
Prevalence and Levels of Anti-SARS-CoV-2 Antibodies in the Eswatini Population and Subsequent Severity of the Fourth COVID-19 Epidemic Wave

 , , , ,
, , , ,
Abstract
1. Background
2. Methods
2.1. Study Setting
2.2. Sample Collection and Processing
2.3. Sample Size and Sampling
2.4. Data Collection
2.5. Statistical Analyses
2.6. Ethics
3. Results
3.1. Participants
3.2. Seroprevalence
3.3. Calculated SARS-CoV-2 Infections
3.4. COVID-19 Fatality Rates
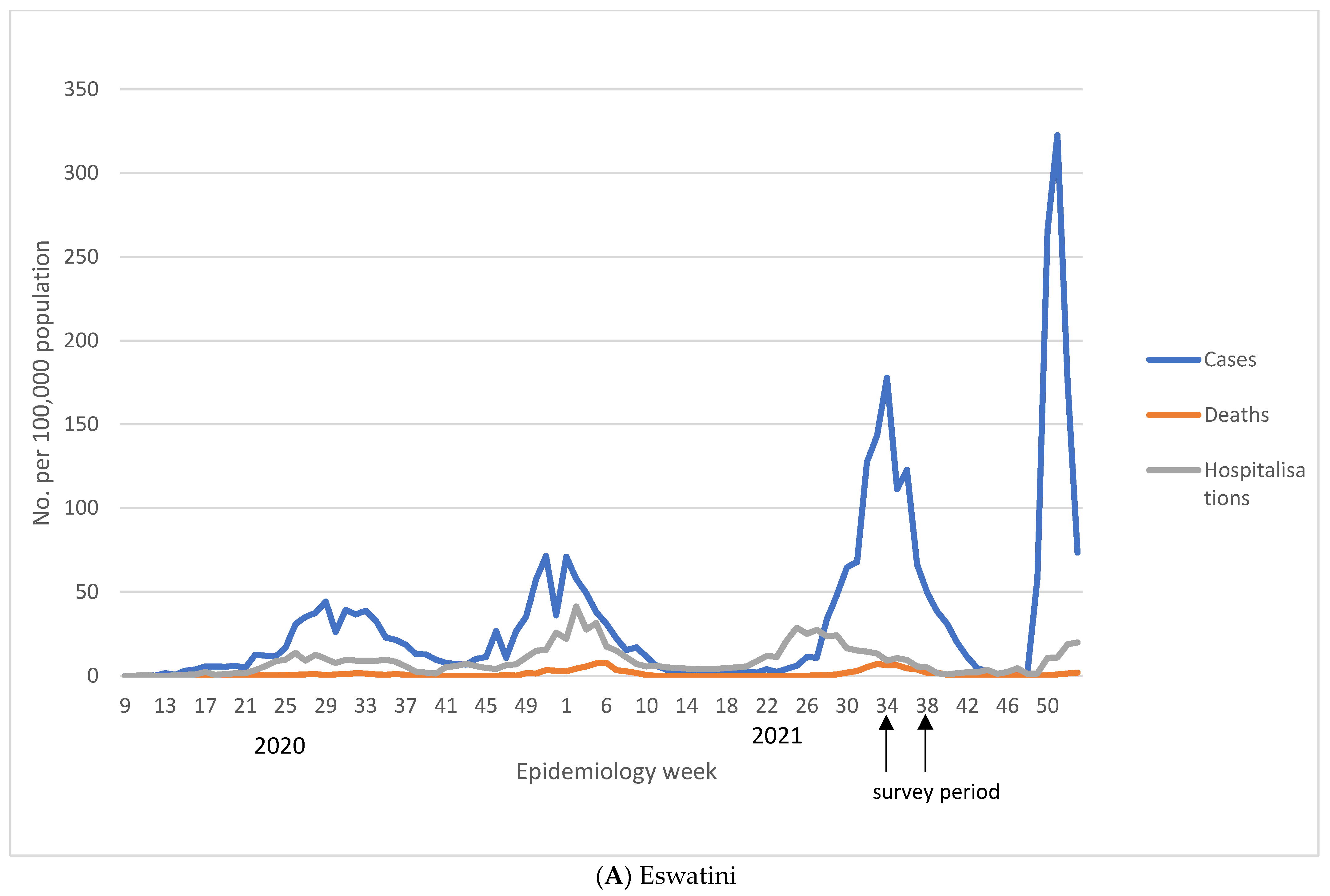
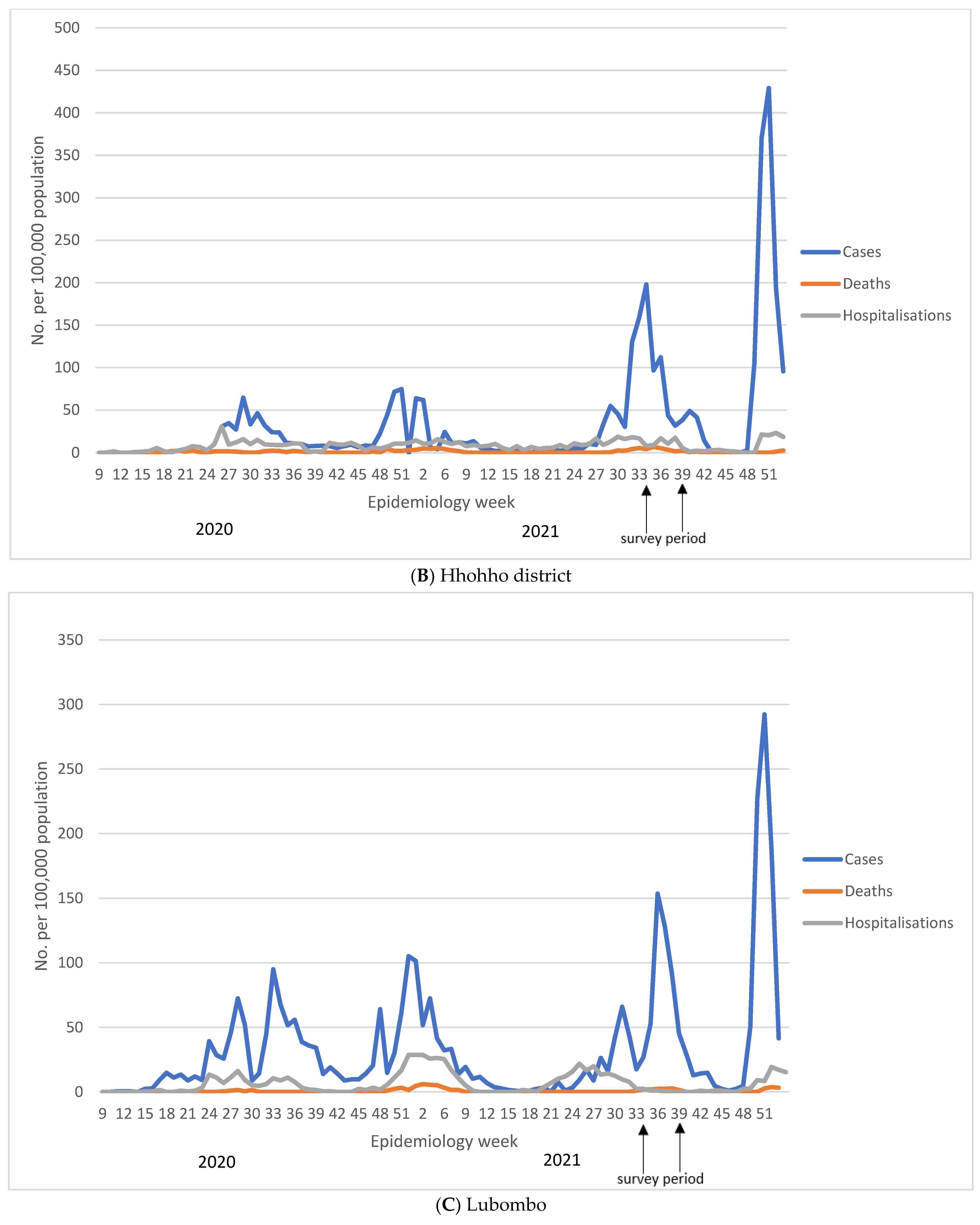
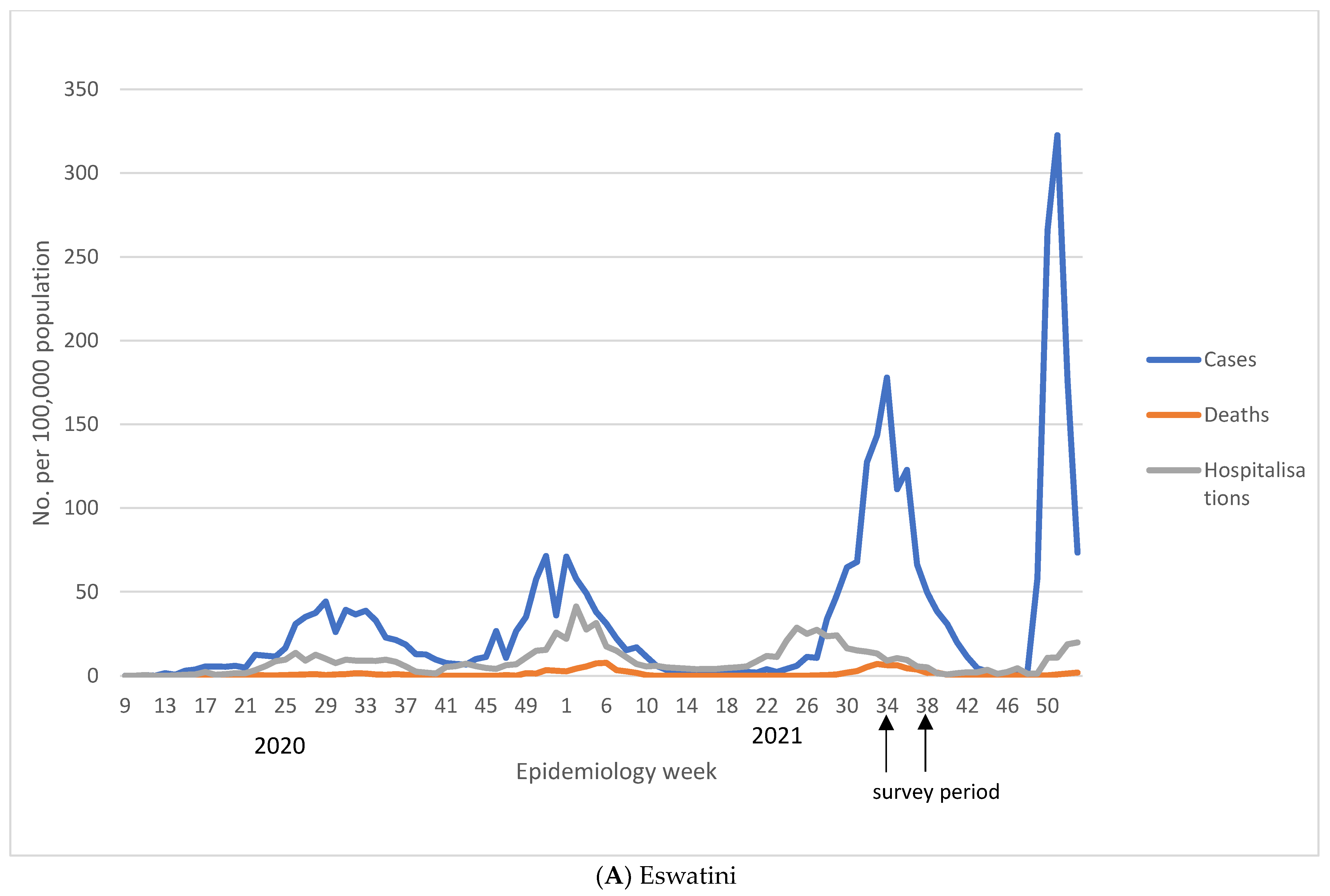
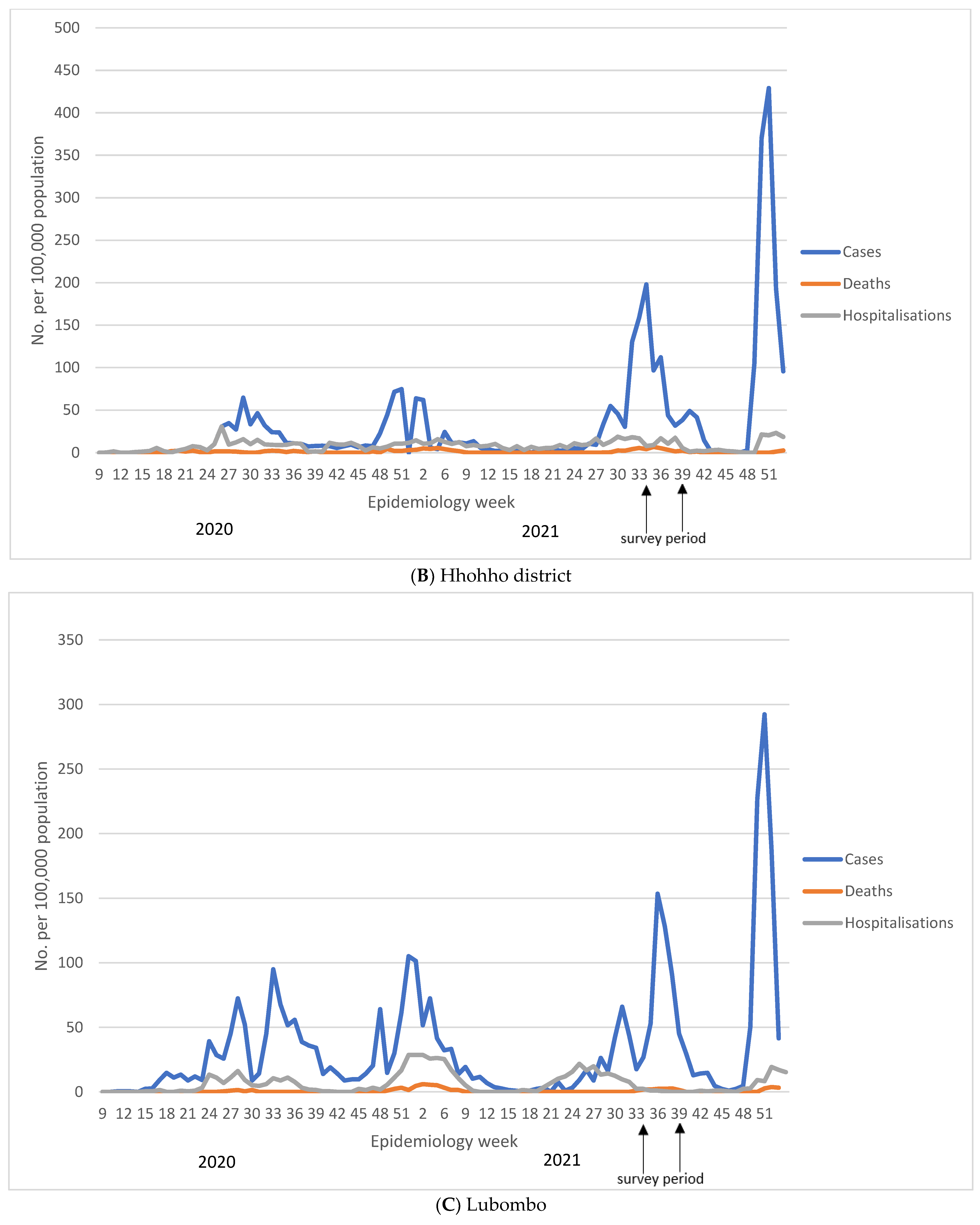
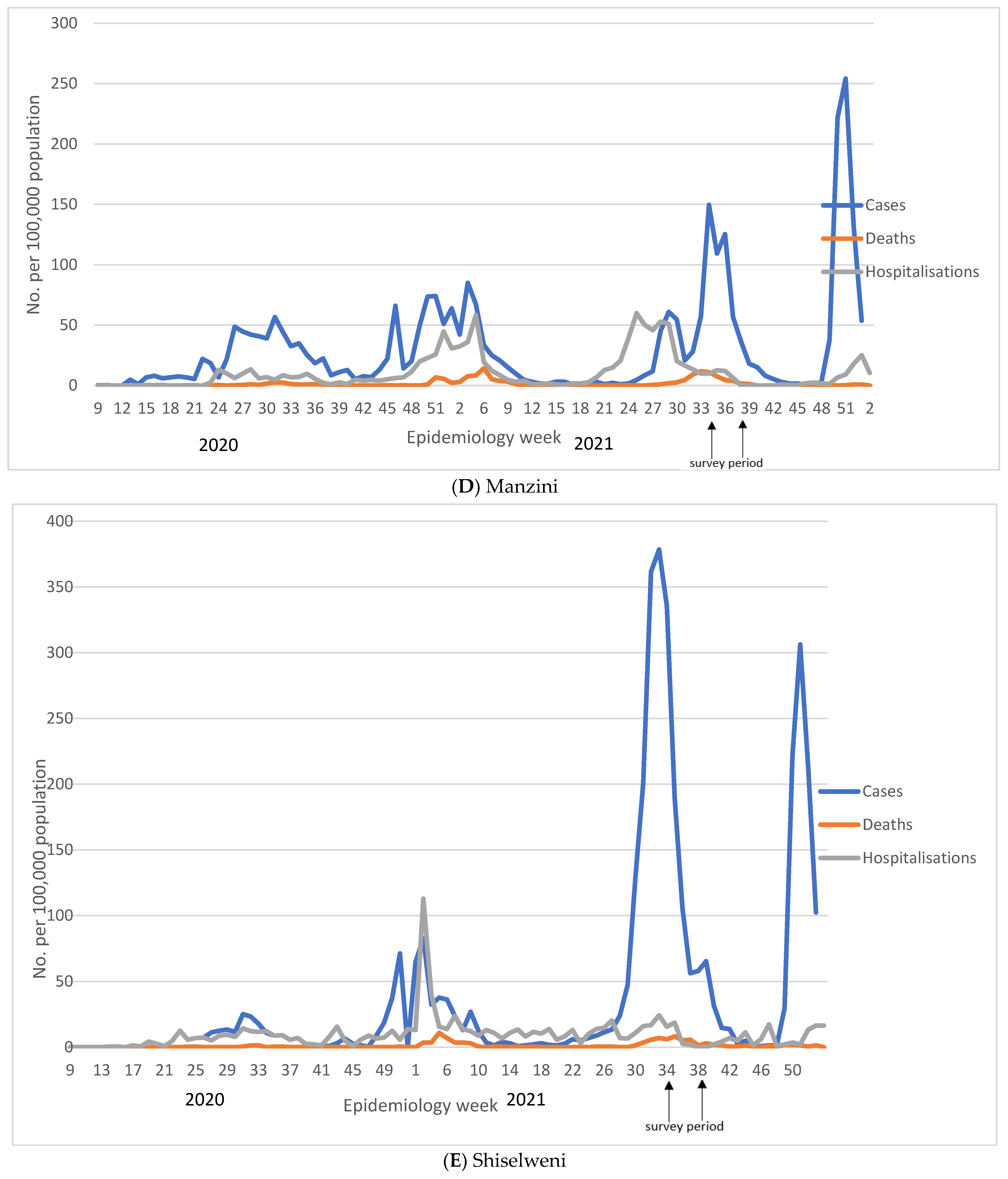
3.5. Decoupling of COVID-19 Cases, Hospitalizations, and Deaths
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Our World in Data. COVID-19 Data Explorer. Available online: https://ourworldindata.org/explorers/coronavirus-data-explorer2021 (accessed on 23 February 2022).
