
Favipiravir for COVID-19 Pneumonia: Effectiveness, Safety, and Clinical Outcomes: A Retrospective Single-Center Experience

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gralinski, L.E.; Menachery, V.D. Return of the Coronavirus: 2019-nCoV. Viruses 2020, 12, 135. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lai, C.; Shih, T.; Ko, W.; Tang, H.; Hsueh, P. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Saudi Ministry of Health. MOH Reports First Case of Coronavirus Infection. 2021. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-03-02-002.aspx (accessed on 2 January 2021).
- Barry, M.; Ghonem, L.; Alsharidi, A.; Alanazi, A.; Alotaibi, N.H.; Al-Shahrani, F.S.; Majid, F.; BaHammam, A. Coronavirus disease-2019 pandemic in the Kingdom of Saudi Arabia: Mitigation measures and hospital preparedness. J. Nat. Sci. Med. 2020, 3, 155. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Qomara, W.F.; Primanissa, D.N.; Amalia, S.H.; Purwadi, F.V.; Zakiyah, N. Effectiveness of Remdesivir, Lopinavir/Ritonavir, and Favipiravir for COVID-19 Treatment: A Systematic Review. Int. J. Gen. Med. 2021, 14, 8557–8571. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Joshi, S.; Vora, A.; Venugopal, K.; Dadhich, P.; Daxini, A.; Bhagat, S.; Patil, S.; Barkate, H. Real-World Experience with Favipiravir for the Treatment of Mild-to-Moderate COVID-19 in India. Pragmat. Obs. Res. 2022, 13, 33–41. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lowe, D.M.; Brown, L.K.; Chowdhury, K.; Davey, S.; Yee, P.; Ikeji, F.; Ndoutoumou, A.; Shah, D.; Lennon, A.; Rai, A.; et al. FLARE Investigators. Favipiravir, lopinavir-ritonavir, or combination therapy (FLARE): A randomised, double-blind, 2 × 2 factorial placebo-controlled trial of early antiviral therapy in COVID-19. PLoS Med. 2022, 19, e1004120. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mallah, S.I.; Ghorab, O.K.; Al-Salmi, S.; Abdellatif, O.S.; Tharmaratnam, T.; Iskandar, M.A.; Sefen, J.A.N.; Sidhu, P.; Atallah, B.; El-Lababidi, R.; et al. COVID-19: Breaking down a global health crisis. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 35. [Google Scholar] [CrossRef]
- Hung, D.T.; Ghula, S.; Aziz, J.M.A.; Makram, A.M.; Tawfik, G.M.; Abozaid, A.A.-F.; Pancharatnam, R.A.; Ibrahim, A.M.; Shabouk, M.B.; Turnage, M.; et al. The efficacy and adverse effects of favipiravir on patients with COVID-19: A systematic review and meta-analysis of published clinical trials and observational studies. Int. J. Infect. Dis. 2022, 120, 217–227. [Google Scholar] [CrossRef]
- Liu, K.; Chen, Y.; Lin, R.; Han, K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J. Infect. 2020, 80, e14–e18. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Pisaturo, M.; Zollo, V.; Martini, S.; Maggi, P.; Numis, F.G.; Gentile, I.; Sangiovanni, N.; Rossomando, A.M.; Bianco, V.; et al. Obesity as a Risk Factor of Severe Outcome of COVID-19: A Pair-Matched 1:2 Case-Control Study. J. Clin. Med. 2023, 12, 4055. [Google Scholar] [CrossRef] [PubMed]
- Abid, A.; Umar, A.; Qamar, S. Disease Outcomes of COVID-19 in Diabetic and Hypertensive Patients During the Hospital Stay. Cureus 2023, 15, e46943. [Google Scholar] [CrossRef] [PubMed]
- Tavakolifard, N.; Moeini, M.; Haddadpoor, A.; Heidari, K.; Rezaee, M.; Amini, Z. Clinical Symptoms of COVID-19 and Their Association with Disease Outcome. Adv. Biomed. Res. 2022, 11, 2. [Google Scholar] [CrossRef]
- Fernandes, M.; Brábek, J. COVID-19, corticosteroids and public health: A reappraisal. Public Health 2021, 197, 48–55. [Google Scholar] [CrossRef]
