Abstract
Background/Objectives: This retrospective observational study investigated coronavirus disease 2019 (COVID-19)-related mortality trends in the US throughout the pandemic. Methods: We performed a retrospective, descriptive analysis between 2020 and 2024 using data from the US National Center for Health Statistics. Results: The total number of COVID-19 deaths rose by 19% from 2020 to 2021, followed by a significant decline in the subsequent years, with an average reduction factor of 0.44. Mortality rates remained higher in males compared to females, with a gender disparity between 52 and 62%. Age-specific crude mortality rates increased with advancing age, with higher mortality observed in older populations. However, crude death rates significantly declined across all ages except for the 1–4 years group, which experienced a 33% increase. The majority of fatalities occurred in medical facilities (63–80%), but this proportion gradually decreased over time, while the percentage of deaths occurring at home nearly doubled from 2020 to 2024 (6% to 11%). Conclusions: The initial mortality peak for COVID-19 was followed by a substantial decline, likely influenced by the widespread availability of vaccines, improvements in clinical management, and the emergence of less virulent variants. The persistent gender and age disparities, alongside the fluctuating distribution of the places of death, offer insights for refining healthcare policies and optimizing resource allocation in this and other future pandemics.
1. Introduction
The coronavirus disease 2019 (COVID-19) pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has had a significant impact on global health, society, and economy since its emergence in late 2019 [1].
Mortality data provide important insights into the severity and progression of this disease and enable the identification of important risk factors such as age, pre-existing health conditions, and socioeconomic factors that predispose individuals to adverse outcomes, thus supporting the implementation of tailored interventions to protect or treat specific populations at increased risk [2]. Analyzing mortality trends for a particular disease is essential for evaluating healthcare system capacity and care efficiency. Such analyses indicate where additional human resources are needed, including doctors, nurses, and other healthcare professionals, as well as technical resources such as primary care, hospital beds, ventilators, essential medical supplies, and personal protective equipment [3]. Monitoring the impact of novel vaccines and therapeutic interventions on mortality rates also informs clinical practice by guiding the adoption of the most effective treatment strategies [4]. Detailed mortality data also play a pivotal role in epidemiological modeling and forecasting, enhancing the reliability of predictions regarding future disease waves and the associated demands on healthcare infrastructure [5]. Beyond addressing the immediate challenges of a pandemic like COVID-19, the collection and analysis of mortality data contribute to constructing a robust knowledge base for future global health threats. Policymakers and healthcare administrators can use this rationale to enhance preparedness and resilience against emerging crises [6]. In summary, the thorough study of mortality data serves as a cornerstone for saving lives, improving health system performance, and fostering resilience in the face of current and future public health challenges.
Therefore, this study aims to analyze COVID-19-related mortality in the US during the first five years of the pandemic. Specifically, we examined trends in overall mortality, as well as demographic factors such as gender, age, and place of occurrence to identify patterns and disparities in COVID-19 mortality. This analysis is expected to provide valuable insights into the broader impact of the pandemic on the general population, representing a reliable basis for controlling the spread of new variants or future infectious outbreaks [7].
2. Materials and Methods
We conducted a retrospective, descriptive study accessing the “Provisional Multiple Cause of Death” database maintained by the US National Center for Health Statistics (NCHS) through the Wide-Ranging Online Data for Epidemiologic Research (WONDER) interface [8]. This platform provides comprehensive nationwide information extracted from death certificates, including demographic data, geographical details, and the primary underlying causes of death. Our analysis focused on records identified by the International Classification of Diseases, 10th Revision (ICD-10) code U07.1, explicitly designated for “COVID-19” [9]. Our digital search encompassed the period from January 2020 to December 2024. Additional searches were conducted to stratify the data by gender, ten-year age groups, and place of death, combining these variables with the ICD-10 code U07.1. The resulting data included age-adjusted mortality rates (×100,000) for gender analysis, crude mortality rates (×100,000) for an analysis of the ten-year age classes, and total death counts with corresponding percentages for an analysis of the place of death. Both crude and age-adjusted mortality rates were reported alongside their respective 95% confidence intervals (95% CIs). This study was performed in agreement with the principles of the Declaration of Helsinki and complied with all relevant local regulations. As the NCHS WONDER is a publicly available, anonymized, and freely searchable database, this study was exempt from Ethical Committee approval.
3. Results
According to the NCHS, the total number of COVID-19-related US deaths (ICD-10 code U07.1) was 350,831 in 2020, 416,893 in 2021, 186,552 in 2022, 49,942 in 2023, and 30,483 in 2024. Cumulatively, the number of deaths for COVID-19 increased by around 19% from 2020 to 2021 but then declined considerably in the following years, by a mean factor of 0.44 (range 0.27–0.61).