- Callaway, E. Heavily mutated Omicron variant puts scientists on alert. Nature 2021, 600, 21. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 23 February 2022).
- European Centre for Disease Prevention and Control. Implications of the Emergence and Spread of the SARS-CoV-2 B.1.1. 529 Variant of Concern (Omicron) for the EU/EEA; European Centre for Disease Prevention and Control: Solna, Sweden, 2021; Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Implications-emergence-spread-SARS-CoV-2%20B.1.1.529-variant-concern-Omicron-for-the-EU-EEA-Nov2021.pdf (accessed on 23 January 2022).
- UK Health Security Agency. SARS-CoV-2 Variants of Concern and Variants under Investigation in England. Technical Briefing 29; UK Health Security Agency: London, UK, 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1036501/Technical_Briefing_29_published_26_November_2021.pdf (accessed on 17 December 2021).
- Chen, J.; Wang, R.; Gilby, N.B.; Wei, G.W. Omicron Variant (B.1.1.529): Infectivity, Vaccine Breakthrough, and Antibody Resistance. J. Chem. Inf. Model. 2022, 62, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Office CS. The 2017 Population and Housing Census: The Kingdom of Swaziland. 2017. Available online: https://www.gov.sz/index.php/scholarship/124-economic-planning-a-development/2455-eswatini-census-documents (accessed on 7 June 2021).
- The World Bank in Eswatini. 2022. Available online: https://www.worldbank.org/en/country/eswatini/overview#1 (accessed on 23 February 2022).
- Corona Virus Disease (COVID-19) Situational Report. 2021. Available online: https://www.gov.sz/index.php/COVID-19-corona-virus/COVID-19-documents (accessed on 7 January 2022).
- Omicron-Fuelled COVID-19 Surge in Africa Plateaus. WHO Afro. 2022. Available online: https://www.afro.who.int/news/omicron-fuelled-COVID-19-surge-africa-plateaus (accessed on 15 March 2022).
- Kwatra, G.; Nunes, M.; Dhar, N.; Baillie, V.; Serafin, N.; Jones, S.; Madhi, S.A. Correlation of dried blood spots and plasma for quantification of Immunoglobulin (IgG) against Receptor binding domain and full length spike protein of SARS-CoV-2. J. Virol. Methods 2021, 300, 114394. [Google Scholar] [CrossRef] [PubMed]
- Madhi, S.A.; Kwatra, G.; Myers, J.E.; Jassat, W.; Dhar, N.; Mukendi, C.K.; Nana, A.J.; Blumberg, L.; Welch, R.; Ngorima-Mabhena, N.; et al. Population Immunity and COVID-19 Severity with Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 1314–1326. [Google Scholar] [CrossRef] [PubMed]
- Mutevedzi, P.C.; Kawonga, M.; Kwatra, G.; Moultrie, A.; Baillie, V.; Mabena, N.; Mathibe, M.N.; Rafuma, M.M.; Maposa, I.; Abbott, G.; et al. Estimated SARS-CoV-2 infection rate and fatality risk in Gauteng Province, South Africa: A population-based seroepidemiological survey. Int. J. Epidemiol. 2022, 51, 404–417. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Population-Based Age-Stratified Seroepidemiological Investigation Protocol for COVID-19 Virus Infection; WHO: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/331656 (accessed on 7 March 2021).
