
Mental Health Impacts of the COVID-19 Pandemic on Australian Children and Adolescents with a Medical Condition: Longitudinal Findings
 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Measures
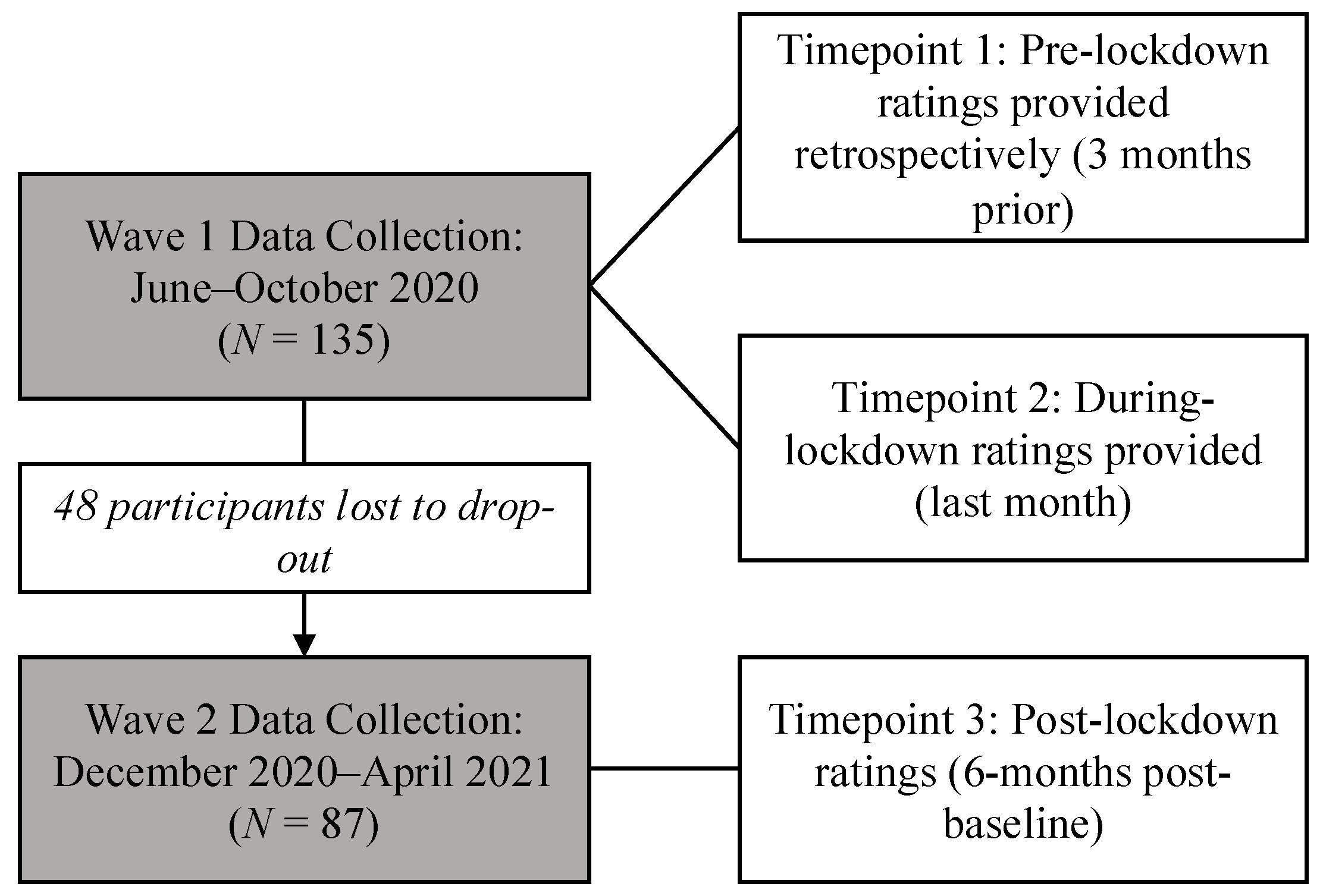
2.2. Procedure
2.3. Statistical Analyses
3. Results
3.1. Mental Health Symptoms During Lockdown (T2)
3.2. Mental Health Symptoms Post-Lockdown (T3)
3.3. Mental Health Symptoms and Covariates
3.4. Child and Adolescent Activities
3.5. Healthcare
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Edwards, B.; Barnes, R.; Rehill, P.; Ellen, L.; Zhong, F.; Killigrew, A.; Gonzalez, P.R.; Sheard, E.; Zhu, R.; Philips, T. Variation in Policy Response to COVID-19 Across Australian States and Territories; Blavatnik School of Government: Oxford, UK; University of Oxford: Oxford, UK, 2022. [Google Scholar]
- Creswell, C.; Shum, A.; Pearcey, S.; Skripkauskaite, S.; Patalay, P.; Waite, P. Young people’s mental health during the COVID-19 pandemic. Lancet Child Adolesc. Health 2021, 5, 535–537. [Google Scholar] [CrossRef] [PubMed]
- Samji, H.; Wu, J.; Ladak, A.; Vossen, C.; Stewart, E.; Dove, N.; Long, D.; Snell, G. Mental health impacts of the COVID-19 pandemic on children and youth—A systematic review. Child Adolesc. Ment. Health 2022, 27, 173–189. [Google Scholar] [CrossRef] [PubMed]
- Sicouri, G.; March, S.; Pellicano, E.; De Young, A.C.; Donovan, C.L.; Cobham, V.E.; Rowe, A.; Brett, S.; Russell, J.K.; Uhlmann, L. Mental health symptoms in children and adolescents during COVID-19 in Australia. Aust. N. Z. J. Psychiatry 2023, 57, 213–229. [Google Scholar] [CrossRef] [PubMed]
- Kauhanen, L.; Wan Mohd Yunus, W.M.A.; Lempinen, L.; Peltonen, K.; Gyllenberg, D.; Mishina, K.; Gilbert, S.; Bastola, K.; Brown, J.S.; Sourander, A. A systematic review of the mental health changes of children and young people before and during the COVID-19 pandemic. Eur. Child Adolesc. Psychiatry 2023, 32, 995–1013. [Google Scholar] [CrossRef] [PubMed]
- Cobham, V.E.; Hickling, A.; Kimball, H.; Thomas, H.J.; Scott, J.G.; Middeldorp, C.M. Systematic review: Anxiety in children and adolescents with chronic medical conditions. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 595–618. [Google Scholar] [CrossRef] [PubMed]
