1. Introduction
With an incidence of 7 deaths per 100,000, self-inflicted gunshot wounds (SIGSWs) to the face are the leading cause of gun-related deaths in the United States. For those that survive, SIGSWs produce devastating facial defects that pose a challenging problem for reconstructive surgeons. GSWs may be classified as low- or high-velocity and cause direct damage at the point of entry, followed by a shock wave that secondarily injures distant tissues. Injuries are highly variable, and are dependent on the tissue strength of anatomic sites and firearm characteristics such as bullet caliber and muzzle velocity [
1]. SIGSWs are generally more complex than GSWs characteristic of interpersonal violence. Because the firearm is always placed in close proximity to the face, SIGSWs lead to greater impact injuries resulting in greater bony comminution and soft tissue avulsion [
1,
2,
3]. Despite this, many patients with facial SIGSWs survive, particularly if young and lacking penetrating brain injury [
4]. As such, the armamentarium required to tackle such severe injuries is vast [
5,
6,
7].
A paradigm shift in recent decades has prioritized performing primary reconstruction for victims of severe facial trauma within 48 or 72 h [
1,
3,
5,
7,
8,
9,
10]. While principles of early reconstruction have been advocated for facial GSWs for some time, only recently have their merits and feasibility been investigated for isolated facial SIGSWs [
11]. The classical approach to maxillofacial injuries following patient stabilization includes the judicious debridement of nonviable tissue, the exposure of all fracture fragments, precise internal rigid fixation with immediate bone grafting, and definitive soft-tissue coverage. This allows for the rapid re-establishment of a scaffold upon which soft tissues can settle, thereby reducing scar contracture and improving overall cosmetic outcomes [
7,
12]. Afterwards, secondary reconstruction can refine the form and function of detailed facial structures. Reconstructive challenges are numerous, including limited tissue volume, modest vascularity, a hostile wound environment, and the complexity of severe composite defects. However, the advent of sophisticated free tissue transfer techniques has revolutionized the capacity to tackle large, complex defects of the face [
5,
8,
9,
13]. The ability to introduce reliable well-vascularized tissue that is less bulky and more easily contourable than many local flaps allows for the rapid definitive reconstruction of both bone and soft tissue without compromising survivability.
The overall uncommon incidence of SIGSWs, high mortality rate, and heterogenous nature of structural and psychosocial trauma inherent to the mechanism create a paucity of comprehensive studies examining reconstructive management, complications, and outcomes among this specific subset of patients [