- Alemu, B.N.; Addissie, A.; Mamo, G.; Deyessa, N.; Abebe, T.; Abagero, A.; Ayele, W.; Abebe, W.; Haile, T.; Argaw, R.; et al. Sero-prevalence of anti-SARS-CoV-2 Antibodies in Addis Ababa, Ethiopia. Ethiop. J. Health Dev. 2021, 35, 367–374. [Google Scholar]
- Chen, X.; Chen, Z.; Azman, A.S.; Deng, X.; Sun, R.; Zhao, Z.; Zheng, N.; Chen, X.; Lu, W.; Zhuang, T.; et al. Serological evidence of human infection with SARS-CoV-2: A systematic review and meta-analysis. Lancet Glob. Health 2021, 9, e598–e609. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, M.; Davies, M.-A.; Kalk, E.; Hardie, D.; Naidoo, M.; Centner, C.; van Zyl, G.; Chapanduka, Z.; Opie, J.; Mahomed, J.; et al. SARS-CoV-2 Seroprevalence in the Cape Town Metropolitan Subdistricts after the Peak of Infections; COVID-19 Special Public Health Surveillance Bulletin; National Institute for Communicable Diseases: Johannesburg, South Africa, 2020; Volume 18, Available online: https://www.nicd.ac.za/wp-content/uploads/2020/09/COVID-19-Special-Public-Health-Surveillance-Bulletin_Issue-5.pdf (accessed on 23 February 2021).
- Majiya, H.; Aliyu-Paiko, M.; Balogu, V.T.; Musa, D.A.; Salihu, I.M.; Kawu, A.A.; Bashir, I.Y.; Sani, A.R.; Baba, J.; Muhammad, A.T.; et al. Seroprevalence of COVID-19 in Niger State. JMIRx Med. 2023, 4, e29587. [Google Scholar] [CrossRef] [PubMed]
- Rostami, A.; Sepidarkish, M.; Leeflang, M.M.G.; Riahi, S.M.; Shiadeh, M.N.; Esfandyari, S.; Mokdad, A.H.; Hotez, P.J.; Gasser, R.B. SARS-CoV-2 seroprevalence worldwide: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Arora, R.K.; Joseph, A.; Van Wyk, J.; Rocco, S.; Atmaja, A.; May, E.; Yan, T.; Bobrovitz, N.; Chevrier, J.; Cheng, M.P.; et al. SeroTracker: A global SARS-CoV-2 seroprevalence dashboard. Lancet Infect. Dis. 2021, 21, e75–e76. [Google Scholar] [CrossRef] [PubMed]
- Cohen, C.; Kleynhans, J.; von Gottberg, A.; McMorrow, M.L.; Wolter, N.; Bhiman, J.N.; Moyes, J.; du Plessis, M.; Carrim, M.; Buys, A.; et al. SARS-CoV-2 incidence, transmission, and reinfection in a rural and an urban setting: Results of the PHIRST-C cohort study, South Africa, 2020–21. Lancet Infect. Dis. 2022, 22, 821–834. [Google Scholar] [CrossRef] [PubMed]
- Wiens, K.E.; Mawien, P.N.; Rumunu, J.; Slater, D.; Jones, F.K.; Moheed, S.; Caflish, A.; Bior, B.K.; Jacob, I.A.; Lako, R.L.L.; et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Juba, South Sudan: A population-based study. medRxiv 2021. [Google Scholar] [CrossRef]
- Lewis, H.C.; Ware, H.; Whelan, M.; Subissi, L.; Li, Z.; Ma, X.; Nardone, A.; Valenciano, M.; Cheng, B.; Noel, K.; et al. SARS-CoV-2 infection in Africa: A systematic review and meta-analysis of standardised seroprevalence studies, from January 2020 to December 2021. BMJ Glob. Health 2022, 7, e008793. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Excess Mortality Collaborators. Estimating excess mortality due to the COVID-19 pandemic: A systematic analysis of COVID-19-related mortality, 2020–21. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef] [PubMed]
- Our World in Data. Excess Mortality during the Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/excess-mortality-covid2021 (accessed on 23 January 2022).
- Nishiura, H.; Ito, K.; Anzai, A.; Kobayashi, T.; Piantham, C.; Rodríguez-Morales, A.J. Relative Reproduction Number of SARS-CoV-2 Omicron (B.1.1.529) Compared with Delta Variant in South Africa. J. Clin. Med. 2021, 11, 30. [Google Scholar] [CrossRef] [PubMed]
- Pulliam, J.R.C.; Schalkwyk, C.; Govender, N.; von Gottberg, A.; Cohen, C.; Groome, M.J.; Dushoff, J.; Mlisana, K.; Moultrie, H. Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa. Science 2022, 376, 4947. [Google Scholar] [CrossRef] [PubMed]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef] [PubMed]
- Keeton, R.; Tincho, M.B.; Ngomti, A.; Baguma, R.; Benede, N.; Suzuki, A.; Khan, K.; Cele, S.; Bernstein, M.; Karim, F.; et al. SARS-CoV-2 spike T cell responses induced upon vaccination or infection remain robust against Omicron. medRxiv 2021. [Google Scholar] [CrossRef]
- Milne, G.; Hames, T.; Scotton, C.; Gent, N.; Johnsen, A.; Anderson, R.M.; Ward, T. Does infection with or vaccination against SARS-CoV-2 lead to lasting immunity? Lancet Respir. Med. 2021, 9, 1450–1466. [Google Scholar] [CrossRef]
- Tarke, A.; Coelho, C.H.; Zhang, Z.; Dan, J.M.; Yu, E.D.; Methot, N.; Bloom, N.I.; Goodwin, B.; Phillips, E.; Mallal, S.; et al. SARS-CoV-2 vaccination induces immunological T cell memory able to cross-recognize variants from Alpha to Omicron. Cell 2022, 185, 847–859. [Google Scholar] [CrossRef]
- Gronvall, G.; Connell, N.; Kobokovich, A.; West, R.; Lane Warmbrod, K.; Shearer, M.P.; Mullen, P.; Inglesby, T. Developing a National Strategy for Serology (Antibody Testing) in the United States; Johns Hopkins Bloomberg School of Public Health, Centre for Health Security: Baltimore, MD, USA, 2020. [Google Scholar]
- COVID-19 Surveillance Reports. 2022. Available online: https://www.nicd.ac.za/diseases-a-z-index/COVID-19/surveillance-reports/weekly-testing-summary (accessed on 1 June 2022).


