
Mild SARS-CoV-2 Infection with the Omicron Variant Mimicking Metastatic Cancer on Whole-Body 18-F FDG PET/CT Imaging

 ,
,  , ,
, , {kind=link}
{kind=link}
Abstract
1. Introduction
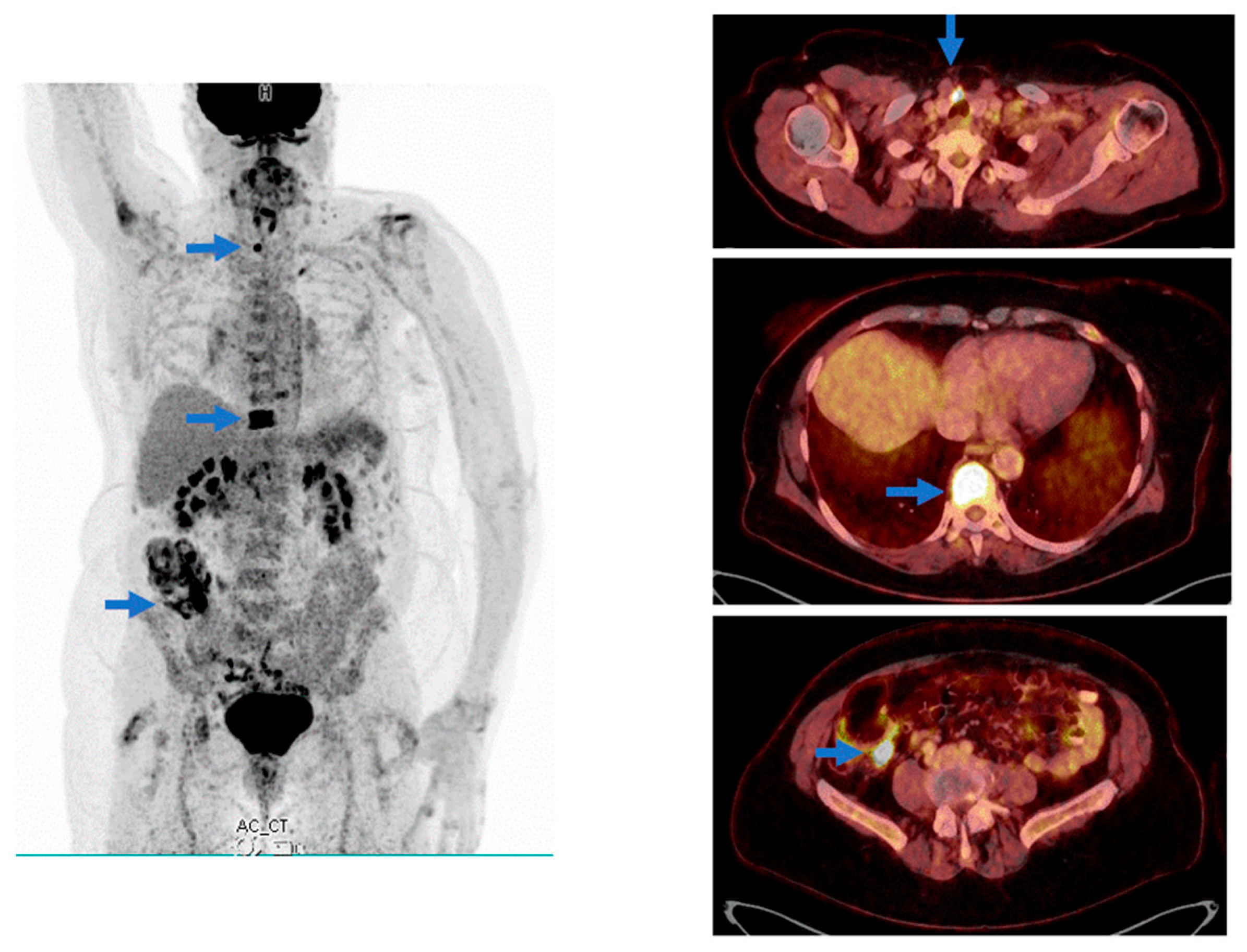
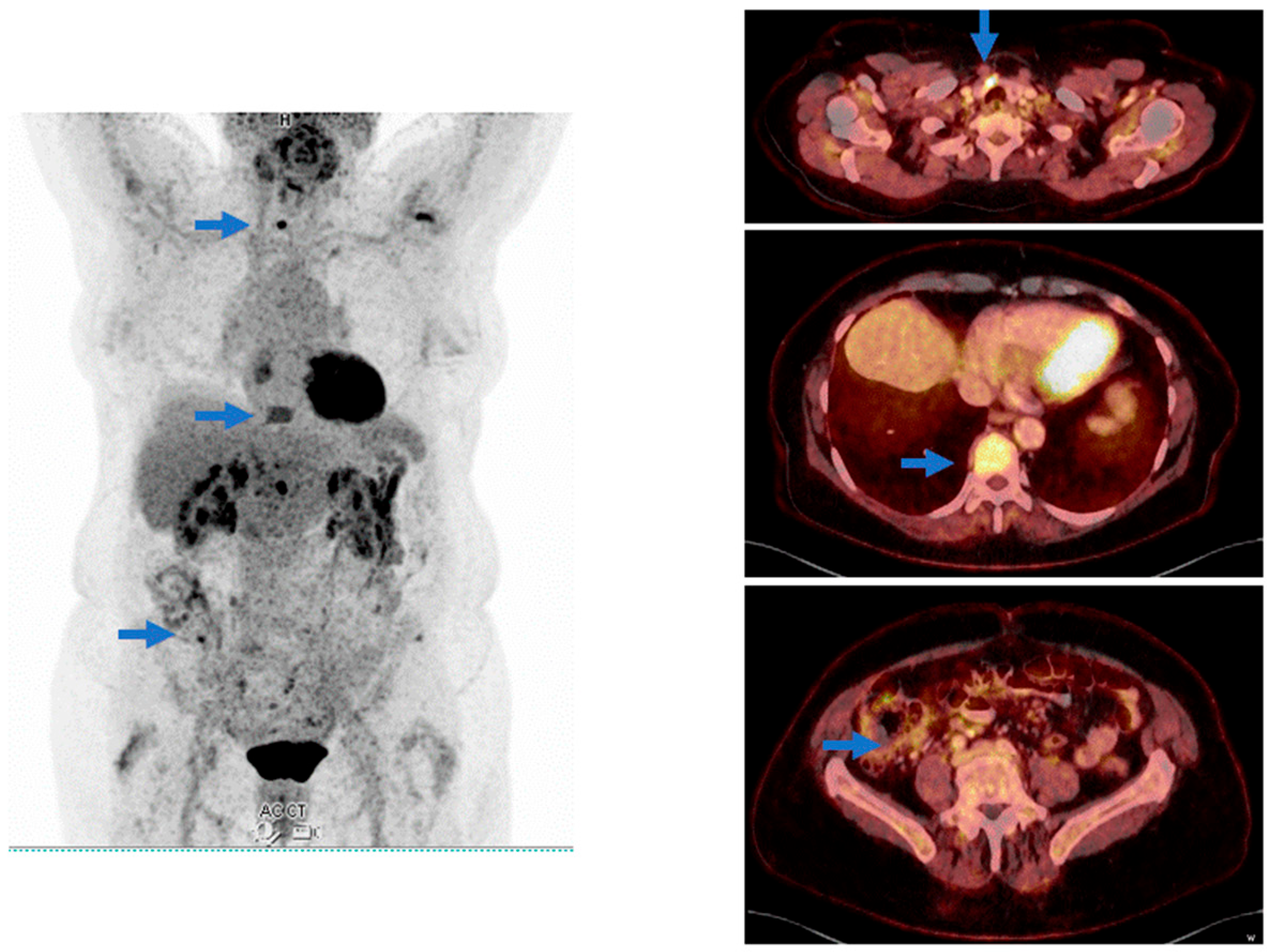
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data; World Health Organization: Geneva, Switzerland, 2025. [Google Scholar]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. China Medical Treatment Expert Group for Covid-19. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.J.; Dong, X.; Liu, G.H.; Gao, Y.D. Risk and Protective Factors for COVID-19 Morbidity, Severity, and Mortality. Clin. Rev. Allergy Immunol. 2023, 64, 90–107. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Zou, S.; Zhu, X. FDG PET/CT of COVID-19. Radiology 2020, 296, E118. [Google Scholar] [CrossRef] [PubMed]
- Vaz, N.; Franquet, E.; Heidari, P.; Chow, D.Z.; Jacene, H.A.; Ng, T.S.C. COVID-19: Findings in nuclear medicine from head to toe. Clin. Imaging 2023, 99, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.; Krauthammer, S.H.; Wolf, I.; Even-Sapir, E. Hypermetabolic lymphadenopathy following administration of BNT162b2 mRNA Covid-19 vaccine: Incidence assessed by [18F]FDG PET-CT and relevance to study interpretation. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1854–1863. [Google Scholar] [CrossRef] [PubMed]
- Pai, T.S.; Rojas, C.; Wasserman, M.C.; Parent, E.E.; Cornell, L.; Chumsri, S. Asymptomatic coronavirus disease 2019 mimicking metastatic breast cancer on positron emission tomography/computed tomography imaging. Radiol. Case Rep. 2021, 16, 2226–2230. [Google Scholar] [CrossRef] [PubMed]
- Kavanal, A.J.; Jena, S.R.; Kumar, R.; Das, C.K.; Kumar, S.; Mittal, B.R. Effect of COVID-19 on 18F-FDG PET/CT: Is There a Need to Consider COVID-19 Status Before Planning 18F-FDG PET/CT for Oncologic Evaluation? J. Nucl. Med. Technol. 2021, 49, 284–285. [Google Scholar] [CrossRef] [PubMed]
- SNMMI Statement: Possible Effect of Omicron Infection on FDG PET/CT Scans 2022. J. Nucl. Med. 2022, 63, 11N. [PubMed]
- Sugitani, I. Active surveillance of low-risk papillary thyroid microcarcinoma. Best. Pract. Res. Clin. Endocrinol. Metab. 2023, 37, 101630. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Helmsdal, G.; Clemmensen, S.; Mortensen, J.; Kristiansen, M.F.; Petersen, M.S.; Johannesen, H.L. Mild SARS-CoV-2 Infection with the Omicron Variant Mimicking Metastatic Cancer on Whole-Body 18-F FDG PET/CT Imaging. COVID 2025, 5, 98. https://doi.org/10.3390/covid5070098
Helmsdal G, Clemmensen S, Mortensen J, Kristiansen MF, Petersen MS, Johannesen HL. Mild SARS-CoV-2 Infection with the Omicron Variant Mimicking Metastatic Cancer on Whole-Body 18-F FDG PET/CT Imaging. COVID. 2025; 5(7):98. https://doi.org/10.3390/covid5070098
Chicago/Turabian StyleHelmsdal, Gunnhild, Sissal Clemmensen, Jann Mortensen, Marnar Fríðheim Kristiansen, Maria Skaalum Petersen, and Herborg L. Johannesen. 2025. "Mild SARS-CoV-2 Infection with the Omicron Variant Mimicking Metastatic Cancer on Whole-Body 18-F FDG PET/CT Imaging" COVID 5, no. 7: 98. https://doi.org/10.3390/covid5070098
APA StyleHelmsdal, G., Clemmensen, S., Mortensen, J., Kristiansen, M. F., Petersen, M. S., & Johannesen, H. L. (2025). Mild SARS-CoV-2 Infection with the Omicron Variant Mimicking Metastatic Cancer on Whole-Body 18-F FDG PET/CT Imaging. COVID, 5(7), 98. https://doi.org/10.3390/covid5070098