
SARS-CoV-2 and HCoV IgG Antibodies in the Breast Milk of a Postpartum SARS-CoV-2 Patient Following Bamlanivimab Administration: A Case Report

 , , ,
, , ,
Abstract
1. Introduction
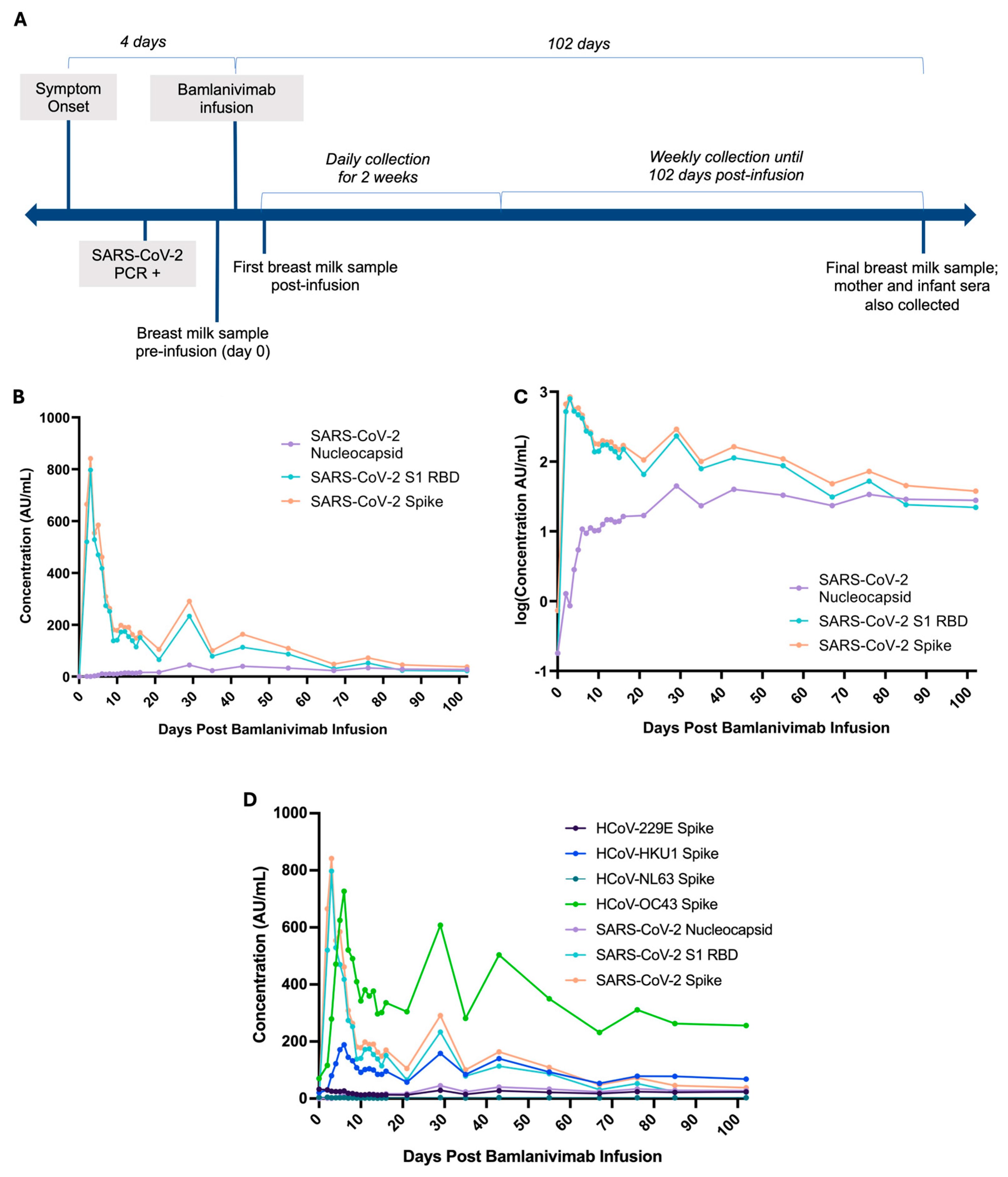
2. Detailed Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| HCoV | Human coronaviruses |
| IgG | Immunoglobulin G |
| PCR | Polymerase chain reaction |
| mAb | Monoclonal antibody |
References
- Vassilopoulou, E.; Feketea, G.; Koumbi, L.; Mesiari, C.; Berghea, E.C.; Konstantinou, G.N. Breastfeeding and COVID-19: From Nutrition to Immunity. Front. Immunol 2021, 12, 661806. [Google Scholar] [CrossRef]
- Scrimin, F.; Campisciano, G.; Comar, M.; Ragazzon, C.; Davanzo, R.; Quadrifoglio, M.; Giangreco, M.; Stabile, G.; Ricci, G. IgG and IgA Antibodies Post SARS-CoV-2 Vaccine in the Breast Milk and Sera of Breastfeeding Women. Vaccines 2022, 10, 125. [Google Scholar] [CrossRef]
- Olearo, F.; Radmanesh, L.S.; Felber, N.; von Possel, R.; Emmerich, P.; Pekarek, N.; Pfefferle, S.; Nörz, D.; Hansen, G.; Diemert, A.; et al. Anti-SARS-CoV-2 antibodies in breast milk during lactation after infection or vaccination: A cohort study. J. Reprod. Immunol. 2022, 153, 103685. [Google Scholar] [CrossRef] [PubMed]
- Narayanaswamy, V.; Pentecost, B.T.; Schoen, C.N.; Alfandari, D.; Schneider, S.S.; Baker, R.; Arcaro, K.F. Neutralizing Antibodies and Cytokines in Breast Milk After Coronavirus Disease 2019 (COVID-19) mRNA Vaccination. Obstet. Gynecol. 2022, 139, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Perl, S.H.; Uzan-Yulzari, A.; Klainer, H.; Asiskovich, L.; Youngster, M.; Rinott, E.; Youngster, I. SARS-CoV-2–Specific Antibodies in Breast Milk After COVID-19 Vaccination of Breastfeeding Women. JAMA 2021, 325, 2013–2014. [Google Scholar] [CrossRef]