11]. The aims of this study were to (1) characterize SIGSWs to the face and the reconstructive trends at our center, and (2) identify parameters influencing complications and outcomes among survivors of SIGSWs following facial reconstruction.
2. Materials and Methods
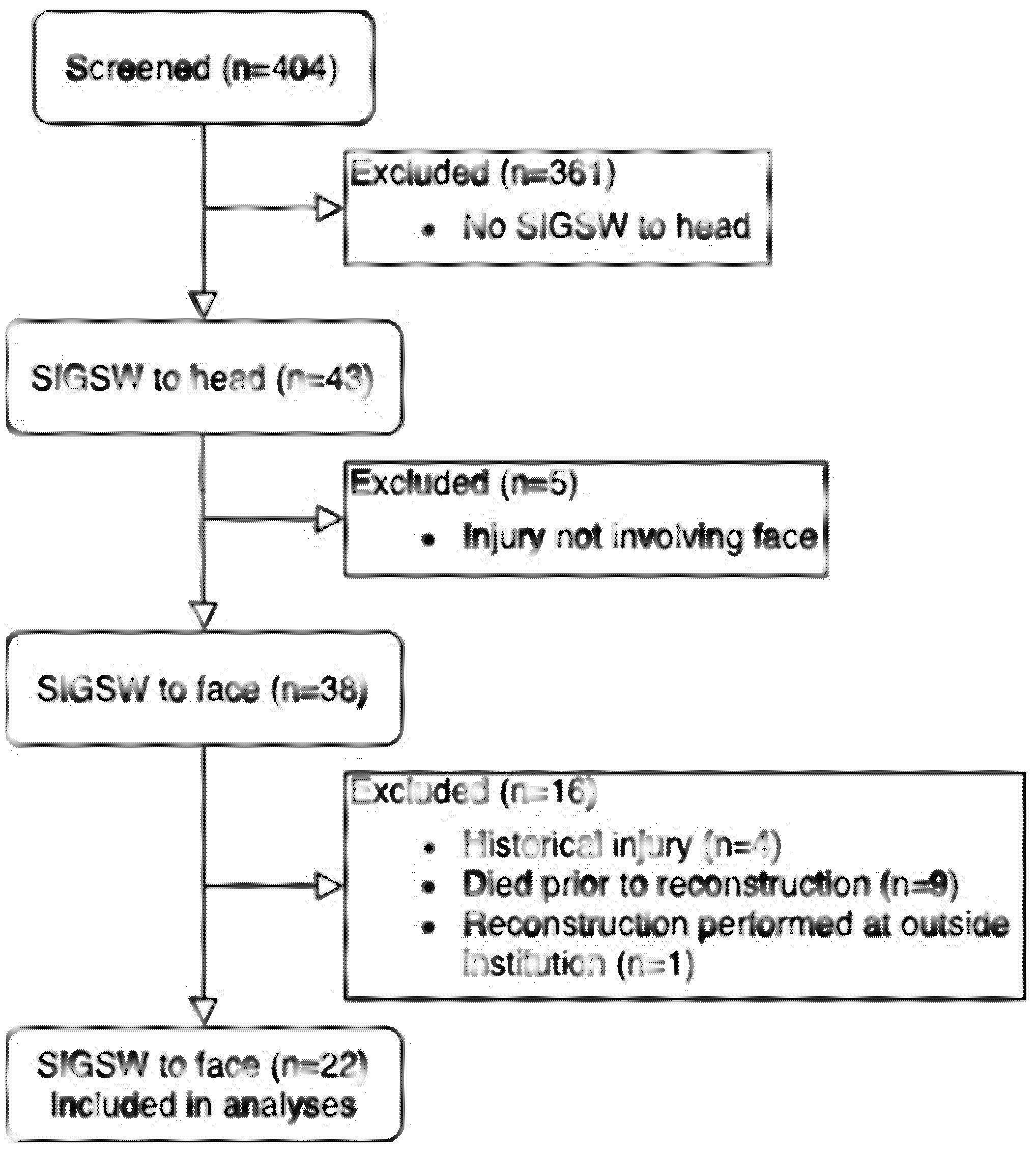
After approval by the Institutional Review Board, medical records of 404 adult patients with possible SIGSWs to the head were retrospectively reviewed. These patients presented within a ten-year period from January 2009 to December 2019 at a tertiary-care level 1 trauma center in Milwaukee, Wisconsin. Given the lack of uniform coding of facial SIGSWs, it was necessary to identify subjects utilizing a combination of International Classification of Disease-9 and 10 diagnoses including codes for intentional self-harm or suicide (by firearm), accidental or undetermined discharge from firearm, suicide attempt, head injury, and other modifiers including procedure and provider codes.
After generating a list of potential subjects with these coded diagnoses, charts had been manually examined to confirm a SIGSW to the head before data were extracted to a Microsoft Excel spreadsheet. Patients were excluded from further analysis if they had not suffered a SIGSW to the face (i.e., had an isolated calvarial injury), had not required or proceeded with a reconstructive procedure, had died, had had incomplete records, or had had historical SIGSWs reconstructed at other centers. Following subject exclusion, a comprehensive extraction of patient data was performed from patient charts. Outcome measures were assessed by review of follow-up documentation with reconstructive-service or primary-care physicians.
Factors and endpoints were defined as follows: a reconstructive procedure was defined as any procedure that aimed to restore lost form and function, including: bony fixation, laceration repairs including those at the bedside, local and free tissue transfers including grafts and flaps, staged debulking, the implantation or removal of hardware and tissue expanders, and complication takebacks to the operating room. Postinjury infection was defined as an infection occurring within 30 days of injury after receiving prophylactic antibiotics within 8 h of admission and continued for at least 48 h without evidence of infection. Wound healing was coded as “well-healed” if documented as such, and no complaints were reported. Completed reconstruction was defined as the surgeon documenting the transition to as-needed or simple monitoring follow-ups. Patients were considered to be lost to follow-up if they did not meet these criteria or if the surgeon documented intention to reassess the need for additional procedures without the patient returning to do so.
