butera, E.; Cerri, C.G.; Cornaggia, C.M.; Febbo, F.; Mollica, A.; Berardino, G.; Piscitelli, D.; Resta, E.; Logroscino, G.; et al. Suicidal behaviour in older age: A systematic review of risk factors associated to suicide attempts and completed suicides. Neurosci. Biobehav. Rev. 2021, 127, 193–211. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, G.M.; Fridel, E.E.; Trovato, D. Disproportionate burden of violence: Explaining racial and ethnic disparities in potential years of life lost among homicide victims, suicide decedents, and homicide-suicide perpetrators. PLoS ONE 2024, 19, e0297346. [Google Scholar] [CrossRef] [PubMed]
- El Ibrahimi, S.; Xiao, Y.; Bergeron, C.D.; Beckford, N.Y.; Virgen, E.M.; Smith, M.L. Suicide Distribution and Trends Among Male Older Adults in the U.S., 1999–2018. Am. J. Prev. Med. 2021, 60, 802–811. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, S.K. Society and culture. In Reducing Suicide: A National Imperative; Goldsmith, S.K., Pellmar, T.C., Kleinman, A.M., Bunney, W.E., Eds.; National Academies Press: Washington, DC, USA, 2002. Available online: https://www.ncbi.nlm.nih.gov/books/NBK220948/ (accessed on 18 May 2025).
- Dhole, A.R.; Petkar, P.; Choudhari, S.G.; Mendhe, H.; Petkar, D. Understanding the Factors Contributing to Suicide Among the Geriatric Population: A Narrative Review. Cureus 2023, 15, e46387. [Google Scholar] [CrossRef]
- Mitchell, O.; Lusardi, A. Remaking Retirement: Debt in an Aging Economy; Oxford University Press: Oxford, UK, 2020. [Google Scholar]
- Smith, L.; Shin, J.I.; Carmichael, C.; Jacob, L.; Kostev, K.; Grabovac, I.; Barnett, Y.; Butler, L.; Lindsay, R.K.; Pizzol, D.; et al. Association of food insecurity with suicidal ideation and suicide attempts in adults aged ≥50 years from low- and middle-income countries. J. Affect. Disord. 2022, 309, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Kułak-Bejda, A.; Bejda, G.; Waszkiewicz, N. Mental Disorders, Cognitive Impairment and the Risk of Suicide in Older Adults. Front. Psychiatry 2021, 12, 695286. [Google Scholar] [CrossRef]
- Schmutte, T.; Olfson, M.; Maust, D.T.; Xie, M.; Marcus, S.C. Suicide risk in first year after dementia diagnosis in older adults. Alzheimer’s Dement. 2021, 18, 262–271. [Google Scholar] [CrossRef]
- Richard-Devantoy, S.; Szanto, K.; Butters, M.; Kalkus, J.; Dombrovski, A. Cognitive inhibition in elderly high-lethality suicide attempters. Eur. Psychiatry 2015, 30, 1793. [Google Scholar] [CrossRef][Green Version]
- Villarejo-Galende, A.; García-Arcelay, E.; Piñol-Ripoll, G.; del Olmo-Rodríguez, A.; Viñuela, F.; Boada, M.; Franco-Macías, E.; de la Peña, A.I.; Riverol, M.; Puig-Pijoan, A.; et al. Awareness of Diagnosis in Persons with Early-Stage Alzheimer’s Disease: An Observational Study in Spain. Neurol. Ther. 2022, 11, 1183–1192. [Google Scholar] [CrossRef]
- Juurlink, D.N.; Herrmann, N.; Szalai, J.P.; Kopp, A.; Redelmeier, D.A. Medical Illness and the Risk of Suicide in the Elderly. Arch. Intern. Med. 2004, 164, 1179–1184. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Older Adults: Chronic Disease Indicators; Centers for Disease Control and Prevention (CDC): Atlanta, GA, USA, 2024. Available online: https://www.cdc.gov/cdi/indicators/older-adults.html (accessed on 18 May 2025).