- Trofin, F.; Nastase, E.V.; Roșu, M.F.; Bădescu, A.C.; Buzilă, E.R.; Miftode, E.G.; Manciuc, D.C.; Dorneanu, O.S. Inflammatory Response in COVID-19 Depending on the Severity of the Disease and the Vaccination Status. Int. J. Mol. Sci. 2023, 24, 8550. [Google Scholar] [CrossRef]
- Luan, Y.Y.; Yin, C.H.; Yao, Y.M. Update Advances on C-Reactive Protein in COVID-19 and Other Viral Infections. Front. Immunol. 2021, 12, 720363. [Google Scholar] [CrossRef]
- Rajendran, V.; Gopalan, S.; Varadaraj, P.; Pandurangan, V.; Marappa, L.; Nair, A.M.; Madhavan, S.; Mani, R.; Bhaskar, E. Course of COVID-19 Based on Admission D-Dimer Levels and Its Influence on Thrombosis and Mortality. J. Clin. Med. Res. 2021, 13, 403–408. [Google Scholar] [CrossRef]
- Nakayama, R.; Bunya, N.; Tagami, T.; Hayakawa, M.; Yamakawa, K.; Endo, A.; Ogura, T.; Hirayama, A.; Yasunaga, H.; Uemura, S.; et al. Associated organs and system with COVID-19 death with information of organ support: A multicenter observational study. BMC Infect. Dis. 2023, 23, 814. [Google Scholar] [CrossRef]
- Karimi Shahri, M.; Niazkar, H.R.; Rad, F. COVID-19 and hematology findings based on the current evidences: A puzzle with many missing pieces. Int. J. Lab. Hematol. 2021, 43, 160–168. [Google Scholar] [CrossRef]
- Li, G.; Xu, F.; Yin, X.; Wu, N.; Li, Y.; Zhang, T.; Chen, D.; Liu, K.; Qiu, Q. Lactic dehydrogenase-lymphocyte ratio for predicting prognosis of severe COVID-19. Medicine 2021, 100, e24441. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.Y. Mortality Rate of Patients with COVID-19 Based on Underlying Health Conditions. Disaster Med. Public Health Prep. 2021, 16, 2480–2485. [Google Scholar] [CrossRef] [PubMed]