All statistical analyses were conducted using R. Fischer’s exact test was used to compare categorical outcomes. The Wilcoxon rank-sum test was used to compare continuous outcomes. Continuous independent variables were analyzed via logistic or linear regression. Statistical significance was set to α < 0.05. All patients depicted in photographs gave signed consent to allow their use.
3. Results
Through our database queries, 404 patients were identified as potentially having had a SIGSW to the head. Of those, 84 patients were shot in the head, with 43 being self-inflicted. Following exclusion (
Figure 1), 22 patients were included in our analysis.
Patient characteristics of our sample are shown in
Table 1. Patients were primarily Caucasian males with a mean age of 45.3 years old (range: 18 to 76); there were no African Americans despite a relatively high local population. Injury characterization is shown in
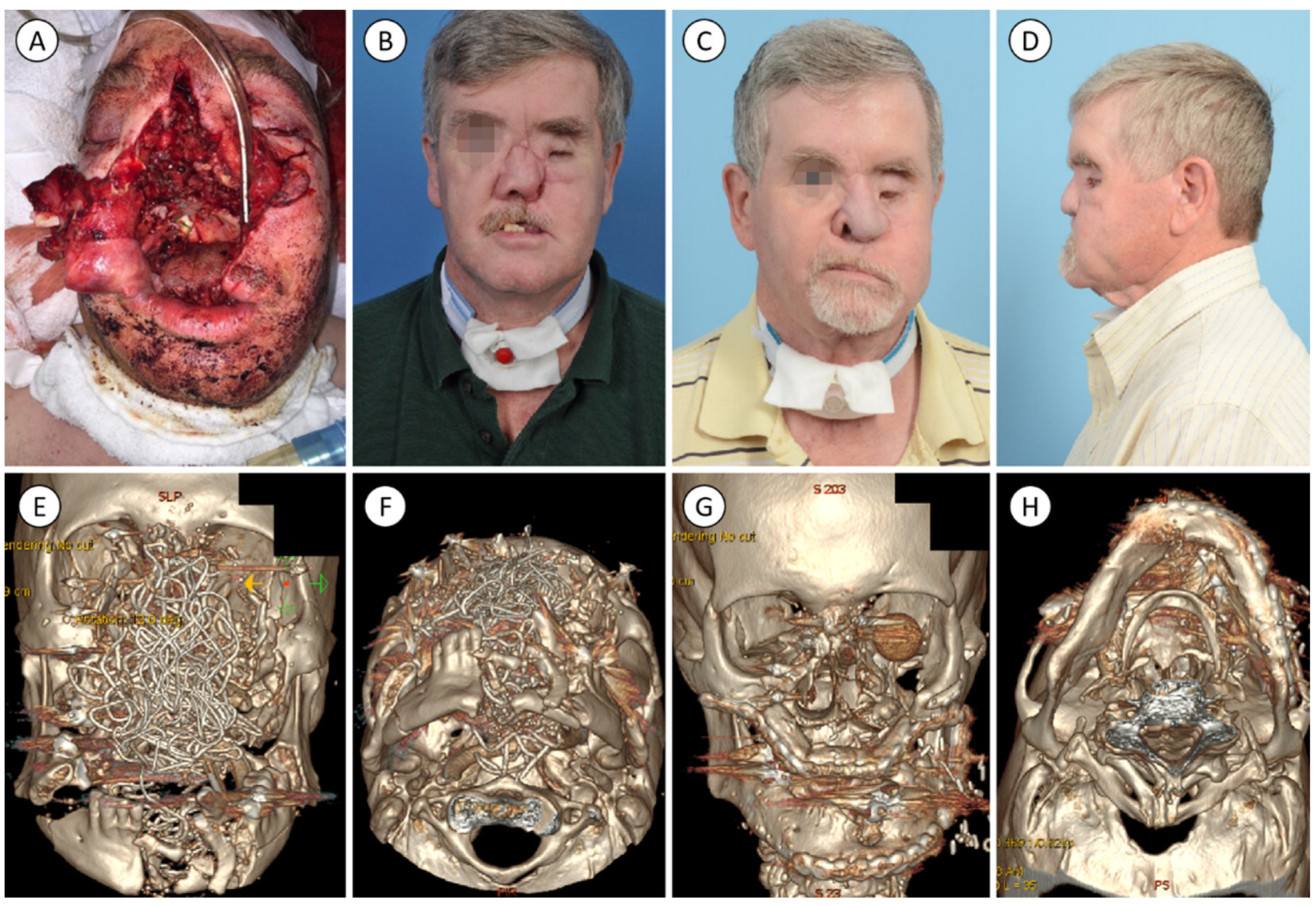
Table 2. Nine (40.9%) individuals used a handgun, five (22.7%) used a rifle, and eight (36.4%) utilized a shotgun. The most common orientation was submental (59.1%). All wounds were classified as Sherman and Parish type III. The midface was injured in all patients, while the single most injured bony structure was the mandible (
Figure 2 and
Figure 3). Soft tissue defects were considered severe in thirteen cases and were more commonly associated with shotgun and rifle injuries. Prior to injury, many patients had significant psychiatric morbidity and psychosocial stressors (
Table 3).