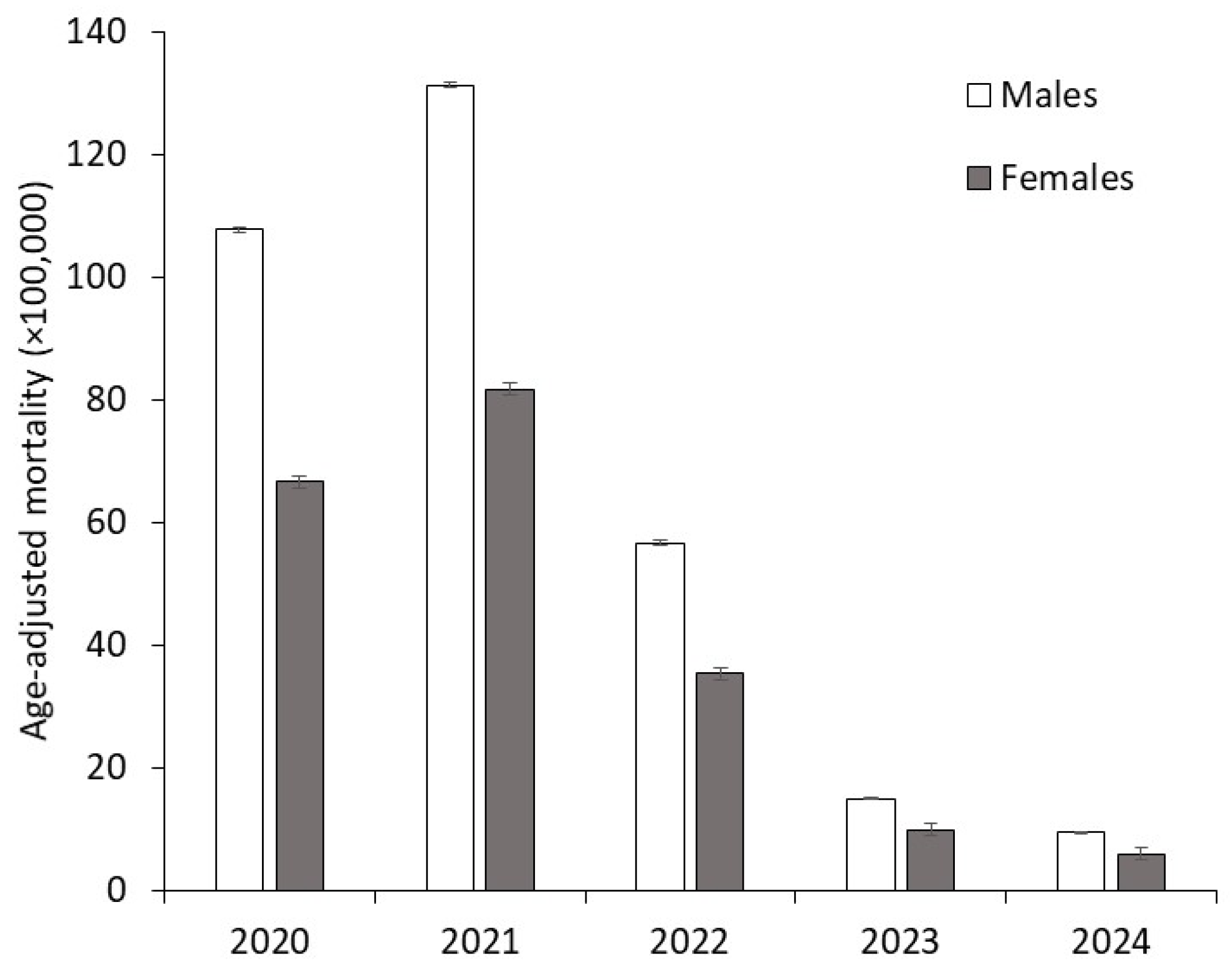
The age-adjusted mortality rates for COVID-19 across the first five years of the pandemic stratified by gender are illustrated in Figure 1.
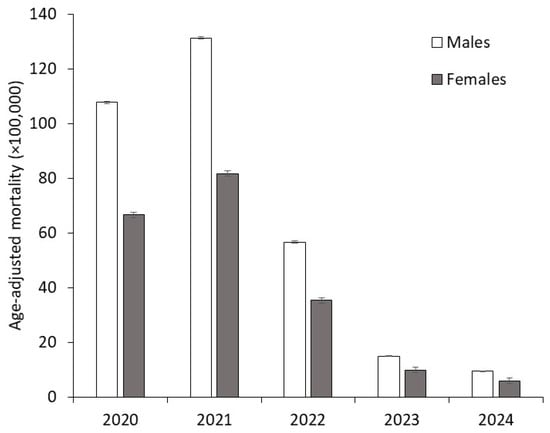
Figure 1.
Age-adjusted mortality rates for coronavirus disease 2019 (COVID-19) stratified by gender across the first five years of the pandemic (2020–2024).
