Abstract
Higher education professionals are subject to high levels of stress as they support student populations at risk of trauma. Compassion fatigue, which represents dimensions of secondary traumatic stress and burnout, is associated with a poorer health-related quality of life (HRQOL) among those providing student services. Prior studies on helping professionals have found that mindful self-care mediates the relationship between compassion satisfaction, the positive aspects of helping others in one’s role, and compassion fatigue, but this has not been sufficiently explored in this population. A total of 559 respondents (faculty, students, and staff) who provide non-instructional support across 23 student service areas at 22 comprehensive regional universities completed a cross-sectional survey assessing mindful self-care, professional quality of life and HRQOL. Path analyses were conducted using EQS 6.4 software to test one model controlled for age, progressing from compassion satisfaction to mindful self-care, to compassion fatigue, to HRQOL. Mindful self-care, particularly supportive structure, mediated the relationship between compassion satisfaction and compassion fatigue. Compassion satisfaction was positively associated with HRQOL through mindful self-care and compassion fatigue. Institutions seeking to address compassion fatigue and promote well-being should implement policies to facilitate self-care by ensuring manageable workloads and balancing internal and external demands.
1. Introduction
Higher education professionals who provide non-instructional services to students may experience stress as they try to balance the official obligations of their institutional role with providing informal support to students, many of whom may experience significant life events or trauma prior to or during their college experience [1]. We use this term to refer to a range of personnel including, but not limited to counselors, coaches, administrators, programmatic staff working in student service areas (e.g. financial aid, student conduct, cultural centers, disability services), and administrative support personnel. Compassion fatigue has been associated with poor health-related quality of life (HRQOL) in this population [2]. Mindfulness is a promising practice to foster well-being and self-care among student affairs professionals [3]. However, the role of mindful self-care in the relationship between compassion satisfaction and compassion fatigue, and the resulting effect on HRQOL, has not been sufficiently explored.
Singer and Klimecki refer to compassion as the ability to maintain an emotional boundary when empathizing with their joy or suffering of another person [4]. It refers to the healthy dimensions of empathy, which can result in feelings of joy and motivation, and positive health outcomes. Empathic distress, traditionally referred to as compassion fatigue, can occur when someone takes on the pain of another as their own, leading them over time to feel repelled by the suffering of those they serve and distance themselves as a protective mechanism. This can lead to isolation and adverse health outcomes. Employee emotional health risks, which are measured by depressive symptoms, daily emotional health, and high stress level, are inversely associated with living optimal lifestyle [5]. Compassion fatigue captures the effects of secondary traumatic stress and burnout [6]. Interventions focused on increasing the levels of compassion satisfaction have found it to be protective against compassion fatigue [7].
Secondary traumatic stress (STS) describes the occurrence of symptoms of psychological injury likened to post-traumatic stress disorder among helping professionals in response to their exposure to individuals who have experienced or are currently experiencing trauma [8,9,10]. Lynch and Glass created a five-factor model for STS among student affairs professionals that measures symptoms classified under post-traumatic stress disorder in the DSM-V: negative alteration to mood or cognition, physical arousal and reactivity, emotional arousal and reactivity, avoidance, and intrusion [11]. Their study of student affairs professionals found that 9 in 10 reported supporting a student experiencing trauma in the past year, and more than two-thirds reported supporting students through one or more of the following traumas: “death of a loved one; sexual violence; suicidal ideation, attempt, or completion; severe mental health episode; and/or hate crimes and discrimination [11].
Stamm describes the positive and negative sequalae of working in the capacity of helping others, defined, respectively, as compassion satisfaction and compassion fatigue [12]. A failure to train student affairs professionals in how to deal with emotional distress in students without taking on their pain can heighten their risk for compassion fatigue [13]. Compassion fatigue encapsulates STS as well as burnout, the latter of which results from chronic stress due to how one’s work is organized and delivered [14]. Burnout is characterized by emotional exhaustion, cynicism towards elements of one’s role, and a reduced sense of personal accomplishment. In a study of student affairs professionals, job stress and burnout were found to be positively associated with job dissatisfaction and turnover intentions [15]. A separate study conducted with student affairs professionals found that more than two thirds of them were unable to balance priorities and demands [16].
Compassion satisfaction reflects the extent to which one is able to derive pleasure and positive feelings from the work they do, such as the feeling that they are helping to fulfill a greater purpose. Studies of hospice professionals [17] and employee assistance professionals [18] indicate an inverse relationship between compassion satisfaction and compassion fatigue. Research conducted among ER staff in the UK found that low levels of compassion satisfaction were associated with earlier retirement, greater irritability with clients, and poorer compliance with standards for quality care [19]. Vilardaga et al. found that higher levels of peer support were associated with lower levels of burnout in addictive counselors, while higher levels of supervisor support were associated with higher levels of emotional exhaustion (burnout) [20]. Multilevel approaches to provide support and improve perceived control were recommended as strategies to increase compassion satisfaction, including making workloads more manageable, teaching coping skills, and building a sense of cohesion among teams.
The theory of self-care evolved from the field of nursing, referring to practices initiated by patients to care for themselves [21]. The field of social work promotes self-care as a modality to combat burnout and foster resilience, the ability to recover from adversity and move forward [22,23,24,25,26,27]. Harker et al. found that resilience and mindfulness were protective against STS and burnout among a wide range of human services professionals [28], while another study found that resilience and trait negative affect were protective factors against burnout [29]. Burke et al. proposed that the practice of mindfulness, wherein one notes and addresses their stress, can help to foster wellness, increase focus, and reduce burnout and attrition among student affairs professionals [3]. Previous studies have indicated that compassion satisfaction is positively associated with emotional care, spiritual care, and work-life balance, while compassion fatigue is negatively associated with these factors as well as psychological self-care [17].
