
Self-Reported Body Weight Change and Weight Loss Practices During the COVID-19 Pandemic: A Mixed-Methods Study from Türkiye


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sampling
2.2. Measures
2.2.1. Demographic Information
2.2.2. Self-Reported Body Weight Change
2.2.3. Qualitative Setting
2.2.4. Weight Loss Practices
2.3. Statistical Analysis
3. Results
3.1. Participants
3.2. Self-Reported Body Weight Change During the COVID-19 Pandemic
3.3. Pandemic-Related Changes in Participants Causing Body Weight Change
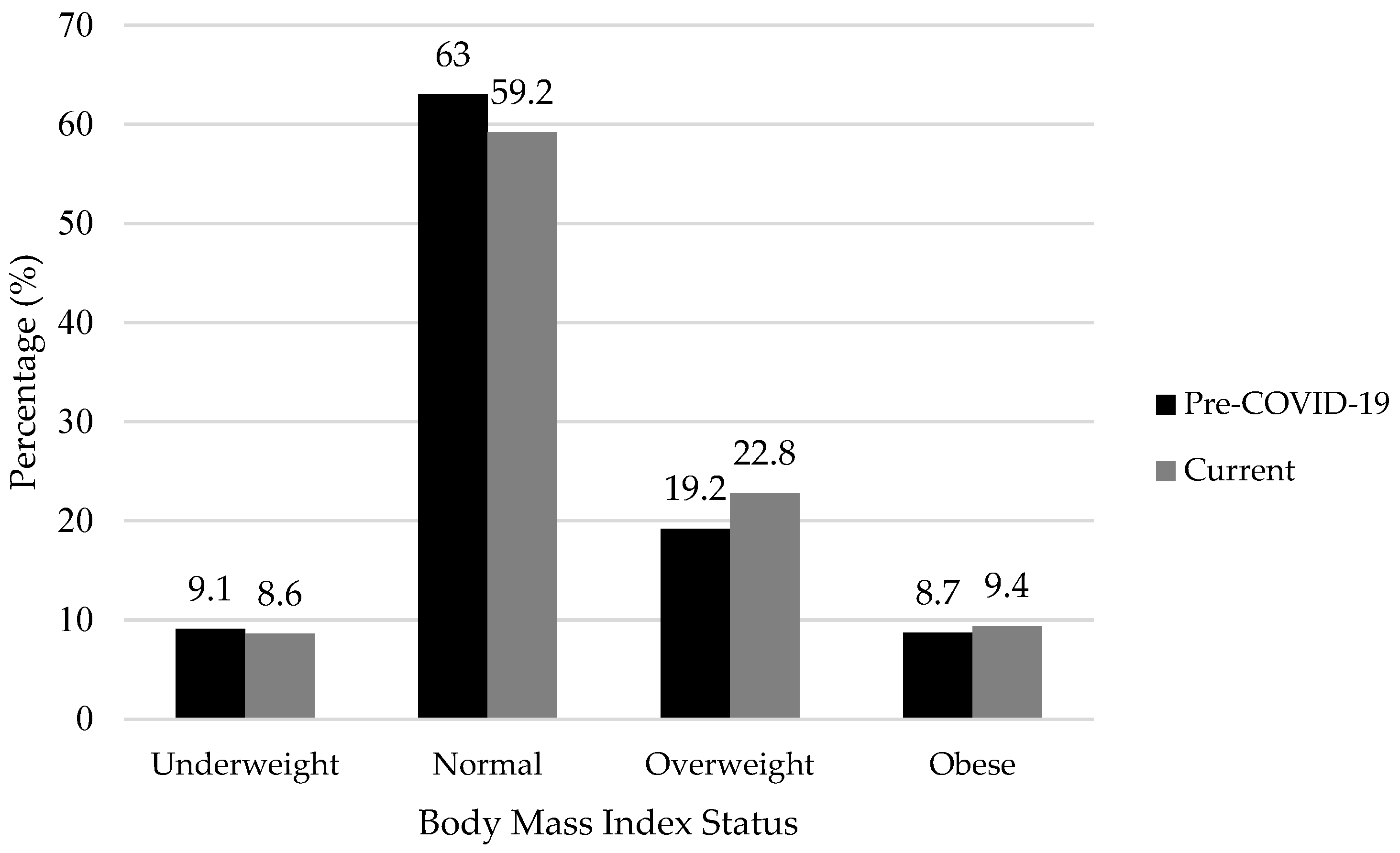