- Perez, S.E.; Luna Centeno, L.D.; Cheng, W.A.; Marentes Ruiz, C.J.; Lee, Y.; Congrave-Wilson, Z.; Powell, R.L.; Stellwagen, L.; Pannaraj, P.S. Human Milk SARS-CoV-2 Antibodies up to 6 Months After Vaccination. Pediatrics 2022, 149, e2021054260. [Google Scholar] [CrossRef]
- Graciliano, N.G.; Goulart, M.O.F.; de Oliveira, A.C.M. Impact of Maternal Exposure to SARS-CoV-2 on Immunological Components of Breast Milk. Int. J. Mol. Sci. 2025, 26, 2600. [Google Scholar] [CrossRef]
- Armistead, B.; Jiang, Y.; Carlson, M.; Ford, E.S.; Jani, S.; Houck, J.; Wu, X.; Jing, L.; Pecor, T.; Kachikis, A.; et al. Spike-specific T cells are enriched in breastmilk following SARS-CoV-2 mRNA vaccination. Mucosal Immunol. 2023, 16, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Marshall, N.E.; Blanton, M.B.; Doratt, B.M.; Malherbe, D.C.; Rincon, M.; Messaoudi, I. Monoclonal Antibody Therapy of Breastfeeding Patient Infected with SARS-CoV-2: A Case Report. Breastfeed. Med. 2023, 18, 626–630. [Google Scholar] [CrossRef]
- Eli Lilly Canada, Inc. Bamlanivimab Product Monograph; Eli Lilly Canada, Inc.: Toronto, ON, Canada, 2021; pp. 1–19. [Google Scholar]
- Regulatory Decision Summary—Bamlanivimab—Health Canada [Internet]. Available online: https://covid-vaccine.canada.ca/info/regulatory-decision-summary-detailTwo.html?linkID=RDS00719& (accessed on 30 May 2025).