Cook-Cottone refers to mindful self-care as a process of fusing intentional acts of self-care to promote well-being with mindful awareness and an understanding of personal needs and outside demands [30]. The six domains of mindful self-care encompass internally oriented practices (physical care and self-compassion and purpose); externally oriented practices (supportive relationships and supportive structure); and practices that integrate the internal and the external (mindful awareness and mindful relaxation). Mindful awareness refers to practices such as meditation, yoga, and intentionally practicing mindfulness throughout the day. Mindful relaxation encompasses activities that allow for self-soothing, such as deep breathing. Physical care refers to engaging in proper nutrition and exercise, accessing routine health care, and adhering to medical regimens. Self-compassion and purpose refer to: (1) relating to oneself with mindfulness, recognition of common humanity, and kindness; and (2) having a sense of purpose in life, such as spirituality or a mission to fulfill. Supportive relationships refer to those that are beneficial and have healthy boundaries, while supportive structure refers to one’s physical environment, the way in which the workspace is organized, and striking a balance between personal work goals and the demands of others.
Mindful self-care practices may help to explain the relationship between compassion satisfaction and compassion fatigue among helping professionals. In a study conducted with hospice professionals, mindful self-care mediated the relationship between compassion satisfaction and burnout [31]. A study conducted with chaplains found that all domains of mindful self-care as well as STS mediated the relationship between compassion satisfaction and risk for burnout; those who had higher levels of compassion satisfaction and practiced a variety of self-care practices on a frequent basis had lower risk of burnout [32]. In a study with student affairs professionals, an individual’s effort to achieve a balance between internal and external demands was found dependent on the intention to commit to engaging in mindful self-care, which follows the self-care domain or self-compassion and purpose [33]. Furthermore, researchers contend that addressing social determinants of health can provide a structural foundation to make self-care feasible and practical for individuals [34].
It is critical to examine how professional quality of life and interventions such as mindful self-care impact the well-being of student services professionals. A study conducted among college students found that all dimensions of mindful self-care were positively correlated with mental indicators of HRQOL, while only physical care was positively associated with physical indicators of HRQOL [35]. Our previous research found that higher levels of supportive structure and mindful awareness were significant predictors of better HRQOL among faculty, staff, and students who provide non-instructional services to student populations that are disproportionately prone to experiencing trauma (hereafter referred to as student services professionals to be inclusive of, but not limited to, student affairs) [2]. Furthermore, there was a unique relationship between compassion fatigue and HRQOL above the effects of mindful self-care, compassion satisfaction, and gender.
This study builds upon our prior research by examining the role of mindful self-care as a potential mediator in the relationship between compassion satisfaction and compassion fatigue among student services professionals. It explores whether compassion satisfaction is indirectly associated with HRQOL through the pathway of mindful self-care and compassion fatigue. Our null hypotheses are as follows:
Hypothesis 1 (H1).
Mindful self-care does not mediate the relationship between compassion satisfaction and compassion fatigue.
Hypothesis 2 (H2).
Compassion satisfaction is not indirectly associated with HRQOL through compassion fatigue or mindful self-care.
These hypotheses served to formulate the structural portion of the conceptual model illustrated in Figure 1 [36]. The structural equation model tested the progression of the model from compassion satisfaction to mindful self-care, which in turn related to compassion fatigue, and ultimately HRQOL. This manuscript was structured using the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) Criteria.

Figure 1.
Conceptual Model. This figure is the conceptual model used to develop the hypotheses.
2. Materials and Methods
2.1. Participants
Our full sample consisted of 599 faculty, staff, and students at 22 regional comprehensive universities in the Western U.S. during the months of February and March of 2020 [2]. Convenience sampling was used to identify participants through university websites, and those who completed the survey were encouraged to share it with colleagues. The inclusion criteria for our study were as follows: 1) over the age of 18; 2) affiliation with one of the included institutions as a faculty, staff, or student; 3) formal role serving one of 23 indicated student service areas. Of 639 total survey respondents, 80 were excluded for failure to complete any measures. This met the requirements of our power analysis, which indicated that a sample of 394 would be required to achieve statistical power of >0.80 [37]. Participants who did not complete the HRQOL-14 were excluded and there was a total sample of 457. Figure 2 describes the number of participants at each stage in the study.
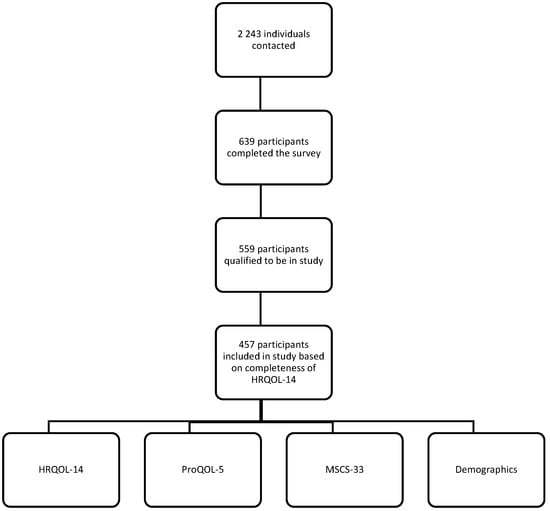
Figure 2.
Participant Model. The total number of participants is shown for different parts of the study.
2.2. Materials
Qualtrics software was used to distribute an online survey that assessed professional quality of life, mindful self-care practices, HRQOL, as well as demographics and factors pertinent to one’s professional role. Qualitative measures that explored role-related challenges faced by individuals and their coping practices will be reported separately.
2.2.1. Compassion Satisfaction and Compassion Fatigue
The Professional Quality of Life scale (ProQOL-5) assesses the impact of one’s role as a helper on quality of life through three ten-item scales measuring compassion satisfaction, burnout, and STS [6]. We addressed issues related to construct validity in the original measure by using the ProQOL-21 [38], which collapses STS and burnout into a larger measure of compassion fatigue, and also combines select response categories in order to improve overall fit. Our reliability scores for compassion fatigue (α = 0.90) and compassion satisfaction (α = 0.89) were acceptable.