3.4. Self-Reported Nutritional Status Change During the Pandemic
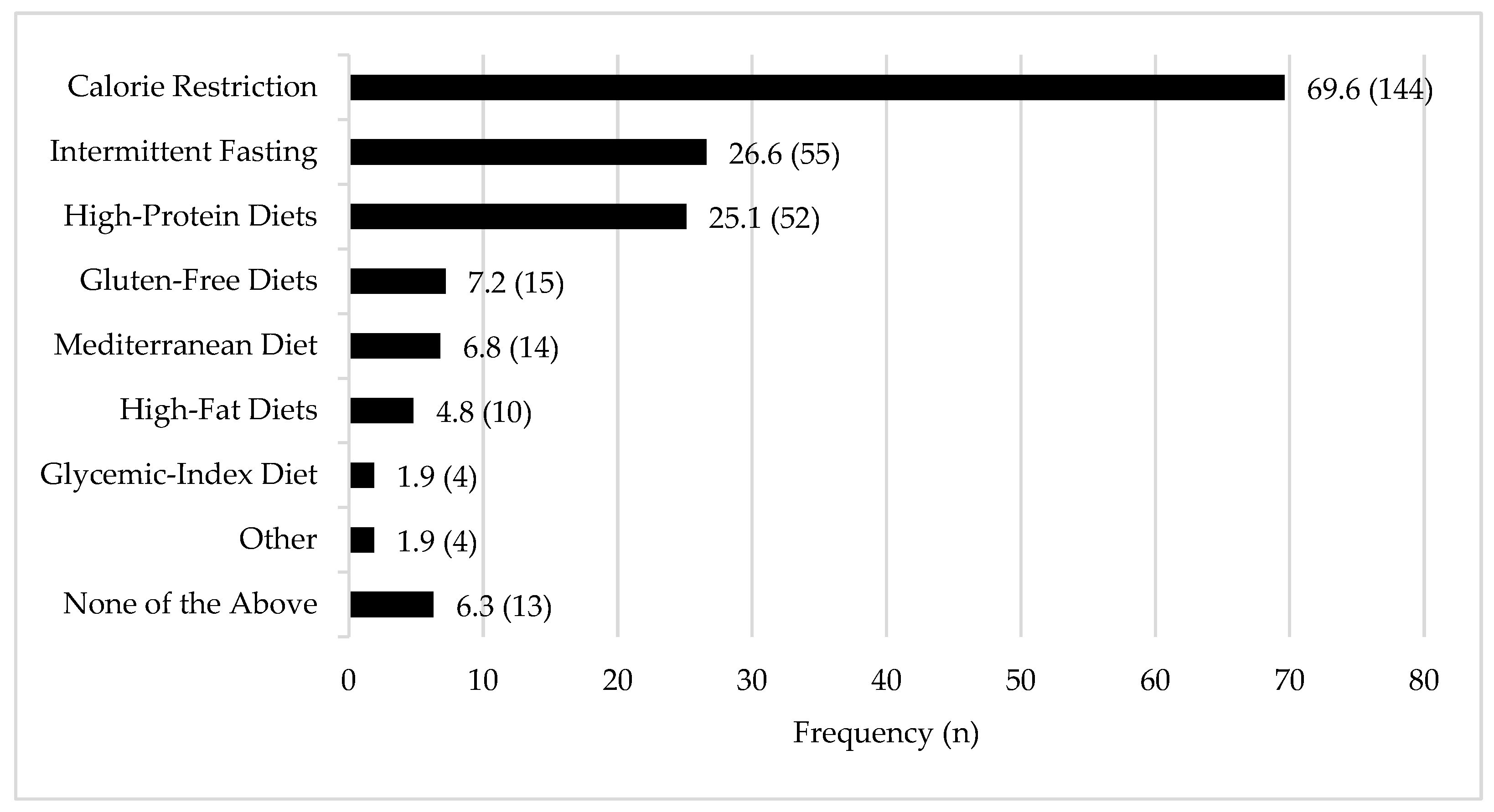
3.5. Weight Loss Practices During the COVID-19 Pandemic
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| CI | Directory of Open Access Journals |
| COVID-19 | Coronavirus disease 2019 |
| SD | Standard deviation |
| SPSS | Statistical Package for the Social Sciences |
| WHO | World Health Organization |
References
- WHO. Listings of WHO’s Response to COVID-19. 2020. Available online: https://www.who.int/news/item/29-06-2020-covidtimeline (accessed on 8 May 2025).