- Huang, A.T.; Garcia-Carreras, B.; Hitchings, M.D.T.; Yang, B.; Katzelnick, L.C.; Rattigan, S.M.; Borgert, B.A.; Moreno, C.A.; Solomon, B.D.; Trimmer-Smith, L.; et al. A systematic review of antibody mediated immunity to coronaviruses: Kinetics, correlates of protection, and association with severity. Nat. Commun. 2020, 11, 4704. [Google Scholar] [CrossRef]
- Tanunliong, G.; Liu, A.C.; Kaweski, S.; Irvine, M.; Reyes, R.C.; Purych, D.; Krajden, M.; Morshed, M.; Sekirov, I.; Gantt, S.; et al. Age-Associated Seroprevalence of Coronavirus Antibodies: Population-Based Serosurveys in 2013 and 2020, British Columbia, Canada. Front. Immunol. 2022, 13, 836449. [Google Scholar] [CrossRef]
- Aydillo, T.; Rombauts, A.; Stadlbauer, D.; Aslam, S.; Abelenda-Alonso, G.; Escalera, A.; Amanat, F.; Jiang, K.; Krammer, F.; Carratala, J.; et al. Immunological imprinting of the antibody response in COVID-19 patients. Nat. Commun. 2021, 12, 3781. [Google Scholar] [CrossRef]
- Tso, F.Y.; Lidenge, S.J.; Peña, P.B.; Clegg, A.A.; Ngowi, J.R.; Mwaiselage, J.; Ngalamika, O.; Julius, P.; West, J.T.; Wood, C. High prevalence of pre-existing serological cross-reactivity against severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) in sub-Saharan Africa. Int. J. Infect. Dis. 2021, 102, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Shrwani, K.; Sharma, R.; Krishnan, M.; Jones, T.; Mayora-Neto, M.; Cantoni, D.; Temperton, N.J.; Dobson, S.L.; Subramaniam, K.; McNamara, P.S.; et al. Detection of Serum Cross-Reactive Antibodies and Memory Response to SARS-CoV-2 in Prepandemic and Post–COVID-19 Convalescent Samples. J. Infect. Dis. 2021, 224, 1305–1315. [Google Scholar] [CrossRef]
- Aguilar-Bretones, M.; Westerhuis, B.M.; Raadsen, M.P.; de Bruin, E.; Chandler, F.D.; Okba, N.M.; Haagmans, B.L.; Langerak, T.; Endeman, H.; Akker, J.P.v.D.; et al. Seasonal coronavirus–specific B cells with limited SARS-CoV-2 cross-reactivity dominate the IgG response in severe COVID-19. J. Clin. Investig. 2021, 131, e150613. [Google Scholar] [CrossRef]
- Röltgen, K.; Nielsen, S.C.; Silva, O.; Younes, S.F.; Zaslavsky, M.; Costales, C.; Yang, F.; Wirz, O.F.; Solis, D.; Hoh, R.A.; et al. Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination. Cell 2022, 185, 1025–1040.e14. [Google Scholar] [CrossRef]
- Demers-Mathieu, V.; DaPra, C.; Mathijssen, G.; Sela, D.A.; Järvinen, K.M.; Seppo, A.; Fels, S.; Medo, E. Human Milk Antibodies against S1 and S2 Subunits from SARS-CoV-2, HCoV-OC43, and HCoV-229E in Mothers with a Confirmed COVID-19 PCR, Viral SYMPTOMS, and Unexposed Mothers. Int. J. Mol. Sci. 2021, 22, 1749. [Google Scholar] [CrossRef]
- Demers-Mathieu, V.; DaPra, C.; Mathijssen, G.B.; Medo, E. Previous viral symptoms and individual mothers influenced the leveled duration of human milk antibodies cross-reactive to S1 and S2 subunits from SARS-CoV-2, HCoV-229E, and HCoV-OC43. J. Perinatol. 2021, 41, 952–960. [Google Scholar] [CrossRef] [PubMed]