2.2.2. Mindful Self-Care
The 33-item Mindful Self-Care Scale (MSCS-33) reports the frequency of individual participation in self-care practices as well as elements of one’s external environment that help to facilitate mindfulness and well-being [39]. The 33-item scale includes questions across six domains, as well as three global questions related to the variety and novelty of one’s practice. Prior studies indicate this scale has strong internal consistency reliability and construct validity [40]. Our reliability scores for each domain were consistent with earlier findings: mindful relaxation (α = 0.75), physical care (α = 0.74), self-compassion and purpose (α = 0.86), supportive relationships (α = 0.85), supportive structure (α = 0.84), and mindful awareness (α = 0.92).
2.2.3. Health-Related Quality of Life
The four-item core health days module from HRQOL-14 was used to measure physical and mental indicators of quality of life [40]. Respondents rated their general health status and indicated the number of days during the past 30 days that were unhealthy due to poor physical health, poor mental health, or limited activity due to poor physical and/or mental health. These items were used to develop a summary score that has had strong goodness of fit and validity in previous studies [41].
2.2.4. Demographic and Role Variables
Participants indicated the following background characteristics: sex assigned at birth, gender identity, sexual orientation, age, race, ethnicity, household size and income, highest education level, and marital status. To facilitate data analysis, select variables were transformed to reduce the number of categories (income) or to create dummy variables (sexual orientation, gender identity, marital status). Participants reported the following professional characteristics: primary campus affiliation, formal role in indicated student service areas, their role level, and role duration. Student service areas were included based on previous studies on secondary trauma among higher education professionals and consultations with staff members at various institutions. They included: athletics; academic advising; basic needs programs (food and housing security); centers for underrepresented minority groups and other populations such as LGBTQIA+, women, veterans, men of color, the formerly incarcerated, students with disabilities, current and former foster youth, and undocumented students; counseling and psychological services; educational opportunity programs and TRIO; financial aid; housing and residential life; student conduct; Title IX; and other student affairs or services not listed.
2.3. Data Collection
A sampling frame was built by identifying potential participants on university websites and staff directories. A weeklong pilot was conducted with 52 participants representing five percent of the sampling frame. Subsequently, the survey was distributed via email. Upon accessing the survey, participants had the opportunity to read through the informed consent and opt out. During the three-week period that the survey was open, weekly email reminders were sent. Participants who completed the survey were given an opportunity to opt-in to future focus groups on well-being. A list of campus employee assistance programs was provided in case anyone experienced discomfort related to the survey. Opportunity drawings for $50 Amazon gift cards were held once the survey closed, with two recipients drawn for each institution.
2.4. Data Analysis
A summary of the demographic background and professional profile of the respondents, as well as scores for each scale, was created using descriptive statistics [2]. The following background characteristics were assessed as potential covariates: age, gender identity, sexual orientation, race, education, ethnicity, and income. Professional characteristics that were assessed as potential covariates include work setting (campus size, number of student service areas), and role duration. We used the HRQOL summary score reported in our previous paper. The STS and burnout scale items that Heritage et al. (2018) recommended for inclusion were recoded as a measure of compassion fatigue [38]. Higher scores of compassion satisfaction and compassion fatigue reflected higher levels of each dimension. The sum of mean totals for each domain score was used to calculate a total mindful self-care score. Within our sample population, quartiles were used to indicate low (25th percentile), mean, and high (75th percentile) scores for compassion satisfaction, compassion fatigue, and mindful self-care.
Measurement of the Hypothesized Model
In the conceptual model, which comprises the structure and measurement representations (see Figure 2 in Results), the measured variables are presented in rectangles [35]. The model begins with the compassion satisfaction relating directly to compassion fatigue and indirectly through mindful self-care, and, ultimately, compassion fatigue relating to HRQOL. Mindful self-care was measured using the total score in Model 1 and, if found significant, the subscales would be tested in subsequent models. The analyses that follow present an empirical evaluation of the proposed model.
Since demographic variables—including gender, income, sexual orientation, ethnicity, race, education, marital status, time in current role, level of role, and number of service areas—could potentially play a role with respect to compassion satisfaction, these variables were assessed as covariates to establish the unique role of these variables to subsequent pathways independent of the demographic variables.
3. Results
3.1. Descriptive Analyses
Our sample was largely female (76.2%)) who identified as heterosexual (76%). Our participants represented 22 regional comprehensive universities, with 25% of the sample based at three institutions. The majority of participants were between the ages of 26 and 44 (62%), and reported having earned a Master’s degree or higher (68.4%). Roughly half of the sample reported being married or in domestic partnership (50.5%), and the mean household size was 2.8. One in five respondents reported a household income below $50,000 (18.6%), while 39.3% reported a household income between $50,000 and $99,000. Most of the respondents serve in the capacity of staff (69.1%) and provide direct services to students (63.5%). The highest reported primary student service areas were housing and residential life (11.9%), academic advising (11%), and counseling and psychological services (10.3%).
Complete demographic and professional variables are listed in Table 1 and Table 2, respectively. The means, standard deviations, and Pearson product moment correlations of all measured variables are presented in Table 3. Positive and significant correlations emerged, indicating that it was appropriate to proceed with model estimation based on the conceptual model, p < 0.05. Over the 2243 individuals who were contacted, 639 participants completed the survey. After reviewing the inclusion criteria, 559 participants qualified to be in the study. However, our mediation analyses are based on 457 respondents who completed the four items related to HRQOL given this measure was our variable of focus.

Table 1.
Demographic Variables.
Table 2.
Professional Variables.
