1. Introduction
The COVID-19 virus had affected countries all around the world and healthcare systems had to respond to exponentially increasing infection numbers [
1]. In general, the response of healthcare systems can be separated into three levels: National, Regional or Hospital Grouping Level, and Hospital Level [
2,
3,
4]. In this paper, the author’s aim is to give light to this last level of organizational changes. Being in the front line of the global “war” against COVID-19, hospitals had to make several institutional, strategic decisions to allocate extra capacity for treating COVID-19 patients, while solving the problem of maintaining outpatient care in other departments as well [
5,
6]. Each hospital had to adapt to the new situation in a limited amount of time, which meant there was huge pressure on institutional leaderships to tackle all kinds of operational, logistical, managerial, and strategic difficulties [
7].
Many publications in the current international literature provide alternative solutions to several challenges [
8,
9], while fewer publications concentrate on the leadership systems that hospitals implemented during the pandemic [
10]. This paper focuses on different management and leadership approaches. The discussion includes decision making, command and information distribution, and operative control. After overviewing the current international literature, we identified three different kinds of leadership structures that had been used “against” the virus.
With the Horizontal Approach, we present a position where hospitals maintained their pre-COVID-19 management structure and supplemented it with an additional function, that of COVID-19 care.
The Vertical Approach will regard situations where hospitals changed their organizational structure, and tried to structurally adapt to the crisis. These institutions centralized their leadership and operative control; their command and information distribution channels became vertical, and, therefore, hierarchical.
The third one is the Intermedier Approach, which essentially is a mixture of the Vertical and the Horizontal structures that uses ideas from both approaches.
At the second part of this review article, we introduce the strategic approach of one of Hungary’s largest centrum hospital’s used during the pandemic. The North-Buda Szent János Central Hospital had to transform their institution to a COVID-19 centrum hospital in the middle of the first wave; therefore, the leadership decided to implement a vertical, military-like command–control system to handle the crisis and to provide COVID-19 treatment for patients in different physical conditions.
2. Methodology
2.1. Horizontal Approach
In this chapter, we discuss a form of leadership response, where hospitals maintained their management structure and supplemented it with COVID-19 care, without reorganizing the institutional hierarchy. We would like to introduce a typical example of the aforementioned approach. The Bichat–Claude-Bernard Hospital [
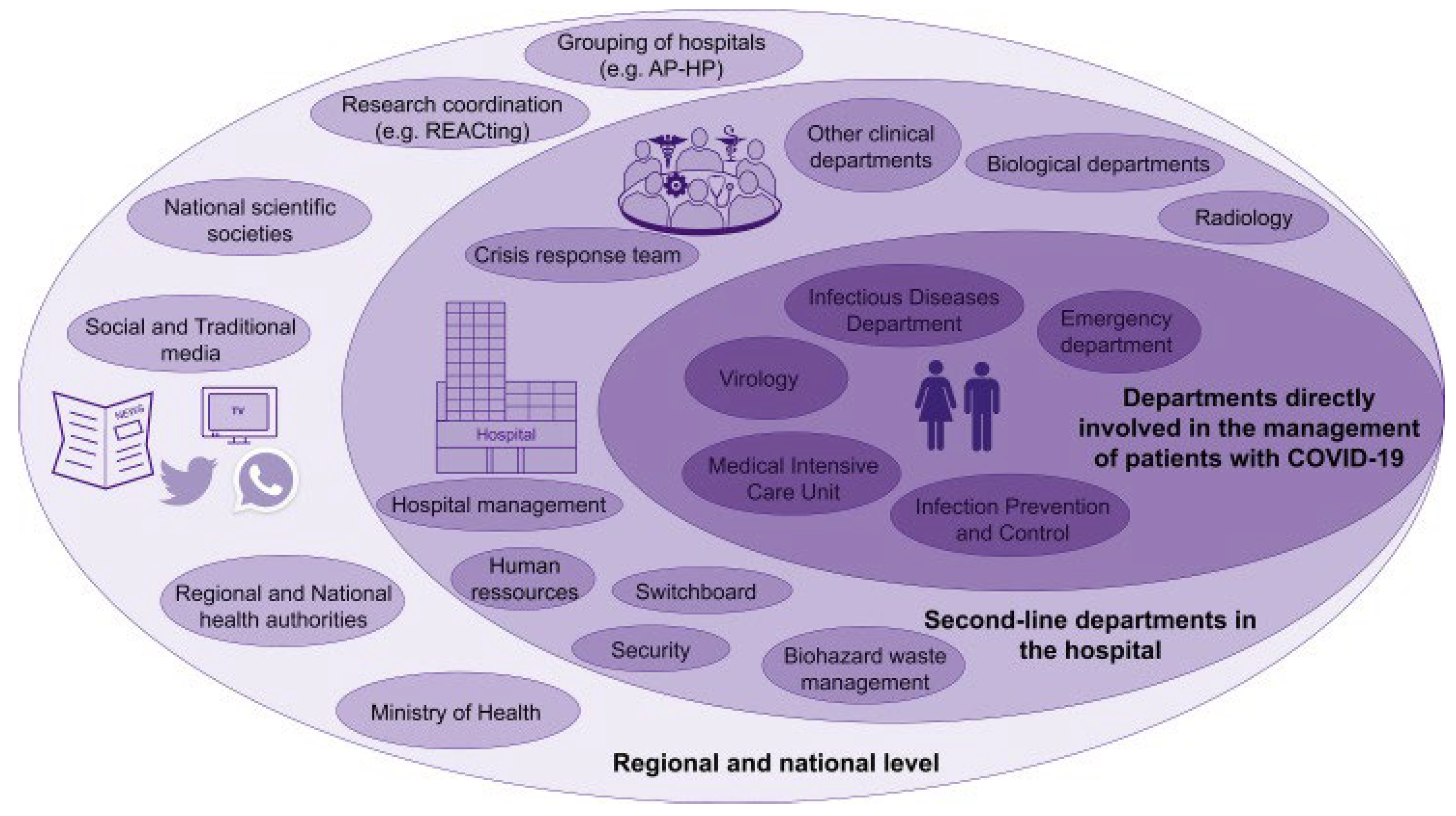
11] is a university hospital which has 1000 beds. The institution belongs to the biggest European hospital complex, the Assistance Publiquee Hôpitaux de Paris (AP-HP). As we can see in
Figure 1, three responsibility levels (lines) were defined in the institution. From our article’s point of view, the first two levels are the important ones; they show the hospital’s strategic levels.
