
An Australian Approach to Managing Traumatic Abdominal Wall Hernias

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics and Presentation
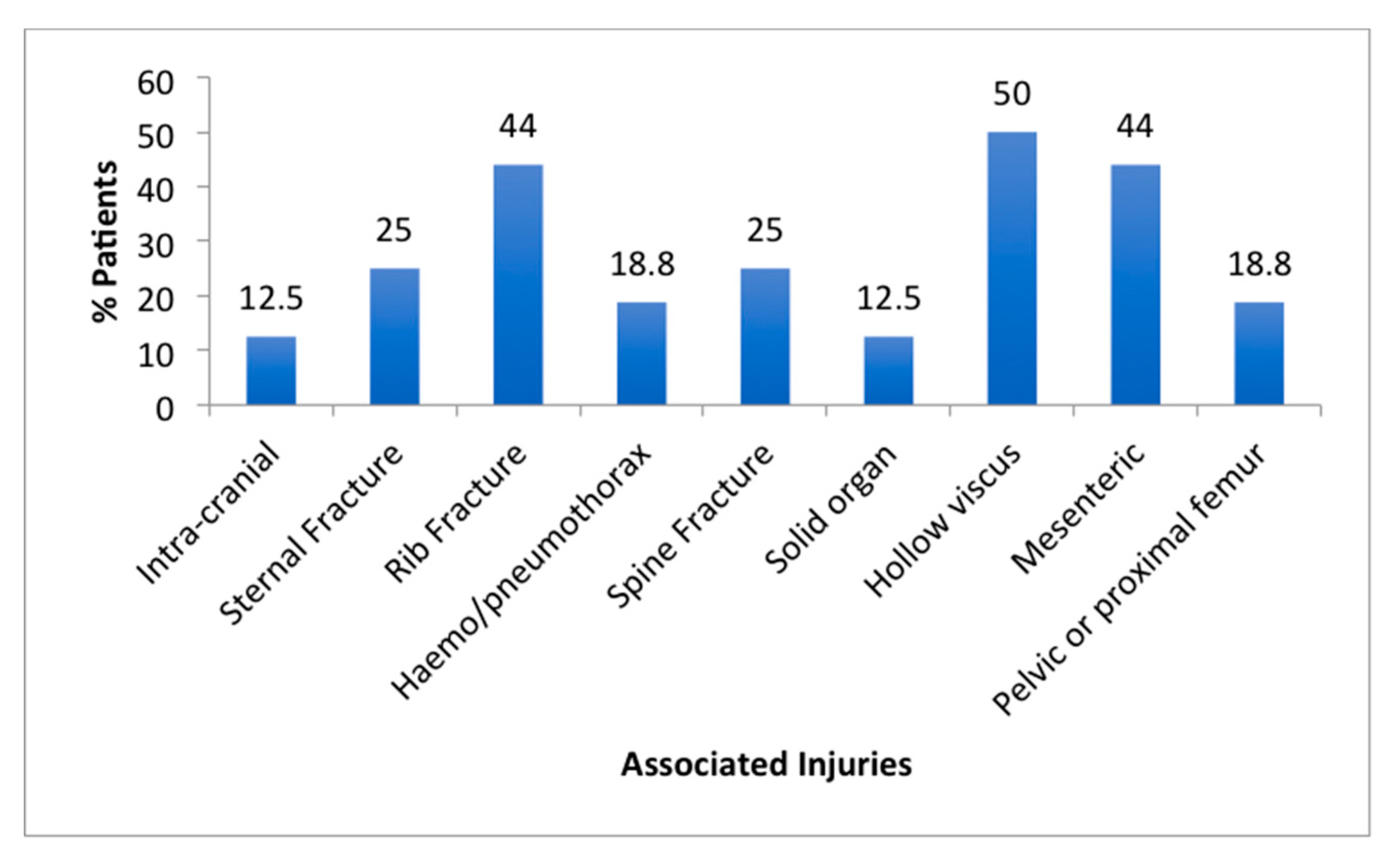
3.2. Pattern of Injury
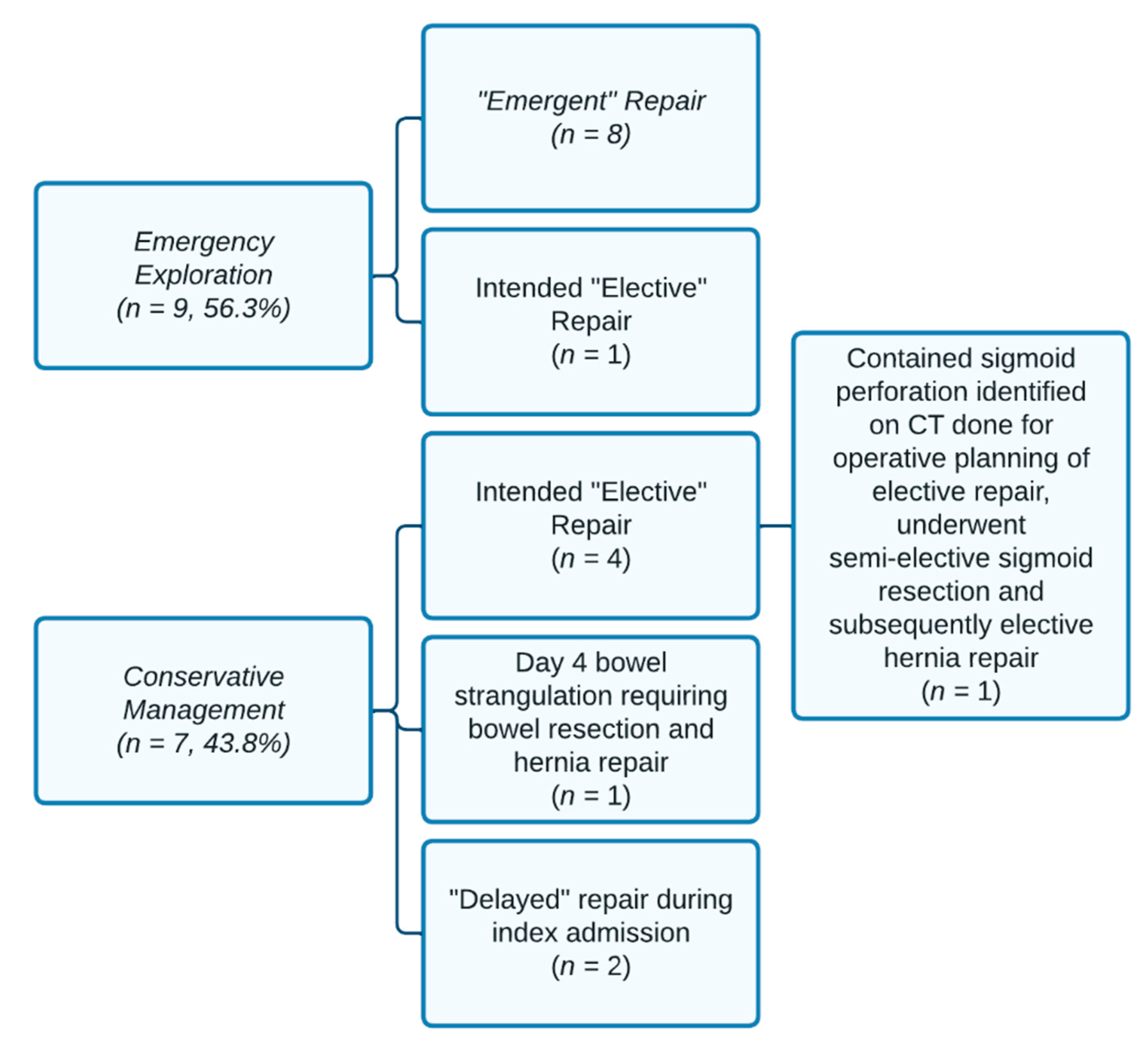
3.3. Urgent Surgical Exploration
3.4. Conservative Management
3.5. Approach to Repair
3.6. Follow-Up
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Honaker, D.; Green, J. Blunt traumatic abdominal wall hernias: Associated injuries and optimal timing and method of repair. J. Trauma Acute Care Surg. 2014, 77, 701–704. [Google Scholar] [CrossRef] [PubMed]
- Netto, F.A.; Hamilton, P.; Rizoli, S.B.; Nascimento, B., Jr.; Brenneman, F.D.; Tien, H.; Tremblay, L.N. Traumatic abdominal wall hernia: Epidemiology and clinical implications. J. Trauma Acute Care Surg. 2006, 61, 1058–1061. [Google Scholar] [CrossRef] [PubMed]
- Dennis, R.W.; Marshall, A.; Deshmukh, H.; Bender, J.S.; Kulvatunyou, N.; Lees, J.S.; Albrecht, R.M. Abdominal wall injuries occurring after blunt trauma: Incidence and grading system. Am. J. Surg. 2009, 197, 413–417. [Google Scholar] [CrossRef] [PubMed]
- Akbaba, S.; Gundogdu, R.H.; Temel, H.; Oduncu, M. Traumatic Abdominal Wall Hernia: Early or Delayed Repair? Indian J. Surg. 2015, 77 (Suppl. 3), 963–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karhof, S.; Boot, R.; Simmermacher, R.K.J.; van Wessem, K.J.P.; Leenen, L.P.H.; Hietbrink, F. Timing of repair and mesh use in traumatic abdominal wall defects: A systematic review and meta-analysis of current literature. World J. Emerg. Surg. 2019, 14, 59. [Google Scholar] [CrossRef] [PubMed]