Table 3.
Bivariate Correlations of Measured Variables.
3.2. Model Estimation
There were no univariate or multivariate outliers, and none of the measured variables were significantly skewed as evaluated through R [42] and EQS 6.4 [43]. However, the normalized coefficient of kurtosis was 5.51, indicating the presence of multivariate kurtosis, and a maximum likelihood estimation with robust fit indices and standard errors would be appropriate [44]. Measured variables contained between 5.7% and 10.2% missing data. The missing completed at random test (MCAR) [45] as implemented in the BaylorEdPsych package in R [46] was used to evaluate the missing data mechanism and revealed the data were not missing completed at random, χ2 (57) = 297.62, p < 0.001, indicating that maximum likelihood imputation using observed standard errors would be appropriate.
Path analyses were performed using EQS 6.4 software [43]. All paths depicted in Figure 1 as well as error variances of measured variables were freely estimated. Finally, all paths not shown in Figure 3, including correlations among errors, were fixed to 0, and thus, not estimated.

Figure 3.
Model 1. This figure displays the level of significance at the p < 0.05 level for the variables connected with the one-way arrow for those noted with an asterisk (*).
The demographic variables were evaluated separately as potential covariates for the model depicted in Figure 3 (see Section 3.2.2 Model 2), and age was found to be a significant covariate (β = 0.10, p < 0.05). All remaining paths were interpreted after controlling for age. The model with 5 degrees of freedom produced a Yuan-Bentler χ2 of 12.82, and RCFI of 0.965, a Bentler-Bonett NNFI of 0.931, and an RMSEA of 0.049 (90% CI 0.005–0.089), all indicating an adequate fit to the data. Furthermore, the model R2 of 0.107 indicated that approximately 11% of the variability in HRQOL can be accounted for by the combination of compassion satisfaction, mindful self-care, and compassion fatigue.
3.2.1. Model 1
Figure 3 provides the standardized parameter estimates, representing the beta-weights (one-way arrows). Compassion satisfaction related significantly and positively to mindful self-care (β = 0.40, p < 0.05), and negatively to compassion fatigue (β = −0.19, p < 0.05), indicating that increases in compassion satisfaction were associated with higher levels of mindful self-care and lower levels of compassion fatigue. Additionally, mindful self-care related significantly and negatively to compassion fatigue (β = −0.29, p < 0.05). Furthermore, compassion fatigue negatively and significantly related to HRQOL (β = −0.33, p < 0.05), indicating that higher levels of compassion fatigue was associated with poorer HRQOL. In addition, compassion satisfaction (β = 0.10, p < 0.05) and mindful self-care (β = 0.09, p < 0.05) had significant indirect effects on HRQOL, and compassion satisfaction also had a significant indirect effect on compassion fatigue (β = −0.12, p < 0.05). Components of these indirect effects include paths from compassion satisfaction to HRQOL, indicating further – in accordance with the conceptual model – that higher levels of compassion satisfaction were associated with better HRQOL through mindful self-care and compassion fatigue.
3.2.2. Model 2
To further investigate the role of mindful self-care, the six mindful self-care subscales replaced the total score from model 1 and were tested simultaneously. The model specifications were the same as model 1, except the error covariances among each mindful self-care subscale were estimated. The model with 15 degrees of freedom produced a Yuan-Bentler χ2 of 29.71, and RCFI of 0.991, a Bentler-Bonett NNFI of 0.974, and an RMSEA of 0.036 (90% CI 0.000–0.064), all indicating an adequate fit to the data. Furthermore, the model R2 of 0.10 indicated that approximately 10% of the variability in HRQOL can be accounted for by the combination of compassion satisfaction, six mindful self-care subscales, and compassion fatigue.
Figure 4 provides the standardized parameter estimates, representing the beta-weights (one-way arrows). Compassion satisfaction was significantly and positively related to five of the mindful self-care subscales [mindful relaxation (β = 0.28, p < 0.05), self-compassion and purpose, (β = 0.41, p < 0.05), supportive relationships (β = 0.33, p < 0.05), supportive structure (β = 0.26, p < 0.05), and mindful awareness (β = 0.34, p < 0.05)] but not physical care (β = 0.08, p > 0.05), and significantly and negatively to compassion fatigue, (β = −0.16, p < 0.05), indicating that increases in compassion satisfaction were associated with higher levels of all areas of mindful self-care except physical care, and lower levels of compassion fatigue. Correlations among the mindful self-care subscales were all positive and significant, with values ranging from 0.09 to 0.60. Of the six mindful self-care subscales, only supportive structure related significantly to compassion fatigue (β = −0.46, p < 0.05), indicating that increases in supportive structure related to decreases in compassion fatigue. Furthermore, compassion fatigue negatively and significantly related to HRQOL (β = −0.31, p < 0.05), indicating higher levels of compassion fatigue was associated with poorer HRQOL after controlling for compassion satisfaction and mindful self-care. Compassion satisfaction (β = 0.08, p < 0.05) and supportive structure (β = 0.14, p < 0.05) had significant indirect effects on HRQOL, and compassion satisfaction also had a significant indirect effect on compassion fatigue (β = −0.11, p < 0.05). Components of these indirect effects include paths from compassion satisfaction to HRQOL, indicating that, in accordance with the conceptual model, higher levels of compassion satisfaction were associated with better HRQOL through supportive structure and compassion fatigue.
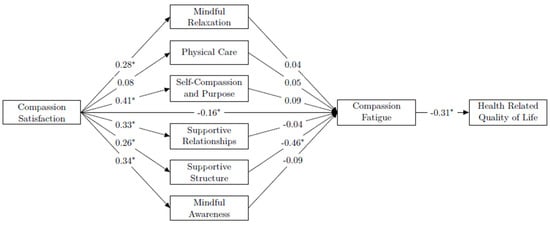
Figure 4.
