
Eating Habits and Mental Health of College Students in Japan during the COVID-19 Pandemic



Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Design and Participants
2.2. Survey Questionnaire on Eating Habits
2.3. Questionnaire on Mental Health
2.4. Cluster Analysis to Determine the Relationships between Eating Habits and Mental Health
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. Descriptive Statistics
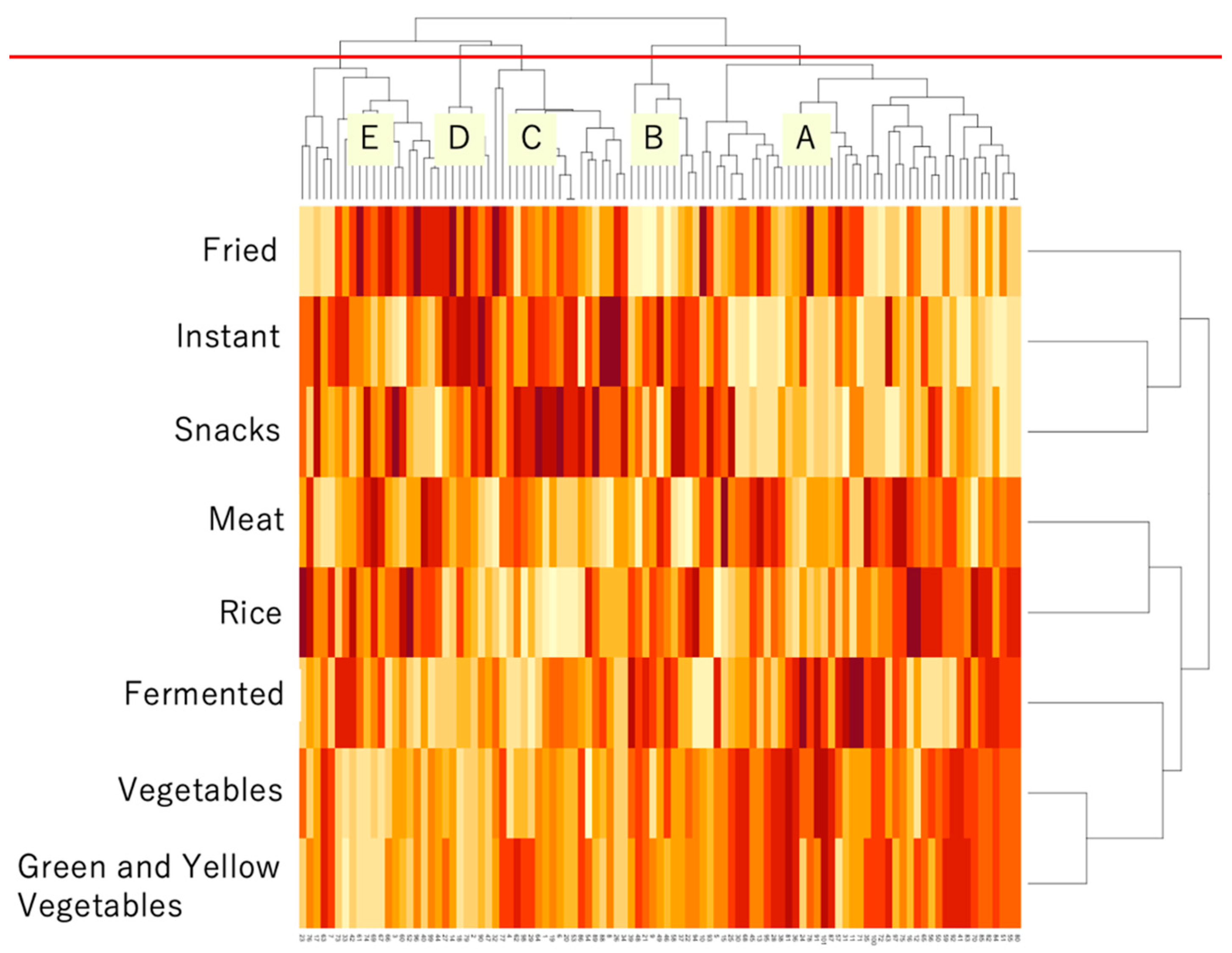
3.2. Results of Cluster Analysis
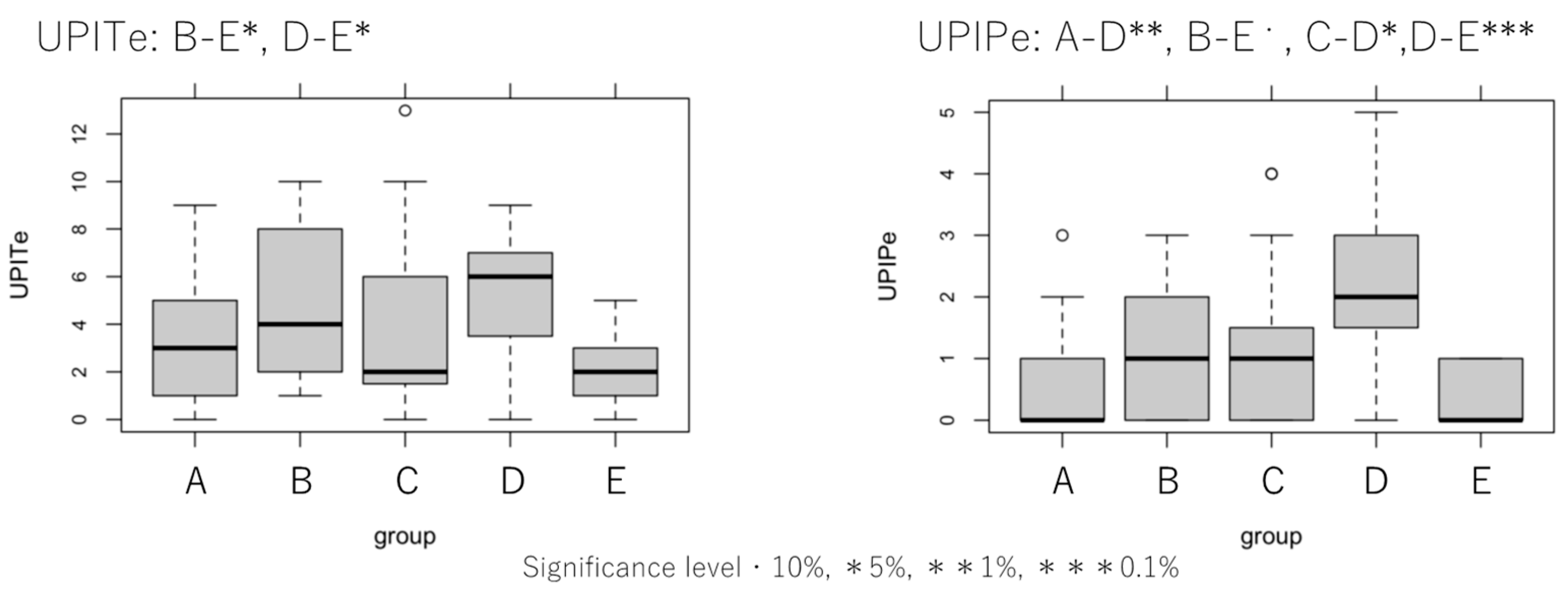
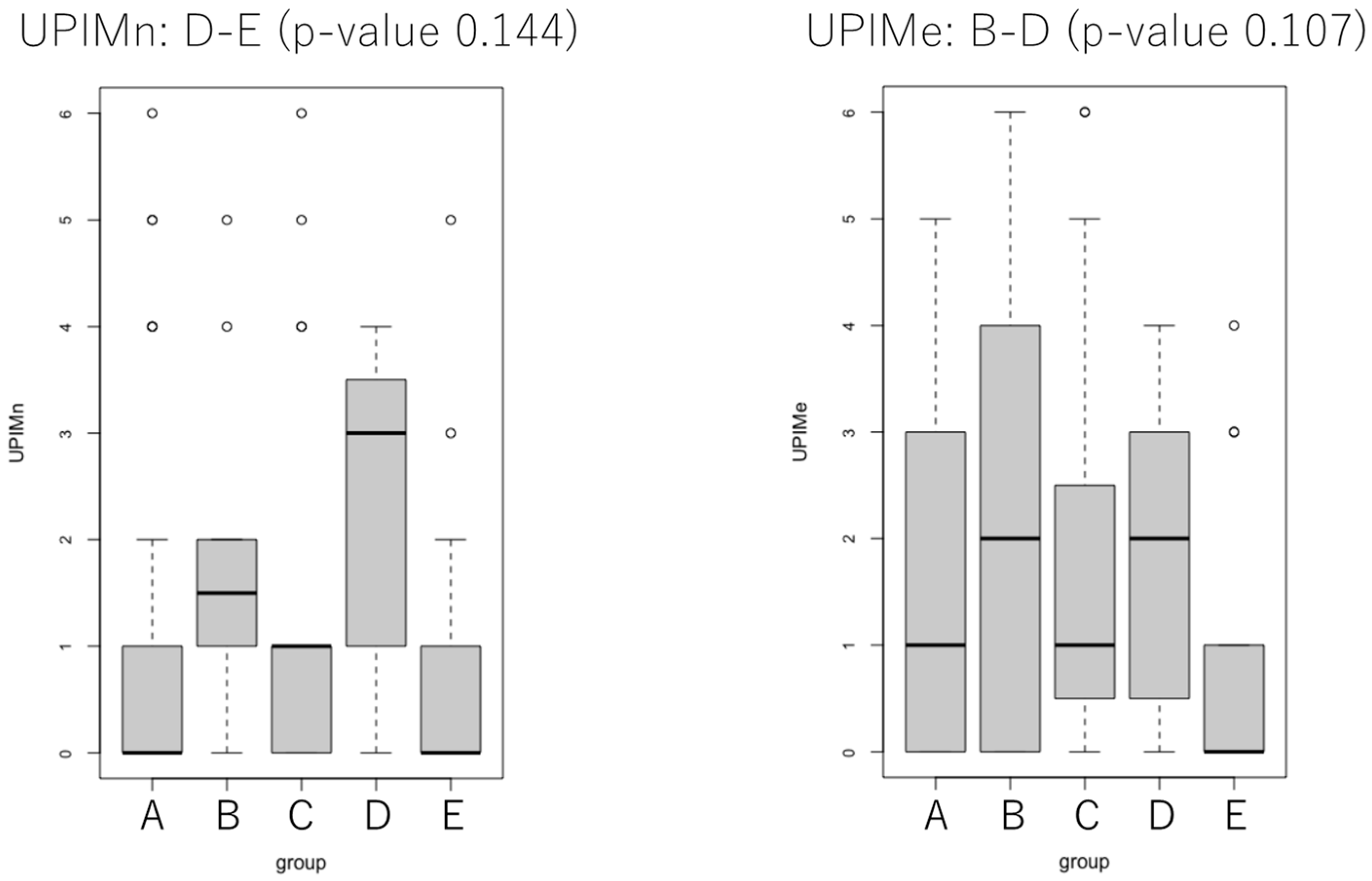
3.3. Results of Statistical Analysis of UPI Scores
4. Discussion
5. Conclusions
- Group A, with 45 participants, was the largest; the proportions of male students and those in the first grade were 46.7% and 20.0%, respectively. This group had relatively high vegetable intake, balanced eating habits, and a high level of mental health.
- Group B included 10 participants. The proportions of male participants and those in the first grade were 60.0% and 20.0%, respectively. This group was similar to group A in eating habits; however, it had a lower degree of mental health. Group B increased the intake of some food items owing to anxiety about COVID-19.
- Group C, with 19 participants, had the highest proportion of female participants (63.2%). Furthermore, the proportion of participants in the first grade was 21.1%. This group was characterized by the lowest intake of rice. They were at an intermediate level of mental health.
- Group D, with seven participants, had the highest proportions of male (71.4%) and first-grade (28.6%) participants. They had the highest intake of fried foods, instant foods, snacks, bread, soft drinks, and alcohol; their mental health level was relatively low.