In the first line are the departments directly involved in the management of COVID-19 patient care, including Virology, ID (Infectious Diseases Department), ED (Emergency Department), IPC (Infection Prevention Control), and the ICU (Intensive Care Unit). The second line is called “Second-Line Departments in Hospital”. This level is composed of Hospital Management, Human Resources, Switchboard, Security, Biohazard Waste Management, Biological Departments, Radiology, and Other Departments. On the same level, the leadership also created a multidisciplinary Crisis Response Team which supported decision making on pandemic response and updated the hospital on the current literature about the pandemic. In the Crisis Response Team, specialists were delegated from the IPC, ICU, and ID departments, and the hospital management also had a representative there. This team was co-working with the hospital management to boost the efficiency of decision making, and enhance the effectiveness of in-hospital communications. Biological Departments, Human Resources, Switchboard, and Security also belonged to that second line, supporting the care-giving departments. To ensure a “comprehensive and collective” crisis strategy, the hospital held regular crisis meetings, involving HCWs (Healthcare Workers), heads of departments, and administrative staff. We call this example horizontal: because the management structure is composed of three horizontal responsibility levels, information distribution does not have a hierarchical one-way route. Also, decision making is less centralized than in the Vertical Approach examples.
2.2. Vertical Approach
In this chapter, we introduce another aspect of management changes. As soon as the COVID-19 pandemic spread out, hospitals in this group had to change their leadership and communication structure and decided to restructure it as hierarchical and vertical. There are two typical ways of vertical implementation: the first is the Strict Military Approach, whilst the second is the Incidental Command System.
The military system [
12] relies on commander–subordinate relationships. The essence of this relationship is that the commander has the vision, sees the big picture, defines the aims, and communicates it in clear intentions to a subordinate. After the intent is conveyed, the subordinate has relative freedom regarding how they achieve the goals and how they combine different resources. At the end of the day, what matters is whether the goals are achieved. That makes decision making quick and centralized, and the execution effective and decentralized. In the next chapter we show a practical implementation of the military approach from Israel.
2.3. Strict Military Approach
Rambam Health Care Campus [
13] is a 1000-bed academic hospital serving the over-2 million residents of Northern Israel. The institution responded to the pandemic by first pre-defining intra-hospital communication groups, which were placed in a strict hierarchy to avoid communicational chaos and information loss. The medical teams of the hospital were inserted into those communication groups; all groups used the so-called Ex-TeamsTM communication and command platform, which was essentially a virtual cloud-based communication tool. This system allowed transmission roots to be cut as soon as possible, and the leadership could track the efforts of each department and was able to allocate resources accordingly.
Figure 2 presents the implemented structure.
On the top of the communication hierarchy stood the Hospital Level COVID-19 Control Center, which was in direct communication with the Department Level Control Centers (DLCC). The DLCC members were the departments’ head doctor, the head nurse, and a hospital management representative. Under the DLCC, in the communication hierarchy, stood the Patient Care Unit. This unit also had a head doctor and a head nurse who were in contact with the medical staff who were treating the COVID-19 patients.
To sum up, the hospital created a hierarchical communication system by implementing a piece of real-time cloud-based software and a strict set of rules for communicating orders and command forwarding. Decisions were based on real-time data collected by high-tech sensors and were processed by artificial intelligence overseen by political and military experts (National Mission Control Dashboard).