{kind=link}
{kind=link}
{kind=link}
| Sub-Region | * Total Population | Overall Sample Size (%) | A Anti-N IgG; n (%); [95% CI] | B Anti-S IgG n (%); [95% CI] | C Overall Anti-N or Anti-S IgG n (%) [95% CI] | D Overall Anti-N or Anti-S IgG n; (%) [ 95% CI]—Unvaccinated | E Overall Anti-N or Anti-S IgG n; (%) [95% CI]—Vaccinated |
|---|---|---|---|---|---|---|---|
| Hhohho North | 150,801 | 711 (0.47) | 322 (45.3) [41.7–49.0] | 429 (60.3) [56.7–63.9] | 448 (63.0) [59.4–66.5] | 342/588 (58.2); [54.1–62.1] | 106/123 (86.2); [78.9–91.2] |
| Hhohho South | 187,083 | 648 (0.35) | 204 (31.5) [28.0–35.2] | 327 (50.5) [46.6–54.3] | 352 (54.3) [50.5–58.1] | 254/532 (47.7); [43.5–52.0] | 98/116 (84.5); [76.7–90.0] |
| Hhohho Region Total | 337,884 | 1359 (0.40) | 526 (38.7) [36.1–41.3] | 756 (55.6) [53.0–58.3] | 800 (58.9) [56.2–61.5] | 596/1120 (53.2); [50.3–56.1] | 204/239 (85.4); [80.3–89.3] |
| Lubombo North | 112,330 | 479 (0.43) | 159 (33.2) [29.1–37.5] | 243 (50.7) [46.3–55.2] | 257 (53.7) [49.2–58.1] | 176/378 (46.6); [41.6–51.6] | 81/101 (80.2); [71.3–86.9] |
| Lubombo South | 104,569 | 589 (0.56) | 248 (42.1) [38.2–46.1] | 363 (61.6) [57.6–65.5] | 376 (63.8) [59.9–67.6] | 284/484 (58.7); [54.2–63.0] | 92/105 (87.6); [79.8–92.7] |
| Lubombo Region Total | 216,899 | 1068 (0.49) | 407 (38.1) [35.2–41.1] | 606 (56.7) [53.7–59.7] | 633 (59.3) [56.3–62.2] | 460/862 (53.4); [50.0–56.7] | 173/206 (84.0); [78.3–88.4] |
| Manzini East | 248,446 | 587 (0.24) | 251 (42.8) [38.8–46.8] | 342 (58.3) [54.2–62.2] | 365 (62.2) [58.2–66.0] | 257/462 (55.6); [51.1–60.1] | 108/125 (86.4); [79.2–91.4] |
| Manzini West | 125,757 | 519 (0.41) | 262 (50.5) [46.2–54.8] | 346 (66.7) [62.5–70.6] | 356 (68.6) [64.5–72.4] | 259/406 (63.8); [59.0–68.3] | 97/113 (85.8); [78.1–91.1] |
| Manzini Region Total | 374,203 | 1106 (0.30) | 513 (46.4) [43.5–49.3] | 688 (62.2) [59.3–65.0] | 721 (65.2) [62.3–67.9] | 516/868 (59.4); [56.1–62.7] | 206/238 (86.1); [81.1–90.0] |
| Shiselweni North | 143,190 | 563 (0.39) | 257 (45.6) [41.6–49.8] | 313 (55.6) [51.5–59.7] | 333 (59.1) [55.0–63.1] | 261/473 (55.2); [50.7–59.6] | 72/90 (80.0); [70.5–87.0] |
| Shiselweni South | 87,970 | 468 (0.53) | 192 (41.0) [36.7–45.5] | 264 (56.4) [51.9–60.8] | 282 (60.3) [55.7–64.6] | 207/378 (54.8); [49.7–59.7] | 75/90 (83.3); [74.2–89.7] |
| Shiselweni Region Total | 231,160 | 1031 (0.45) | 449 (43.5) [40.6–46.6] | 577 (56.0) [52.9–59.0] | 615 (59.7) [56.6–62.6] | 468/851 (55.0); 5[1.6–58.3] | 147/180 (81.7); [75.3–86.7] |
| Eswatini National Total | 1,160,146 | 4564 (0.39) | 1895 (41.5) [40.1–43.0] | 2627 (57.6) [56.1–59.0] | 2769 (60.7) [59.2–62.1] | 2040/3701 (55.1); [53.5–56.7] | 729/863 (84.5); [81.9–86.7] |
| n (%) | Seroprevalence % n; (%) [95 CI] | uaIRR [95 CI] | aIRR [95 CI] | |
|---|---|---|---|---|
| Gender: Male | 1895 (41.5) | 1046 (55.2) [52.9–57.4] | Ref | |
| Female | 2669 (58.5) | 1723 (64.6) [62.7–66.3] | 1.17 [1.11–1.23] | 1.12 [1.06–1.18] |
| * Vaccination status: Unvaccinated | 3701 (81.1) | 2040 (55.1) [53.5–56.7] | Not evaluated | Not evaluated |
| Vaccinated | 863 (18.9) | 729 (84.5) [81.9–86.7] | ||
| Vaccination status by age: <5 years, unvaccinated | 671 (14.7) | 319 (47.5) [43.8–51.3] | 0.80 [0.73–0.87] | 0.75 [0.67–0.85] |
| 5–11 years, unvaccinated | 751 (16.5) | 366 (48.7) [45.2–52.3] | 0.82 [0.75–0.89] | 0.79 [0.72–0.87] |