- Group E, with 20 participants, had the second-highest proportion of male participants (70.0%) and the lowest proportion of those in the first grade (5.0%). They had a relatively low frequency of intake of most foods and increased intake of soft drinks, which may relieve stress; their mental health was the highest among the five groups.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grant, F.; Scalvedi, M.L.; Scognamiglio, U.; Turrini, A.; Rossi, L. Eating habits during the COVID-19 lockdown in Italy: The nutritional and lifestyle side effects of the pandemic. Nutrients 2021, 13, 2279. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.F.O.; Cobucci, R.N.; Gonçalves, A.K.; Lima, S.C.V.C. Systematic review of the association between dietary patterns and perinatal anxiety and depression. BMC Pregnancy Childbirth 2019, 19, 212. [Google Scholar] [CrossRef] [PubMed]
- Konishi, K. Associations between healthy Japanese dietary patterns and depression in Japanese women. Public Health Nutr. 2021, 24, 1753–1765. [Google Scholar] [CrossRef] [PubMed]
- Beesdo, K.; Bittner, A.; Pine, D.S.; Stein, M.B.; Höfler, M.; Lieb, R.; Wittchen, H.U. Incidence of social anxiety disorder and the consistent risk for secondary depression in the first three decades of life. Arch. Gen. Psychiatry 2007, 64, 903–912. [Google Scholar] [CrossRef]
- Lewinsohn, P.M.; Rohde, P.; Seeley, J.R.; Klein, D.N.; Gotlib, I.H. Natural course of adolescent major depressive disorder in a community sample: Predictors of recurrence in young adults. Am. J. Psychiatry 2000, 157, 1584–1591. [Google Scholar] [CrossRef] [PubMed]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on college students’ mental health in the United States: Interview survey study. J. Med. Internet. Res. 2020, 22, e21279. [Google Scholar] [CrossRef]
- National Federation of University Cooperative Associations. Full report on the Pandemic’s Impact on University Life: A Survey. Available online: https://www.univcoop.or.jp/en/activity/pdf/pdf_activity01.pdf (accessed on 10 August 2021).
- Horowitz, J.L.; Garber, J. The prevention of depressive symptoms in children and adolescents: A meta-analytic review. J. Consult. Clin. Psychol. 2006, 74, 401–415. [Google Scholar] [CrossRef]
- Miyake, Y.; Okamoto, Y. Mental health of university students. Jpn. J. Psychosom. Med. 2015, 55, 1360–1366. [Google Scholar]
- Yokoro, M.; Wakimoto, K.; Otaki, N.; Fukuo, K. Increased prevalence of breakfast skipping in female college students in Covid-19. Asia Pacific J. Public Health 2021, 33, 438–440. [Google Scholar] [CrossRef]
- Pendergast, F.J.; Livingstone, K.M.; Worsley, A.; McNaughton, S.A. Correlates of meal skipping in young adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 125. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, H.; Fujita, T.; Kubo, M. Dietary factors that influence the mental health of university students. Mem. Fac. Agric. Kinki Univ. 2008, 41, 17–25. [Google Scholar]
- Konishi, K.; Hyakutake, A.; Muramatsu, T. Dietary patterns and health-related QOL among female university students. Shinshu J. Public Health 2013, 7, 83–94. [Google Scholar]
- Tominaga, M.; Shimizu, M.; Mori, T.; Kodama, K.; Sato, K. Relationship between life style focusing on eating habits and mental health of junior and high school students, and university students. J. Home Econ. Jpn. 2001, 52, 499–510. [Google Scholar]
- Marani, M.; Katul, G.G.; Pan, W.K.; Parolari, A.J. Intensity and frequency of extreme novel epidemics. Proc. Natl. Acad. Sci. USA 2021, 118, e2105482118. [Google Scholar] [CrossRef] [PubMed]
- Poblacion, A.; de Cuba, S.E.; Cook, J.T. Comparing food security before and during the COVID-19 pandemic: Considerations when choosing measures. J. Acad. Nutr. Diet. 2021, 121, 1945–1947. [Google Scholar] [CrossRef]
- Le, L.M.; Flores, G.; Edejer, T.T.-T.; Tran, T.K.; Nguyen, C.T.K.; Tran, D.T.; Ho, P.D.; Agorinya, I.A.; Tediosi, F.; Ross, A. Investigating the effect of recall period on estimates of inpatient out-of-pocket expenditure from household surveys in Vietnam. PLoS ONE 2020, 15, e0242734. [Google Scholar] [CrossRef]
- Isobe, Y.; Shigematsu, R. Study on the dietary life of university students. Jpn. Bull. Fac. Educ. Mie Univ. 2007, 58, 63–76. [Google Scholar]
- Ikeda, J.; Asano, M.; Kitani, T.; Nagata, H. Study on food intake frequency among elderly persons. Jpn. J. Nutr. Diet. 1991, 49, 257–271. [Google Scholar] [CrossRef]
- Savige, G.; MacFarlane, A.; Ball, K.; Worsley, A.; Crawford, D. Snacking behaviours of adolescents and their association with skipping meals. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 36. [Google Scholar] [CrossRef]
- The Yomiuri Shimbun. Speculation Prompts Rise in Fermented Food Sales. Available online: https://www.yomiuri.co.jp/national/20200517-OYT1T50101/ (accessed on 19 May 2020).