- Tegethoff, M.; Belardi, A.; Stalujanis, E.; Meinlschmidt, G. Association between mental disorders and physical diseases in adolescents from a nationally representative cohort. Psychosom. Med. 2015, 77, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Wauters, A.; Vervoort, T.; Dhondt, K.; Soenens, B.; Vansteenkiste, M.; Morbée, S.; Waterschoot, J.; Haerynck, F.; Vandekerckhove, K.; Verhelst, H. Mental health outcomes among parents of children with a chronic disease during the COVID-19 pandemic: The role of parental burn-out. J. Pediatr. Psychol. 2022, 47, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Ademhan Tural, D.; Emiralioglu, N.; Tural Hesapcioglu, S.; Karahan, S.; Ozsezen, B.; Sunman, B.; Nayir Buyuksahin, H.; Yalcin, E.; Dogru, D.; Ozcelik, U. Psychiatric and general health effects of COVID-19 pandemic on children with chronic lung disease and parents’ coping styles. Pediatr. Pulmonol. 2020, 55, 3579–3586. [Google Scholar] [CrossRef] [PubMed]
- Hawke, L.D.; Monga, S.; Korczak, D.; Hayes, E.; Relihan, J.; Darnay, K.; Cleverley, K.; Lunsky, Y.; Szatmari, P.; Henderson, J. Impacts of the COVID-19 pandemic on youth mental health among youth with physical health challenges. Early Interv. Psychiatry 2021, 15, 1146–1153. [Google Scholar] [CrossRef] [PubMed]
- Strisciuglio, C.; Martinelli, M.; Lu, P.; Lev, M.R.B.; Beinvogl, B.; Benninga, M.A.; Di Lorenzo, C.; Nastro, F.F.; Nurko, S.; Pearlstein, H. Overall impact of coronavirus disease 2019 outbreak in children with functional abdominal pain disorders: Results from the first pandemic phase. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, K.D.; Exner-Cortens, D.; McMorris, C.A.; Makarenko, E.; Arnold, P.; Van Bavel, M.; Williams, S.; Canfield, R. COVID-19 and student well-being: Stress and mental health during return-to-school. Can. J. Sch. Psychol. 2021, 36, 166–185. [Google Scholar] [CrossRef] [PubMed]
- Gordon-Hacker, A.; Bar-Shachar, Y.; Egotubov, A.; Uzefovsky, F.; Gueron-Sela, N. Trajectories and associations between maternal depressive symptoms, household Chaos and Children’s adjustment through the COVID-19 pandemic: A four-wave longitudinal study. Res. Child Adolesc. Psychopathol. 2023, 51, 103–117. [Google Scholar] [CrossRef] [PubMed]
- Campbell, D. Josh Frydenberg Says Melbourne is the World’s Most Locked Down City. Is That Correct? Australian Broadcasting Corporation. 2021. Available online: https://www.abc.net.au/news/2021-10-25/fact-check-is-melbourne-most-locked-down-city/100560172 (accessed on 22 December 2024).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Merikangas, K.; Milham, M.; Stringaris, A.; Bromet, E.; Colcombe, S.; Zipunnikov, V. The Coronavirus Health Impact Survey (CRISIS). Available online: www.crisissurvey.org (accessed on 16 September 2024).