| 12–17 years, unvaccinated | 534 (11.7) | 333 (62.4) [58.2–66.4] | 1.05 [0.97–1.13] | 1.00 |
| 18–50 years, unvaccinated | 1342 (29.4) | 799 (59.5) [56.9–62.1] | Ref | |
| 18–50 years, vaccinated | 300 (6.6) | 262 (87.3) [83.1–90.6] | 1.47 [1.38–1.56] | 1.40 [1.31–1.49] |
| 51–65 years, unvaccinated | 271 (5.9) | 161 (59.4) [53.5–65.1] | 1.00 [0.90–1.11] | 0.98 [0.88–1.09] |
| 51–65 years, vaccinated | 315 (6.9) | 267 (84.8) [80.4–88.3] | 1.42 [1.33–1.52] | 1.37 [1.28–1.47] |
| >65 years, unvaccinated | 132 (2.9) | 62 (47.0) [38.6–55.5] | 0.79 [0.65–0.95] | 0.80 [0.66–0.96] |
| >65 years, vaccinated | 248 (5.4) | 200 (80.7) [75.3–85.1] | 1.35 [1.26–1.46] | 1.35 [1.25–1.47] |
| Reported previous COVID-19 test: Never tested | 3813 (83.6) | 2210 (58.0) [56.4–59.5] | Ref | |
| Tested positive | 156 (3.4) | 146 (93.6) [88.5–96.5] | 1.61 [1.54–1.70] | 1.44 [1.36–1.53] |
| Tested negative | 595 (13.0) | 413 (69.4) [65.6–73.0] | 1.20 [1.13–1.27] | 1.04 [0.98–1.10] |
| ¥ Residential type: Formal stand-alone house | 2667 (58.5) | 1551 (58.2) [56.3–60.0] | Ref | |
| Informal or traditional dwelling | 1690 (37.1) | 1097 (64.9) [62.6–67.2] | 1.12 [1.06–1.17] | 1.00 [0.95–1.05] |
| Block of flats/high rise buildings | 204 (4.5) | 120 (58.8) [51.9–65.4] | 1.01 [0.90–1.14] | 0.94 [0.84–1.06] |
| Occupation: Unemployed | 2351 (51.5) | 1418 (60.3) [60.3; 58.3–62.3] | Ref | |
| Student | 1444 (31.6) | 789 (54.6) [52.1–57.2] | 0.91 [0.86–0.96] | 0.98 [0.91–1.06] |
| Formally employed | 541 (11.9) | 411 (76.0) [72.2–79.4] | 1.26 [1.19–1.33] | 1.12 [1.05–1.19] |
| Informally employed | 228 (5.0) | 151 (66.2) [59.8–72.1] | 1.10 [1.00–1.21] | 1.03 [0.93–1.13] |
| † Smoking: Smoker | 198 (4.3) | 100 (50.5) [43.6–57.4] | Ref | |
| Non-smoker | 4366 (95.7) | 2669 (61.6) [59.7–62.6] | 1.21 [1.05–1.39] | 1.21 [1.05–1.38] |
| Multiple morbidity: None | 1582 (34.7) | 1031 (65.2) [62.8–67.5] | Ref | |
| 1 or more | 1026 (22.5) | 720 (70.2) [67.3–72.9] | 1.08 [1.02–1.14] | 0.99 [0.94–1.05] |
| Under 18 years | 1956 (42.9) | 1018 (52.0) [49.8–54.3] | Not evaluated | |
| Region: Manzini | 1106 (24.2) | 721 (65.2) [62.3–67.9] | Ref | |
| Hhohho | 1359 (29.8) | 800 (58.9) [56.2–61.5] | 0.90 [0.85–0.96] | 0.92 [0.87–0.98] |
| Lubombo | 1068 (23.4) | 633 (59.3) [56.3–62.2] | 0.91 [0.85–0.97] | 0.93 [0.87–0.99] |
| Shiselweni | 1031 (22.6) | 615 (59.7) [56.6–62.6] | 0.92 [0.86–0.98] | 0.95 [0.89–1.01] |
| Sub-Region | n | A Seroprevalence | B Imputed SARS-CoV-2 Infections | C Imputed SARS-CoV-2 Infection Incidence Per 100,000 | D Documented COVID-19 Cases | E Documented COVID-19 Cases Per 100,000 |
|---|---|---|---|---|---|---|
| Hhohho North | 588 | 342 (58.2) [54.1–62.1] | 87,711 [81,628–93,633] | 58,163 [54,130–62,090] | 1202 | 797 |
| Hhohho South | 532 | 254 (47.7) [43.5–52.0] | 89,322 [81,428–97,276] | 47,744 [43,525–51,996] | 5083 | 2717 |
| Region Total | 1120 | 596 (53.2) [50.3–56.1] | 179,803 [169,900–189,631] | 53,214 [50,283–56,123] | 6285 | 1860 |
| Lubombo North | 378 | 176 (46.6) [41.6–51.6] | 52,302 [46,709–57,972] | 46,561 [41,582–51,609] | 3262 | 2904 |
| Lubombo South | 484 | 284 (58.7) [54.2–63.0] | 61,359 [56,710–65,864] | 58,678 [54,232–62,987] | 1531 | 1464 |
| Region Total | 862 | 460 (53.4) [50.0–56.7] | 115,747 [108,499–122,929] | 53,364 [50,023–56,676] | 4793 | 2210 |
| Manzini East | 462 | 257 (55.6) [51.1–60.1] | 138,205 [126,860–149,318] | 55,628 [51,062–60,101] | 6377 | 2567 |
