
The Effect of the FIFA 11+ on Injury Prevention and Performance in Football: A Systematic Review with Meta-Analysis


Abstract
:1. Introduction
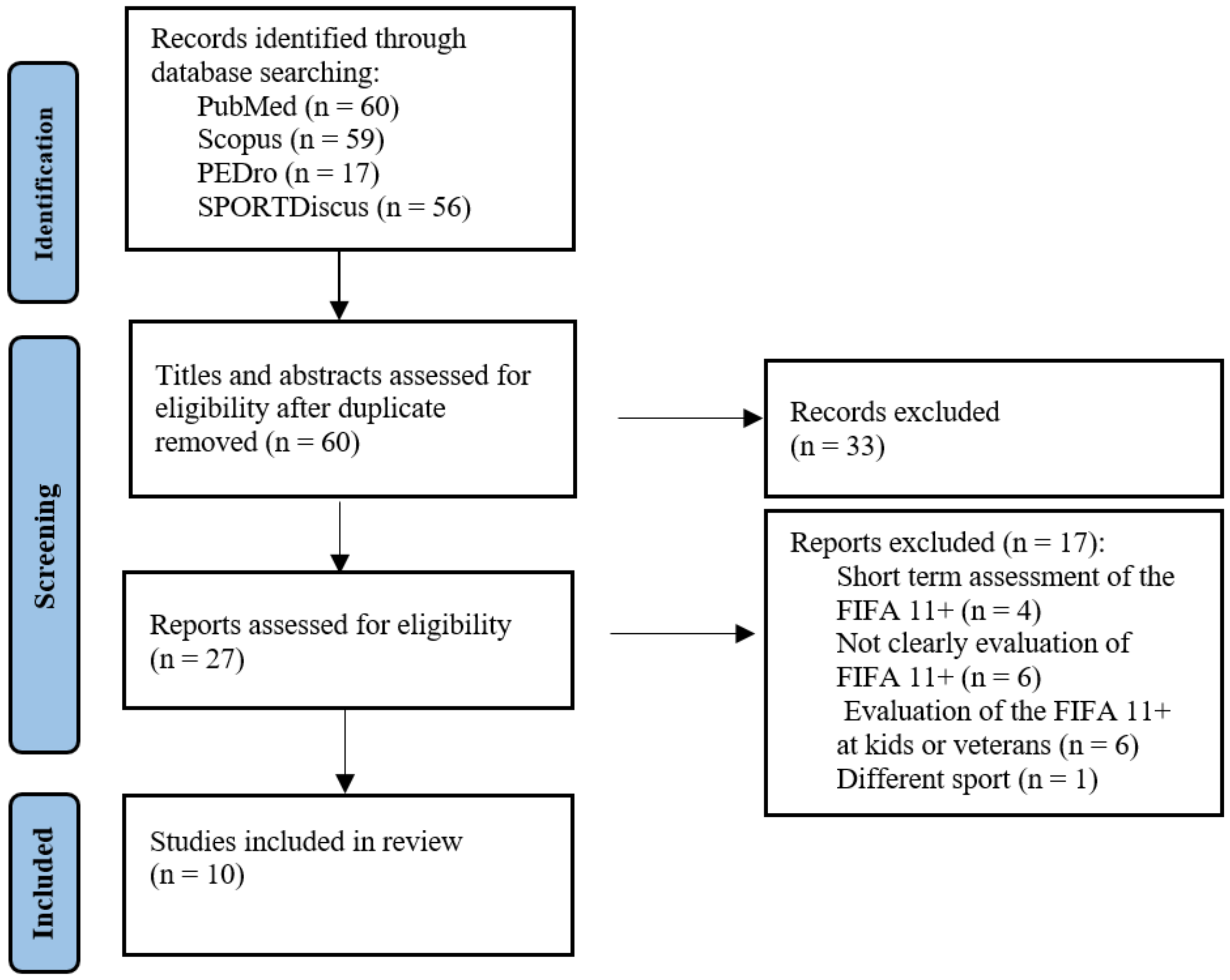
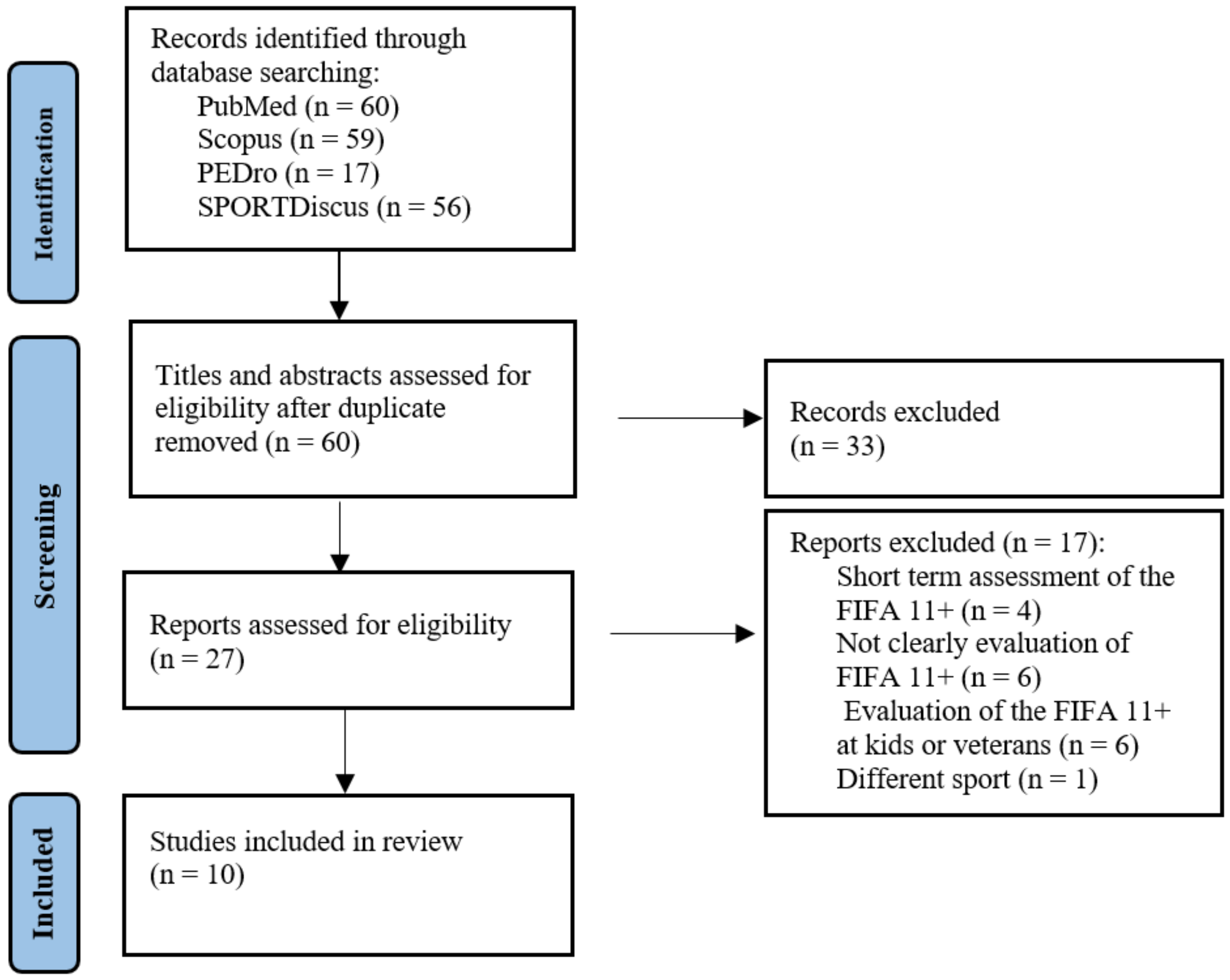
2. Materials and Methods
2.1. Participants
2.2. Intervention
2.3. Comparison Groups
2.4. Outcome Measures
2.5. Study Design
2.6. Quality Assessment
2.7. Data Extraction
2.8. Meta-Analysis
3. Results
3.1. Characteristics of the Studies
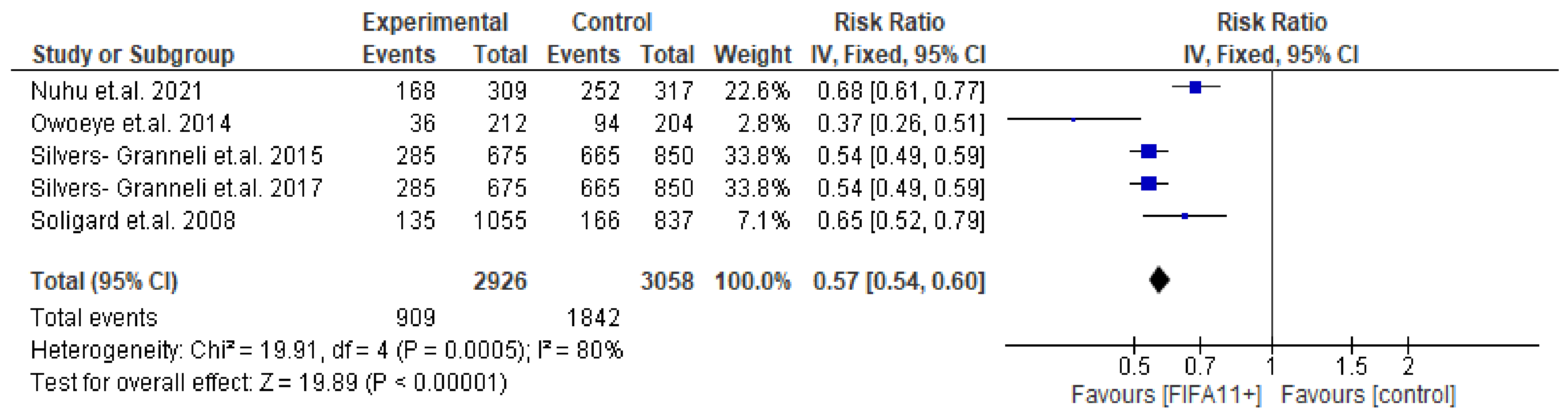
3.2. Injury Prevention
3.3. Severity
3.4. Performance
4. Discussion
4.1. Limitations
4.2. Effectiveness
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pfirrmann, D.; Herbst, M.; Ingelfinger, P.; Simon, P.; Tug, S. Analysis of injury incidences in male professional adult and elite youth soccer players: A systematic review. J. Athl. Train. 2016, 51, 410–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silvers-Granelli, H.J.; Bizzini, M.; Arundale, A.; Mandelbaum, B.R.; Snyder-Mackler, L. Does the FIFA 11+ injury prevention program reduce the incidence of ACL injury in male soccer players? Clin. Orthop. Relat. Res. 2017, 475, 2447–2455. [Google Scholar] [CrossRef] [PubMed]
- Bizzini, M.; Impellizzeri, F.M.; Dvorak, J.; Bortolan, L.; Schena, F.; Modena, R.; Junge, A. Physiological and performance responses to the “FIFA 11+”(part 1): Is it an appropriate warm-up? J. Sports Sci. 2013, 31, 1481–1490. [Google Scholar] [CrossRef]
- Silvers-Granelli, H.; Mandelbaum, B.; Adeniji, O.; Insler, S.; Bizzini, M.; Pohlig, R.; Junge, A.; Snyder-Mackler, L.; Dvorak, J. Efficacy of the FIFA 11+ injury prevention program in the collegiate male soccer player. Am. J. Sports Med. 2015, 43, 2628–2637. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, J.E.; Forte, P.; Ferraz, R.; Leal, M.; Ribeiro, J.; Silva, A.J.; Barbosa, T.M.; Monteiro, A.M. Monitoring Accumulated Training and Match Load in Football: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 3906. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, J.E.; Forte, P.; Ferraz, R.; Leal, M.; Ribeiro, J.; Silva, A.J.; Barbosa, T.M.; Monteiro, A.M. Quantifying Sub-Elite Youth Football Weekly Training Load and Recovery Variation. Appl. Sci. 2021, 11, 4871. [Google Scholar] [CrossRef]