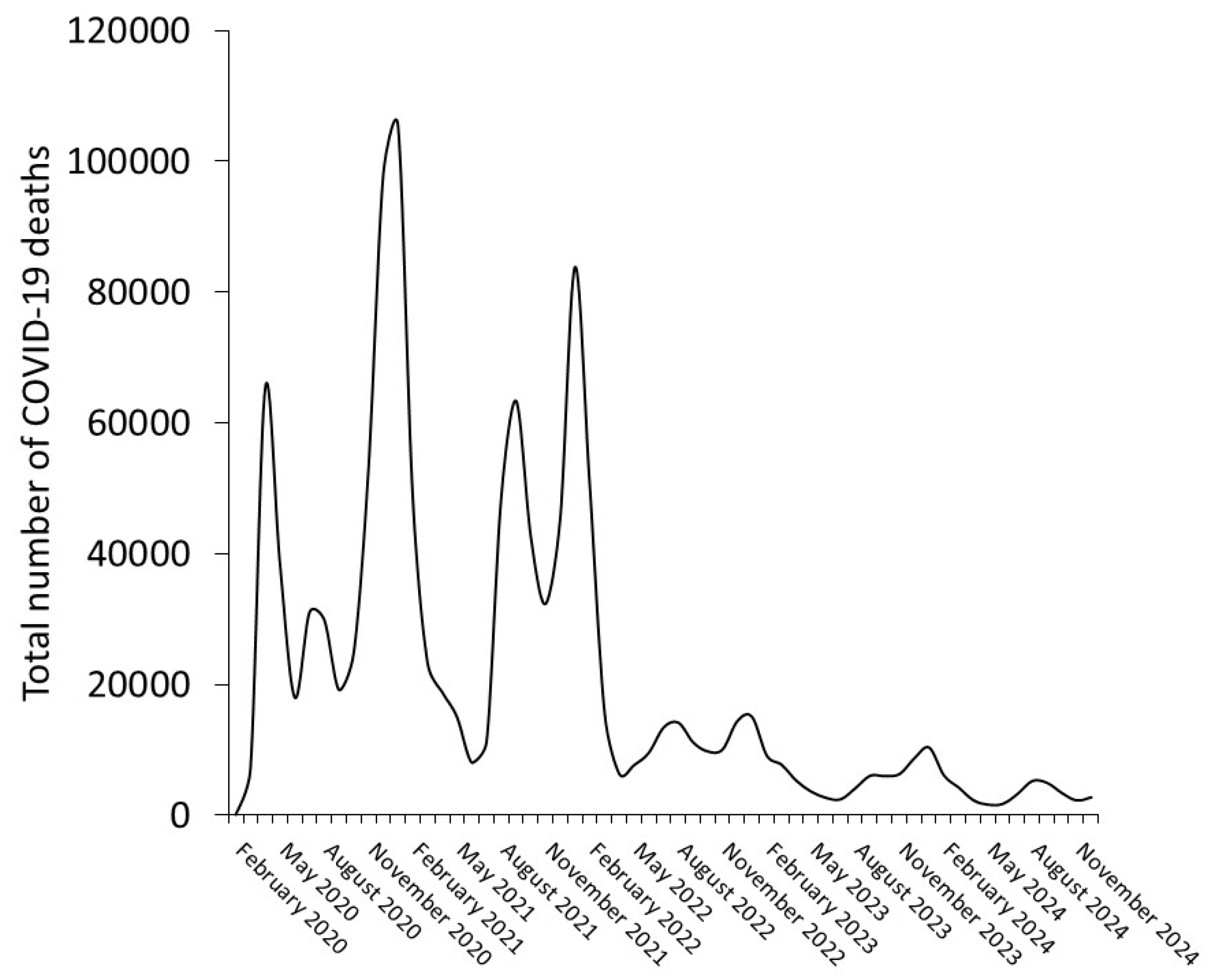
Mortality consistently remained approximately 60% higher in males compared to females. The male-to-female mortality ratio was 1.62 in 2020 and 1.61 in 2021, slightly decreased to 1.60 in 2022, and dropped to 1.52 in 2023 but then returned to 1.61 in 2024. As monthly age-adjusted or crude COVID-19 mortality rates are unavailable from the CDC WONDER dataset, Figure 2 presents the trend in the cumulative number of COVID-19 deaths by month from 2020 to 2024.
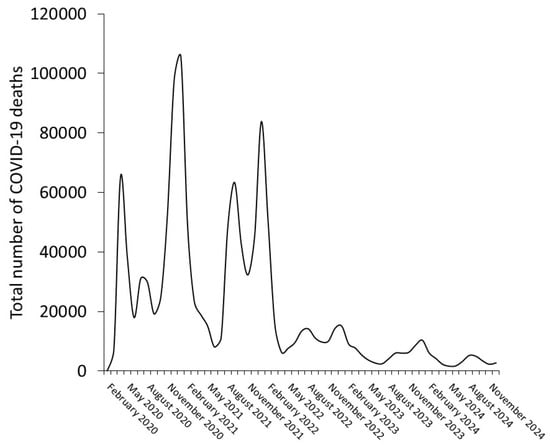
Figure 2.
Monthly trend in the cumulative number of COVID-19 deaths across the first five years of the pandemic (2020–2024).
