1. Introduction
People’s health and quality of life are strongly influenced by social, political, economic, environmental, and cultural contexts [
1]. In this sense, the current health crisis deriving from COVID-19 is a life event that seems to be impacting people’s mental health negatively [
2,
3,
4,
5,
6,
7,
8], and there are fears that it could increase the risk of DBS, as has been the case in other crises [
4,
5,
6,
7,
8], due to its destructive direct or indirect repercussions on social well-being, mental health, housing, work, and financial security. Some studies, however, have shown that suicide rates may decrease during or immediately after a crisis, with the risk varying from one group of people to another due to, among other aspects, cultural, religious, genetic, and socioeconomic factors [
5]. Indeed, in general terms, there seems to be no clear trend in DBS after, for example, a natural disaster [
9].
1.1. Previous Crises
As an example of the consequences deriving from a global crisis, the mortality data of 27 European countries in the period of the economic recession of 2008 [
10] showed an increase in DBS in men in the first postcrisis year (2009) compared with the eight precrisis years of 2000–2007 (RR = 1.042; CI: 1.035–1.081), while in women, it remained stable (RR = 1.003; CI: 0.995–1.010).
In Spain during the same crisis, pre-to-post comparison (2006–2007 vs. 2011–2012) showed an increase in the prevalence of mental health problems among men (RR = 1.15; CI: 1.04–1.26), while in women, there was a slight decrease (RR = 0.92, CI: 0.87–0.98) [
4]. In the same context, the rate of suicide attempts increased for both sexes during the 5 years after the onset of the crisis (2008–2012) compared with the precrisis period (2003–2007) [
11], and the rate of completed suicides underwent an overall 8% increase during the period 2005–2010, being greater in men (RR = 1.10; CI: 1.026–1.179) than in women (RR = 1.013; CI: 0.894–1.149) [
12].
1.2. Background to the COVID-19 Health Crisis
With respect to the health consequences expected during a health crisis, the immediate antecedent was the 2003 Severe Acute Respiratory Syndrome (SARS) epidemic in which some biopsychosocial risk factors for suicide, such as loneliness, social disconnection, limited access to medical care, and stress induced by the fear of suffering from those factors, were associated with an exceptionally high rate of DBS in persons older than 65, passing from 28.44 per 100,000 inhabitants in 2002 to values in the range from 37.46 to 40.35 depending on the different studies [
13,
14,
15]. Specifically, social disconnection and loneliness, especially in the elderly, could generate or enhance depressive symptoms [
16] and suicidal behaviors [
17,
18,
19,
20,
21,
22].
1.3. COVID-19 Crisis
In Spain, when the World Health Organization declared the emergency situation caused by the epidemic outbreak of COVID-19 [
23] to be an international pandemic, the country’s government adopted the first urgent measures to confront the disease’s spread and its economic impact [
24]. Some days later, on 14 March 2020, it declared a state of alarm to manage the health crisis situation over the whole of the national territory. Confinement was the first measure adopted. This included the “limitation of persons’ freedom of movement,” which meant that the entire Spanish population remained confined to their homes during the time the state of alarm was in force [
25]. These extraordinary measures underwent six continuous extensions until 00:00 h 21 June [
26].
These restrictions on everyday life generated a series of stressors capable of directly affecting people’s health [
2,
3,
27,
28,
29]. The duration of the confinement, the lack of information, the fear of getting ill or infecting others, the frustration caused by being unable to carry out daily activities such as leaving the house, the loss of freedom, the separation from one’s environment, and uncertainty were some of the psychosocial stressors associated with the health crisis situation that were potential generators of negative psychological effects during the pandemic [
30], effects that could be risk factors for suicidal behavior [
4,
5,
6,
7,
8,
31].
Early studies during the first months of the pandemic found no significant increase in DBS. Indeed, while some indicated absence of significant differences in any direction [
32,
33,
34], others found a decrease in suicides during confinement in the first months of the pandemic [
35,
36,
37,
38,
39,
40].
In Massachusetts (USA), no significant differences were observed in the DBS incidence rate registered from March to May 2020 compared with 2019 (RR = 0.94; CI: 0.76–1.15) [
32], neither were any significant differences found for Queensland (Australia) when comparing DBS rates for the period from February to August 2020 with the same period from 2015 to 2019 (RR = 0.94; CI: 0.82–1.06) [
33].
However, in Austria, a significant decrease in DBS was observed in the first 6 months of the response to the pandemic (from April to September of 2020) when compared with the mean of the years 2006 to 2019 (chi-squared = 4.553, df = 1,
p = 0.033), although the comparison by trimesters only showed significance for that from July to September (chi-squared = 4.21, df = 1
p = 0.040) [
39]. In Leipzig (Germany), there was an intra-annual reduction in DBS registered between the confinement and nonconfinement months of 2020, although no significant differences were found when the comparison was with the years 2015–2019 (RR = 1.084; CI: 0.665–1.766) [
34]. In the same line, research in Japan [
35] found a 14% decline during the months of February to June (RR = 0.86; CI: 0.82–0.90) and a 16% increase during the months of July to October (RR = 1.16; CI: 1.11–1.21) relative to the preceding 5 years, although another study in Japan, which compared the period from March to June 2020 with the same period of the preceding 10 years [
36], did not find any significant differences, but it did find an overall decrease in cases. Norway [
37] and Korea [
38] have published DBS statistics for the first months of the pandemic. They both indicate a reduction in DBS compared with previous years, although neither publication included any statistical analysis as to whether the differences were significant.