- Stata/SE 18.5; StataCorp LLC: College Station, TX, USA, 2024.
- Shum, A.; Skripkauskaite, S.; Pearcey, S.; Waite, P.; Creswell, C. Children and Adolescents’ Mental Health: One Year in the Pandemic; Co-Space Study: Oxford, UK, 2021. [Google Scholar]
- Orben, A.; Tomova, L.; Blakemore, S.-J. The effects of social deprivation on adolescent development and mental health. Lancet Child Adolesc. Health 2020, 4, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Ellis, W.E.; Dumas, T.M.; Forbes, L.M. Physically isolated but socially connected: Psychological adjustment and stress among adolescents during the initial COVID-19 crisis. Can. J. Behav. Sci. 2020, 52, 177. [Google Scholar] [CrossRef]
- Lissak, G. Adverse physiological and psychological effects of screen time on children and adolescents: Literature review and case study. Environ. Res. 2018, 164, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Reilly, C.; Muggeridge, A.; Cross, J.H. The perceived impact of COVID-19 and associated restrictions on young people with epilepsy in the UK: Young people and caregiver survey. Seizure 2021, 85, 111–114. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Total n = 135 | |
|---|---|
| Child characteristics | |
| Age [years], M (SD) | 10.1 (3.6) |
| Sex [male], n (%) | 79 (58.5) |
| Education setting, n (%) | |
| Pre-school/kinder/ELC | 17 (12.6) |
| Primary/secondary school | 117 (86.7) |
| Not attending any | 1 (0.7) |
| Parent characteristics | |
| Respondent, n (%) | |
| Mother | 125 (92.6) |
| Father | 9 (6.6) |
| Other | 1 (0.7) |
| Born in Australia, n (%) | 112 (83.0) |
| Indigenous Australian, n (%) | 4 (3.0) |
| English only, n (%) | 120 (88.9) |
| Partnered, n (%) | 103 (76.3) |
| Highest education, n (%) | |
| Less than high school | 20 (14.8) |
| High school | 5 (3.7) |
| Certificate/diploma | 48 (35.6) |
| Bachelor’s degree | 31 (23.0) |
| Postgraduate | 31 (23.0) |
| Anxiety | Fatigue | |||||
|---|---|---|---|---|---|---|
| B | (95% CI) | p | B | 95% CI | p | |
| Time | ||||||
| Pre-COVID-19 (T1) | Ref. | Ref. | ||||
| Lockdown (T2) | 0.49 | (0.30, 0.69) | <0.001 | 0.34 | (0.17, 0.52) | <0.001 |
| Post-lockdown (T3) | 0.32 | (0.11, 0.52) | 0.002 | 0.17 | (−0.02, 0.36) | 0.071 |
| Covariates | ||||||
| Sex (female) | 0.22 | (−0.06, 0.50) | 0.129 | 0.003 | (−0.27, 0.28) | 0.982 |
| Age (per 5 years) | 0.09 | (−0.07, 0.25) | 0.288 | 0.03 | (−0.13, 0.18) | 0.724 |
| Parent stress | 0.005 | (−0.001, 0.010) | 0.117 | 0.002 | (−0.004, 0.008) | 0.494 |
| Screen time | 0.03 | (−0.03, 0.09) | 0.313 | −0.002 | (−0.054, 0.049) | 0.931 |
| Parent education | −0.04 | (−0.18, 0.11) | 0.603 | −0.01 | (−0.16, 0.13) | 0.858 |
| Distractibility | Sadness | |||||
| B | (95% CI) | p | B | (95% CI) | p | |
| Time | ||||||
| Pre-COVID-19 (T1) | Ref. | Ref. | ||||
| Lockdown (T2) | 0.17 | (0.003, 0.341) | 0.046 | 0.45 | (0.27, 0.64) | <0.001 |
| Post-lockdown (T3) | 0.16 | (−0.02, 0.33) | 0.089 | 0.58 | (0.38, 0.78) | <0.001 |
| Covariates | ||||||
| Sex (Female) | −0.24 | (−0.57, 0.10) | 0.164 | −0.01 | (−0.26, 0.24) | 0.935 |