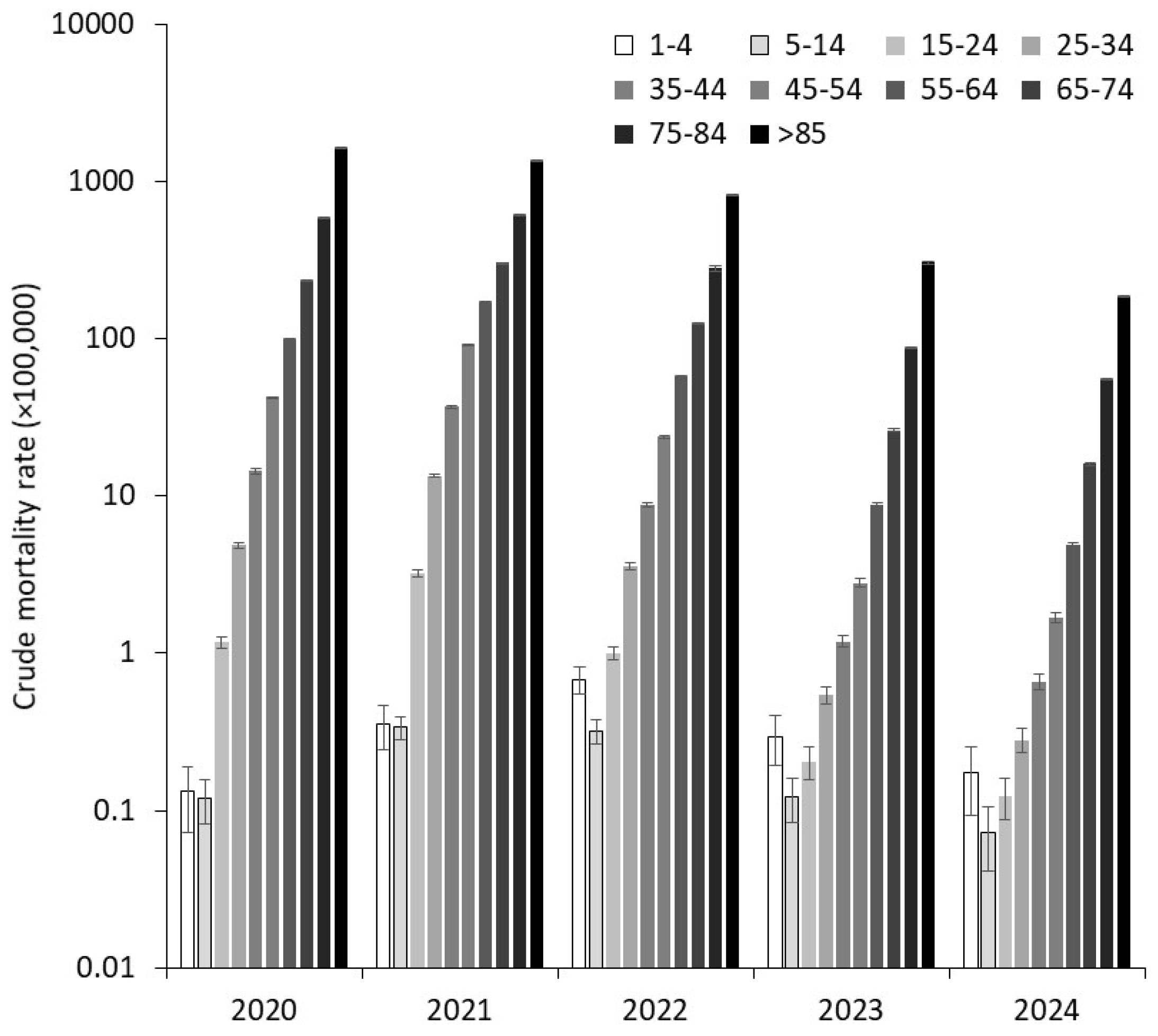
The mortality data for age groups are displayed in Figure 3, showing that crude death rates consistently increased with age across all five pandemic years.
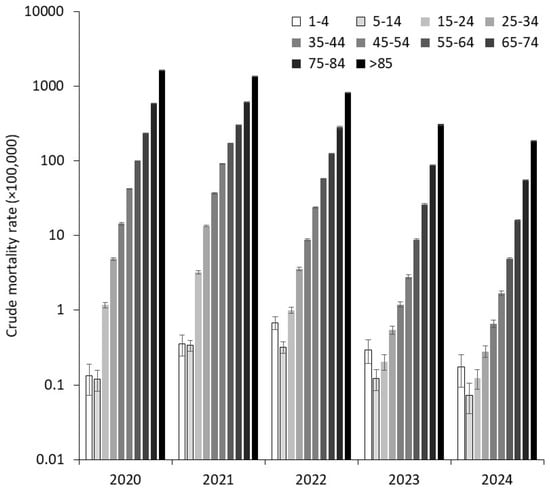
Figure 3.
Crude mortality rates for coronavirus disease 2019 (COVID-19) stratified by age classes across the first five years of the pandemic (2020–2024).
This trend remained remarkably consistent yearly, highlighting the persistent correlation between advancing age and higher mortality rates. However, a general decline in crude mortality rates was observed across all age groups except the youngest population. Specifically, the ratio of crude mortality between the years 2024 and 2020 showed an increase of +33% in the 1–4 years age group but significant declines in older age groups, as follows: −39% for those between 5 and 14 years, −89% for those between 15 and 24 years, −94% for those between 25 and 34 years, −95% for those between 35 and 44 years, −96% for those between 45 and 54 years, −95% for those between 55 and 64 years, −93% for those between 65 and 74 years, −91% for those between 75 and 84 years, and −89% for individuals aged 85 years and older.