- Teixeira, J.E.; Alves, A.R.; Ferraz, R.; Forte, P.; Leal, M.; Ribeiro, J.; Silva, A.J.; Barbosa, T.M.; Monteiro, A.M. Effects of Chronological Age, Relative Age, and Maturation Status on Accumulated Training Load and Perceived Exertion in Young Sub-Elite Football Players. Front. Physiol. 2022, 13, 832202. [Google Scholar] [CrossRef]
- Barengo, N.C.; Meneses-Echávez, J.F.; Ramírez-Vélez, R.; Cohen, D.D.; Tovar, G.; Correa Bautista, J.E. The impact of the FIFA 11+ training program on injury prevention in football players: A systematic review. Int. J. Environ. Res. Public Health 2014, 11, 11986–12000. [Google Scholar] [CrossRef] [Green Version]
- Soligard, T.; Myklebust, G.; Steffen, K.; Holme, I.; Silvers, H.; Bizzini, M.; Junge, A.; Dvorak, J.; Bahr, R.; Andersen, T.E. Comprehensive warm-up programme to prevent injuries in young female footballers: Cluster randomised controlled trial. BMJ Clin. Res. Ed. 2008, 337, a2469. [Google Scholar] [CrossRef] [Green Version]
- Sadigursky, D.; Braid, J.A.; De Lira, D.N.L.; Machado, B.A.B.; Carneiro, R.J.F.; Colavolpe, P.O. The FIFA 11+ injury prevention program for soccer players: A systematic review. BMC Sports Sci. Med. Rehabil. 2017, 9, 18. [Google Scholar] [CrossRef]
- Gomes Neto, M.; Conceição, C.S.; de Lima Brasileiro, A.J.A.; de Sousa, C.S.; Carvalho, V.O.; de Jesus, F.L.A. Effects of the FIFA 11+ training program on injury prevention and performance in football players: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Paraskevopoulos, E.; Karanasios, S.; Gioftsos, G.; Tatsios, P.; Koumantakis, G.; Papandreou, M. The effectiveness of neuromobilization exercises in carpal tunnel syndrome: Systematic review and meta-analysis. Physiother. Theory Pract. 2022, 1–40. [Google Scholar] [CrossRef] [PubMed]
- Daneshjoo, A.; Mokhtar, A.H.; Rahnama, N.; Yusof, A. Effects of the 11+ and Harmoknee Warm-up Programs on Physical Performance Measures in Professional Soccer Players. J. Sports Sc.i Med. 2013, 12, 489–496. [Google Scholar]