- Kim, Y.A.; Bogner, H.R.; Brown, G.K.; Gallo, J.J. Chronic Medical Conditions and Wishes to Die among Older Primary Care Patients. Int. J. Psychiatry Med. 2006, 36, 183–198. [Google Scholar] [CrossRef]
- Erlangsen, A.; Stenager, E.; Conwell, Y. Physical diseases as predictors of suicide in older adults: A nationwide, register-based cohort study. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1427–1439. [Google Scholar] [CrossRef]
- Chang, C.H.; Chen, S.J.; Liu, C.Y.; Tsai, H.C. Suicidal drug overdose following stroke in elderly patients: A retrospective population-based cohort study. Neuropsychiatr. Dis. Treat. 2018, 14, 443–450. [Google Scholar] [CrossRef]
- Ahmedani, B.K.; Peterson, E.L.; Hu, Y.; Rossom, R.C.; Lynch, F.; Lu, C.Y.; Waitzfelder, B.E.; Owen-Smith, A.A.; Hubley, S.; Prabhakar, D.; et al. Major Physical Health Conditions and Risk of Suicide. Am. J. Prev. Med. 2017, 53, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Cheatle, M.D.; Wasser, T.; Foster, C.; Olugbodi, A.; Bryan, J. Prevalence of suicidal ideation in patients with chronic non-cancer pain referred to a behaviorally based pain program. Pain Physician 2014, 17, E359–E367. [Google Scholar] [CrossRef]
- Edwards, R.R.; Smith, M.T.; Kudel, I.; Haythornthwaite, J. Pain-related catastrophizing as a risk factor for suicidal ideation in chronic pain. Pain 2006, 126, 272–279. [Google Scholar] [CrossRef]
- Ratcliffe, G.E.; Enns, M.W.; Belik, S.L.; Sareen, J. Chronic pain conditions and suicidal ideation and suicide attempts: An epidemiologic perspective. Clin. J. Pain 2008, 24, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Themelis, K.; Gillett, J.L.; Karadag, P.; Cheatle, M.D.; Giordano, N.A.; Balasubramanian, S.; Singh, S.P.; Tang, N.K. Mental Defeat and Suicidality in Chronic Pain: A Prospective Analysis. J. Pain 2023, 24, 100587. [Google Scholar] [CrossRef]
- Santos, J.; Martins, S.; Azevedo, L.F.; Fernandes, L. Pain as a risk factor for suicidal behavior in older adults: A systematic review. Arch. Gerontol. Geriatr. 2020, 87, 104000. [Google Scholar] [CrossRef] [PubMed]
- Gayman, M.D.; Brown, R.L.; Cui, M. Depressive symptoms and bodily pain: The role of physical disability and social stress. Stress Health 2011, 27, 52–53. [Google Scholar] [CrossRef]
- Anguiano, L.; Mayer, D.K.; Piven, M.L.; Rosenstein, D. A Literature Review of Suicide in Cancer Patients. Cancer Nurs. 2012, 35, E14–E26. [Google Scholar] [CrossRef]
- Potter, A.L.; Haridas, C.; Neumann, K.; Kiang, M.V.; Fong, Z.V.; Riddell, C.A.; Pope, H.G.; Yang, C.-F.J. Incidence, Timing, and Factors Associated with Suicide Among Patients Undergoing Surgery for Cancer in the US. JAMA Oncol. 2023, 9, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Saad, A.M.; Gad, M.M.; Al-Husseini, M.J.; AlKhayat, M.A.; Rachid, A.; Alfaar, A.S.; Hamoda, H.M. Suicidal death within a year of a cancer diagnosis: A population-based study. Cancer 2019, 125, 972–979. [Google Scholar] [CrossRef]
- Wang, C.; Qiu, X.; Yang, X.; Mao, J.; Li, Q. Factors Influencing Social Isolation among Cancer Patients: A Systematic Review. Healthcare 2024, 12, 1042. [Google Scholar] [CrossRef]
- Chesney, E.; Goodwin, G.M.; Fazel, S. Risks of all-cause and suicide mortality in mental disorders: A meta-review. World Psychiatry 2014, 13, 153–160. [Google Scholar] [CrossRef]
- Obuobi-Donkor, G.; Nkire, N.; Agyapong, V.I.O. Prevalence of Major Depressive Disorder and Correlates of Thoughts of Death, Suicidal Behaviour, and Death by Suicide in the Geriatric Population—A General Review of Literature. Behav. Sci. 2021, 11, 142. [Google Scholar] [CrossRef]