2.4. Incidental Command System
Incidental Command System (ICS) is officially defined as a “standardized approach to the command, control, and coordination of on-scene incident management that provides a common hierarchy within which personnel from multiple organizations can be effective” [
14]. This system is essentially a vertical command-forwarding structure, which provides operational information and commands from top to bottom as the hierarchy stands. ICSs are designed to organize responses to crisis situations and disease outbreaks (for example, SARS in Taiwan, H1N1 in Mexico) [
15,
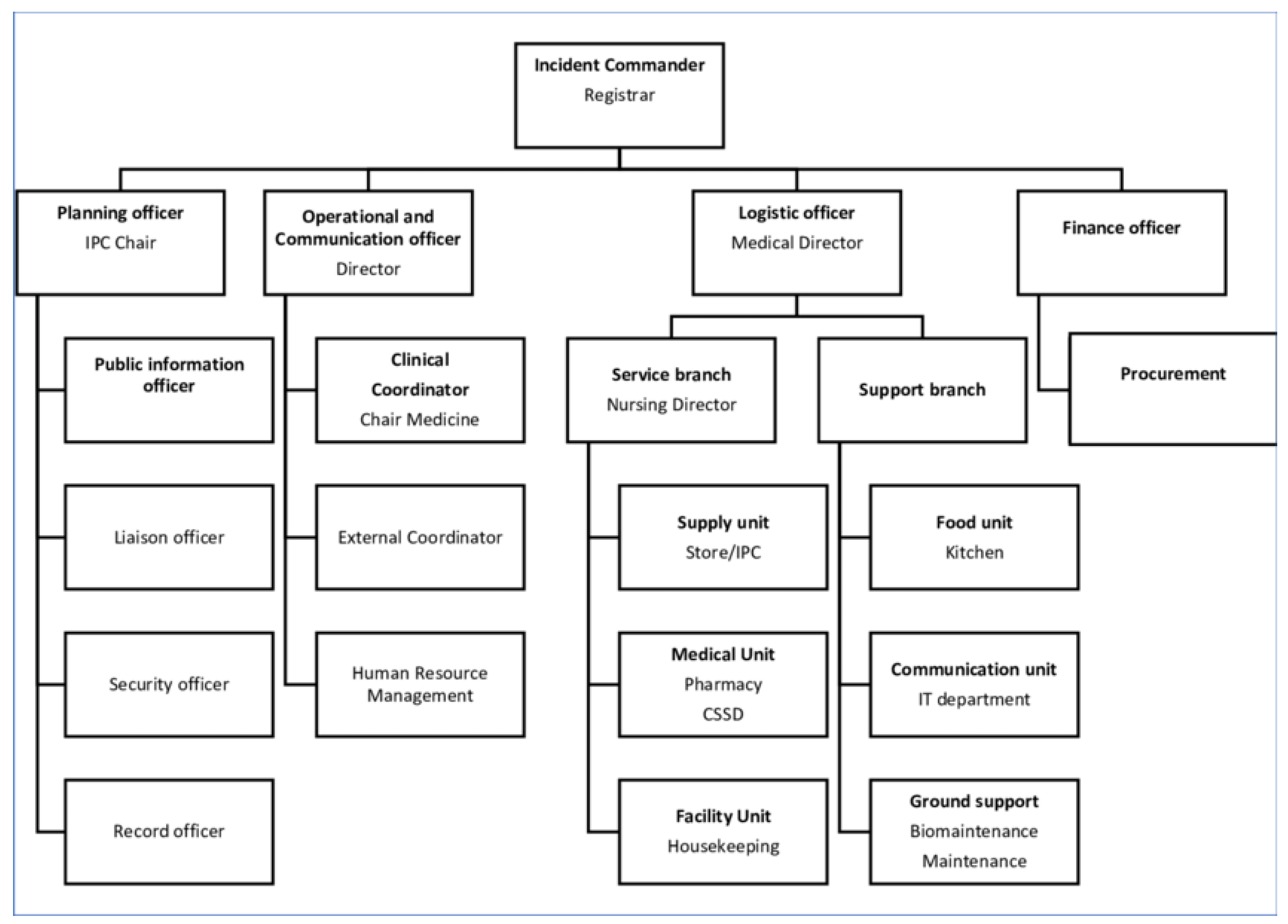
16]. To give an example of the visual structure of this system, we shortly discuss the implementation of a Hospital Incidental Command System (HICS) from a hospital in Nepal (
Figure 3).
The Patan Hospital is one of Nepal’s largest hospitals and operates as a teaching hospital for health sciences. The institution activated their ICS before the second wave of COVID-19 patients had been found in their region. As we can see in the picture, the incident commander is the head of the leadership. Under them, four different hierarchical branches provide planning, operational and communicational, logistical, and financial duties. The commands and aims are distributed in a strict top–down manner; the decision making is centralized as the incident commander’s duty is to make final decisions on pandemic response and operation [
17].
Additionally, we would like to mention that two prestigious hospitals, namely Stamford Hospital [
18] and Mayo Clinic [
19], also implemented the HICS and highlighted the following facts: HICSs were designed to tackle short term, local (or single-site) crisis situations. In the case of a Hospital Grouping over a longer time period (several month/years), the system must be personalized to the institutions and a separated Hospital Response Plan needs to be developed as well.