- Li, F.F.; Liu, A.; Gibbs, E.; Tanunliong, G.; Marquez, A.C.; Gantt, S.; Frykman, H.; Krajden, M.; Morshed, M.; Prystajecky, N.A.; et al. A novel multiplex electrochemiluminescent immunoassay for detection and quantification of anti-SARS-CoV-2 IgG and anti-seasonal endemic human coronavirus IgG. J. Clin. Virol. 2022, 146, 105050. [Google Scholar] [CrossRef]
- Korchinski, I.; Marquez, C.; McClymont, E.; Av-Gay, G.; Andrade, J.; Elwood, C.; Jassem, A.; Krajden, M.; Morshed, M.; Sadarangani, M.; et al. Maternal-infant transfer of SARS-CoV-2 antibodies following vaccination in pregnancy: A prospective cohort study. Vaccine 2024, 42, 126123. [Google Scholar] [CrossRef]
- Tretyn, A.; Szczepanek, J.; Skorupa, M.; Jarkiewicz-Tretyn, J.; Sandomierz, D.; Dejewska, J.; Ciechanowska, K.; Jarkiewicz-Tretyn, A.; Koper, W.; Pałgan, K. Differences in the Concentration of Anti-SARS-CoV-2 IgG Antibodies Post-COVID-19 Recovery or Post-Vaccination. Cells 2021, 10, 1952. [Google Scholar] [CrossRef]
- Chigutsa, E.; O’Brien, L.; Ferguson-Sells, L.; Long, A.; Chien, J. Population Pharmacokinetics and Pharmacodynamics of the Neutralizing Antibodies Bamlanivimab and Etesevimab in Patients With Mild to Moderate COVID-19 Infection. Clin. Pharmacol. Ther. 2021, 110, 1302–1310. [Google Scholar] [CrossRef]
- Post, N.; Eddy, D.; Huntley, C.; van Schalkwyk, M.C.I.; Shrotri, M.; Leeman, D.; Rigby, S.; Williams, S.V.; Bermingham, W.H.; Kellam, P.; et al. Antibody response to SARS-CoV-2 infection in humans: A systematic review. PLoS ONE 2020, 15, e0244126. [Google Scholar] [CrossRef]
- Kim, P.S.; Dimcheff, D.E.; Siler, A.; Schildhouse, R.J.; Chensue, S.W. Effect of monoclonal antibody therapy on the endogenous SARS-CoV-2 antibody response. Clin. Immunol. 2022, 236, 108959. [Google Scholar] [CrossRef]
- Petro, C.D.; Hooper, A.T.; Peace, A.; Mohammadi, K.; Eagan, W.; Elbashir, S.M.; DiPiazza, A.; Makrinos, D.; Pascal, K.; Bandawane, P.; et al. Monoclonal antibodies against the spike protein alter the endogenous humoral response to SARS-CoV-2 vaccination and infection. Sci. Transl. Med. 2024, 16, eadn0396. [Google Scholar] [CrossRef]
- LaHue, S.C.; Anderson, A.; Krysko, K.M.; Rutatangwa, A.; Dorsey, M.J.; Hale, T.; Mahadevan, U.; Rogers, E.E.; Rosenstein, M.G.; Bove, R. Transfer of monoclonal antibodies into breastmilk in neurologic and non-neurologic diseases. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7, e769. [Google Scholar] [CrossRef]
- Sagar, M.; Reifler, K.; Rossi, M.; Miller, N.S.; Sinha, P.; White, L.F.; Mizgerd, J.P. Recent endemic coronavirus infection is associated with less-severe COVID-19. J. Clin. Investig. 2021, 131, e143380. [Google Scholar] [CrossRef]
- Fillmore, N.R.; Szalat, R.E.; La, J.; Branch-Elliman, W.; Monach, P.A.; Nguyen, V.; Samur, M.K.; Brophy, M.T.; Do, N.V.; Munshi, N.C. Recent common human coronavirus infection protects against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection: A Veterans Affairs cohort study. Proc. Natl. Acad. Sci. USA 2022, 119, e2213783119. [Google Scholar] [CrossRef]