- Hassanipour, S.; Arab-Zozani, M.; Amani, B.; Heidarzad, F.; Fathalipour, M.; Martinez-De-Hoyo, R. The efficacy and safety of Favipiravir in treatment of COVID-19: A systematic review and meta-analysis of clinical trials. Sci. Rep. 2021, 11, 11022. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency, N (%) | ||
|---|---|---|
| Gender | Female | 129 (43.4%) |
| Male | 165 (55.6%) | |
| Age | Mean (SD) | 61.47 (16.8) |
| Range | 23–106 | |
| BMI (Kg/m2) | Mean (SD) | 31.15 (7.4) |
| Range | 20.7–56.0 | |
| Smoking History | No | 277 (93.3%) |
| Yes | 6 (2.0%) | |
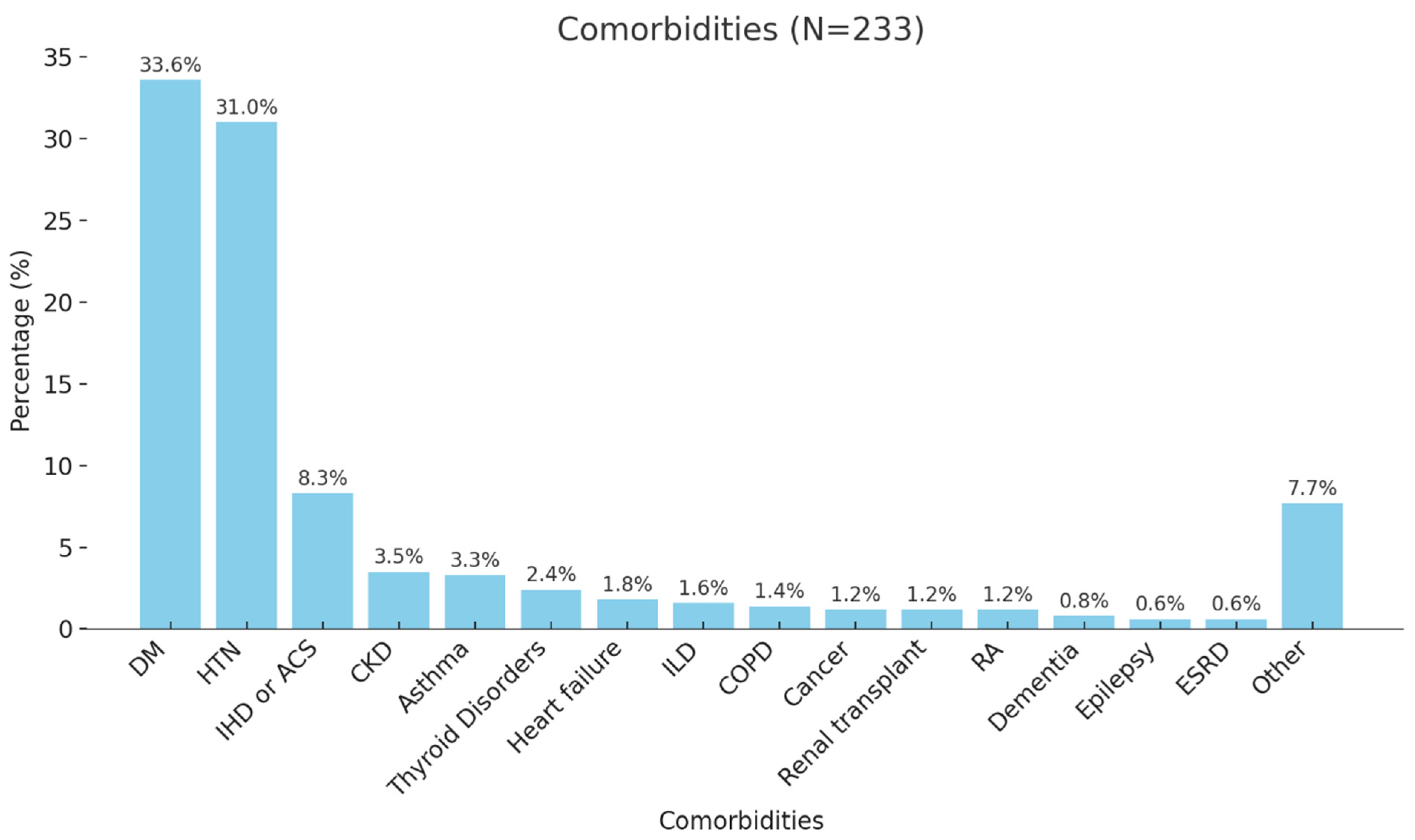
| Comorbidities | No | 73 (24.6%) |
| Yes | 223 (75.1%) | |
| Non-COVID-19-related | ACEI/ARB | 23 (7.7%) |
| Anticoagulants | 77 (25.9%) | |
| Antidiabetics | 137 (46.1%) | |
| Antiplatelets | 2 (0.7%) | |
| Betablockers | 11 (3.7%) | |
| CCB | 7 (2.4%) | |
| Diuretics | 4 (1.3%) | |
| Statins | 14 (4.7%) | |
| Thyroxin Drugs | 2 (0.7%) | |
| Days of Favipiravir Use | Mean (SD) | 8.3 (21.6) |
| Antibiotics | Carbapenems | 16 (5.4%) |
| Cephalosporin | 104 (35.0%) | |
| Fluoroquinolones | 22 (7.4%) | |
| Macrolides | 129 (43.4%) | |
| Penicillins | 3 (1.0%) | |
| Tetracyclines | 13 (4.4%) | |
| Corticosteroids | Long-acting | 224 (75.4%) |
| Short-acting | 11 (3.7%) | |
| Mean (SD) | Range (Min–Max) | |
|---|---|---|
| CBC | ||
| Hemoglobin (Hb) (g/dL) | 14.29 (6.17) | 7.50–112.00 |
| White blood cell (WBC) count (109/L) | 6.51 (3.37) | 1.90–22.78 |
| Platelet count (109/L) | 219.96 (82.67) | 52.00–656.00 |
| Erythrocyte sedimentation rate (ESR) (mm/h) | 70.31 (29.86) | 6.00–120.00 |
| LFTs | ||
| Alanine aminotransferase (ALT) (U/L) | 32.58 (22.82) | 6.00–160.00 |
| Aspartate aminotransferase (AST) (U/L) | 42.89 (25.49) | 13.00–204.00 |