- Stoop, R.; Clijsen, R.; Leoni, D.; Soldini, E.; Castellini, G.; Redaelli, V.; Barbero, M. Evolution of the methodological quality of controlled clinical trials for myofascial trigger point treatments for the period 1978–2015: A systematic review. Musculoskelet. Sci. Pract. 2017, 30, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Moseley, A.M.; Herbert, R.D.; Sherrington, C.; Maher, C.G. Evidence for physiotherapy practice: A survey of the Physiotherapy Evidence Database (PEDro). Aust. J. Physiother. 2002, 48, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ Clin. Res. Ed. 2021, 372, n71. [Google Scholar] [CrossRef]
- Mantel, N.; Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar]
- Akbari, H.; Sahebozamani, M.; Daneshjoo, A.; Amiri-Khorasani, M.; Shimokochi, Y. Effect of the FIFA 11+ on Landing Patterns and Baseline Movement Errors in Elite Male Youth Soccer Players. J. Sport Rehabil. 2020, 29, 730–737. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Bizzini, M.; Dvorak, J.; Pellegrini, B.; Schena, F.; Junge, A. Physiological and performance responses to the FIFA 11+ (part 2): A randomised controlled trial on the training effects. J. Sports Sci. 2013, 31, 1491–1502. [Google Scholar] [CrossRef]
- Nuhu, A.; Jelsma, J.; Dunleavy, K.; Burgess, T. Effect of the FIFA 11+ soccer specific warm up programme on the incidence of injuries: A cluster-randomised controlled trial. PLoS ONE 2021, 16, e0251839. [Google Scholar] [CrossRef]
- Owoeye, O.B.; Akinbo, S.R.; Tella, B.A.; Olawale, O.A. Efficacy of the FIFA 11+ warm-up programme in male youth football: A cluster randomised controlled trial. J. Sports Sci. Med. 2014, 13, 321. [Google Scholar] [PubMed]
- Nawed, A.; Khan, I.A.; Jalwan, J.; Nuhmani, S.; Muaidi, Q.I. Efficacy of FIFA 11+ training program on functional performance in amateur male soccer players. J. Back Musculoskelet. Rehabil. 2018, 31, 867–870. [Google Scholar] [CrossRef] [PubMed]
- Daneshjoo, A.; Mokhtar, A.H.; Rahnama, N.; Yusof, A. The effects of comprehensive warm-up programs on proprioception, static and dynamic balance on male soccer players. PLoS ONE 2012, 7, e51568. [Google Scholar] [CrossRef]