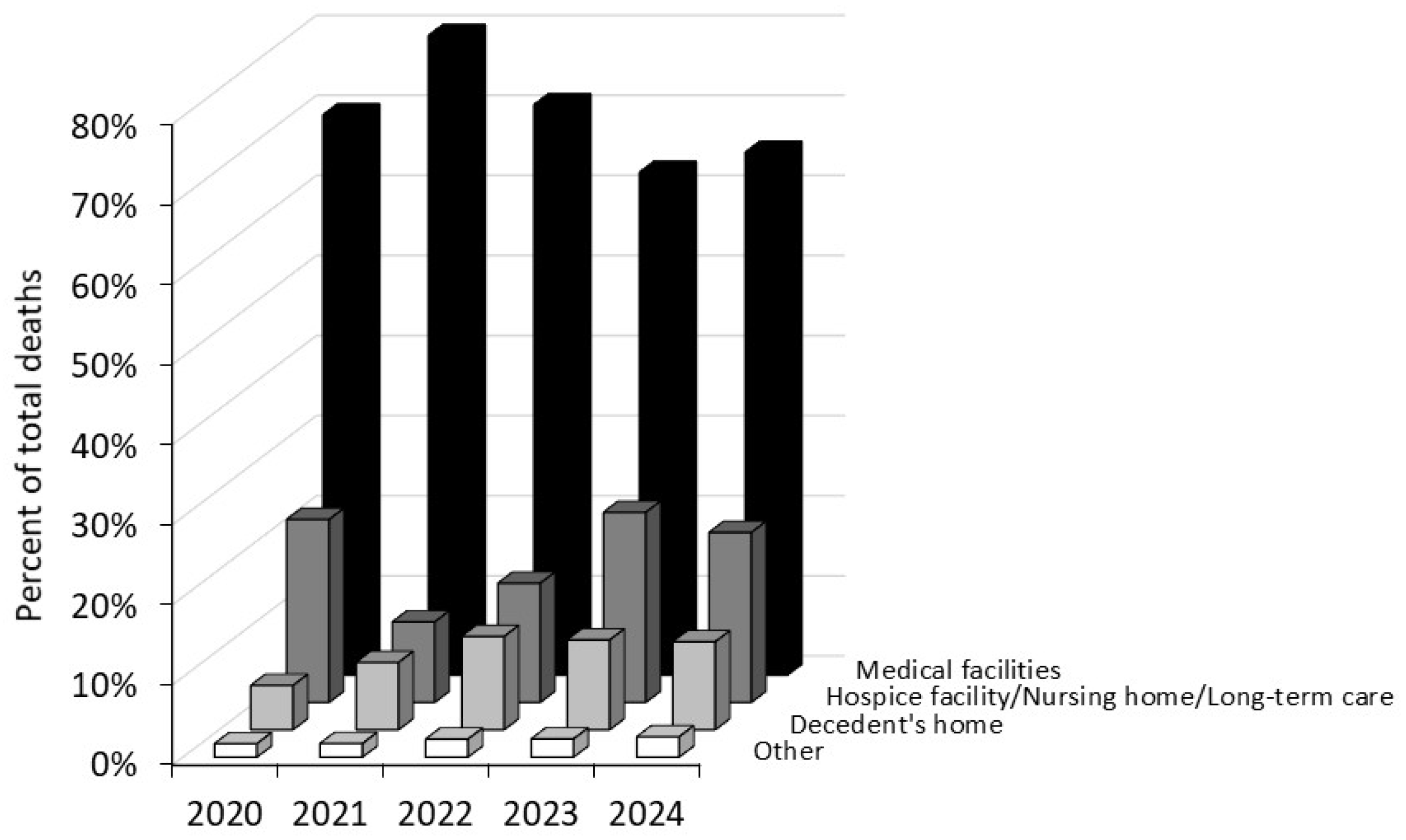
Regarding a descriptive analysis of the place of death, the majority of COVID-19 fatalities throughout the pandemic occurred in medical facilities (63–80%), followed by hospice facilities, nursing homes or long-term care settings (10–23%), decedents’ homes (6–12%), and other locations (2–3%) (Figure 4).
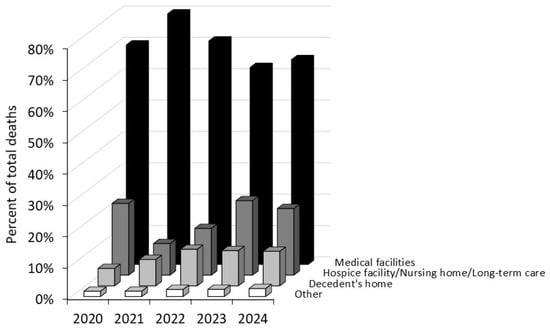
Figure 4.
Mortality for coronavirus disease 2019 (COVID-19) stratified by the place of death across the first five years of the pandemic (2020–2024).
Cumulatively, the percentage of deaths occurring in medical facilities clearly decreased over time, while the proportion of deaths in residents’ homes nearly doubled between 2020 and 2024.
4. Discussion
The systematic analysis of mortality data for a certain pathology is essential to better understand the trajectory of disease, its demographic impact, and trends over time [10]. The results of our analysis show that COVID-19 mortality in the US varied remarkably across years, gender, age groups, and places of death.
The dynamics of COVID-19-related mortality during the first five years of the pandemic reflect the evolving nature of the crisis, with a considerable decline observed over time. This reduction can be attributed to multiple interrelated factors, including the widespread availability of COVID-19 vaccines and the development of natural immunity against the virus [11,12]; advances in clinical management that have improved and refined the therapeutic arsenal against this life-threatening disease [13]; and the high mortality among older and more vulnerable populations during the early pandemic years (2020–2021) which may have further reduced the pool of individuals at the highest risk of a worse clinical outcome and contributed to fewer deaths in subsequent years, along with the emergence of less virulent variants that has led to the gradual attenuation of SARS-CoV-2 virulence [14].
Our analysis provides additional evidence that males have been disproportionately impacted by COVID-19, exhibiting consistently higher mortality rates than females (between 52 and 62%). This gender disparity is likely driven by a combination of biological, behavioral, and social factors, such as weaker immune responses in males, a higher prevalence of comorbidities among men, and lower healthcare-seeking behaviors in males [15]. However, our findings are consistent with those reported by Ramírez-Soto et al. [16], who analyzed COVID-19 fatality rates across 73 different countries during the years 2020–2021 and concluded that the infection fatality rate was 40% higher in men than in women (3.17% vs. 2.26%).