Information about initial management and reconstructive course is shown in
Table 4. Patients averaged 21.7 days in the hospital following SIGSW (range: 2 to 67 days). Average time to debridement was 17.4 h (range: 0.2 to 123 h), and to soft-tissue closure was 1.1 days (range: 0 to 10). The majority of patients (81.8%) required bony fixation. Among those with fractures requiring fixation, average time to fixation was 2.6 days (range: 0 to 8); however, nine (50%) were fixated within 48 h and only five (27.8%) took longer than 72 h. Ampicillin or sulbactam was the preferred prophylactic antibiotic upon entering the trauma bay and perioperative antibiotic during primary reconstruction. Including prophylaxis, the average length of antibiotic treatment in the initial hospital stay was 20.1 days (range: 1 to 60).
Patients averaged 5.4 reconstructive surgeries (range: 1 to 26), although some patients moved away or were lost to follow-up. Nine patients (40.9%) had 5 or more procedures, and three (13.6%) had 10 or more. Five patients (22.7%) ultimately received at least one regional flap, while seven (31.8%) received at least one free flap. Seven (31.8%) of these were free fibulas: four for mandibular and three for maxillary reconstruction. There were 11 regional and 11 free flaps performed in total, including 2 radial forearm flaps, 1 anterolateral thigh flap, and 1 serratus anterior flap. The average time to initiating secondary reconstruction with a free or regional flap was 179 days (range: 9 to 676), although four of the seven patients began within 60 days.
Complications and other outcome measures are shown in
Table 5 and
Table 6, respectively. Fifteen patients (68.2%) had at least one major complication requiring medical or surgical intervention. Nine patients (40.9%) ultimately had infectious complications, although only five (22.7%) were within the first 30 days. Many patients were lost to follow-up, with a mean time from initial presentation to most recent follow-up of 2.5 years. Thirteen patients (59.1%) successfully completed reconstruction. Despite an expected degree of functional sequalae in many patients, patients ultimately healed well, and over 80% recovered substantial function in certain domains. Eight patients (36.4%) had confirmed employment at the time of final follow-up. All patients with severe soft-tissue injury were subjectively deemed to have an improved cosmetic outcome following reconstruction. Three patients died: the first from metastatic cancer, the second following a seizure secondary to a known disorder, and the third from a traumatic brain injury during an unrelated incident. Fourteen patients (63.6%) were confirmed to have visited outpatient mental health. No patients reattempted suicide.
Selected comparisons between factors and outcomes are shown in
Table 7. Not all analyses are shown for brevity. Associations reaching statistical significance included handguns being less likely to receive a free flap (95% CI: 0–0.71,
p = 0.016), rifle injuries with functional impairments in swallowing (95% CI: 1.02–1317.71,
p = 0.023), submental orientation with a longer initial length of stay (LOS) (95% CI: −32.99–−3.00,
p = 0.027), external fixation with a longer LOS (95% CI: −53.00–−12.00,
p = 0.014), financial stressors with a shorter LOS (95% CI: 0.99–32.00,
p = 0.031), and severe soft tissue injury with an increased total number of reconstructive surgeries (95% CI: –6.00–0.00,
p = 0.039) and with incomplete reconstruction (95% CI: 0.0015–0.99,
p = 0.031).
4. Discussion
SIGSWs to the face lead to significant morbidity for those who survive. Patients are not only left aesthetically and functionally disfigured, but also psychologically harmed. Furthermore, a review of our practice reveals an overall high incidence of complications among patients with SIGSWs to the face despite efforts to follow classic principles of post-traumatic management and reconstruction. This is not unexpected given the massive, unpredictable, and heterogeneous nature of these injuries. Despite these difficulties, it is evident that facial reconstruction following SIGSW could provide substantial functional and aesthetic recovery.