Model 2. This figure shows the level of significance at the p < 0.05 level for the variables connected with the one-way arrow for those noted with an asterisk (*).
4. Discussion
Research on self-care practices and the impact of professional factors and health on quality of life is limited among professionals in university-based settings and has not traditionally expanded to other services beyond student affairs that also serve students who may be disproportionately prone to experiencing trauma [1]. The previously published data for this study found that compassion fatigue was associated with poorer HRQOL [2]. The aim of our study was to explore how mindful self-care impacted professional quality of life and HRQOL among a wide range of individuals who provide non-instructional services to students, given that mindful self-care is used to promote well-being while being aware of one’s needs [30]. The analysis sought to confirm the null hypotheses that mindful self-care does not mediate the relationship between compassion satisfaction and compassion fatigue, and that compassion satisfaction is not indirectly associated with HRQOL through compassion fatigue or mindful self-care. Of the demographic and professional background variables examined, only age was significant. As a result, age was included as a covariate in our model, and our findings are independent of this factor.
Our first model indicated that mindful self-care (represented by the total score) mediates the relationship between compassion satisfaction and compassion fatigue. Specifically, increasing levels of compassion satisfaction were associated with mindful self-care, and increasing levels of mindful self-care were associated with lower compassion fatigue. Thus, mindful self-care helps to explain the underlying relationship between compassion satisfaction and compassion fatigue. This is consistent with earlier research conducted in hospice care professionals [31] and chaplains [32], which rather than using compassion fatigue, maintained STS and burnout as separate dimensions in order to also explore the effect of STS as a potential mediator. These studies found that mindful self-care as well as STS were mediators in the relationship between compassion satisfaction and burnout. Other studies in social work have promotes self-care in order to foster resilience and decrease the levels of burnout [22,23,24,25,26,27]. Harker et al. found that resilience and mindfulness in human services professionals serve as protective factors against burnout and STS [28]. Interventions to increase compassion satisfaction may be effective in helping to facilitate engagement in self-care, which are partnered with effective organization-level strategies to mitigate stressors, can help lessen compassion fatigue.
Our second model tested all of the mindful self-care domains simultaneously, finding that increases in compassion satisfaction were associated with higher levels of all areas of mindful self-care except physical care. This finding is consistent with the results of previous research conducted with hospice professionals [31]. An earlier study conducted with hospice care professionals using Saakvitne and Pearlman’s self-care assessment worksheet to measure engagement in self-care practices found that while emotional care, spiritual care, and balance were positively associated with compassion satisfaction, there was no significant relationship for physical care, psychological care, or workplace self-care [17]. Thus, interventions that specifically address practices such as nutrition, hydration, exercise, and mind-body practices may be needed to help this population develop an intentional self-care practice that focuses on their physical needs. It is also important to address foundational needs (e.g., physical care) before moving onto higher level needs such as compassion satisfaction [31].
Our second model indicated that only one MSC domain, supportive structure, mediated the relationship between compassion satisfaction and compassion fatigue. Supportive structure captures the extent to which one reports having: 1) a manageable workload and schedule; 2) a workspace that is conductive to completing assigned tasks; 3) the ability to balance personal priorities against external demands; and 4) a comfortable living space. Our findings suggest that factors pertaining to how individuals navigate their organizational context and external demands have important implications for overall quality of life and well-being. However, previous studies found that additional domains of MSC mediated the relationship between compassion satisfaction and burnout, with self-compassion and purpose and mindful self-awareness having the strongest mediation effects [31,32]. This is consistent with results of a mindfulness intervention conducted with entry-level student affairs professionals and graduate assistants enrolled in a graduate student affairs program [3], in which participants reported greater awareness of stress and an increased capacity to address their internal needs (e.g., emotional) following the intervention. The researchers posited that such interventions to promote well-being and self-care among student affairs professionals could, in turn, positively impact the quality of service that student service professionals are able to provide to students. The risk for compassion fatigue increases when individuals on not properly trained on how to navigate working with students who have or are currently experiencing trauma [13].
Future interventions to address compassion fatigue and HRQOL among student services professionals and other helping professions should seek to improve supportive structure by implementing organizational practices, policies, and procedures that promote manageable individual workloads, create realistic work schedules, and allow for the successful balance of external and internal demands. Prior research conducted with student affairs professionals found that those identified by peers as embodying balance defined the term as a lifelong developmental process involving a commitment to self-care, self-knowledge, intentionality, and reflection [33]. Both intentionality and self-knowledge are consistent with the MSC domain of self-compassion and sense of purpose. Reflection is consistent with the domain of mindful awareness. Participants recommended conscious mentorship and role modeling of balance for new professionals, mindful that the failure to do so could negatively affect recruitment and retention.
Prior research conducted among student affairs professionals has indicated that stress and burnout are associated with job dissatisfaction and turnover intentions [15]. In a study on attrition among student affairs professionals, more than two-thirds of respondents reported an inability to balance internal priorities and external demands [16]. Lower levels of compassion satisfaction in emergency room staff were associated with lower quality of care, retirement at an earlier age, and more irritability with their patients [21]. One in three cited work-life conflict as a deciding factor in departing from a student affairs role. The researchers acknowledged the positive and motivating effect that having a sense of purpose in one’s work, measured in our study as compassion satisfaction. However, they emphasized the need for the field to communicate upfront the expectations of an organizational culture that demands extended hours and often requires the prioritization of student needs over personal needs. Furthermore, one must be mindful of and attentive to the burden such expectations can have on individual long-term well-being and decisions to stay in one’s position or leave the field.