- The Ministry of Interior of the Republic of Türkiye. Additional Circular on COVID-19 Measures Sent to 81 Provincial Governorships. 2020. Available online: https://www.icisleri.gov.tr/81-il-valiligine-koronavirus-tedbirleri-konulu-ek-genelge-gonderildi (accessed on 8 May 2025).
- Turkish Statistical Institute. Death and Causes of Death Statistics 2021. 2023. Available online: https://data.tuik.gov.tr/Bulten/Index?p=death-and-causes-of-death-statistics-2021-45715&dil=2 (accessed on 8 May 2025).
- Galea, S.; Keyes, K. Understanding the COVID-19 Pandemic through the lens of population health science. Am. J. Epidemiol. 2020, 189, 1232–1237. [Google Scholar] [CrossRef] [PubMed]
- McBride, E.; Arden, M.A.; Chater, A.; Chilcot, J. The impact of COVID-19 on health behaviour, well-being, and long-term physical health. Br. J. Health Psychol. 2021, 26, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Massoud, L.; Zoghi, M. The effects of the covid-19 pandemic on food systems: Limitations and opportunities. Discover Food 2024, 4, 102. [Google Scholar] [CrossRef]
- Jafri, A.; Mathe, N.; Aglago, E.K.; Konyole, S.O.; Ouedraogo, M.; Audain, K.; Zongo, U.; Laar, A.K.; Johnson, J.; Sanou, D. Food availability, accessibility and dietary practices during the covid-19 pandemic: A multi-country survey. Public Health Nutr. 2021, 24, 1798–1805. [Google Scholar] [CrossRef]
- Dolati, S.; Hariri Far, A.; Mollarasouli, Z.; Imani, A. The impact of the COVID-19 pandemic on changes in food choice, purchase, and consumption patterns in the world: A review study. J. Nutr. Food Secur. 2022, 7, 388–397. [Google Scholar] [CrossRef]
- Cecchetto, C.; Aiello, M.; Gentili, C.; Ionta, S.; Osimo, S.A. increased emotional eating during COVID-19 associated with lockdown, psychological and contextual factors. Appetite 2021, 160, 105122. [Google Scholar] [CrossRef]
- Marchitelli, S.; Mazza, C.; Lenzi, A.; Ricci, E.; Gnessi, L.; Roma, P. Weight gain in a sample of patients affected by overweight/obesity with and without a psychiatric diagnosis during the COVID-19 lockdown. Nutrients 2020, 12, 3525. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.N.; Yoshida-Montezuma, Y.; Dewart, N.; Jalil, E.; Khattar, J.; De Rubeis, V.; Carsley, S.; Griffith, L.E.; Mbuagbaw, L. Obesity and weight change during the COVID-19 pandemic in children and adults: A systematic review and meta-analysis. Obes. Rev. 2023, 24, e13550. [Google Scholar] [CrossRef]
- Khan, M.A.; Menon, P.; Govender, R.; Abu Samra, A.M.; Allaham, K.K.; Nauman, J.; Östlundh, L.; Mustafa, H.; Smith, J.E.M.; AlKaabi, J.M. Systematic review of the effects of pandemic confinements on body weight and their determinants. Br. J. Nutr. 2022, 127, 298–317. [Google Scholar] [CrossRef]
- Daniel, M.M.; Liboredo, J.C.; Souza, T.C.d.M.; Anastácio, L.R.; Ferreira, A.R.S.; Ferreira, L.G. The Impact of the COVID-19 Pandemic: A Longitudinal Analysis of Body Weight Variations and Their Implications for Daily Habits. Int. J. Environ. Res. Public Health 2024, 21, 1510. [Google Scholar] [CrossRef]