- Nguyen-Contant, P.; Embong, A.K.; Kanagaiah, P.; Chaves, F.A.; Yang, H.; Branche, A.R.; Topham, D.J.; Sangster, M.Y.; Ellebedy, A.; Schultz-Cherry, S. S Protein-Reactive IgG and Memory B Cell Production after Human SARS-CoV-2 Infection Includes Broad Reactivity to the S2 Subunit. mBio 2020, 11, e01991-20. [Google Scholar] [CrossRef]
- van den Elsen, L.W.J.; Kollmann, T.R.; Verhasselt, V. Microbial antigen in human milk: A natural vaccine? Mucosal Immunol. 2022, 15, 1058–1059. [Google Scholar] [CrossRef] [PubMed]
- Goenka, A.; Kollmann, T.R. Development of immunity in early life. J. Infect. 2015, 71, S112–S120. [Google Scholar] [CrossRef]

{kind=link}
| Days Post Infusion | Sample Type | Description | HCoV-229E Spike (AU/mL) | HCoV-HKU1 Spike (AU/mL) | HCoV-NL63 Spike (AU/mL) | HCoV-OC43 Spike (AU/mL) | SARS-CoV-2 Nucleocapsid (AU/mL) | SARS-CoV-2 S1 RBD (AU/mL) | SARS-CoV-2 Spike (AU/mL) |
|---|---|---|---|---|---|---|---|---|---|
| 0 | milk | Pre-infusion baseline, 4 days post-symptom onset | 32.69 | 20.73 | 4.57 | 70.23 | 0.18 | 0.18 | 0.74 |
| 102 | milk | mother milk | 23.62 | 68.38 | 3.08 | 255.79 | 27.92 | 22.13 | 37.86 |
| serum | mother serum | 17,712.70 | 46,143.88 | 2009.79 | 165,563.13 | 18,506.28 | 34,046.59 | 31,833.55 | |
| serum | infant serum | 2336.92 | 1311.99 | 245.42 | 4257.35 | 6836.31 | 14,140.66 | 16,418.68 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanunliong, G.; Condin, C.; Márquez, A.C.; Li, S.; Binning, N.; Gibson, M.; Griffiths, B.; Wright, A.; Money, D.; Krajden, M.; et al. SARS-CoV-2 and HCoV IgG Antibodies in the Breast Milk of a Postpartum SARS-CoV-2 Patient Following Bamlanivimab Administration: A Case Report. COVID 2025, 5, 123. https://doi.org/10.3390/covid5080123
Tanunliong G, Condin C, Márquez AC, Li S, Binning N, Gibson M, Griffiths B, Wright A, Money D, Krajden M, et al. SARS-CoV-2 and HCoV IgG Antibodies in the Breast Milk of a Postpartum SARS-CoV-2 Patient Following Bamlanivimab Administration: A Case Report. COVID. 2025; 5(8):123. https://doi.org/10.3390/covid5080123
Chicago/Turabian StyleTanunliong, Guadalein, Christopher Condin, Ana Citlali Márquez, Susan Li, Nimrat Binning, Miriam Gibson, Brayden Griffiths, Alissa Wright, Deborah Money, Mel Krajden, and et al. 2025. "SARS-CoV-2 and HCoV IgG Antibodies in the Breast Milk of a Postpartum SARS-CoV-2 Patient Following Bamlanivimab Administration: A Case Report" COVID 5, no. 8: 123. https://doi.org/10.3390/covid5080123
APA StyleTanunliong, G., Condin, C., Márquez, A. C., Li, S., Binning, N., Gibson, M., Griffiths, B., Wright, A., Money, D., Krajden, M., Morshed, M., Jassem, A. N., Haljan, G., & Sekirov, I. (2025). SARS-CoV-2 and HCoV IgG Antibodies in the Breast Milk of a Postpartum SARS-CoV-2 Patient Following Bamlanivimab Administration: A Case Report. COVID, 5(8), 123. https://doi.org/10.3390/covid5080123