- Lenze, E.J.; Mulsant, B.H.; Shear, M.K.; Schulberg, H.C.; Dew, M.A.; Begley, A.E.; Pollock, B.G.; Reynolds, C.F. Comorbid Anxiety Disorders in Depressed Elderly Patients. Am. J. Psychiatry 2000, 157, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Bakkane Bendixen, A.; Engedal, K.; Selbæk, G.; Hartberg, C.B. Anxiety symptoms in older adults with depression are associated with suicidality. Dement. Geriatr. Cogn. Disord. 2018, 45, 180–189. [Google Scholar] [CrossRef]
- Wærn, M.; Runeson, B.S.; Allebeck, P.; Beskow, J.; Rubenowitz, E.; Skoog, I.; Wilhelmsson, K. Mental Disorder in Elderly Suicides: A Case-Control Study. Am. J. Psychiatry 2002, 159, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Cornaggia, C.M.; Beghi, M.; Rosenbaum, J.F.; Cerri, C. Risk factors for fatal and nonfatal repetition of suicide attempts: A literature review. Neuropsychiatr. Dis. Treat. 2013, 9, 1725–1736. [Google Scholar] [CrossRef]
- Mezuk, B.; Lohman, M. Suicide rates are high and rising among older adults in the US. Health Aff. 2023, 42, 507–514. [Google Scholar]
- Lykouras, L.; Gournellis, R. Depression in the elderly. Ann. Gen. Psychiatry 2008, 7, 1. [Google Scholar] [CrossRef]
- Bossé, C.; Préville, M.; Vasiliadis, H.-M.; Béland, S.-G.; Lapierre, S.; Scientific Committee of the ESA Study. Suicidal Ideation, Death Thoughts, and Use of Benzodiazepines in the Elderly Population. Can. J. Community Ment. Health 2011, 30, 1–13. [Google Scholar] [CrossRef]
- Favril, L.; Yu, R.; Uyar, A.; Sharpe, M.; Fazel, S. Risk factors for suicide in adults: Systematic review and meta-analysis of psychological autopsy studies. Évid. Based Ment. Health 2022, 25, 148–155. [Google Scholar] [CrossRef]
- Blow, F.C.; Brockmann, L.M.; Barry, K.L. Role of Alcohol in Late-Life Suicide. Alcohol. Clin. Exp. Res. 2004, 28, 48S–56S. [Google Scholar] [CrossRef]
- Morin, J.; Wiktorsson, S.; Marlow, T.; Olesen, P.J.; Skoog, I.; Waern, M. Alcohol Use Disorder in Elderly Suicide Attempters: A Comparison Study. Am. J. Geriatr. Psychiatry 2013, 21, 196–203. [Google Scholar] [CrossRef]
- Pompili, M.; Serafini, G.; Innamorati, M.; Dominici, G.; Ferracuti, S.; Kotzalidis, G.D.; Serra, G.; Girardi, P.; Janiri, L.; Tatarelli, R.; et al. Suicidal Behavior and Alcohol Abuse. Int. J. Environ. Res. Public Health 2010, 7, 1392–1431. [Google Scholar] [CrossRef] [PubMed]
- Jeste, D.V.; Blazer, D.G.; First, M. Aging-Related Diagnostic Variations: Need for Diagnostic Criteria Appropriate for Elderly Psychiatric Patients. Biol. Psychiatry 2005, 58, 265–271. [Google Scholar] [CrossRef]
- Laranjeira, C.; Querido, A. Hope and optimism as an opportunity to improve the “positive mental health” demand. Front. Psychol. 2022, 13, 827320. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Brown, G.; Berchick, R.J.; Stewart, B.L.; Steer, R.A. Relationship Between Hopelessness and Ultimate Suicide: A Replication with Psychiatric Outpatients. Focus 2006, 4, 291–296. [Google Scholar] [CrossRef]
- Luthar, S.S.; Cicchetti, D.; Becker, B. The Construct of Resilience: A Critical Evaluation and Guidelines for Future Work. Child Dev. 2000, 71, 543–562. [Google Scholar] [CrossRef]
- Johnson, J.; Wood, A.M.; Gooding, P.; Taylor, P.J.; Tarrier, N. Resilience to suicidality: The buffering hypothesis. Clin. Psychol. Rev. 2011, 31, 563–591. [Google Scholar] [CrossRef]
- Gooding, P.A.; Hurst, A.; Johnson, J.; Tarrier, N. Psychological resilience in young and older adults. Int. J. Geriatr. Psychiatry 2011, 27, 262–270. [Google Scholar] [CrossRef]
- Heisel, M.J.; Flett, G.L. Purpose in Life, Satisfaction with Life, and Suicide Ideation in a Clinical Sample. J. Psychopathol. Behav. Assess. 2004, 26, 127–135. [Google Scholar] [CrossRef]