2.5. Intermedier Approach
In this chapter we introduce an example from China, where the leadership created a response system that was a structural novelty in their institution, but it was neither strictly vertical nor hierarchical; it converged more on the Horizontal Approach.
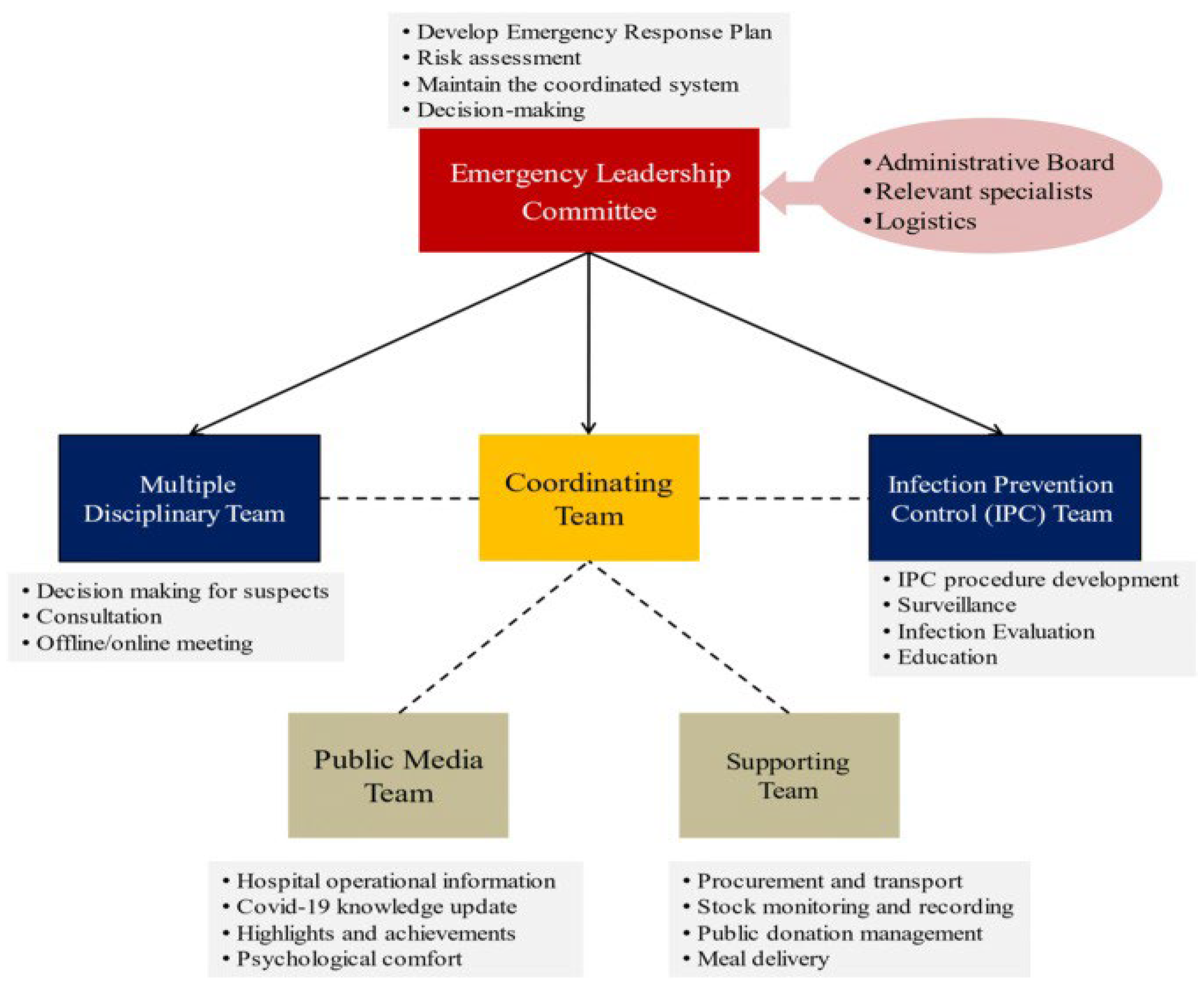
Zhongda Hospital, Southeast University [
20], is an academic and comprehensive regional medical center in Nanjing, Jiangsu Province, China. It is equipped with 2000 beds. As can be seen in
Figure 4, the institution established an Emergency Leadership Committee (ELC), created and oversaw their response plan, and also made strategic decisions. Below the ELC in the hierarchical branch, other coordinating and healthcare professional teams cooperated to tackle operative difficulties.
2.6. Summary of Main Characteristics
The Horizontal Approach is an organic response, where hospitals maintain their original management structure. These are decentralized structures, which promotes collaboration, autonomy, and information sharing across the organization. Decision making is based on discussions, and usually supported by a multidisciplinary team of healthcare workers. Communication channels are maintained; the COVID-19 care function is essentially added to the pre-COVID-19 operation.