1.4. Justification for the Study
This work was carried out in the Extremadura region (Spain), which has a censused population of 1,063,565 inhabitants and whose annual rate of DBS has remained fairly stable over the preceding 5 years. Specifically, 2020 showed a slight increase of 3.70% compared with 2019 in particular and of 4.60% compared with the mean of the preceding 5 years (2015–2019). In Spain, apart from overall figures, there are no official data available and no studies that the authors are aware of analyzing the variation in DBS rates in the months of confinement and postconfinement during the COVID-19 crisis. The objective of this study was therefore to determine to what extent and in which sense the period of confinement that was decreed during the state of alarm may have affected the incidence of DBS in the Extremadura region.
4. Discussion
This study aimed at exploring the possible impact of the confinement measures imposed during COVID-19 on the incidence of deaths by suicide in the Extremadura region. Given the antecedents of observations in previous crises on their consequences for people’s mental health and the increase in suicides [
4,
5,
6,
7,
8,
10,
11,
12], a similar impact could be expected during the course of the COVID-19 pandemic. Some studies have already shown the negative consequences of this crisis on mental health [
2,
3,
27,
28,
29], but there as yet seems to be no evidence for any increase in DBS during the confinement period—rather there seems to be stability [
32,
33,
34] or a decline [
35,
36,
37,
38,
39,
40]—and there are still insufficient data to indicate otherwise. Nonetheless, the possible immediate impact in the months following confinement and the general medium and long term impacts remain to be explored in greater depth. At the moment, some data already indicate that the feared increase in DBS could well occur [
35].
Based on this work, it cannot be affirmed that there has been a significant change in the trend of DBS in the region of Extremadura during either the confinement period of 2020 or in the months following confinement. There could be some unidentified factor, apart from the exceptional situation of confinement, underlying the variations observed in the incidence rates because it was impossible to carry out an exhaustive analysis of the potential differentiating variables present in the year 2020 relative to the other years that might have provided some tentative explanation. Specifically, for many cases of DBS in the 2015–2018 period, there was no information available on sociodemographic (age, marital status, etc.), socioeconomic (employment situation), and personal (physical or mental health status, divorce rates, etc.) variables. Hence, the significant difference in DBS for the months of July–October between the years 2020 and 2015 can neither be attributed to chance nor be explained on the basis of the available data.
The incidence for the entire March to June period stayed fairly stable relative to the years preceding the crisis (RR = 0.94; CI: 0.56–1.58). Such a finding is coherent with those of other studies on the incidence of DBS during the first months of the pandemic [
32,
33,
34], especially with the Massachusetts (RR = 0.94; CI: 0.76–1.15) [
32] and the Queensland (RR = 0.94, CI: 0.82–1.06) [
33] studies.
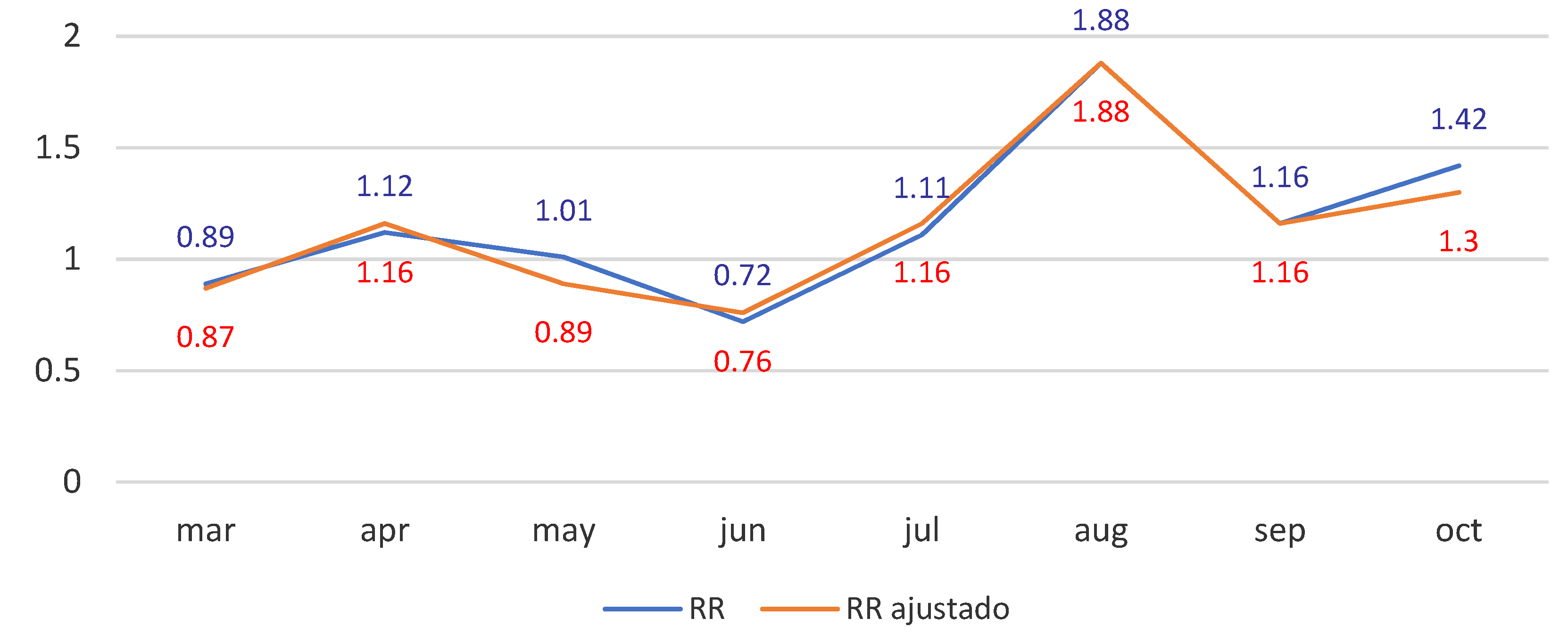
With regard to the rates of DBS observed in the months of July to October, these differences are not coherent with the results reported for Japan (RR = 1.16; CI: 1.11–1.21) [
35], in which there was a significant 16% increase. In our analysis for the Extremadura region, the risk ratios for the years 2017 and 2019 were similar to that of 2020 for these same months, so that one cannot rule out that the variation observed was due to chance.
There are various possible mediating factors underlying these results. The government of Spain approved exceptional economic measures to mitigate the impact of COVID-19. These included actions aimed at strengthening the health sector, protecting families’ welfare, helping employees and self-employed whose incomes had fallen, and supporting firms in terms of liquidity and flexibility so as to minimize unemployment. At the psychoemotional level, the social cohesion at individual, family, and community scales generated by the confinement situation could have acted as a protective factor for mental health [