- Park, A.H.; Zhong, S.; Yang, H.; Jeong, J.; Lee, C. Impact of COVID-19 on physical activity: A rapid review. J. Glob. Health 2022, 12, 05003. [Google Scholar] [CrossRef] [PubMed]
- Kriaučionienė, V.; Grincaitė, M.; Raskilienė, A.; Petkevičienė, J. Changes in Nutrition, Physical Activity, and Body Weight among Lithuanian Students during and after the COVID-19 Pandemic. Nutrients 2023, 15, 4091. [Google Scholar] [CrossRef] [PubMed]
- The Republic of Türkiye Ministry of Health. Turkey Nutrition and Health Survey (TBSA). 2019. Available online: https://hsgm.saglik.gov.tr/depo/birimler/saglikli-beslenme-ve-hareketli-hayat-db/Dokumanlar/Kitaplar/Turkiye_Beslenme_ve_Saglik_Arastirmasi_TBSA_2017.pdf (accessed on 8 May 2025).
- Turkish Statistical Institute. Turkey Health Survey 2022. 2023. Available online: https://data.tuik.gov.tr/Bulten/Index?p=Turkiye-Health-Survey-2022-49747&dil=2 (accessed on 8 June 2025).
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- WHO. A Healthy Lifestyle—WHO Recommendations. 2010. Available online: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (accessed on 8 May 2025).
- Anton, S.D.; Hida, A.; Heekin, K.; Sowalsky, K.; Karabetian, C.; Mutchie, H.; Barnett, T.E. Effects of popular diets without specific calorie targets on weight loss outcomes: Systematic review of findings from clinical trials. Nutrients 2017, 9, 822. [Google Scholar] [CrossRef] [PubMed]
- Freire, R. Scientific evidence of diets for weight loss: Different macronutrient composition, intermittent fasting, and popular diets. Nutrition 2020, 69, 110549. [Google Scholar] [CrossRef]
- Hayran, M.; Hayran, M. Sağlık Araştırmaları İçin Temel İstatistik, 2nd ed.; Omega Araştırma: Ankara, Türkiye, 2018. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Barazzoni, R.; Bischoff, S.C.; Breda, J.; Wickramasinghe, K.; Chourdakis, M. Impact of the first COVID-19 lockdown on body weight: A combined systematic review and a meta-analysis. Clin. Nutr. 2022, 41, 3046–3054. [Google Scholar] [CrossRef]
- Kalligeros, M.; Shehadeh, F.; Mylona, E.K.; Benitez, G.; Beckwith, C.G.; Chan, P.A.; Mylonakis, E. Association of obesity with disease severity among patients with Coronavirus Disease 2019. Obesity 2020, 28, 1200–1204. [Google Scholar] [CrossRef]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M.; et al. High prevalence of obesity in severe acute respiratory syndrome coronavirus-2 (SARS-COV-2) requiring invasive mechanical ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef]
- Griffin, T.; Grey, E.; Lambert, J.; Gillison, F.; Townsend, N.; Solomon-Moore, E. Life in lockdown: A qualitative study exploring the experience of living through the initial COVID-19 lockdown in the UK and its impact on diet, physical activity and mental health. BMC Public Health 2023, 23, 588. [Google Scholar] [CrossRef]