The Vertical Approach is characterized by centralized decision making, strict predefined communication channels, and a reconstructed vertical hierarchy. Communication is based on forwarding commands and reporting in a clear, one-way route.
The Intermedier Approach example was a borderline solution to the crisis. The presented hospital established teams to tackle the new challenges. They assigned one team to lead the decision making, and other teams cooperated with each other. This solution used ideas from both the aforementioned approaches.
In general, organizations with a vertical structure and a strict hierarchy can adapt easily to quickly changing environments, like crisis situations, wars, or pandemics, while organizations with horizontal structures can operate more effectively in a complex and slowly changing environment [
21]. The theoretical main characteristics of the Vertical Approach and the Horizontal Approach are summed up in
Table 1.
3. Case Study—North-Buda Szent János Centrum Hospital and the COVID-19 Pandemic Challenge
In 2020, healthcare systems and hospitals were trying to devise a strategy to cope with a new, unknown epidemic [
22,
23]. The North-Buda Szent János Central Hospital (in Hungarian: Észak-budai Szent János Centrumkórház, hereafter referred to as “Szent János Hospital”) was given a priority assignment in the fight against the COVID-19 epidemic for a large part of Budapest and the neighboring regions.
In the spring of 2020, the hospital was tasked with creating and operating a COVID-19 unit. The Szent János Hospital had not had a similar function since WW2, and procedures and guidelines for such a situation were scant. In Budapest, a city of 2 million inhabitants, the Szent László Hospital had previously handled most infectious disease functions. The number of physicians and nursing staff available was limited. Our work was made more difficult by the fact that most of the organizational tasks had to be carried out while the unit was already in operation and gradually expanding. Meanwhile, the other functions of this large hospital also had to be maintained and other departments needed to be kept COVID-19-free.
3.1. Vertical Idea—Military Experience
The hospital had to react to external changes at short notice, so a rapid-response hospital strategy had to be developed for effective management. Only a system with a vertical structure, based on quick decisions and personal supervision, could compete with the ever-increasing number of infections in the middle of the first wave. Among the hospital’s assets, it is noteworthy that the person assigned to supervise the COVID-19 coordination tasks (the first author) had considerable military medical experience (in Afghanistan). In the following chapters, we would like to discuss our Hospital Response Strategy during the COVID-19 pandemic.
3.2. The 4+1 Basis of the Response Strategy
Precise and efficient patient distribution was the basis of the strategy. The distribution was provided by the occasionally set up Outpatient Clinic Triage Department. To enhance effectiveness, we organized a 4+1 level of care in our hospital, based on the protocol issued by the Hungarian Public Health Centre [
24]. Patients were sorted into different levels, considering their physical condition and characteristic symptoms (effort dyspnea, tachypnea, low oxygen saturation, chest pain, radiological abnormality). Patients in suspected/mild/moderate condition were assigned to the first level of care. The second level was for moderate–severe cases. This was followed by the third, severe level. Infected patients in critical condition requiring intensive therapy were assigned to the fourth level, in which mechanical ventilation took place. After categorizing the patients, each of them was transferred to one of the four departments that were assigned to acute COVID-19 patient care. The “level-based” distribution is going to be shown on the following graph. The hospital, as its own idea, created the “+1” Chronic COVID Department, where the treatment and rehabilitation of patients who had undergone the critical part of infection, and did not require acute care, took place. In the following chapters, we will describe the leadership, control, and operational management strategy that the hospital implemented. Another important part of the operation was that each patient’s condition was monitored day by day regarding whether they should have been transferred to another level of department based on their physical conditions.