Peer and managerial support can significantly influence elements of supportive structure, including one’s ability to navigate personal goals and external demands, as well as the extent to which one’s workspace is comfortable or hostile. A study on burnout among nurses found that while resilience and trait negative affect were most predictive of burnout, peer and managerial support were also important factors [29]. Research conducted with addictive counselors found that peer support in the work context was negatively associated with two dimensions of burnout—personal sense of accomplishment and emotional exhaustion—while support from supervisors was positively associated with emotional exhaustion [20]. This is consistent with our finding of an indirect relationship between supportive structure and compassion fatigue. However, the same study found that dimensions of one’s practice of mindfulness and commitment to core values were ultimately more predictive of burnout than factors related to the nature of one’s work (e.g., workload, social support, job control), and suggested that interventions address both individual and organizational level factors in order to effect change. This finding that mindfulness was more predictive of burnout than supportive structure is not consistent with the results we have presented here, but prior research suggests that higher levels of all domains of mindful self-care are associated with lower levels of burnout among helping professionals [31,32].
Research on burnout indicates that interventions designed to improve how individuals experience and deal with stress that address characteristics at both the individual level (e.g., strengthening coping skills, social support) and the organizational level (e.g., increasing shared decision-making, a sense of control in one’s role, or managing workload) achieve longer-lasting reductions in reported burnout than those that focus on the individual level alone. Shifting towards addressing burnout as an element of organizational culture helps to ensure positive effects do not attenuate over time [47].
The results of our path analysis suggest an indirect effect of compassion satisfaction on HRQOL through mindful self-care, particularly supportive structure, and compassion fatigue. Our findings indicate that those who have higher levels of compassion satisfaction also have higher levels of supportive structure. In turn, they have lower levels of compassion fatigue, and better HRQOL. Our findings are consistent with previous studies that have found that HRQOL is positively associated with compassion satisfaction and negatively associated with compassion fatigue [48]. Factors that increase compassion satisfaction among student services professionals may influence adoption of mindful self-care practices. Singer and Klimecki found that training in compassion, such as lovingkindness meditation, can help improve one’s ability to cope with stress and respond with greater resilience [4]. Interventions focusing on increasing compassion satisfaction can help individuals to develop positive emotions that serve as a protective factor against becoming overwhelmed by the negative emotions of others, thus avoiding chronic empathic distress in which one withdraws emotionally from the populations they serve [7].
Increased compassion satisfaction was not associated with physical care, a fundamental element of overall well-being, in several studies discussed here. Additional attention should also be given to providing opportunities and resources for engaging in physical care practices such as proper nutrition, hydration, exercise, and utilization of routine medical care to further improve HRQOL.
Limitations
Inferences about the role of STS and burnout cannot be made from our results due to the fact that we used the approach proposed by Heritage et al. to examine trauma and burnout-related indicators together as one measure indicating compassion fatigue [38]. While this approach helped to address issues with construct validity, we are not able to confirm the results of prior research, which has indicated that both mindful self-care and STS mediate the relationship between compassion satisfaction and burnout [31,32]. Due to the self-report nature of our survey, it is possible that recall bias as well as the desire to adhere to norms may have influenced information reported by respondents. Moreover, those who found the topic of interest or relevance may have been more likely to participate in the survey. While nearly half of our sample is non-white and is representative of the demographic makeup of the population from which participants were drawn, our sample is also largely female. Future studies should aim to include a more diverse sample of individuals to better detect differences based on demographic characteristics. While some service areas were well-represented in our study, others were underrepresented. We explored correlational relationships between the variables in this study and cannot draw conclusions regarding causality.
Future research should use separate scales to directly investigate the effects of STS and burnout in this population. STS can be measured using scales developed for resident assistants [49] and student affairs professionals [11]. Burnout can be directly measured using scales such as the Maslach Burnout Inventory [50]. It would be valuable to identify the specific self-care practices individuals employ to cope with role challenges, and to identify any maladaptive coping practices. Furthermore, a longitudinal approach could explore causal relationships among variables and how they unfold over time.
5. Conclusions
We found that supportive structure is negatively associated with compassion fatigue, and that both compassion satisfaction and supportive structure have an indirect, positive effect on HRQOL. Organizations looking to improve student academic success and well-being should be attentive to the negative consequences of compassion fatigue among those who serve students. Efforts to improve compassion satisfaction and HRQOL in this population should address individual and organizational level components of mindful self-care. By taking steps to ensure manageable workloads and facilitate a supportive work environment in which individuals are able to navigate both external demands and personal needs, employees may experience improved professional quality of life and avoid negative physical and mental health outcomes. In turn, this can positively impact their ability to support students and sustain institutional initiatives to foster student success.
Author Contributions
Conceptualization, P.J.P.; methodology, P.J.P.; software P.J.P. and K.S.J.P..; validation, D.S. and P.J.P.; formal analysis, K.S.J.P.; investigation, P.J.P. and D.S.; resources, P.J.P.; data curation, P.J.P. and D.S.; writing—original draft preparation, P.J.P.; writing—review and editing, P.J.P., D.S. and K.S.J.P.; visualization, P.J.P.; supervision, P.J.P.; project administration, P.J.P.; funding acquisition, P.J.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by California State University Chancellor’s Office, grant CPO number 19-0088.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of California State University Fullerton (HSR-19-20-96 and 01-20-2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The full data are not publicly available due to privacy concerns.
Acknowledgments
We would like to acknowledge Hannah Peterson, Athena Corral Carlos, and Aaliyah Reed for their contributions to data collection, Laura Gil-Trejo and Frederick Rose for their guidance in study design in data collection, and Carrie Lane for feedback on earlier versions of this manuscript. Delia Sanchez was affiliated with the Department of Public Health at California State University Fullerton, but is currently affiliated with Empowered to Exhale (email: delia@empoweredtoexhale.com).