- Esposito, T.J.; Fedorak, I. Traumatic lumbar hernia: Case report and literature review. J. Trauma. 1994, 37, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Mahajna, A.; Ofer, A.; Krausz, M.M. Traumatic abdominal hernia associated with large bowel strangulation: Case report and review of the literature. Hernia 2004, 8, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Coleman, J.J.; Fitz, E.K.; Zarzaur, B.L.; Steenburg, S.D.; Brewer, B.L.; Reed, R.L.; Feliciano, D.V. Traumatic abdominal wall hernias: Location matters. J. Trauma Acute Care Surg. 2016, 80, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.; Jain, S.K.; Arora, J.K.; Sharma, P.; Sharma, A.; Bhagwan, J.; Goyal, K.; Sahoo, B.S. Traumatic abdominal wall hernia: Delayed repair: Advantageous or taxing. Int. J. Surg. Case Rep. 2013, 4, 36–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singal, R.; Gupta, R.; Mittal, A.; Gupta, A.; Singal, R.P.; Singh, B.; Gupta, S.; Mittal, G. Delayed presentation of the traumatic abdominal wall hernia; dilemma in the management—Review of literature. Indian J. Surg. 2012, 74, 149–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pardhan, A.; Mazahir, S.; Rao, S.; Weber, D. Blunt Traumatic Abdominal Wall Hernias: A Surgeon’s Dilemma. World J. Surg. 2016, 40, 231–235. [Google Scholar] [CrossRef]
- Abbreviated Injury Scale: 2015 Revision, 6th ed.; Association for the Advancement of Automotive Medicine: Chicago, IL, USA, 2018.
- Selby, C.D. Direct abdominal hernia of traumatic origin. J. Am. Med. Assoc. 1906, 47, 1485–1486. [Google Scholar] [CrossRef] [Green Version]
- Sall, I.; El Kaoui, H.; Bouchentouf, S.M.; Ait Ali, A.; Bounaim, A.; Hajjouji, A.; Baba, H.; Fahssi, M.; Alhyane, A.; Zentar, A.; et al. Delayed repair for traumatic abdominal wall hernia: Is it safe? Hernia 2009, 13, 447–449. [Google Scholar] [CrossRef] [PubMed]
- Hickey, N.A.; Ryan, M.F.; Hamilton, P.A.; Bloom, C.; Murphy, J.P.; Brenneman, F. Computed tomography of traumatic abdominal wall hernia and associated deceleration injuries. Can. Assoc. Radiol. J. 2002, 53, 153–159. [Google Scholar] [PubMed]