- Fischer, I.C.; Nichter, B.; Feldman, D.B.; Na, P.J.; Tsai, J.; Harpaz-Rotem, I.; Schulenberg, S.E.; Pietrzak, R.H. Purpose in life protects against the development of suicidal thoughts and behaviors in U.S. veterans without a history of suicidality: A 10-year, nationally representative, longitudinal study. J. Affect. Disord. 2023, 340, 551–554. [Google Scholar] [CrossRef] [PubMed]
- Ohiokpehai, J.; Gammack, J.K.; Siddiqui, M.; Nyahoda, T. Loneliness and Social Isolation in Older Adults. Mo. Med. 2025, 122, 118–123. [Google Scholar]
- Hajek, A.; Sutin, A.R.; Posi, G.; Stephan, Y.; Peltzer, K.; Terracciano, A.; Luchetti, M.; König, H.-H. Chronic loneliness and chronic social isolation among older adults. A systematic review, meta-analysis and meta-regression. Aging Ment. Health 2024, 29, 185–200. [Google Scholar] [CrossRef] [PubMed]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; Smit, A.P.; van Dam, C.; Schuster, N.A.; de Breij, S.; Holwerda, T.J.; Huisman, M.; Dent, E.; Andrew, M.K. Frailty Combined with Loneliness or Social Isolation: An Elevated Risk for Mortality in Later Life. J. Am. Geriatr. Soc. 2020, 68, 2587–2593. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Social Isolation and Loneliness in Older Adults: Opportunities for the Health Care System; The National Academies Press: Washington, DC, USA, 2020. [Google Scholar]
- Müller, J.; Elsaesser, M.; Berger, R.; Müller, W.; Hellmich, M.; Zehender, N.; Riedel-Heller, S.; Bewernick, B.H.; Wagner, M.; Frölich, L.; et al. The Impact of Loneliness on Late-Life Depression and Anxiety During the COVID-19 Pandemic. Am. J. Geriatr. Psychiatry 2025, 33, 717–729. [Google Scholar] [CrossRef]
- Jain, S.; Dhall, M. Social isolation in COVID-19: Impact of loneliness and NCDs on mental and physical health of older adults. In Handbook of Aging, Health and Public Policy; Bloom, D.E., Ed.; Springer: Singapore, 2023. [Google Scholar]
- Unsar, S.; Erol, O.; Sut, N. Social Support and Quality of Life Among Older Adults. Int. J. Caring Sci. 2016, 9, 249–257. [Google Scholar]
- Wand, A.P.F.; Zhong, B.-L.; Chiu, H.F.K.; Draper, B.; De Leo, D. COVID-19: The implications for suicide in older adults. Int. Psychogeriatr. 2020, 32, 1225–1230. [Google Scholar] [CrossRef]
- Drageset, J. Social support. In Health Promotion in Health Care: Vital Theories and Research; Haugan, G., Eriksson, M., Eds.; Springer: Cham, Switzerland, 2021; Chapter 11. [Google Scholar]
- Gerlach, L.B.; Solway, E.S.; Malani, P.N. Social Isolation and Loneliness in Older Adults. J. Am. Med. Assoc. 2024, 331, 2058. [Google Scholar] [CrossRef]
- Brausch, A.M.; Decker, K.M. Self-Esteem and Social Support as Moderators of Depression, Body Image, and Disordered Eating for Suicidal Ideation in Adolescents. J. Abnorm. Child Psychol. 2013, 42, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Harrison, K.E.; Dombrovski, A.Y.; Morse, J.Q.; Houck, P.; Schlernitzauer, M.; Reynolds, C.F.; Szanto, K. Alone? Percieved social support and chronic interpersonal difficulties in suicidal elders. Int. Psychogeriatr. 2009, 22, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Farrell, T.W.; Korniyenko, A.; Hu, G.; Fulmer, T. Geriatric medicine is advancing, not declining: A proposal for new metrics to assess the health of the profession. J. Am. Geriatr. Soc. 2024, 73, 323–328. [Google Scholar] [CrossRef]
- AARP Policy Institute. Innovation and Opportunity: 2023 Long-Term Services and Supports State Scorecard; AARP Policy Institute: Washington, DC, USA, 2023; Available online: https://ltsschoices.aarp.org/scorecard-report/innovation-and-opportunity (accessed on 18 May 2025).