| Alkaline phosphatase(ALP) (U/L) | 70.42 (35.08) | 28.0–263.0 |
| Gamma-glutamyl transferase (GGT) (U/L) | 51.29 (59.36) | 8.0–516.0 |
| Total bilirubin (µmol/L) | 14.46 (18.20) | 0.4–292.3 |
| Direct bilirubin (µmol/L) | 4.44 (10.41) | 0.1–170.1 |
| RFTs | ||
| Creatinine (µmol/L) | 100.16 (63.26) | 37–581 |
| Urea (mmol/L) | 7.32 (5.06) | 2–36 |
| Serum Profile | ||
| Sodium (mmol/L) | 133.57 (4.67) | 116.00–161.00 |
| Potassium (mmol/L) | 4.21 (0.58) | 3–7 |
| Corrected calcium (mmol/L) | 3.11 (13.96) | 1.89–232 |
| Phosphorus (mmol/L) | 1.22 (3.20) | 0.49–53 |
| Magnesium (mmol/L) | 0.78 (0.10) | 0.52–1.26 |
| Other | ||
| D-Dimer (mg/L) | 3.18 (27.42) | 0.19–455.00 |
| Ferritin (ng/mL) | 439.41 (598.67) | 6.90–4454.00 |
| C-reactive protein (CRP)(mg/L) | 72.11 (55.62) | 5.0–345.2 |
| Lactic acid dehydrogenase (LDH)(U/L) | 302.63 (137.85) | 98.00–1411.00 |
| FiO2 | 80.25 (18.66) | 0–100 |
| Hematocrit (%) | 42.82 (6.17) | 23.2–59.5 |
| Temperature (°C) | 38.75 (21.05) | 23.9–373.0 |
| Heart rate | 96.46 (17.35) | 54.0–196.0 |
| Respiratory rate | 20.51 (1.45) | 17.0–28.0 |
| Mean arterial pressure (MAP) | 88.50 (11.05) | 64.0–118.0 |
| Frequency N (%) | ||
|---|---|---|
| Microbiology and Imaging | ||
| Blood Culture | Negative | 200 (67.3%) |
| Positive | 26 (8.8%) | |
| Common Pathogen Class (Staphylococcus) | 13 (4.4%) | |
| Urine Culture | Negative | 168 (56.6%) |
| Positive | 15 (5.1%) | |
| Commonly Mixed Growth | 5 (1.5%) | |
| Sputum Culture | Negative | 112 (37.7%) |
| Positive (WBCs and Mixed Bacteria) | 8 (2.7%) | |
| Tracheal Culture | Negative | 84 (28.3%) |
| Positive (WBCs and Mixed Bacteria) | 9 (3.0%) | |
| CT Findings | No CT Performed | 232 (78.1%) |
| Normal | 10 (3.4%) | |
| Consolidation | 27 (9.1%) | |