- Ayala, F.; Pomares-Noguera, C.; Robles-Palazón, F.J.; del Pilar García-Vaquero, M.; Ruiz-Pérez, I.; Hernández-Sánchez, S.; Croix, M.D.S. Training effects of the FIFA 11+ and harmoknee on several neuromuscular parameters of physical performance measures. Int. J. Sports Med. 2017, 38, 278–289. [Google Scholar] [CrossRef]
- Alentorn-Geli, E.; Myer, G.D.; Silvers, H.J.; Samitier, G.; Romero, D.; Lázaro-Haro, C.; Cugat, R. Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: Mechanisms of injury and underlying risk factors. Knee Surg. Sports Traumatol. Arthrosc. 2009, 17, 705–729. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Tsuda, E.; Yamamoto, Y.; Maeda, S.; Kimura, Y.; Fujita, Y.; Ishibashi, Y. Core-muscle training and neuromuscular control of the lower limb and trunk. J. Athl. Train. 2019, 54, 959–969. [Google Scholar] [CrossRef] [Green Version]
- Wingfield, K. Neuromuscular training to prevent knee injuries in adolescent female soccer players. Clin. J. Sport Med. 2013, 23, 407–408. [Google Scholar] [CrossRef]
- Rivera, M.J.; Winkelmann, Z.K.; Powden, C.J.; Games, K.E. Proprioceptive training for the prevention of ankle sprains: An evidence-based review. J. Athl. Train. 2017, 52, 1065–1067. [Google Scholar] [CrossRef] [Green Version]
- Brukner, P. Hamstring injuries: Prevention and treatment—An update. Br. J. Sports Med. 2015, 49, 1241–1244. [Google Scholar] [CrossRef] [Green Version]
- Ueno, R.; Navacchia, A.; Schilaty, N.D.; Myer, G.D.; Hewett, T.E.; Bates, N.A. Hamstrings contraction regulates the magnitude and timing of the peak ACL loading during the drop vertical jump in female athletes. Orthop. J. Sports Med. 2021, 9, 23259671211034487. [Google Scholar] [CrossRef]
- Willems, T.M.; Witvrouw, E.; Delbaere, K.; Mahieu, N.; De Bourdeaudhuij, L.; De Clercq, D. Intrinsic risk factors for inversion ankle sprains in male subjects: A prospective study. Am. J. Sports Med. 2005, 33, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Steffen, K.; Emery, C.A.; Romiti, M.; Kang, J.; Bizzini, M.; Dvorak, J.; Finch, C.F.; Meeuwisse, W.H. High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in Canadian youth female football players: A cluster randomised trial. Br. J. Sports Med. 2013, 47, 794–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Close, G.L.; Sale, C.; Baar, K.; Bermon, S. Nutrition for the prevention and treatment of injuries in track and field athletes. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 189–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Studies | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Overall |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Soligard et al., 2008 [9] | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7/10 |
| Owoeye et al., 2014 [21] | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5/10 |
| Akbari et al., 2019 [18] | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6/10 |
| Silvers-Granneli et al., 2017 [2] | Y | Y | N | N | N | N | N | Y | N | Y | Y | 4/10 |
| Silvers-Granneli et al., 2015 [4] | Y | Y | Y | Y | N | N | N | Y | N | Y | Y | 6/10 |
| Nuhu et al.,2021 [20] | Y | Y | Y | N | N | N | Y | Y | Y | Y | Y | 7/10 |
| Impellizzeri et al., 2013 [19] | Y | Y | N | Y | N | N | Y | Y | N | Y | Y | 6/10 |
| Nawed et al., 2018 [22] | N | Y | Y | Y | N | N | N | N | N | Y | Y | 5/10 |
| Daneshjoo et al., 2012 [23] | Y | Y | N | Y | N | N | Y | N | N | Y | Y | 5/10 |
| Ayala et al., 2017 [24] | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5/10 |
| STUDIES | SAMPLE | INTERVENTIONS | PERIOD | RESULTS |
|---|---|---|---|---|
| Silvers-Granneli et al., 2017 [2] | IG = 675 players CG = 850 players Gender: Male Age: 18–25 | IG: FIFA 11+ CG: Conventional warm-up | 3 times/week for 1 season | Total injuries: IG = 285 CG = 665 Knee injuries: IG = 34 CG = 102 Mechanism of ACL: IG = 3 CG = 16 |
| Silvers-Granneli et al., 2015 [4] | IG = 675 players CG = 850 players Gender: Male Age: 18–25 | IG: FIFA 11+ CG: Conventional warm-up | 3 times/week for 1 season | Total injuries: IG = 285 CG = 665 Ankle injuries: IG = 59 CG = 115 Knee injuries: IG = 34 CG = 102 Hamstring injuries: IG = 16 CG = 55 |
| Soligard et al., 2008 [9] | IG = 1055 players CG = 837 Gender: Female Age: 13–17 | IG: FIFA 11+ CG: Conventional warm-up | 3 times/week for 8 months | Total injuries: IG = 135 CG = 166 Acute injuries: IG = 112 CG = 130 Overuse injuries: IG = 27 CG = 48 |