- KFF. Payment Rates for Medicaid Home- and Community-Based Services: States’ Responses to Workforce Challenges; KFF: San Francisco, CA, USA, 2023; Available online: https://www.kff.org/medicaid/issue-brief/payment-rates-for-medicaid-home-and-community-based-services-states-responses-to-workforce-challenges/ (accessed on 18 May 2025).
- Centers for Disease Control Prevention (CDC). Suicide Self-Harm Deaths in the United States 2000–2021; NCHS Data Brief No 483; National Center for Health Statistics: Hyattsville, MD, USA, 2023. Available online: https://www.cdc.gov/nchs/products/databriefs/db483.htm (accessed on 18 May 2025).
- Conwell, Y.; Duberstein, P.R.; Connor, K.; Eberly, S.; Cox, C.; Caine, E.D. Access to Firearms and Risk for Suicide in Middle-Aged and Older Adults. Am. J. Geriatr. Psychiatry 2002, 10, 407–416. [Google Scholar] [CrossRef]
- Doak, M.W.; Nixon, A.C.; Lupton, D.J.; Waring, W.S. Self-poisoning in older adults: Patterns of drug ingestion and clinical outcomes. Age Ageing 2009, 38, 407–411. [Google Scholar] [CrossRef]
- Diego, D.L. Ageism and suicide prevention. Lancet Psychiatry 2018, 5, 192–193. [Google Scholar] [CrossRef]
- Van Orden, K.; Deming, C. Late-life suicide prevention strategies: Current status and future directions. Curr. Opin. Psychol. 2018, 22, 79–83. [Google Scholar] [CrossRef]
- Vauclair, C.; Hanke, K.; Huang, L.; Abrams, D. Are Asian cultures really less ageist than Western ones? It depends on the questions asked. Int. J. Psychol. 2016, 52, 136–144. [Google Scholar] [CrossRef] [PubMed]
- North, M.S.; Fiske, S.T. Modern attitudes toward older adults in the aging world: A cross-cultural meta-analysis. Psychol. Bull. 2015, 141, 993–1021. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.S.; Kannoth, S.; Levy, S.; Wang, S.Y.; Lee, J.E.; Levy, B.R. Global reach of ageism on older persons’ health: A systematic review. PLoS ONE 2020, 15, e0220857. [Google Scholar] [CrossRef] [PubMed]
- Gendron, T.; Camp, A.; Amateau, G.; Iwanaga, K. Internalized ageism as a risk factor for suicidal ideation in later life. Aging Ment. Health 2024, 28, 701–705. [Google Scholar] [CrossRef]
- Urtamo, A.; Jyväkorpi, S.K.; Strandberg, T.E. Definitions of successful ageing: A brief review of a multidimensional concept. Acta Biomed. 2019, 90, 359–363. [Google Scholar]
- Lapierre, S.; Erlangsen, A.; Waern, M.; De Leo, D.; Oyama, H.; Scocco, P.; Gallo, J.; Szanto, K.; Conwell, Y.; Draper, B.; et al. A systematic review of elderly suicide prevention programs. Crisis 2011, 32, 88–98. [Google Scholar] [CrossRef]
- Rodrigues, C.E.; Grandt, C.L.; Abu Alwafa, R.; Badrasawi, M.; Aleksandrova, K. Determinants and indicators of successful aging as a multidimensional outcome: A systematic review of longitudinal studies. Front. Public Health 2023, 11, 1258280. [Google Scholar] [CrossRef]
- Burton, E.; Teater, B.; Chonody, J.; Alford, S. What Does It Mean to Successfully Age?: Multinational Study of Older Adults’ Perceptions. Gerontologist 2024, 64, gnae102. [Google Scholar] [CrossRef]
- Conwell, Y.; Van Orden, K.; Caine, E.D. Suicide in Older Adults. Psychiatr. Clin. N. Am. 2011, 34, 451–468. [Google Scholar] [CrossRef]
- Lee, S.-U.; Park, J.-I.; Lee, S.; Oh, I.-H.; Choi, J.-M.; Oh, C.-M. Changing trends in suicide rates in South Korea from 1993 to 2016: A descriptive study. BMJ Open 2018, 8, e023144. [Google Scholar] [CrossRef]