- Daly, M.; Robinson, E. Psychological distress and adaptation to the COVID-19 crisis. J. Psychiatr. Res. 2021, 136, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Nour, T.Y.; Altintaş, K.H. Effect of the COVID-19 pandemic on obesity and it is risk factors: A systematic review. BMC Public Health 2023, 23, 1018. [Google Scholar] [CrossRef] [PubMed]
- Paltrinieri, S.; Bressi, B.; Costi, S.; Mazzini, E.; Cavuto, S.; Ottone, M.; De Panfilis, L.; Fugazzaro, S.; Rondini, E.; Giorgi Rossi, P. Beyond Lockdown: The Potential Side Effects of the SARS-CoV-2 Pandemic on Public Health. Nutrients 2021, 13, 1600. [Google Scholar] [CrossRef] [PubMed]
- Çengel, B.; Karadavut, U. Covid 19 Pandemisinin Beslenme Alışkanlıklarına Etkisi. Sci. Tech. 21st Century 2020, 2, 39–46. [Google Scholar]
- Zachary, Z.; Brianna, F.; Brianna, L.; Garrett, P.; Jade, W.; Alyssa, D.; Mikayla, K. Self-quarantine and weight gain related risk factors during the COVID-19 pandemic. Obes. Res. Clin. Pract. 2020, 14, 210–216. [Google Scholar] [CrossRef]
- Bisset, S.; Gauvin, L.; Potvin, L.; Paradis, G. Association of body mass index and dietary restraint with changes in eating behaviour throughout late childhood and early adolescence: A 5-year study. Public Health Nutr. 2007, 10, 780–789. [Google Scholar] [CrossRef]
- van Strien, T.; Herman, C.P.; Verheijden, M.W. Dietary restraint and body mass change: A 3-year follow-up study in a representative Dutch sample. Appetite 2014, 76, 44–49. [Google Scholar] [CrossRef]
- Bhutani, S.; Cooper, J.A.; Vandellen, M.R. Self-Reported changes in energy balance behaviors during COVID-19-related home confinement: A cross-sectional study of US adults. Obesity 2021, 29, 1909–1919. [Google Scholar] [CrossRef]
- Li, Y.; Scherer, N.; Felix, L.; Kuper, H. Prevalence of depression, anxiety and post-traumatic stress disorder in health care workers during the COVID-19 pandemic: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0246454. [Google Scholar] [CrossRef]
- van Kessel, R.; Kyriopoulos, I.; Wong, B.L.H.; Mossialos, E. The effect of the COVID-19 pandemic on digital health–seeking behavior: Big data interrupted time-series analysis of Google Trends. J. Med. Internet Res. 2023, 25, e42401. [Google Scholar] [CrossRef]
- Fappa, E.; Micheli, M. Content accuracy and readability of dietary advice available on webpages: A systematic review of the evidence. J. Hum. Nutr. Diet. 2025, 38, e13395. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Sex | ||
| Male | 186 | 23.1 |
| Female | 620 | 76.9 |
| Age groups (years) | ||
| 18–24 | 380 | 47.1 |
| 25–44 | 325 | 40.3 |
| 45–6465 | 101 | 12.5 |
| Marial status | ||
| Married | 287 | 35.6 |
| Single | 497 | 61.7 |
| Divorced or widow | 22 | 2.7 |
| Education level | ||
| University | 659 | 81.8 |
| High school | 102 | 12.7 |
| Lower | 45 | 5.6 |
| Income status | ||
| Less income than expenses | 237 | 29.4 |
| Income equals expenses | 408 | 50.6 |