| Ground Glass | 15 (5.1%) | |
| Pleural Effusion | 6 (2.0%) | |
| Other | 4 (1.3%) | |
| Length of Stay | ||
| Length of Hospital Stay (Days) | Mean (SD) | 6.17 (4.89) |
| Range | 1–20 | |
| Length of ICU Stay (Days) | Mean (SD) | 22.00 (37.52) |
| Range | 3–89 | |
| Outcome and Complications | ||
| Needed Intubation | No | 220 (74.1%) |
| Yes | 65 (21.9%) | |
| Acute respiratory distress syndrome (ARDS) | No | 241 (81.1%) |
| Yes | 40 (13.5%) | |
| Complication | No Complications | 244 (82.2%) |
| ACS | 3 (1.0%) | |
| AKI | 15 (5.1%) | |
| ARDS | 4 (1.3%) | |
| Cardiac Arrest | 8 (2.7%) | |
| CVA | 9 (3.0%) | |
| Liver Failure/Heart Failure | 5 (1.7%) | |
| Pulmonary Embolism (PE) | 9 (3.0%) | |
| Survival | Dead | 62 (20.9%) |
| Alive | 232 (78.1%) | |
| Readmission | Within 15 Days | 96 (32.3%) |
| Within 30 Days | 9 (3.0%) | |
| Within 60 Days | 14 (4.7%) | |
| Within 90 Days | 4 (1.3%) | |
| Overall Outcome/Survival | Sig. Value | |||
|---|---|---|---|---|
| Dead, N (%) | Alive, N (%) | |||
| Gender | Female | 24 (18.8%) | 104 (81.3%) | 0.374 a |
| Male | 38 (23.0%) | 127 (77.0%) | ||
| Age (Year) | Mean (SD) | 70.82 (16.62) | 58.87 (16.02) | <0.001 c |
| BMI (Kg/m2) | Mean (SD) | 29.38 (9.08) | 31.60 (7.15) | 0.273 c |
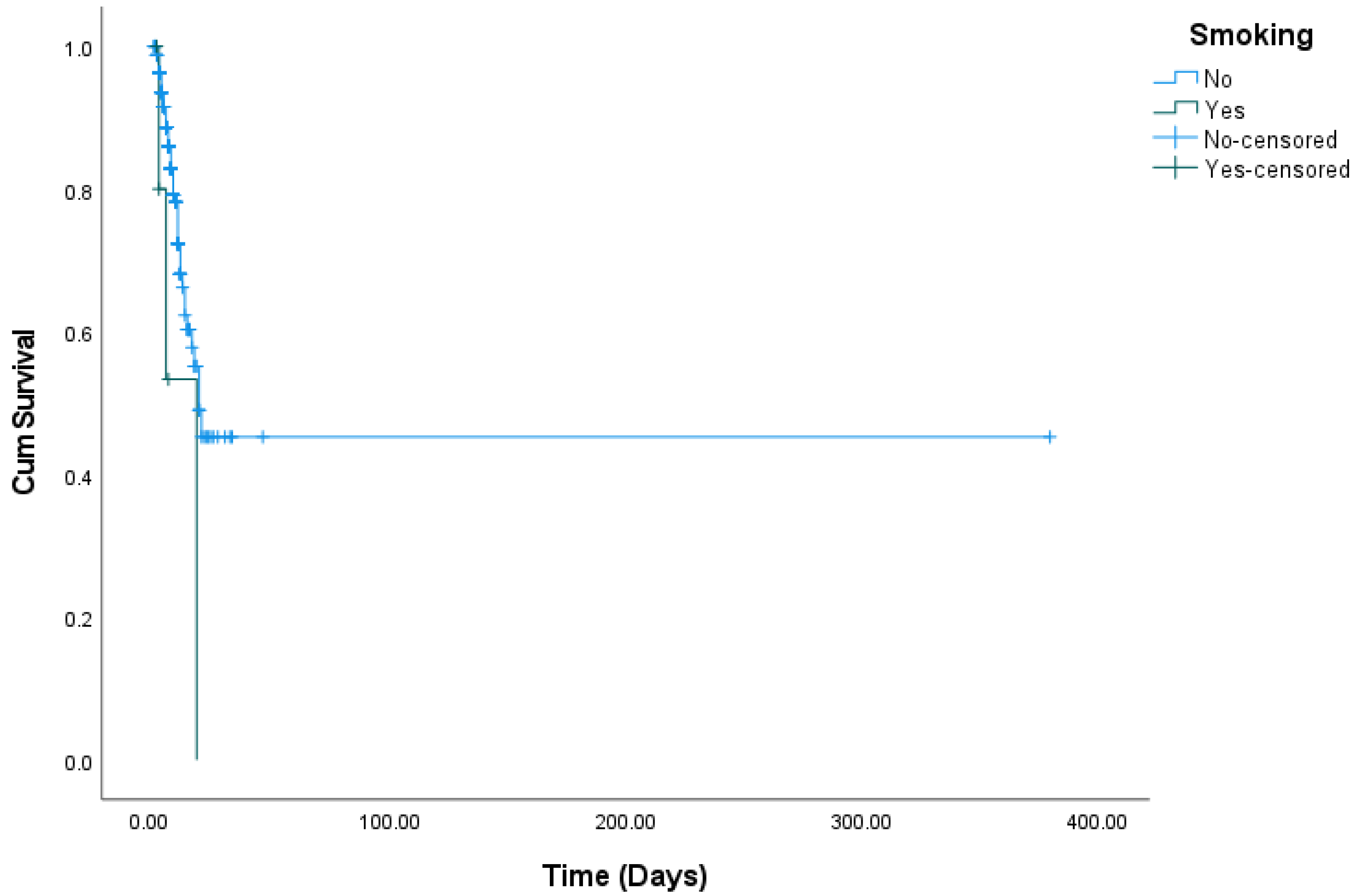
| Smoking | No | 56 (20.3%) | 220 (79.7%) | 0.108 b |
| Yes | 3 (50.0%) | 3 (50.0%) | ||
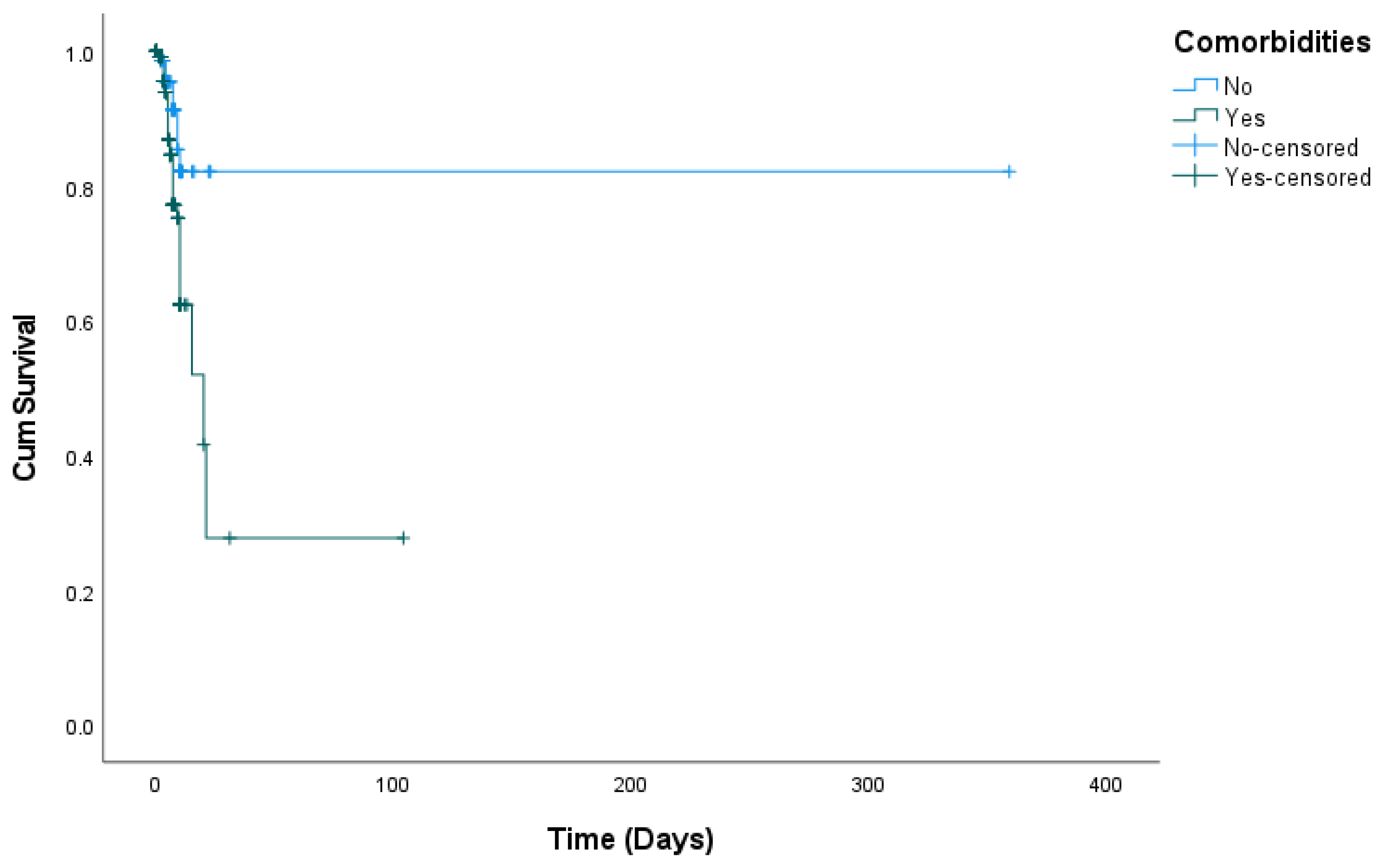
| Comorbidities | No | 8 (11.1%) | 64 (88.9%) | 0.017 a |
| Yes | 54 (24.3%) | 168 (75.7%) | ||
| Complications | No | 31 (12.9%) | 210 (87.1%) | <0.001 a |
| Yes | 31 (58.5%) | 22 (41.5%) | ||
| Blood Culture | Negative | 45 (22.5%) | 155 (77.5%) | 0.173 a |
| Positive | 9 (34.6%) | 17 (65.4%) | ||