The observed injury pattern mimics what was seen among other groups [
4,
5,
13]. Over half the cohort attempted a submental approach, which was associated with longer admission. This is common among rifle and shotgun injuries because their longer barrels make them difficult to otherwise position. Survival and reconstruction are more likely in comparison to lateral approaches, as the bullet trajectory is less aligned with the brain and impacts multiple bones that absorb kinetic energy [
14]. While this results in the formation of secondary projectiles that further propagate damage, the decreased kinetic energy may not be enough to penetrate the cranium [
15]. Lastly, the awkwardness of positioning such a long object while simultaneously pulling the trigger may yield a reflexive jerking extension of the neck, resulting in shifting out of position and missing critical structures [
16]. This may explain the association between rifle use and dysfunctional swallowing, perhaps representing supplementary pharyngeal injury.
While submental injuries may result in the greatest amount of secondary trauma, they could also cause more manageable injuries. Submental shots where the muzzle is placed directly under the chin, posterior to the arch of the mandible, or such that the bullet path is anterior to the midpoint of the mandible may result in primarily soft tissue injuries. Return of function and cosmesis may be achieved with a lower number of procedures, as significant damage to the periosteum and bone is avoided [
5,
16]. However, the loss of soft tissue may hinder achieving early primary closure. Murphy et al. found that delayed primary reconstruction was more common in submental wounds versus intraoral or frontal approaches [
11].
Our mean time to fixation was longer than anticipated. Although we had discussed the benefits of early fixation, we were still able to achieve acceptable results with deferred fixation. Indeed, several studies examining survivors of facial GSWs or SIGSWs are dubious in establishing significant differences between timing of repair. Over the course of 54 free flaps, Futran et al. did not find early bony fixation or soft-tissue coverage to be associated with any outcome measure or complication [
5]. One group [
17] found that time to repair was unrelated to development of complications, while another [
18] found an increase in technical errors among delayed repairs, but not infection or nonunion. Danino et al. abstained from bony primary reconstruction entirely, instead simply reconstructing the soft-tissue framework with a single multiple island latissimus flap [
19]. These reports, in addition to our experience, suggests that acceptable results can be achieved even if delaying fixation is necessary.
Reasonably good cosmesis was achieved overall, even among patients requiring many operations (
Figure 2 and
Figure 3). We utilized a relatively high number of free flaps relative to published reports of other centers [
5,
8,
11]. Although primary soft-tissue coverage was performed quickly, secondary reconstruction with vascularized tissue transfer was delayed in comparison to others such as Sun et al., who reported commencing free tissue transfer in a mean 38 days. While early primary closure is preferable, the timing of secondary reconstruction is more flexible. Benefits of delayed reconstruction include allowing the wound bed to sterilize and become less edematous, allowing for better assessment of underlying maxillofacial structures [
8]. Indeed, the practice of Futran et al. does not impose temporal limitations while performing staged reconstruction, instead opting to set a goal checklist for each phase [
5]. Despite pursuing later secondary reconstruction, we still achieved satisfactory results.
Facial GSWs are at a particularly high risk for infection. Ballistic wounds are inherently contaminated and can be further contaminated with oronasal secretions. Deeper areas of the face may also be seeded by secondary missile and bony projectile fragments [
9]. Several studies demonstrated high rates of infection among high-velocity injuries to the face [
10,
20], but few studies aimed to elucidate patterns of infection in the context of facial SIGSWs. Fagin et al. found high rates of postinjury infection (35%) among facial SIGSW patients despite the use of prophylactic antibiotics in 88% of cases [
21]. All but one of the patients in our series received prophylactic antibiotics, and we had a lower but still relatively high postinjury infection rate of 22.7%. The high incidence of infection despite prophylactic treatment with broad-spectrum antibiotics and early debridement illustrates the particularly elevated susceptibility of these patients. Even following the initial injury period, these patients remained at significant risk for infection, with four patients developing infections after 30 days. Like others [
9,
11], we were unable to identify a statistically significant predictor of infection, likely due to our limited sample size.