| Age (per 5 years) | −0.003 | (−0.188, 0.182) | 0.975 | 0.08 | (−0.06, 0.22) | 0.249 |
| Parent stress | 0.01 | (0.001, 0.015) | 0.024 | 0.01 | (0.000, 0.010) | 0.038 |
| Screen time | 0.03 | (−0.03, 0.08) | 0.350 | 0.06 | (0.01, 0.12) | 0.017 |
| Parent education | −0.17 | (−0.339, 0.002) | 0.053 | −0.08 | (−0.21, 0.05) | 0.214 |
| Irritability | Loneliness | |||||
| B | (95% CI) | p | B | (95% CI) | p | |
| Time | ||||||
| Pre-COVID-19 (T1) | Ref. | Ref. | ||||
| Lockdown (T2) | 0.54 | (0.36, 0.72) | <0.001 | 0.74 | (0.56, 0.91) | <0.001 |
| Post-lockdown (T3) | 0.05 | (−0.14, 0.24) | 0.627 | 0.23 | (0.05, 0.41) | 0.014 |
| Covariates | ||||||
| Sex (Female) | −0.16 | (−0.46, 0.15) | 0.319 | 0.16 | (−0.10, 0.41) | 0.223 |
| Age (per 5 years) | −0.11 | (−0.28, 0.07) | 0.227 | 0.10 | (−0.04, 0.24) | 0.173 |
| Parent stress | 0.01 | (0.006, 0.018) | <0.001 | 0.01 | (0.005, 0.016) | <0.001 |
| Screen time | 0.04 | (−0.02, 0.09) | 0.190 | 0.03 | (−0.02, 0.09) | 0.182 |
| Parent education | −0.05 | (−0.21, 0.11) | 0.517 | −0.03 | (−0.16, 0.10) | 0.633 |
| Worry | ||||||
| B | (95% CI) | p | ||||
| Time | ||||||
| Pre-COVID-19 (T1) | Ref. | |||||
| Lockdown (T2) | 0.45 | (0.30, 0.61) | <0.001 | |||
| Post-lockdown (T3) | −0.04 | (−0.21, 0.12) | 0.629 | |||
| Covariates | ||||||
| Sex (Female) | 0.22 | (-0.02, 0.47) | 0.072 | |||
| Age (per 5 years) | 0.15 | (0.01, 0.28) | 0.036 | |||
| Parent stress | 0.003 | (−0.002, 0.008) | 0.177 | |||
| Screen time | 0.06 | (0.01, 0.10) | 0.016 | |||
| Parent education | 0.04 | (−0.08, 0.17) | 0.491 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crowe, L.M.; Clarke, C.; Geraghty, D.; Collins, B.; Hearps, S.; Pugh, R.; Kilpatrick, N.; Branson, E.; Payne, J.M.; Haebich, K.; et al. Mental Health Impacts of the COVID-19 Pandemic on Australian Children and Adolescents with a Medical Condition: Longitudinal Findings. COVID 2025, 5, 10. https://doi.org/10.3390/covid5010010
Crowe LM, Clarke C, Geraghty D, Collins B, Hearps S, Pugh R, Kilpatrick N, Branson E, Payne JM, Haebich K, et al. Mental Health Impacts of the COVID-19 Pandemic on Australian Children and Adolescents with a Medical Condition: Longitudinal Findings. COVID. 2025; 5(1):10. https://doi.org/10.3390/covid5010010
Chicago/Turabian StyleCrowe, Louise M., Cathriona Clarke, Dan Geraghty, Ben Collins, Stephen Hearps, Remy Pugh, Nicola Kilpatrick, Emma Branson, Jonathan M. Payne, Kristina Haebich, and et al. 2025. "Mental Health Impacts of the COVID-19 Pandemic on Australian Children and Adolescents with a Medical Condition: Longitudinal Findings" COVID 5, no. 1: 10. https://doi.org/10.3390/covid5010010
APA StyleCrowe, L. M., Clarke, C., Geraghty, D., Collins, B., Hearps, S., Pugh, R., Kilpatrick, N., Branson, E., Payne, J. M., Haebich, K., McCloughan, N., Kintakas, C., Charles, G., Trajanovska, M., Hsieh, I., Hartmann, P. L., King, S., Anderson, N., & Anderson, V. (2025). Mental Health Impacts of the COVID-19 Pandemic on Australian Children and Adolescents with a Medical Condition: Longitudinal Findings. COVID, 5(1), 10. https://doi.org/10.3390/covid5010010