- Kagawa, Y. Influence of nutritional intakes in Japan and the United States on COVID-19 infection. Nutrients 2022, 14, 633. [Google Scholar] [CrossRef]
- Hirayama, K. The Management of Mental Health in College Students—User guide for the UPI; Sozo-shuppan: Tokyo, Japan, 2020. (In Japanese) [Google Scholar]
- Oka, I.; Yoshimura, M.; Yamagishi, T. Changes in mental health of freshwomen at Tsuda University. J. Tsuda Univ. 2015, 47, 175–195. [Google Scholar]
- Sakai, W. Reconstruction of University Personality Inventory Based on Student Counseling Model. Doctoral Dissertation, Nagoya University, Nagoya, Japan, 2016. [Google Scholar]
- Hobart, E. Japan’s Most Polarising Superfood? BBC.com. Available online: https://www.bbc.com/travel/article/20200727-japans-most-polarising-superfood (accessed on 29 July 2020).
- Oba, M.; Rongduo, W.; Saito, A.; Okabayashi, T.; Yokota, T.; Yasuoka, J.; Sato, Y.; Nishifuji, K.; Wake, H.; Nibu, Y.; et al. Natto extract, a Japanese fermented soybean food, directly inhibits viral infections including SARS-COV-2 in vitro. Biochem. Biophys. Res. Commun. 2021, 570, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-M.; Lee, E. Association between soft-drink intake and obesity, depression, and subjective health status of male and female adults. Int. J. Environ. Res. Public Health 2021, 18, 10415. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| UPIP | UPIM | UPIC | |
|---|---|---|---|
| 1 | I feel tired | I have emotional ups and downs | I feel uneasy about my income owing to poor economic conditions |
| 2 | I have no appetite | I tend to get pessimistic | I want to restart my current school year even if I take a leave of absence or have to repeat a year |
| 3 | I get tired easily | I’m too lethargic to do anything | I don’t fully understand local governments’ system of infection control and inspection |
| 4 | I’m having trouble with sleeplessness | I sometimes get anxious or worried about the present or future | I’m worried about getting infected with COVID-19 |
| 5 | My eyes feel tired | I feel lonely | I may neglect infection control measures |
| 6 | I feel dizzy or as if I am about to collapse | I have no one I feel free to talk with about what bothers me |
| Under the State of Emergency (April to May 2020) | At the Time of the Survey | |
|---|---|---|
| I feel tired | ||
| I have no appetite | ||
| I have emotional ups and downs | ||
| I’m having trouble with sleeplessness | ||
| I may feel uneasy about my income owing to poor economic conditions |
| UPITn | UPITe | UPIPn | UPIPe | UPIMn | UpiMe | UPICn | UPICe | |
|---|---|---|---|---|---|---|---|---|
| Male | 2.75 | 2.94 | 0.77 | 0.75 | 1.06 | 1.47 | 0.92 | 0.72 |
| Female | 3.42 | 3.98 | 0.90 | 0.98 | 1.31 | 1.79 | 1.21 | 1.21 |
| UPITn | UPITe | UPIPn | UPIPe | UPIMn | UpiMe | UPICn | UPICe | |
|---|---|---|---|---|---|---|---|---|