| Nuhu et al., 2021 [20] | IG = 309 players CG = 317 players Gender: Male Mean age: 20 | IG: FIFA 11+ CG: Conventional warm-up | 3 times/week for 7 months | Total injuries: IG = 168 CG = 252 Overuse: IG = 8 CG = 15 Trauma: IG = 160 CG = 191 Severity: Minimal → IG > CG Mild → IG < CG Moderate → IG < CG Severe → IG < CG |
| Owoeye et al., 2014 [21] | IG = 212 players CG = 204 players Gender: Male Mean age: 17.50 | IG: FIFA 11+ CG: Conventional warm-up | 3 times/week for 6 months | Total injuries: IG = 36 CG = 94 Overuse injuries: IG = 2 CG = 14 Acute injuries: IG = 34 CG = 80 Severity: Minimal → IG < CG Mild → IG < CG Moderate → IG < CG Severe → IG > CG (No significant difference) |
| Akbari et al., 2019 [18] | IG = 12 players CG = 12 players Gender: Male Mean age: 16.79 | IG: FIFA 11+ CG: Conventional warm-up | 3 times/week for 8 weeks | LESS Score Landing patterns: IG: High-risk → −2.93 Low-risk → −1.3 CG: High-risk → 0 Low-risk → +0.2 |
| Daneshjoo et al., 2012 [23] | Group A = 12 players Group B = 12 players Group C = 12 players Gender: Male Age: 17–20 | Group A: FIFA 11+ Group B: HarmoKnee Group C: Conventional warm-up | 3 times/week for 2 months | Proprioception: Biodex Isokinetic Dynamometer 30°, 45°, 60° Proprioception error: Group A: 45° → ↓2.8% 60° → ↓ 1.7% Group B: 45° → ↓ 3% 60° → ↓ 2.1% Group C: no significant improvement Dynamic Balance: Star Excursion Balance Test (SEBT) Dynamic Balance: Group A: ↑ 12.4% Group B: ↑ 17.6% Group C: no significant improvement Static Balance: Stork stand balance test Static Balance (eyes open): Group A: ↑ 10.9% Group B: ↑ 6.1% Group C: no significant improvement (eyes closed): Group A: ↑ 12.4% Group B: ↑ 17.6% Group C: no significant improvement |
| Impellizzeri et al., 2013 [19] | IG = 42 players CG = 39 players Gender: Male Mean age: 23.5 | IG: FIFA 11+ CG: Conventional warm-up | 3 times/week for 9 weeks | Time to stabilization: Jump landing task Significant Improvements: Time to stabilization: −2.8% for IG Core stability: −8.9% for IG Concentric/Eccentric strength of flexors/extensors: Cybex NORM isokinetic dynamometer Concentric strength of flexors: IG: ↑ 3.2% Eccentric strength of flexors: IG: ↑ 3.8% |