Older adults have faced a significantly higher risk of aggravation (e.g., intensive care unit [ICU] admission) and mortality due to age-related vulnerabilities, including weakened immune responses, a higher prevalence of underlying medical conditions, and potentially lower care access [17,18]. Nevertheless, our analysis revealed a differential impact of COVID-19 on very early child (1–4 years) mortality, with a 33% increase observed between 2020 and 2024, although the crude death rate in 2024 was still nearly 70% lower compared to the peak mortality in 2022 for this age group. This indicates that the overall mortality rate for children has dropped far below the highest levels recorded during the pandemic height. This trend is divergent when compared to the mortality rates of other age groups, which showed a considerable decline between 2020 and 2024. One significant factor that may have contributed to the observed trend in early child mortality is the potential misclassification or incorrect attribution of the ICD-10 code, especially during the first few years of the pandemic, thus leading to the potential underestimation of total deaths in 2020. During the initial wave of the COVID-19 pandemic, several challenges arose regarding the timely and accurate assignment of ICD-10 codes for pediatric deaths. Children often present with atypical or less pronounced symptoms of COVID-19 compared to adults, which could have led to the misidentification of the direct cause of death [19]. Specifically, some pediatric COVID-19 cases may have been misclassified as other respiratory illnesses, such as influenza or respiratory syncytial virus (RSV) infections, which are more commonly diagnosed in children [20]. As a result, some deaths may have been attributed to these conditions rather than directly to COVID-19, potentially distorting the accuracy of mortality data and hindering a comprehensive understanding of the pandemic’s impact on pediatric health.
Beyond demographic disparities, the place of death provides critical insights into the role of the healthcare system during the pandemic. Although the statistical evaluation of the differences is delayed until we will perform and publish deeper analyses, it can be inferred that a substantial proportion of deaths occurred in medical facilities, underscoring the immense strain on hospitals during peak pandemic waves. This observation is consistent with early data reported by the US Cybersecurity & Infrastructure Security Agency (CISA) COVID Task Force [21], which indicated that when ICU bed usage nationwide reached 75% capacity, an estimated 12,000 additional excess deaths occurred over the subsequent two weeks. Nevertheless, the notable proportion of deaths that occurred in nursing homes, hospice facilities, and private residences highlights the extensive impact of the COVID-19 pandemic on vulnerable populations outside traditional hospital settings [22].
The infection fatality rate (IFR) of SARS-CoV-2 increases markedly with age, approximately doubling every five years from childhood onward. Among individuals over 80 years of age, the IFR exceeds 8% [23]. This age-dependent risk is further exacerbated by immunological factors, notably including circulating autoantibodies that neutralize type I interferons (IFN-α, IFN-ω, and/or IFN-β). Such autoantibodies are detected in approximately 20% of COVID-19-related deaths across all age groups [24,25]. Importantly, these autoantibodies are typically pre-existing and show an age-associated increase in prevalence, present in ~1% of individuals under 70 and more than 4% of those over 70 in the general population [24,25]. Autoimmunity against type I interferons is a strong predictor of COVID-19 mortality. Individuals under 70 years old who harbor autoantibodies neutralizing both IFN-α2 and IFN-ω exhibit a relative risk of death up to 188-fold higher than those without these autoantibodies [24]. In parallel, genetic predispositions also contribute to severe COVID-19 outcomes, particularly among males. Loss-of-function mutations in TLR7, a gene on the X chromosome essential for sensing viral single-stranded RNA, have been identified in 1.4–2.1% of young males with life-threatening COVID-19 pneumonia [26]. These mutations compromise both type I and type II interferon signaling pathways. These findings underscore the critical interplay between age-related immunological decline, genetic susceptibility, and defective innate immune responses in the pathogenesis of severe COVID-19 [27,28].
Regional disparities in COVID-19 mortality have been well-documented in the US. For instance, Stoto et al. reported that, as of 31 May 2020, the Southern states experienced significantly higher mortality rates than other regions, accounting for over 60% of potentially avoidable deaths [29]. Based on this, multiple studies have highlighted the profound influence of ethnicity on COVID-19 outcomes across the age spectrum. Among older adults, structural racism and long-standing health inequities have contributed to a disproportionate burden of COVID-19 morbidity and mortality among Black, Latinx, and Indigenous populations, as these groups have experienced higher IFRs and faced systemic barriers to healthcare access compared to non-Hispanic white populations [30]. In pediatric and adolescent populations, the effects of ethnicity have also been pronounced. The social determinants of health—including family composition, socioeconomic status, and exposure to racism—have intensified the transgenerational impacts of the pandemic. Non-white and Spanish-speaking families, in particular, have reported heightened financial stress and food insecurity and diminished access to critical resources, all of which contribute to widening health disparities [31]. While public perception often frames older adults as the most vulnerable to COVID-19, evidence suggests that racial and ethnic disparities span all age groups, albeit through different mechanisms and with varying degrees of impact [32]. These findings highlight the imperative for equity-centered public health strategies to mitigate the age-transcending effects of ethnicity on COVID-19 outcomes.
We finally acknowledge that this study may have some limitations. As a retrospective observational analysis, this study is subject to the inherent bias associated with the reliability of secondary data sources. Exclusive reliance on death certificates from the NCHS introduces the potential for misclassification and incomplete reporting, especially during the early phases of the COVID-19 pandemic, when diagnostic accuracy was constrained. While this study examines mortality trends across demographic groups, it cannot account for key confounding factors such as socioeconomic disparities, care access, preventive behaviors, vaccine uptake, and the impact of SARS-CoV-2 variants, as these variables are unavailable in the WONDER database. Finally, it is well established that the number of reported COVID-19 deaths substantially underestimates the true mortality burden attributable to SARS-CoV-2 infection, whether directly or indirectly, during the course of the pandemic.