| Urine Culture | Negative | 41 (24.4%) | 127 (75.6%) | 0.534 a |
| Positive | 5 (33.3%) | 10 (66.7%) | ||
| Sputum Culture | Negative | 18 (16.1%) | 94 (83.9%) | 0.006 b |
| Positive | 5 (62.5%) | 3 (37.5%) | ||
| Tracheal Culture | Negative | 16 (19.0%) | 68 (81.0%) | <0.001 b |
| Positive | 8 (88.9%) | 1 (11.1%) | ||
| Readmission | Within 15 Days | 2 (2.1%) | 94 (97.9%) | 0.028 b |
| Within 30 Days | 1 (11.1%) | 8 (88.9%) | ||
| Within 60 Days | 2 (14.3%) | 12 (85.7%) | ||
| Within 90 Days | 1 (25.0%) | 3 (75.0%) | ||
| Alive, Mean (SD) | Dead, Mean (SD) | |||
| Length of Hospital Stay (Days) | 9.33 (9.7) | 5.0 (3.3) | 0.182 | |
| Length of ICU Stay (Days) | 3.0 (-) | 5.50 (3.5) | 0.333 | |
| Laboratory Parameters | ||||
| Hemoglobin (Hb) (g/dl) | 13.40 (2.18) | 14.53 (6.83) | 0.207 | |
| White Blood Cells (WBCs) (109/L) | 7.91 (4.10) | 6.15 (3.05) | <0.001 | |
| Platelets (109/L) | 226.23 (77.03) | 218.29 (84.19) | 0.506 | |
| Erythrocyte Sedimentation Rate (ESR) (mmh/h) | 76.19 (31.68) | 68.91 (29.36) | 0.217 | |
| D-Dimer (mg/L) | 3.18 (7.53) | 3.18 (30.45) | 0.999 | |
| Lactic Acid Dehydrogenase (LDH) (U/L) | 346.30 (203.06) | 291.10 (112.51) | 0.007 | |
| Aspartate Aminotransferase (AST) (U/L) | 50.49 (36.16) | 40.91 (21.55) | 0.010 | |
| Creatinine (µmol/L) | 114.28 (72.36) | 96.45 (60.27) | 0.052 | |
| Urea (mmol/L) | 8.85 (5.46) | 6.93 (4.88) | 0.009 | |
| C-Reactive Protein (CRP) (mg/l) | 88.50 (60.19) | 67.77 (53.66) | 0.011 | |
| Alkaline Phosphatase (ALP) (U/L) | 86.93 (48.87) | 66.13 (29.15) | <0.001 | |
| Gamma-Glutamyl Transferase (GGT) (U/L) | 72.58 (102.13) | 45.85 (40.64) | 0.002 | |
| Total Bilirubin (µmol/L) | 13.44 (7.43) | 14.73 (20.10) | 0.628 | |
| FiO2 | 73.80 (20.50) | 83.35 (17.06) | 0.035 | |
| Vital Parameters | ||||