3.3. Szent János Hospital’s Vertical Contro–Command System
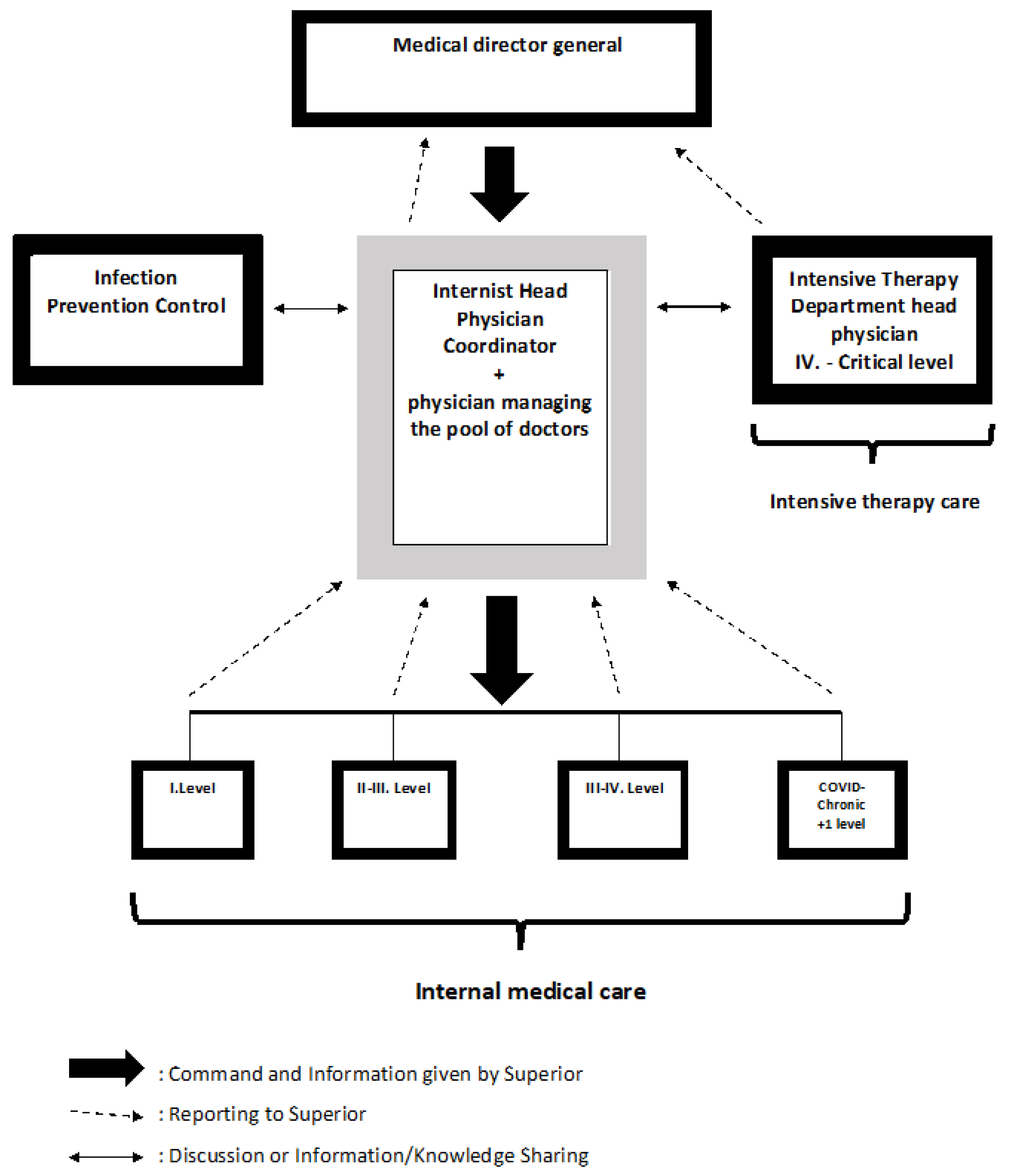
The basic idea was to build the central control vertically, where we could transmit commands in one direction and the reporting system could go the other way. With this hierarchically organized communication structure, we intended to ensure effective execution, precise control, and to minimize information loss. As can be seen in
Figure 5, the trunk of the organizational system is formed by the positions of the medical director general and Internist Head Physician Coordinator (IHCP). Under the direction of the leadership group were the heads of COVID-19 patient care sites, based on the 4+1 levels idea mentioned earlier. To complement the group laterally, Infection Prevention Control (IPC) and the Head Physician of the Intensive Therapy Department were also supporting the centralized decision making.
3.4. Command
Strategic decisions were made by the medical director general. He then issued the decision, in the form of a direct order, to the IHPC, who personally visited the various COVID-19 departments each morning where, after conducting the medical visit, he held a briefing on the director’s instructions in the presence of the designated heads and staff of departments. From that point onwards, the departments were responsible for the precise execution of orders, whether administrative, medical, or organizational.
3.5. Control
Personal supervision was considered important to control the precise execution of orders and the quality of care. This was also entrusted to the IHPC, who monitored the functioning of the wards, the number of doctors (Physician–Patient ratio), the quality of caregiving, the progression of patients’ conditions, and the hygienic protocol executions. Once the information was collected, the IHPC reported directly to the director, and these reports formed the basis for the decisions which followed. The IHCP also coordinated the Physician Pool, which was a centralized pool of physicians working in our hospital. The pool was established to relieve the department heads from the responsibility of human resource logistics.
3.6. Decision Making, Knowledge and Information Sharing
The medical director general was responsible for centralized decision making. In practice, the director made the institutional decisions alone, but he considered the options and processed the given information in cooperation with the head physician of the Intensive Therapy Department and the Internist Head Physician Coordinator, who were both experienced professionals in their specialties. They occasionally held meetings, where they could discuss certain changes in the pandemic situation, human resource management, operative difficulties and achievements, overview new protocols, and also could assess the risks of decision options. Besides these meetings, the IPC Department informed the IHCP about the pandemic statistics, hygiene protocol changes and the updated international literature on antiviral medication, infected condition progressions, and current patient care recommendations. With this centralized system, our hospital managed to have quick and effective responses to the new challenges in every wave.
4. Conclusions
All over the world, hospitals had to adapt to the previously unseen challenge of the COVID-19 epidemic [
25,
26,
27]. Overviewing the international literature, we identified three different strategic approaches to tackle the unseen challenges of the pandemic. We summarized the characteristic differences between the Horizontal and Vertical Approaches and presented an Intermedier example as well.