5. Conclusions
In conclusion, the results of our analysis indicate that COVID-19-related mortality in the US peaked in 2021 and has significantly declined in the subsequent years. This trend is likely attributable to a combination of factors, including increased population immunity through vaccination and natural infection, better healthcare preparedness, advancements in clinical management strategies, and evolution of the virus into variants with potentially lower pathogenicity [33]. Mortality consistently increased with age, though crude death rates declined across most age groups except the youngest. Male mortality was approximately 60% higher than female mortality throughout the pandemic. A significant shift in the place of death occurred over time, with an apparent decline in deaths in medical facilities and a nearly doubling of home deaths by 2024 (further statistical analyses are warranted to more accurately characterize the significance of these trends), thus underscoring the need for enhanced vigilance and strengthened home-based care for patients at a higher risk of developing more aggressive forms of COVID-19.
Author Contributions
Conceptualization, C.M. and G.L.; methodology, C.M.; formal analysis, G.L.; data curation, G.L.; writing—original draft preparation, C.M.; writing—review and editing, G.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The NCHS WONDER is a publicly available, anonymized, and freely searchable database, so this study was exempt from Ethical Committee approval.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| COVID-19 | Coronavirus disease 2019 |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| NCHS | National Center for Health Statistics |
| WONDER | Wide-Ranging Online Data for Epidemiologic Research |
| ICD-10 | International Classification of Diseases, 10th Revision |
| ICU | Intensive care unit |
| RSV | Respiratory syncytial virus |
| CISA | Cybersecurity & Infrastructure Security Agency |
References
- Mattiuzzi, C.; Lippi, G. COVID-19: Lessons from the Past to Inform the Future of Healthcare. COVID 2025, 5, 4. [Google Scholar] [CrossRef]
- Hernandez, J.B.R.; Kim, P.Y. Epidemiology Morbidity And Mortality. [Updated 3 October 2022]. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK547668/ (accessed on 13 January 2025).
- Khan, J.R.; Awan, N.; Islam, M.M.; Muurlink, O. Healthcare Capacity, Health Expenditure, and Civil Society as Predictors of COVID-19 Case Fatalities: A Global Analysis. Front. Public Health 2020, 8, 347. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Tran, T.N.; Howerton, E.; Boni, M.F.; Servadio, J.L. Benefits of near-universal vaccination and treatment access to manage COVID-19 burden in the United States. BMC Med. 2023, 21, 321. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M.; Plebani, M. A Simple Epidemiologic Model for Predicting Impaired Neutralization of New SARS-CoV-2 Variants. Vaccines 2023, 11, 128. [Google Scholar] [CrossRef]
- Filip, R.; Gheorghita Puscaselu, R.; Anchidin-Norocel, L.; Dimian, M.; Savage, W.K. Global Challenges to Public Health Care Systems during the COVID-19 Pandemic: A Review of Pandemic Measures and Problems. J. Pers. Med. 2022, 12, 1295. [Google Scholar] [CrossRef]
- Cueni, T. Lessons learned from COVID-19 to stop future pandemics. Lancet 2023, 401, 1340. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Provisional Mortality on CDC WONDER Online Database. Data Are from the Final Multiple Cause of Death Files, 2018–2022, and from Provisional Data for Years 2023–2024, as Compiled from Data Provided by the 57 Vital Statistics Jurisdictions Through the Vital Statistics Cooperative Program. Available online: http://wonder.cdc.gov/mcd-icd10-provisional.html (accessed on 13 January 2025).
- ICD-10-CM Codes. 2025 ICD-10-CM Diagnosis Code U07.1. Available online: https://www.icd10data.com/ICD10CM/Codes/U00-U85/U00-U49/U07-/U07.1 (accessed on 13 January 2025).
- Matthes, K.L.; Staub, K. The Need to Analyse Historical Mortality Data to Understand the Causes of Today’s Health Inequalities. Int. J. Public Health 2024, 69, 1607739. [Google Scholar] [CrossRef]
- Franchi, M.; Pellegrini, G.; Cereda, D.; Bortolan, F.; Leoni, O.; Pavesi, G.; Galli, M.; Valenti, G.; Corrao, G. Natural and vaccine-induced immunity are equivalent for the protection against SARS-CoV-2 infection. J. Infect. Public Health 2023, 16, 1137–1141. [Google Scholar] [CrossRef]
- Tsagkli, P.; Geropeppa, M.; Papadatou, I.; Spoulou, V. Hybrid Immunity against SARS-CoV-2 Variants: A Narrative Review of the Literature. Vaccines 2024, 12, 1051. [Google Scholar] [CrossRef]
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; Baden, L.; Cheng, V.C.C.; Edwards, K.M.; Gallagher, J.C.; Gandhi, R.T.; Muller, W.J.; Nakamura, M.M.; et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients With COVID-19 (September 2022). Clin. Infect. Dis. 2024, 78, e250–e449. [Google Scholar] [CrossRef]