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Read, J.P.; Ouimette, P.; White, J.; Colder, C.; Farrow, S. Rates of DSM-IV-TR Trauma Exposure and Posttraumatic Stress Disorder Among Newly Matriculated College Students. Psychol. Trauma 2011, 3, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Jackson Preston, P.; Peterson, H.; Sanchez, D.; Corral Carlos, A.; Reed, A. Serving students takes a toll: Self-care, health, and professional quality of life. J. Stud. Aff. Res. Pract. 2021, 58, 163–178. [Google Scholar] [CrossRef]
- Burke, M.G.; Dye, L.; Hughey, A.W. Teaching Mindfulness for the Self-Care and Well-Being of Student Affairs Professionals. Coll. Stud. Aff. J. 2016, 34, 93–107. [Google Scholar] [CrossRef][Green Version]
- Singer, T.; Klimecki, O.M. Empathy and compassion. Curr. Biol. 2014, 24, R875–R878. [Google Scholar] [CrossRef]
- Pronk, N.P.; Katz, A.S.; Gallagher, J.; Austin, E.; Mullen, D.; Lowry, M.; Kottke, T.E. Adherence to optimal lifestyle behaviors is related to emotional health indicators among employees. Popul. Health Manag. 2011, 14, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Stamm, B.H. The Concise ProQOL Manual. Available online: https://programs.caringsafely.org/wp-content/uploads/2018/01/ProQOL_Concise_2ndEd_12-2010.pdf (accessed on 1 May 2020).
- Stoewen, D.L. Moving from compassion fatigue to compassion resilience Part 2: Understanding compassion fatigue. Can. Vet. J. 2019, 60, 1004–1006. [Google Scholar] [PubMed]
- Figley, C.R. Compassion Fatigue: Secondary Traumatic Stress Disorders from Treating the Traumatized; Routledge, Taylor & Francis Group: Philadelphia, PA, USA, 1995. [Google Scholar]
- Magnavita, N. Work-related psychological injury is associated with metabolic syndrome components in apparently healthy workers. PLoS ONE 2015, 10, e0130944. [Google Scholar] [CrossRef] [PubMed]
- Newell, J.M.; Nelson-Gardell, D.; MacNeil, G. Clinician Responses to Client Traumas: A Chronological Review of Constructs and Terminology. Trauma Violence Abus. 2016, 17, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Lynch, R.J.; Glass, C.R. The Development of the Secondary Trauma in Student Affairs Professionals Scale (STSAP). J. Stud. Aff. Res. Pract. 2018, 56, 1–18. [Google Scholar] [CrossRef]
- Stamm, B.H. Measuring compassion satisfaction as well as fatigue: Developmental history of the compassion satisfaction and fatigue test. In Treating Compassion Fatigue; Figley, C.R., Ed.; Brunner-Routledge: New York, NY, USA, 2002; pp. 107–119. [Google Scholar]
- Raimondi, T.P. Compassion Fatigue in Higher Education: Lessons from Other Helping Fields. Change: Mag. High. Learn. 2019, 51, 52–58. [Google Scholar] [CrossRef]
- Pines, A.; Maslach, C. Characteristics of staff burnout in mental health settings. Psychiatr. Serv. 1978, 29, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Mullen, P.R.; Malone, A.; Denney, A.; Dietz, S.S. Job Stress, Burnout, Job Satisfaction, and Turnover Intention Among Student Affairs Professionals. Coll. Stud. Aff. J. 2018, 36, 94–108. [Google Scholar] [CrossRef]
- Marshall, S.M.; Gardner, M.M.; Hughes, C.; Lottery, U. Attrition from Student Affairs: Perspectives from Those Who Exited the Profession. J. Stud. Aff. Res. Pract. 2016, 53, 146–159. [Google Scholar] [CrossRef]
- Alkema, K.; Linton, J.M.; Davies, R. A study of the relationship between self-care, compassion satisfaction, compassion fatigue, and burnout among hospice professionals. J. Soc. Work. End—Life Palliat. Care 2008, 4, 101–119. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, J.M. Risk of compassion fatigue and burnout and potential for compassion satisfaction among employee assistance professionals: Protecting the workforce. Traumatology 2012, 18, 64–72. [Google Scholar] [CrossRef]
- Dasan, S.; Gohil, P.; Cornelius, V.; Taylor, C. Prevalence, causes and consequences of compassion satisfaction and compassion fatigue in emergency care: A mixed-methods study of UK NHS Consultants. Emerg. Med. J. 2015, 32, 588–594. [Google Scholar] [CrossRef]
- Vilardaga, R.; Luoma, J.B.; Hayes, S.C.; Pistorello, J.; Levin, M.E.; Hildebrandt, M.J.; Kohlenberg, B.; Roget, N.A.; Bond, F. Burnout among the addiction counseling workforce: The differential roles of mindfulness and values-based processes and work-site factors. J. Subst. Abus. Treat. 2011, 40, 323–335. [Google Scholar] [CrossRef]
- Denyes, M.J.; Orem, D.E.; Bekel, G. SozWiss. Self-care: A foundational science. Nurs. Sci. Q. 2001, 14, 48–54. [Google Scholar] [CrossRef]
- Bercier, M.L.; Maynard, B.R. Interventions for Secondary Traumatic Stress with Mental Health Workers. Res. Soc. Work. Pract. 2014, 25, 81–89. [Google Scholar] [CrossRef]
- Bloomquist, K.R.; Wood, L.; Friedmeyer-Trainor, K.; Kim, H.-W. Self-care and Professional Quality of Life: Predictive Factors among MSW Practitioners. Adv. Soc. Work. 2016, 16, 292–311. [Google Scholar] [CrossRef]
- Bressi, S.K.; Vaden, E.R. Reconsidering Self Care. Clin. Soc. Work. J. 2016, 45, 33–38. [Google Scholar] [CrossRef]
- Butler, L.D.; Mercer, K.A.; McClain-Meeder, K.; Horne, D.M.; Dudley, M. Six domains of self-care: Attending to the whole person. J. Hum. Behav. Soc. Environ. 2019, 29, 107–124. [Google Scholar] [CrossRef]