| Ayala et al., 2017 [24] | Group A: CG = 11 players FIFA 11+ = 10 players Group B: CG = 10 players HarmoKnee = 10 players Gender: Male Mean age: 16.8 | CG: Conventional warm-up | 3 times/week for 4 weeks | Dynamic Postural Control: Y-balance test Significant improvements: Group A (in favor of the FIFA 11+ players): Dynamic Postural Control: anterior ↑ 2.5%, posteromedial ↑ 7.2% Single-legged-hop limb symmetry: ↑ 8.3% Sprint speed: 10 m → −8.4% 20 m →−1.8% Vertical jump: ↑ 9.1% Sprint speed 10 m/20 m: Beam photocell gates Group B (in favor of HarmoKnee players): Sprint speed: 10 m → −2.7% 20 m →−2.9% Vertical drop Jump: Contact platform (Ergojump) Vertical jump: ↑ 9.7% |
| Nawed et al., 2018 [22] | IG = 29 players CG = 28 players Gender: Male Mean age: 20.63 | IG: FIFA 11+ CG: Conventional warm-up | 5 times/week for 12 weeks | Leg power: Vertical Jump Test IG → Significant improvements: leg power → Vertical Jump Test: ↑ 4.67% Sprint speed: 20 m. sprint run test Sprint speed → 20 m. sprint run test: −0.38 s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vlachas, T.; Paraskevopoulos, E. The Effect of the FIFA 11+ on Injury Prevention and Performance in Football: A Systematic Review with Meta-Analysis. BioMed 2022, 2, 328-340. https://doi.org/10.3390/biomed2030026
Vlachas T, Paraskevopoulos E. The Effect of the FIFA 11+ on Injury Prevention and Performance in Football: A Systematic Review with Meta-Analysis. BioMed. 2022; 2(3):328-340. https://doi.org/10.3390/biomed2030026
Chicago/Turabian StyleVlachas, Theodosis, and Eleftherios Paraskevopoulos. 2022. "The Effect of the FIFA 11+ on Injury Prevention and Performance in Football: A Systematic Review with Meta-Analysis" BioMed 2, no. 3: 328-340. https://doi.org/10.3390/biomed2030026
APA StyleVlachas, T., & Paraskevopoulos, E. (2022). The Effect of the FIFA 11+ on Injury Prevention and Performance in Football: A Systematic Review with Meta-Analysis. BioMed, 2(3), 328-340. https://doi.org/10.3390/biomed2030026