- Chow, K.L.; Omi, E.C.; Santaniello, J.; Lee, J.K.; McElmeel, D.P.; Thomas, Y.M.; Cartolano, T.J.; Doherty, J.C.; Smith-Singares, E. Traumatic abdominal wall hernias: A single-center case series of surgical management. Trauma Surg. Acute Care Open. 2020, 5, e000495. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Demographics | n = 16 | Patients (%) |
|---|---|---|
| Age | Median 36 (Range 18–59) years | |
| Gender | Male | 10/16 (62.5%) |
| Female | 6/16 (37.5%) | |
| ISS | Median 19.5 (Range 5–34) | |
| Mechanism of Injury | Motor Vehicle (Car) Accident | 12/16 (75%) |
| Crush Injury | 3/16 (18.8%) | |
| Motor Bike Accident | 1/16 (6.3%) | |
| Motor Vehicle Accident Group | Travelling >80 km/h | 8/12 (66.7%) |
| Multi-vehicle accident | 8/12 (66.7%) | |
| Driver of vehicle | 7/12 (58%) | |
| Length of stay | Median 14.5 (Range 2–94) days | |
| Location of Hernia | Right lateral | 6/16 (37.5%) |
| Unilateral Anterior | 3/16 (18.8%) | |
| Bilateral Anterior | 3/16 (18.8%) | |
| Left Lateral | 2/16 (12.5%) | |
| Bilateral Lateral | 1/16 (6.3%) | |
| Left Lateral and Lumbar | 1/16 (6.3%) | |
| Abdominal signs on presentation | MVA group–seatbelt sign documented | 12/12 (100%) |
| Non-MVA group–abdominal contusion documented | 3/4 (75%) | |
| CT trauma series findings | Radiological evidence of TAWH | 16/16 (100%) |
| TAWH included in initial radiology report | 14/16 (87.5%) |
| Emergency Exploration (n = 9) | Type of Injuries Identified | Management | |
|---|---|---|---|
| Intra-abdominal injury identified (n = 7) | Small bowel (n = 4) | Devascularisation due to bucket-handle mesenteric injury (n = 3) Traumatic jejunal perforation(n = 1) | Small bowel resection and anastomosis, and primary repair of TAWH (n = 4) |
| Colonic (n = 2) | Rectosigmoid seromuscular tear (n = 1) | Oversewing of rectosigmoid defect, and mesh repair of TAWH (n = 1) | |