Noninfectious complications in our cohort were primarily related to wound healing. As previously mentioned, colossal trauma to facial architecture coupled by the inherent mechanisms of SIGSWs create an unfavorable wound bed. Previous studies found complex fractures to double the rate of mandibular malunion [
22] and complication rates of 39% were recorded among GSWs traversing the oral cavity [
23]. Sokoya et al. found that, among free-flap recipients, rates of nonunion and overall complications were higher among SIGSWs in comparison to GSWs that were not self-inflicted [
9]. The higher rate of nonunion was attributed to increased body comminution, with likely influences from diabetes and smoking. Smoking tobacco is widely shown to be detrimental to healing following surgery [
24]. Seven patients in our sample continued to use tobacco following reconstruction, and two of three patients with nonunions were smokers. Despite a handful of complications in our series, surgical management resulted in complete resolution apart from a chronic fistula in a single patient.
Only thirteen patients (59.1%) completed reconstruction with their primary reconstructive surgeon before being lost to follow-up. Potential reasons for this loss of follow-up include patients moving away, financial cost, loss of insurance, psychiatric morbidity, or lack of desire for further reconstruction. The index hospitalization for a SIGSW costs nearly
$38,000 on average [
2] and compounded expenditures of secondary reconstruction commonly exceed
$117,000 [
25]. It is critical to understand this phenomenon given the financial and personal costs of staged reconstructive surgery to both the individual and the healthcare system. Curiously, reporting financial concerns as a stressor to SIGSW was significantly associated with a shorter LOS, although causality is uncertain. There are few statistics on incomplete reconstructive courses following facial SIGSW. One Turkish study advocated for doing as much as possible during primary reconstruction as only three out of twelve patients returned for secondary reconstruction, apparently due to disinterest [
26]. Although failing to complete reconstruction was associated with severe tissue injuries, the nature of these injuries warranted a longer reconstructive course and therefore confounds this result. Further studies investigating reasons for loss of follow-up may be worth undertaking.
Despite the many reconstructive challenges faced, most patients healed well with functional breathing, swallowing, and speech. Many patients had residual visual deficits, but only two were completely blind. This was consistent with a prior study that found survivors of SIGSWs to the head often retain well-functioning vision [
25]. It is also notable that, despite relatively low rates of outpatient mental health follow-up, eight individuals went on to resume employment and there were no instances of suicidal recidivism. Discussions of psychosocial outcomes and needs following SIGSW are remarkably insufficient in the literature but are unfortunately beyond the scope of this paper [
24,
27,
28,
29,
30,
31,
32,
33,
34]. Nonetheless, these observations emphasize that these patients may still be very functional in society despite tremendous physical and emotional trauma. Given these findings, we accept the high rate of complications amongst this high-risk group and emphasize that reconstruction following facial SIGSW is a worthwhile endeavor.
For patients with severe facial disfigurement beyond the scope of conventional autologous reconstruction, facial transplantation may offer a final therapeutic option. Over the past two decades, facial transplantation has evolved from an untested experimental strategy to perhaps the final rung on the reconstructive ladder. Transplantation is particularly valuable when catastrophic destruction leaves little original scaffolding for recreation of the midface [
35,
36,
37,
38]. Kiwanuka et al. discussed the aesthetic, functional, and psychosocial outcomes in patients following facial transplant after SIGSW; quality of life was improved in many regards including diet, sensation, and intelligibility of speech, although transplantation is not without morbidity. The consequences of acute rejection and lifelong immunosuppression are consequential, and psychosocial outcomes including self-esteem and depressive symptoms are not universally improved [
6]. Success requires rigorous patient selection and a complex multidisciplinary team; we are yet to implement a facial transplantation program at our institution. Nevertheless, given its valuable increasingly validated benefits, SIGSW as a mechanism of injury should not preclude a patient from facial transplantation provided an equitable and holistic review of candidacy is performed [
37].
This analysis of our experience suffers from several limitations. The retrospective nature of our study means we were unable to determine causality or collect data in all patients, which was already limited in power with only 22 individuals. These associations were also compounded by a lack of standardized controls and the heterogeneity of injuries and patients. These issues are not unique to this study and are commonplace to this challenging population. The propensity towards single-center retrospective chart reviews with fairly small sample sizes was described as a limitation among this area of study [
2,
6,
8,
13,
16,
19,
25,
26,
27,
30,
32,
33]. Lastly, we could not completely evaluate cosmesis due to a lack of photographic documentation in the chart.


 ,
, 



{kind=link}
{kind=link}
{kind=link}