16], especially against suicidal behavior [
19,
21], by contributing a feeling of security and connection. In addition, the confinement measure may have led to a situation that limited access to lethal means for persons with suicidal ideation or intentions. Given the published data on suicidal ideation at the start of the pandemic [
44], this period could have been one of the incubation of active suicidal ideas, which would ultimately be consummated postconfinement.
Faced with the possible future scenario in which the increases in DBS that occurred in periods subsequent to the immediate stressor could be replicated in other crises, psychosocial interventions for the population at risk could prevent postcrisis complications, reduce mental disorders, improve mental health, and augment these persons’ disaster resilience [
45]. To this end, it is important to recognize the need for mechanisms with which to detect persons at risk of suicide during the postconfinement and postcrisis periods.
Finally, following the recommendations of the WHO [
46], in order to implement preventive programs that stop or reduce such suicidal behaviors, as for example, the existing plans of prevention of Spain’s various Autonomous Communities [
47,
48,
49], it would be necessary to monitor the epidemiological trends of suicide in specific geographic areas through studies that help determine which population groups are at greatest risk, as some affected groups (such as women, adolescents, the elderly, or people with depression and post-traumatic stress disorder) suffer more and are more vulnerable to disasters [
45]. The aforecited reference studies [
32,
33,
34,
35,
36,
37,
38,
39,
40] respond implicitly to the need for this type of research at a local level, and their findings will be of relevance for the design of suicide prevention strategies in their specific zones of study. In this sense, a comparative analysis of the DBS registered by the IMLyCFs of Spain’s various Autonomous Communities would show whether the results of this present study done at a local level are generalizable nationally. A thorough analysis of the cases that occurred during the confinement period by means of psychological autopsies [
50,
51] would complement and enrich research in this area. It would help understand the personal circumstances surrounding the persons who have committed suicide, and thus make it possible to identify possible common risk factors, for example, mental health problems, the situation of social isolation, the feeling or perception of loneliness, and the reduced access to medical attention in persons undergoing medical or psychological treatment [
11,
12,
13].
5. Study Limitations
This research has some limitations. Firstly, the incidence rates calculated from the cases registered in our data source might well increase in the coming months. The cases included in this study that occurred during the confinement and postconfinement periods of 2020 were those unequivocally classified as DBS. However, some deaths currently classified as being of unknown cause might come to be reclassified as DBS. Secondly, as the case frequency is low throughout the series, a variation of just one or two cases translates into a large percentage variation. Thirdly, our study was carried out in a single Spanish region with particular population, sociodemographic, and socioeconomic characteristics. This makes it difficult to generalize the results on a national or international level. Another limitation is that the RR is a measure of the effect that indicates whether the incidence of a phenomenon varies under certain circumstances; in this case, the confinement period, but this measure does not determine causality. We consider that to determine causality during COVID-19 confinement to the possible variation of DBS, it would be necessary to know the specific circumstances of each DBS that occurred throughout the study period 2015–2020, something hardly possible with the data that are usually collected by official sources. For this reason, we recommend a psychological autopsy as the proper methodology to know the particular circumstances of each person who committed suicide.





{kind=link}