| Devascularisation due to bucket-handle injury of sigmoid mesentery (n = 1) | Hartmann’s procedure, and primary repair of TAWH (n = 1) | ||
| Bladder (n = 1) | Intraperitoneal bladder rupture (n = 1) | Primary bladder repair, TAWH not repaired (n = 1) | |
| No intra-abdominal injury identified (n = 2) | None | Repair of TAWH at exploratory operation (Mesh repair n = 1; Primary repair n = 1) |
| Type of Repair | Patients | ||
|---|---|---|---|
| Primary (n = 7, 54%) | Timing of repair | Emergent | 6/7 (85.7%) |
| Delayed | 0/7 (0%) | ||
| Elective | 1/7 (14.3%) | ||
| Surgical Wound Type | Dirty/Contaminated/Clean-contaminated | 5/7 (71.4%) | |
| Clean | 2/7 (28.6%) | ||
| Mesh (n = 6, 46%) * | Timing of repair | Emergent | 2/6 (33.3%) |
| Delayed | 3/6 (50%) | ||
| Elective | 1/6 (16.7%) | ||
| Surgical Wound Type | Dirty/Contaminated/Clean-contaminated | 1/6 (16.7%) | |
| Clean | 5/6 (83.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liesegang, A.G.; Murphy, S.J.; Theodore, J.E.; Webb, P.M.; Sethi, H.; Lockwood, D.S.R. An Australian Approach to Managing Traumatic Abdominal Wall Hernias. Trauma Care 2022, 2, 260-267. https://doi.org/10.3390/traumacare2020022
Liesegang AG, Murphy SJ, Theodore JE, Webb PM, Sethi H, Lockwood DSR. An Australian Approach to Managing Traumatic Abdominal Wall Hernias. Trauma Care. 2022; 2(2):260-267. https://doi.org/10.3390/traumacare2020022
Chicago/Turabian StyleLiesegang, Amanda G., Skyle J. Murphy, Jane E. Theodore, Peita M. Webb, Harsheet Sethi, and David S. R. Lockwood. 2022. "An Australian Approach to Managing Traumatic Abdominal Wall Hernias" Trauma Care 2, no. 2: 260-267. https://doi.org/10.3390/traumacare2020022
APA StyleLiesegang, A. G., Murphy, S. J., Theodore, J. E., Webb, P. M., Sethi, H., & Lockwood, D. S. R. (2022). An Australian Approach to Managing Traumatic Abdominal Wall Hernias. Trauma Care, 2(2), 260-267. https://doi.org/10.3390/traumacare2020022