| More income than expenses | 161 | 20.0 |
| Occupation | ||
| Government worker | 161 | 20.0 |
| Employee | 119 | 14.8 |
| Own business | 18 | 2.2 |
| Student | 318 | 39.5 |
| Housewife | 92 | 11.4 |
| Retired | 21 | 2.6 |
| Unemployed | 51 | 6.3 |
| Other | 26 | 3.2 |
| Tobacco Use | ||
| Current smoker | 172 | 21.3 |
| Former smoker | 104 | 12.9 |
| Never smoker | 530 | 65.8 |
| Total | 806 | 100.0 |
| Weight Change Categories | n | % | Pre-COVID-19 Body Weight | Current Body Weight | Difference Value |
|---|---|---|---|---|---|
| Weight increase | 362 | 44.9 | 65.13 ± 13.4 | 69.71 ± 14.2 | 4.59 ± 3.0 |
| No weight change | 148 | 18.4 | 62.97 ± 14.3 | 62.97 ± 14.3 | - |
| Weight decrease | 182 | 22.6 | 66.82 ± 16.2 | 62.06 ± 13.9 | −4.77 ± 3.9 |
| Weight fluctuation | 114 | 14.1 | |||
| Resulted in a gain | 43 | 5.3 | 59.89 ± 11.9 | 63.16 ± 12.6 | 3.28 ± 2.3 |
| Resulted in the same | 17 | 2.1 | 60.82 ± 11.5 | 60.82 ± 11.5 | - |
| Resulted in a loss | 54 | 6.7 | 68.71 ± 14.9 | 64.48 ± 14.7 | −4.2 ± 3.1 |
| Total | 806 | 100.0 | 64.98 ± 14.9 | 65.86 ± 14.9 | 0.88 ± 4.9 * |
| Weight Change Categories | n | Weight Increase n (%) | No Weight Change n (%) | Weight Decrease n (%) | Weight Fluctuation n (%) | p |
|---|---|---|---|---|---|---|
| Sex | 0.031 | |||||
| Male | 186 | 93 (50.0) | 41 (22.0) | 29 (15.6) | 23 (12.4) | |
| Female | 267 (43.1) | 109 (17.6) | 153 (24.7) | 91 (14.7) | ||
| Age groups (years) | 0.004 | |||||
| 18–24 | 380 | 146 (38.4) | 70 (18.4) | 105 (27.6) | 59 (15.5) | |
| 25–44 | 325 | 163 (50.2) | 55 (16.9) | 63 (19.4) | 44 (13.5) | |
| 45–65 | 101 | 51 (50.5) | 25 (24.8) | 14 (13.9) | 11 (10.9) | |
| Marial status | <0.001 | |||||
| Married | 287 | 157 (54.7) | 54 (18.8) | 43 (15.0) | 33 (11.5) | |
| Single * | 519 | 203 (39.1) | 96 (18.5) | 139 (26.8) | 81 (15.6) | |
| Education level | 0.075 | |||||
| University | 659 | 289 (43.9) | 114 (17.3) | 155 (23.5) | 101 (15.3) | |
| High school | 102 | 46 (45.1) | 28 (27.5) | 18 (17.6) | 10 (9.8) | |
| Lower | 45 | 25 (55.6) | 8 (17.8) | 9 (20.0) | 3 (6.7) | |
| Income status | 0.732 | |||||
| Less income than expenses | 237 | 107 (45.1) | 39 (16.5) | 52 (21.9) | 39 (16.5) | |
| Income equals expenses | 408 | 180 (44.1) | 79 (19.4) | 98 (24.0) | 51 (12.5) | |
| More income than expenses | 161 | 73 (45.3) | 32 (19.9) | 32 (19.9) | 24 (14.9) | |
| Occupation † | <0.001 | |||||
| Employed | 324 | 168 (51.9) | 61 (18.8) | 58 (17.9) | 37 (11.4) | |
| Student | 318 | 112 (35.2) | 61 (19.2) | 96 (30.2) | 49 (15.4) | |
| Not employed | 164 | 80 (48.8) | 28 (17.1) | 28 (17.1) | 28 (17.1) | |
| Tobacco Use | 0.091 | |||||
| Current smoker | 172 | 81 (47.1) | 29 (16.9) | 39 (22.7) | 23 (13.4) | |
| Former smoker | 104 | 52 (50.0) | 15 (14.4) | 15 (14.4) | 22 (21.2) | |
| Never smoker | 530 | 227 (42.8) | 106 (20.0) | 128 (24.2) | 69 (13.0) |
| Weight Change Categories | ||||
|---|---|---|---|---|