Then, we introduced our centrum hospital’s strategic response plan to the crisis in the middle of the first wave. Szent János Hospital found itself at the forefront of patient care in the fight against COVID-19 virtually overnight. As a result, it had to develop a care management system that it had not previously had.
In response to the various waves of the epidemic, we kept expanding the spectrum of our COVID-19 care and established a 4+1 level care system with unified oversight and management, and ongoing communication between the heads of the 4+1 care system, under the supervision of the Internist Head Physician Coordinator, the medical director, and the director general of the hospital. The established command–control system with personal operative control turned out to be effective.
Information sharing and discussions helped us to improve from our experiences to make the necessary changes in strategic response. The idea of a centralized doctor pool saved time and energy by reducing logistical challenges for department heads, so they could fully concentrate on patient care. With this vertical transformation of our previous management style and the aforementioned changes, we could keep control in our hands during each of the COVID-19 pandemic’s waves.
Author Contributions
Conceptualization, L.S., B.K., Z.L., J.T.K. and G.W.; Methodology, L.S., B.K., Z.L., J.T.K. and G.W.; Validation, L.S., B.K., Z.L., J.T.K. and G.W.; Investigation, Z.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
The study was conducted in accordance with the Declaration of Helsinki.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
Special thanks to Csaba Zsolt Horváth and András Lakatos for administrative and technical assistance. Their contributions have greatly improved the quality of this paper.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Haldane, V.; De Foo, C.; Abdalla, S.M.; Jung, A.-S.; Tan, M.; Wu, S.; Chua, A.; Verma, M.; Shrestha, P.; Singh, S.; et al. Health systems resilience in managing the COVID-19 pandemic: Lessons from 28 countries. Nat. Med. 2021, 27, 964–980. [Google Scholar] [CrossRef] [PubMed]
- Meessen, B.; Perazzi, S. The role of national hospital associations in health system governance before and during the COVID-19 pandemic: Findings from an exploratory online survey. Health Policy Open 2022, 3, 100077. [Google Scholar] [CrossRef] [PubMed]
- Mathews, K.S.; Seitz, K.P.; Vranas, K.C.; Duggal, A.; Valley, T.S.; Zhao, B.; Gundel, S.; Harhay, M.O.; Chang, S.Y.; Hough, C.L. National Heart, Lung, and Blood Institute Prevention and Early Treatment of Acute Lung Injury (PETAL) Clinical Trials Network. Variation in Initial U.S. Hospital Responses to the Coronavirus Disease 2019 Pandemic. Crit. Care Med. 2021, 49, 1038–1048. [Google Scholar] [CrossRef] [PubMed]
- Rajan, S.; McKee, M.; Hernández-Quevedo, C.; Karanikolos, M.; Richardson, E.; Webb, E.; Cylus, J. What have European countries done to prevent the spread of COVID-19? Lessons from the COVID-19 Health system response monitor. Health Policy 2022, 126, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.G.; Cheng, C.J.; Lii, E.; Mao, K.; Mesbahi, H.; Zhu, T.; Muckstadt, J.A.; Hupert, N. COVID-19 Models for Hospital Surge Capacity Planning: A Systematic Review. Disaster Med. Public Health Prep. 2020, 16, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Nicolás, D.; Coloma, E.; Pericàs, J.M. Alternatives to conventional hospitalisation that enhance health systems’ capacity to treat COVID-19. Lancet Infect. Dis. 2021, 21, 591–593. [Google Scholar] [CrossRef] [PubMed]
- Abdi, Z.; Lega, F.; Ebeid, N.; Ravaghi, H. Role of hospital leadership in combating the COVID-19 pandemic. Health Serv. Manag. Res. 2021, 35, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Winkelmann, J.; Webb, E.; Williams, G.A.; Hernández-Quevedo, C.; Maier, C.B.; Panteli, D. European countries’ responses in ensuring sufficient physical infrastructure and workforce capacity during the first COVID-19 wave. Health Policy 2022, 126, 362–372. [Google Scholar] [CrossRef]
- Davis, B.; Bankhead-Kendall, B.K.; Dumas, R.P. A review of COVID-19’s impact on modern medical systems from a health organization management perspective. Health Technol. 2022, 12, 815–824. [Google Scholar] [CrossRef] [PubMed]
- Hamis, A.A.; Md Bukhori, A.B.; Heng, P.P.; Jane Ling, M.Y.; Shaharuddin MA, A.; AFauzi NA, F.; Masdor, N.A.; Othman, R.; Ismail, A. Strategies, challenges and opportunities in the implementation of COVID-19 field hospitals: A scoping review. BMJ Open 2023, 13, e067227. [Google Scholar] [CrossRef]