- Livieratos, A.; Gogos, C.; Akinosoglou, K. SARS-CoV-2 Variants and Clinical Outcomes of Special Populations: A Scoping Review of the Literature. Viruses 2024, 16, 1222. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, M.; Gültekin, N.; Stanga, Z.; Fehr, J.S.; Ülgür, I.I.; Schlagenhauf, P. Disparities in response to mRNA SARS-CoV-2 vaccines according to sex and age: A systematic review. New Microbes New Infect. 2024, 63, 101551. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Soto, M.C.; Ortega-Cáceres, G.; Arroyo-Hernández, H. Sex differences in COVID-19 fatality rate and risk of death: An analysis in 73 countries, 2020–2021. Infez. Med. 2021, 29, 402–407. [Google Scholar] [CrossRef]
- Shahid, Z.; Kalayanamitra, R.; McClafferty, B.; Kepko, D.; Ramgobin, D.; Patel, R.; Aggarwal, C.S.; Vunnam, R.; Sahu, N.; Jain, R.; et al. COVID-19 and Older Adults: What We Know. J. Am. Geriatr. Soc. 2020, 68, 926–929. [Google Scholar] [CrossRef]
- Rossi, A.P.; Gottin, L.; Donadello, K.; Schweiger, V.; Nocini, R.; Taiana, M.; Zamboni, M.; Polati, E. Obesity as a risk factor for unfavourable outcomes in critically ill patients affected by Covid 19. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 762–768. [Google Scholar] [CrossRef]
- Martin, B.; Rao, S.; Bennett, T.D. Disparities in Multisystem Inflammatory Syndrome in Children and COVID-19 Across the Organ Dysfunction Continuum. JAMA Netw. Open 2023, 6, e2249552. [Google Scholar] [CrossRef]
- Belza, C.; Pullenayegum, E.; Nelson, K.E.; Aoyama, K.; Fu, L.; Buchanan, F.; Diaz, S.; Goldberg, O.; Guttmann, A.; Hepburn, C.M.; et al. Severe Respiratory Disease Among Children With and Without Medical Complexity During the COVID-19 Pandemic. JAMA Netw. Open 2023, 6, e2343318. [Google Scholar] [CrossRef]
- French, G.; Hulse, M.; Nguyen, D.; Sobotka, K.; Webster, K.; Corman, J.; Aboagye-Nyame, B.; Dion, M.; Johnson, M.; Zalinger, B.; et al. Impact of Hospital Strain on Excess Deaths During the COVID-19 Pandemic—United States, July 2020–July 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1613–1616. [Google Scholar] [CrossRef]
- Shen, K.; Loomer, L.; Abrams, H.; Grabowski, D.C.; Gandhi, A. Estimates of COVID-19 Cases and Deaths Among Nursing Home Residents Not Reported in Federal Data. JAMA Netw. Open 2021, 4, e2122885. [Google Scholar] [CrossRef]
- O’Driscoll, M.; Ribeiro Dos Santos, G.; Wang, L.; Cummings, D.A.T.; Azman, A.S.; Paireau, J.; Fontanet, A.; Cauchemez, S.; Salje, H. Age-specific mortality and immunity patterns of SARS-CoV-2. Nature 2021, 590, 140–145. [Google Scholar] [CrossRef]
- Manry, J.; Bastard, P.; Gervais, A.; Le Voyer, T.; Rosain, J.; Philippot, Q.; Michailidis, E.; Hoffmann, H.H.; Eto, S.; Garcia-Prat, M.; et al. The risk of COVID-19 death is much greater and age dependent with type I IFN autoantibodies. Proc. Natl. Acad. Sci. USA 2022, 119, e2200413119. [Google Scholar] [CrossRef] [PubMed]
- Bastard, P.; Gervais, A.; Le Voyer, T.; Rosain, J.; Philippot, Q.; Manry, J.; Michailidis, E.; Hoffmann, H.H.; Eto, S.; Garcia-Prat, M.; et al. Autoantibodies neutralizing type I IFNs are present in ~4% of uninfected individuals over 70 years old and account for ~20% of COVID-19 deaths. Sci. Immunol. 2021, 6, eabl4340. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Bastard, P.; COVID Human Genetic Effort; Cobat, A.; Casanova, J.L. Human genetic and immunological determinants of critical COVID-19 pneumonia. Nature 2022, 603, 587–598. [Google Scholar] [CrossRef] [PubMed]
- Bastard, P. Why do people die from COVID-19? Science 2022, 375, 829–830. [Google Scholar] [CrossRef]
- van der Mescht, M.A.; de Beer, Z.; Steel, H.C.; Anderson, R.; Masenge, A.; Moore, P.L.; Bastard, P.; Casanova, J.L.; Abdullah, F.; Ueckermann, V.; et al. Aberrant innate immune profile associated with COVID-19 mortality in Pretoria, South Africa. Clin. Immunol. 2024, 266, 110323. [Google Scholar] [CrossRef]
- Stoto, M.A.; Schlageter, S.; Kraemer, J.D. COVID-19 mortality in the United States: It’s been two Americas from the start. PLoS ONE 2022, 17, e0265053. [Google Scholar] [CrossRef]
- Garcia, M.A.; Homan, P.A.; García, C.; Brown, T.H. The Color of COVID-19: Structural Racism and the Disproportionate Impact of the Pandemic on Older Black and Latinx Adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e75–e80. [Google Scholar] [CrossRef]
- Yip, S.W.; Jordan, A.; Kohler, R.J.; Holmes, A.; Bzdok, D. Multivariate, Transgenerational Associations of the COVID-19 Pandemic Across Minoritized and Marginalized Communities. JAMA Psychiatry 2022, 79, 350–358. [Google Scholar] [CrossRef]
- Menendez, D.; Labotka, D.; Umscheid, V.A.; Gelman, S.A. The social aspects of illness: Children’s and parents’ explanations of the relation between social categories and illness in a predominantly white U.S. sample. Child Dev. 2024, 95, 1676–1692. [Google Scholar] [CrossRef]
- Lippi, G.; Nocini, R.; Henry, B.M. Analysis of online search trends suggests that SARS-CoV-2 Omicron (B.1.1.529) variant causes different symptoms. J. Infect. 2022, 84, e76–e77. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).