| Themes and Subthemes | Weight Increase (n = 172) n (%) | Weight Decrease (n = 61) n (%) | Weight Fluctuation (n = 41) n (%) | Total (n = 274) n (%) |
| Eating Behaviors | ||||
| Changes in eating quantity and appetite | 35 (20.3) | 8 (13.1) | 10 (24.4) | 53 (19.3) |
| Changes in diet quality and food types | 13 (7.6) | 9 (14.8) | 4 (9.8) | 26 (9.5) |
| Changes in eating frequency and timing | 16 (9.3) | 6 (9.8) | 1 (2.4) | 23 (8.4) |
| Consumption of snacks and comfort foods | 20 (11.6) | - | 2 (4.9) | 22 (8.0) |
| Convenience food/home cooking | 6 (3.5) | 6 (9.8) | 2 (4.9) | 14 (5.1) |
| Intentional weight management behaviors | - | 9 (14.8) | 3 (7.3) | 12 (4.4) |
| Physical Activity and Routines | ||||
| Physical activity level and sedentary behavior | 84 (48.8) | 4 (6.6) | 21 (51.2) | 109 (39.8) |
| Exercise routines and opportunities | 11 (6.4) | 12 (19.7) | 2 (4.9) | 25 (9.1) |
| Psychosocial Factors | ||||
| Psychological distress | 10 (5.8) | 14 (23.0) | 7 (17.1) | 31 (11.3) |
| Boredom | 10 (5.8) | 1 (1.6) | 5 (12.2) | 16 (5.8) |
| Contextual/Environmental Changes | ||||
| Home confinement and free time | 29 (16.9) | 11 (18.0) | 5 (12.2) | 45 (16.4) |
| School/work intensity or model | 11 (6.4) | 2 (3.3) | 1 (2.4) | 14 (5.1) |
| Curfew restrictions | 10 (5.8) | 2 (3.3) | 1 (2.4) | 13 (4.7) |
| Other | 17 (10.1) | 5 (8.2) | 3 (7.2) | 25 (8.8) |
| Current BMI Status | ||||||
|---|---|---|---|---|---|---|
| Underweight n (%) | Normal n (%) | Overweight n (%) | Obese n (%) | Whole Sample n (%) * | p-Value | |
| Weight Loss Diet | 5 (7.2) | 118 (24.7) | 60 (32.6) | 24 (31.6) | 207 (25.7) | 0.002 |
| Exercise for Weight Loss | 9 (13.0) | 162 (34.0) | 55 (29.9) | 17 (22.4) | 243 (30.1) | <0.001 |
| Combined Diet and Exercise | 4 (3.1) | 83 (64.3) | 30 (23.3) | 12 (9.3) | 129 (16.0) | 0.109 |
| Weight Loss Products | - | 5 (1.0) | 6 (3.3) | 1 (1.3) | 12 (1.5) | NA |
| Other | - | 13 (2.7) | 3 (1.6) | 1 (1.3) | 17 (2.1) | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kircali-Haznedar, N.; Haydaroğlu, M.; Bilgiç, P. Self-Reported Body Weight Change and Weight Loss Practices During the COVID-19 Pandemic: A Mixed-Methods Study from Türkiye. COVID 2025, 5, 94. https://doi.org/10.3390/covid5060094
Kircali-Haznedar N, Haydaroğlu M, Bilgiç P. Self-Reported Body Weight Change and Weight Loss Practices During the COVID-19 Pandemic: A Mixed-Methods Study from Türkiye. COVID. 2025; 5(6):94. https://doi.org/10.3390/covid5060094
Chicago/Turabian StyleKircali-Haznedar, Nagihan, Mehmet Haydaroğlu, and Pelin Bilgiç. 2025. "Self-Reported Body Weight Change and Weight Loss Practices During the COVID-19 Pandemic: A Mixed-Methods Study from Türkiye" COVID 5, no. 6: 94. https://doi.org/10.3390/covid5060094
APA StyleKircali-Haznedar, N., Haydaroğlu, M., & Bilgiç, P. (2025). Self-Reported Body Weight Change and Weight Loss Practices During the COVID-19 Pandemic: A Mixed-Methods Study from Türkiye. COVID, 5(6), 94. https://doi.org/10.3390/covid5060094