- Peiffer-Smadja, N.; Lucet, J.C.; Bendjelloul, G.; Bouadma, L.; Gerard, S.; Choquet, C.; Jacques, S.; Khalil, A.; Maisani, P.; Casalino, E.; et al. Challenges and issues about organizing a hospital to respond to the COVID-19 outbreak: Experience from a French reference centre. Clin. Microbiol. Infect. 2020, 26, 669–672. [Google Scholar] [CrossRef] [PubMed]
- Pearce, A.P.; Naumann, D.N.; O’Reilly, D. Mission command: Applying principles of military leadership to the SARS-CoV-2 (COVID-19) crisis. BMJ Mil. Health 2020, 167, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Abbo, A.R.; Miller, A.; Gazit, T.; Savir, Y.; Caspi, O. Technological Developments and Strategic Management for Overcoming the COVID-19 Challenge within the Hospital Setting in Israel. Rambam Maimonides Med. J. 2020, 11, e0026. [Google Scholar] [CrossRef] [PubMed]
- Farcas, A.; Ko, J.; Chan, J.; Malik, S.; Nono, L.; Chiampas, G. Use of Incident Command System for Disaster Preparedness: A Model for an Emergency Department COVID-19 Response. Disaster Med. Public Health Prep. 2020, 15, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.C.; Arnold, J.L.; Chuang, C.C.; Chi, C.H.; Liu, C.C.; Yang, Y.J. Implementation of the Hospital Emergency Incident Command System during an outbreak of severe acute respiratory syndrome (SARS) at a hospital in Taiwan, ROC. J. Emerg. Med. 2005, 28, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Cruz, M.A.; Hawk, N.M.; Poulet, C.; Rovira, J.; Rouse, E.N. Public health incident management: Logistical and operational aspects of the 2009 initial outbreak of H1N1 influenza in Mexico. Am. J. Disaster Med. 2015, 10, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, S.; Rijal, S.; Acharya, P.K.; Sharma, B.P.; Ansari, I.; Rajbhandari, P.; Thapa, P. Hospital incident command system, the pillar of COVID-19 outbreak response: An experience from Patan Hospital, Nepal. J. Patan Acad. Health Sci. 2020, 7, 80–84. [Google Scholar] [CrossRef]
- Hartnett, J.; Houston, K.D.; Rose, S.J. Augmentation of a Hospital Incident Command System to Support Continued Waves of the COVID-19 Pandemic. J. Healthc. Leadersh. 2022, 14, 191–201. [Google Scholar] [CrossRef]
- Love, E.A.; Degen, S.C.; Craig, J.E.; Helmers, R.A. Activating the Hospital Incident Command System Response in a Community Specialty Practice: The Mayo Clinic Experience. WMJ Off. Publ. State Med. Soc. Wis. 2021, 120, 137–141. [Google Scholar]
- Shen, Y.; Cui, Y.; Li, N.; Tian, C.; Chen, M.; Zhang, Y.W.; Huang, Y.Z.; Chen, H.; Kong, Q.F.; Zhang, Q.; et al. Emergency Responses to COVID-19 Outbreak: Experiences and Lessons from a General Hospital in Nanjing, China. SSRN Electron. J. 2020, 43, 810–819. [Google Scholar] [CrossRef]
- Schaedler, L.; Graf-Vlachy, L.; König, A. Strategic leadership in organizational crises: A review and research agenda. Long Range Plan. 2022, 55, 102156. [Google Scholar] [CrossRef]
- Chopra, V.; Toner, E.; Waldhorn, R.; Washer, L. How Should U.S. Hospitals Prepare for Coronavirus Disease 2019 (COVID-19)? Ann. Intern. Med. 2020, 172, 621–622. [Google Scholar] [CrossRef] [PubMed]
- Azzolini, E.; Furia, G.; Cerquetani, F.; Speranza, F.; Chiaradia, S.; Marchianò, V.; Mainelli, M.T.; Vescia, M.; Zoppegno, A.; Quintili, M.; et al. COVID-19 emergency: From a general hospital to a covid hospital in one week, an Italian experience. Ann. Ig. Med. Prev. Comunita 2020, 34, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Szlávik, A. Koronavírus Megbetegedések Megelőzése, Hatékony Terápiás Lehetőségek, OHII Infektológiai Osztály, Dél-Pesti Centrumkórház. 2021. Available online: https://www.nnk.gov.hu/attachments/article/1284/Dr.%20Szlávik%20János.pdf (accessed on 8 April 2021).
- Whitwell, K.; Maynard, R.; Barry, N.; Cowling, V.; Sood, T. Strategic planning and response to COVID-19 in a London emergency department. Emerg. Med. J. 2020, 37, 567–570. [Google Scholar] [CrossRef] [PubMed]
- Pasin, L.; Sella, N.; Correale, C.; Boscolo, A.; Rosi, P.; Saia, M.; Mantoan, D.; Navalesi, P. Regional COVID-19 Network for Coordination of SARS-CoV-2 outbreak in Veneto, Italy. J. Cardiothorac. Vasc. Anesth. 2020, 34, 2341–2345. [Google Scholar] [CrossRef]
- Griffin, K.M.; Karas, M.G.; Ivascu, N.S.; Lief, L. Hospital Preparedness for COVID-19: A Practical Guide from a Critical Care Perspective. Am. J. Respir. Crit. Care Med. 2020, 201, 1337–1344. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}