| Manzini West | 406 | 259 (63.8) [59.0–68.3] | 80,224 [74,196–85,926] | 63,793 [58,999–68,327] | 1595 | 1268 |
| Region Total | 868 | 516 (59.4) [56.1–62.7] | 222,452 [210,086–234,507] | 59,447 [56,142–62,668] | 7972 | 2130 |
| Shiselweni North | 473 | 261 (55.2) [50.7–59.6] | 79,012 [72,549–85,354] | 55,180 [50,666–59,609] | 2127 | 1485 |
| Shiselweni South | 378 | 207 (54.8) [49.7–59.7] | 48,174 [43,731–52,532] | 54,762 [49,711–59,716] | 3871 | 4400 |
| Region Total | 851 | 468 (55.0) [51.6–58.3] | 127,124 [119,355–134,790] | 54,994 [51,633–58,310] | 5998 | 2595 |
| Eswatini | 3701 | 2040 (55.1) [53.5–56.7] | 639,475 [620,824–658,003] | 55,120 [53,513–56,717] | 25,048 | 2159 |
| Region | Sub-Region | Total Population Size | A COVID-19 | B Mortality Rate COVID-19 | C COVID-19 CFR COVID-19 | D Imputed IFR |
|---|---|---|---|---|---|---|
| Hhohho | Hhohho North | 150,801 | 150 | 99.5 | 12.5 | 0.17 [0.16–0.18] |
| Hhohho South | 187,083 | 215 | 114.9 | 4.2 | 0.24 [0.22–0.26] | |
| Region Total | 337,884 | 365 | 108.0 | 5.8 | 0.20 [0.19–0.21] | |
| Lubombo | Lubombo North | 112,330 | 64 | 57.0 | 2.0 | 0.12 [0.11–0.14] |
| Lubombo South | 104,569 | 48 | 45.9 | 3.1 | 0.08 [0.07–0.08] | |
| Region Total | 216,899 | 112 | 51.6 | 2.3 | 0.10 [0.09–0.10] | |
| Manzini | Manzini East | 248,446 | 381 | 153.4 | 6.0 | 0.28 [0.26–0.30] |
| Manzini West | 125,757 | 139 | 110.5 | 8.7 | 0.17 [0.16–0.19] | |
| Region Total | 374,203 | 520 | 139.0 | 6.5 | 0.23 [0.22–0.25] | |
| Shiselweni | Shiselweni North | 143,190 | 127 | 88.7 | 6.0 | 0.16 [0.15–0.18] |
| Shiselweni South | 87,970 | 75 | 85.3 | 1.9 | 0.16 [0.14–0.17] | |
| Region Total | 231,160 | 202 | 87.4 | 3.4 | 0.16 [0.15–0.17] | |
| National Total | Eswatini | 1,160,146 | 1199 | 103.3 | 4.8 | 0.19 [0.18–0.19] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mutevedzi, P.C.; Lokotfwako, V.; Kwatra, G.; Maphalala, G.; Baillie, V.; Dlamini, L.; Dlamini, S.; Mhlanga, F.; Dlamini, T.; Nhlabatsi, N.; et al. Prevalence and Levels of Anti-SARS-CoV-2 Antibodies in the Eswatini Population and Subsequent Severity of the Fourth COVID-19 Epidemic Wave. COVID 2024, 4, 317-333. https://doi.org/10.3390/covid4030021
Mutevedzi PC, Lokotfwako V, Kwatra G, Maphalala G, Baillie V, Dlamini L, Dlamini S, Mhlanga F, Dlamini T, Nhlabatsi N, et al. Prevalence and Levels of Anti-SARS-CoV-2 Antibodies in the Eswatini Population and Subsequent Severity of the Fourth COVID-19 Epidemic Wave. COVID. 2024; 4(3):317-333. https://doi.org/10.3390/covid4030021
Chicago/Turabian StyleMutevedzi, Portia C., Vusie Lokotfwako, Gaurav Kwatra, Gugu Maphalala, Vicky Baillie, Lindiwe Dlamini, Senzokuhle Dlamini, Fortune Mhlanga, Tenelisiwe Dlamini, Nhlanhla Nhlabatsi, and et al. 2024. "Prevalence and Levels of Anti-SARS-CoV-2 Antibodies in the Eswatini Population and Subsequent Severity of the Fourth COVID-19 Epidemic Wave" COVID 4, no. 3: 317-333. https://doi.org/10.3390/covid4030021
APA StyleMutevedzi, P. C., Lokotfwako, V., Kwatra, G., Maphalala, G., Baillie, V., Dlamini, L., Dlamini, S., Mhlanga, F., Dlamini, T., Nhlabatsi, N., Nunes, M. C., Zwane, S., & Madhi, S. A. (2024). Prevalence and Levels of Anti-SARS-CoV-2 Antibodies in the Eswatini Population and Subsequent Severity of the Fourth COVID-19 Epidemic Wave. COVID, 4(3), 317-333. https://doi.org/10.3390/covid4030021