- Newell, J.M. An Ecological Systems Framework for Professional Resilience in Social Work Practice. Soc. Work 2019, 65, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Harmon-Darrow, C.; Frey, J.J. Rethinking professional quality of life for social workers: Inclusion of ecological self-care barriers. J. Hum. Behav. Soc. Environ. 2019, 29, 11–25. [Google Scholar] [CrossRef]
- Harker, R.; Pidgeon, A.M.; Klaassen, F.; King, S. Exploring resilience and mindfulness as preventative factors for psychological distress burnout and secondary traumatic stress among human service professionals. Work 2016, 54, 631–637. [Google Scholar] [CrossRef]
- Rees, C.S.; Eley, R.; Osseiran-Moisson, R.; Francis, K.; Cusack, L.; Heritage, B.; Hegney, D. Individual and environmental determinants of burnout among nurses. J. Health Serv. Res. Policy 2019, 24, 191–200. [Google Scholar] [CrossRef]
- Cook-Cottone, C.P. Mindfulness and Yoga for Self-Regulation: A Primer for Mental Health Professionals; Springer Publishing Company: New York, NY, USA, 2015. [Google Scholar]
- Hotchkiss, J.T. Mindful Self-Care and Secondary Traumatic Stress Mediate a Relationship between Compassion Satisfaction and Burnout Risk among Hospice Care Professionals. Am. J. Hosp. Palliat. Med. 2018, 35, 1099–1108. [Google Scholar] [CrossRef]
- Hotchkiss, J.T.; Lesher, R. Factors Predicting Burnout Among Chaplains: Compassion Satisfaction, Organizational Factors, and the Mediators of Mindful Self-Care and Secondary Traumatic Stress. J. Pastor. Care Couns. 2018, 72, 86–98. [Google Scholar] [CrossRef]
- Guthrie, V.L.; Woods, E.; Cusker, C.; Gregory, M. A Portrait of Balance: Personal and Professional Balance among Student Affairs Educators. Coll. Stud. Aff. J. 2005, 24, 110–127. [Google Scholar]
- Syed, I.U.B. Diet, physical activity, and emotional health: What works, what doesn’t, and why we need integrated solutions for total worker health. BMC Public Health 2020, 20, 152. [Google Scholar] [CrossRef]
- Feng, X.; Mosimah, C.I.; Sizemore, G.; Goyat, R.; Dwibedi, N. Impact of mindful self-care and perceived stress on the health-related quality of life among young-adult students in West Virginia. J. Hum. Behav. Soc. Environ. 2019, 29, 26–36. [Google Scholar] [CrossRef]
- Ullman, J.B.; Bentler, P.M. Structural Equation Modeling. In Handbook of Psychology, 2nd ed.; Tabachnick, B.G., Fidell, L.S., Eds.; Pearson: London, UK, 2012. [Google Scholar]
- Cohen, J. A Power Primer. Sychological Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Heritage, B.; Rees, C.S.; Hegney, D.G. The ProQOL-21: A revised version of the Professional Quality of Life (ProQOL) scale based on Rasch analysis. PLoS ONE 2018, 13, e0193478. [Google Scholar] [CrossRef] [PubMed]
- Cook-Cottone, C.P.; Guyker, W.M. The Development and Validation of the Mindful Self-Care Scale (MSCS): An Assessment of Practices that Support Positive Embodiment. Mindfulness 2018, 9, 161–175. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Health-related quality-of-life measures—United States, 1993. Morb. Mortal. Wkly. Rep. 1995, 44, 195–200. [Google Scholar]
- Yin, S.; Njai, R.; Barker, L.; Siegel, P.Z.; Liao, Y. Summarizing health-related quality of life (HRQOL): Development and testing of a one-factor model. Popul. Health Metr. 2016, 14, 22. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing, Version = 1.9.12. R Foundation for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 1 January 2020).
- Multivariate Software Inc. EQS-Structural Equation Modeling Software Software [Computer Software]. Available online: http://www.mvsoft.com (accessed on 1 May 2020).
- Yuan, K.H.; Lambert, P.L.; Fouladi, R.T. Mardia’s multivariate kurtosis with missing data. Multivar. Behav. Res. 2004, 39, 413–437. [Google Scholar] [CrossRef]
- Little, R.J.A. A test of missing completely at random for multivariate data with missing values. J. Am. Stat. Assoc. 1988, 83, 1198–1202. [Google Scholar] [CrossRef]
- Beaujean, A.A. BaylorEdPsych: R Package for Baylor University Educational Psychology Quantitative Courses, R Package Version 0.5. Available online: http://CRAN.R-project.org/package=BaylorEdPsych (accessed on 1 May 2020).
- Awa, W.L.; Plaumann, M.; Walter, U. Burnout prevention: A review of intervention programs. Patient Educ. Couns. 2010, 78, 184–190. [Google Scholar] [CrossRef]
- Ruiz-Fernandez, M.D.; Ortega-Galan, A.M.; Fernandez-Sola, C.; Hernandez-Padilla, J.M.; Granero-Molina, J.; Ramos-Pichardo, J.D. Occupational Factors Associated with Health-Related Quality of Life in Nursing Professionals: A Multi-Centre Study. Int. J. Environ. Res. Public Health 2020, 17, 982. [Google Scholar] [CrossRef]
- Lynch, R.J. The Development and Validation of the Secondary Trauma in Resident Assistants Scale. J. Coll. Univ. Stud. Hous. 2017, 44, 10–29. [Google Scholar]
- Maslach, C. Understanding Burnout: Definitional Issues in Analyzing a Complex Phenomenon; Paine, W.S., Ed.; Sage: Beverly Hills, CA, USA, 1982. [Google Scholar]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).