- Conwell, Y.; Duberstein, P.R. Suicide in Elders. Ann. N. Y. Acad. Sci. 2001, 932, 132–150. [Google Scholar] [CrossRef] [PubMed]
- Skultety, K.M.; Rodriguez, R.L. Treating geriatric depression in primary care. Curr. Psychiatry Rep. 2008, 10, 44–50. [Google Scholar] [CrossRef]
- Cougnard, A.; Verdoux, H.; Grolleau, A.; Moride, Y.; Begaud, B.; Tournier, M. Impact of antidepressants on the risk of suicide in patients with depression in real-life conditions: A decision analysis model. Psychol. Med. 2008, 39, 1307–1315. [Google Scholar] [CrossRef] [PubMed]
- Barak, Y.; Olmer, A.; Aizenberg, D. Antidepressants Reduce the Risk of Suicide among Elderly Depressed Patients. Neuropsychopharmacology 2005, 31, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Mulsant, B.H.; Blumberger, D.M.; Ismail, Z.; Rabheru, K.; Rapoport, M.J. A Systematic Approach to Pharmacotherapy for Geriatric Major Depression. Clin. Geriatr. Med. 2014, 30, 517–534. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, D.C.; Byrne, G.J. Interventions for generalized anxiety disorder in older adults: Systematic review and meta-analysis. J. Anxiety Disord. 2012, 26, 1–11. [Google Scholar] [CrossRef]
- Szanto, K.; Mulsant, B.H.; Houck, P.; Dew, M.A.; Reynolds, C.F. Occurrence and Course of Suicidality During Short-term Treatment of Late-Life Depression. Arch. Gen. Psychiatry 2003, 60, 610–617. [Google Scholar] [CrossRef]
- Lapierre, S.; Dubé, M.; Bouffard, L.; Alain, M. Addressing Suicidal Ideations Through the Realization of Meaningful Personal Goals. Crisis 2007, 28, 16–25. [Google Scholar] [CrossRef]
- Oyama, H.; Watanabe, N.; Ono, Y.; Sakashita, T.; Takenoshita, Y.; Taguchi, M.; Takizawa, T.; Miura, R.; Kumagai, K. Community-based suicide prevention through group activity for the elderly successfully reduced the high suicide rate for females. Psychiatry Clin. Neurosci. 2005, 59, 337–344. [Google Scholar] [CrossRef]
- Fitzpatrick, A.L.; Powe, N.R.; Cooper, L.S.; Ives, D.G.; Robbins, J.A. Barriers to Health Care Access Among the Elderly and Who Perceives Them. Am. J. Public Health 2004, 94, 1788–1794. [Google Scholar] [CrossRef]
- Cochran, A.L.; McDonald, N.C.; Prunkl, L.; Vinella-Brusher, E.; Wang, J.; Oluyede, L.; Wolfe, M. Transportation barriers to care among frequent health care users during the COVID pandemic. BMC Public Health 2022, 22, 1783. [Google Scholar] [CrossRef]
- Cho, S.; Lee, K. Association between insurance type and suicide-related behavior among US adults: The impact of the Affordable Care Act. Psychiatry Res. 2024, 333, 115714. [Google Scholar] [CrossRef] [PubMed]
- Sall, J.; Brenner, L.; Bell, A.M.M.; Colston, M.J. Assessment and Management of Patients at Risk for Suicide: Synopsis of the 2019 U.S. Department of Veterans Affairs and U.S. Department of Defense Clinical Practice Guidelines. Ann. Intern. Med. 2019, 171, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Cray, H.V.; Pasciak, W.; Breheney, R.; Vahia, I.V. Public Awareness Campaigns on Suicide Prevention Are Not Optimized for Older Adults. Am. J. Geriatr. Psychiatry 2025, 33, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Ng, R.; Chow, T.Y.J. Aging Narratives Over 210 Years (1810–2019). J. Gerontol. Ser. B 2021, 76, 1799–1807. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).