| Temperature, “°C” | 37.29 (0.78) | 39.04 (23.06) | 0.620 | |
| Heart Rate | 98.49 (17.22) | 96.04 (17.38) | 0.400 | |
| Respiratory Rate | 20.39 (1.64) | 20.53 (1.42) | 0.572 | |
| Mean Arterial Pressure (MAP) | 85.67 (10.36) | 88.90 (11.14) | 0.346 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqahtani, S.; Alqahtani, M.; Amer, K.; Ur Rahman, F.; AlMasoudi, R.; Al-Otaibi, S.; Alahmary, B.; Asiri, O.; Alshamrani, A.; Alshehri, R.; et al. Favipiravir for COVID-19 Pneumonia: Effectiveness, Safety, and Clinical Outcomes: A Retrospective Single-Center Experience. COVID 2024, 4, 1971-1984. https://doi.org/10.3390/covid4120139
Alqahtani S, Alqahtani M, Amer K, Ur Rahman F, AlMasoudi R, Al-Otaibi S, Alahmary B, Asiri O, Alshamrani A, Alshehri R, et al. Favipiravir for COVID-19 Pneumonia: Effectiveness, Safety, and Clinical Outcomes: A Retrospective Single-Center Experience. COVID. 2024; 4(12):1971-1984. https://doi.org/10.3390/covid4120139
Chicago/Turabian StyleAlqahtani, Saad, Mushary Alqahtani, Khaled Amer, Fasih Ur Rahman, Razan AlMasoudi, Sahar Al-Otaibi, Batool Alahmary, Osama Asiri, Abdulaziz Alshamrani, Razan Alshehri, and et al. 2024. "Favipiravir for COVID-19 Pneumonia: Effectiveness, Safety, and Clinical Outcomes: A Retrospective Single-Center Experience" COVID 4, no. 12: 1971-1984. https://doi.org/10.3390/covid4120139
APA StyleAlqahtani, S., Alqahtani, M., Amer, K., Ur Rahman, F., AlMasoudi, R., Al-Otaibi, S., Alahmary, B., Asiri, O., Alshamrani, A., Alshehri, R., Asiri, F., Alqahtani, M., Alshahrani, A., & Elsharif, Y. (2024). Favipiravir for COVID-19 Pneumonia: Effectiveness, Safety, and Clinical Outcomes: A Retrospective Single-Center Experience. COVID, 4(12), 1971-1984. https://doi.org/10.3390/covid4120139