| First year | 3.22 | 4.00 | 0.83 | 1.00 | 1.11 | 1.94 | 1.28 | 1.06 |
| Second year | 3.67 | 3.40 | 0.87 | 0.87 | 1.60 | 1.60 | 1.20 | 0.93 |
| Third year | 2.98 | 3.46 | 0.79 | 0.77 | 1.11 | 1.63 | 1.09 | 1.05 |
| Forth year | 2.45 | 2.45 | 1.00 | 1.09 | 1.09 | 1.09 | 0.36 | 0.27 |
| Group | n | Rice | Meat | Greenvege | Vege | Fermented | Fried | Instant | Snacks |
|---|---|---|---|---|---|---|---|---|---|
| A | 45 | 53.75 | 55.09 | 56.15 | 56.87 | 54.40 | 49.73 | 46.43 | 47.13 |
| B | 10 | 58.30 | 49.50 | 56.15 | 57.43 | 59.90 | 44.33 | 58.44 | 58.69 |
| C | 19 | 37.76 | 42.64 | 46.34 | 43.81 | 43.15 | 49.10 | 51.87 | 54.70 |
| D | 7 | 46.60 | 49.17 | 44.32 | 43.58 | 44.67 | 64.23 | 70.32 | 58.69 |
| E | 20 | 50.22 | 46.07 | 38.56 | 38.94 | 43.53 | 49.31 | 44.92 | 44.60 |
| Group | n | Bread | Fish | Egg | Soybean | Milk | Potato | Fruit | Soft drink | Alcohol |
|---|---|---|---|---|---|---|---|---|---|---|
| A | 45 | 52.20 | 52.76 | 53.97 | 53.79 | 53.59 | 52.28 | 52.48 | 51.29 | 49.58 |
| B | 10 | 47.24 | 53.89 | 50.90 | 52.54 | 50.44 | 53.39 | 55.00 | 48.37 | 49.58 |
| C | 19 | 48.45 | 48.45 | 44.77 | 42.88 | 47.64 | 50.42 | 48.85 | 46.40 | 50.64 |
| D | 7 | 55.34 | 50.13 | 47.52 | 52.81 | 46.64 | 51.33 | 46.96 | 56.22 | 52.82 |
| E | 20 | 46.03 | 43.26 | 46.46 | 45.99 | 45.12 | 42.31 | 44.08 | 49.16 | 49.58 |
| Group | n | health | food |
|---|---|---|---|
| A | 45 | 3.44 | 3.49 |
| B | 10 | 3.70 | 3.20 |
| C | 19 | 3.00 | 2.89 |
| D | 7 | 3.00 | 2.29 |
| E | 20 | 2.85 | 2.75 |
| Group | n | Rice | Meat | Greenvege | Vege | Fermentd | Fried | Instant | Snacks | |
|---|---|---|---|---|---|---|---|---|---|---|
| A | 45 | 33.33% | 8.89% | 8.89% | 4.44% | 20.00% | 2.22% | 13.33% | 17.78% | |
| B | 10 | 10.00% | 10.00% | 20.00% | 20.00% | 50.00% | 0.00% | 30.00% | 40.00% | |
| C | 19 | 21.05% | 10.53% | 0.00% | 0.00% | 21.05% | 5.26% | 36.84% | 42.11% | |
| D | 7 | 14.29% | 28.57% | 0.00% | 0.00% | 28.57% | 28.57% | 57.14% | 28.57% | |
| E | 20 | 30.00% | 5.00% | 0.00% | 0.00% | 5.00% | 0.00% | 20.00% | 15.00% | |
| Group | n | Bread | Fish | Egg | Soybean | Milk | Potato | Fruit | Soft drink | Alcohol |
| A | 45 | 17.78% | 4.44% | 11.11% | 11.11% | 6.67% | 0.00% | 2.22% | 11.11% | 8.89% |
| B | 10 | 0.00% | 10.00% | 10.00% | 20.00% | 0.00% | 0.00% | 20.00% | 10.00% | 20.00% |
| C | 19 | 26.32% | 5.26% | 15.79% | 5.26% | 21.05% | 5.26% | 10.53% | 10.53% | 15.79% |
| D | 7 | 28.57% | 14.29% | 28.57% | 14.29% | 0.00% | 0.00% | 0.00% | 0.00% | 0.00% |
| E | 20 | 10.00% | 0.00% | 5.00% | 0.00% | 0.00% | 0.00% | 5.00% | 25.00% | 10.00% |
| Group | Distracted by eating | Time saving, convenient | Cheap, price-performance | Good for health | Expecting strengthen immue system |
|---|---|---|---|---|---|
| A | 26.67% | 26.67% | 15.56% | 20.00% | 8.89% |
| B | 40.00% | 20.00% | 30.00% | 30.00% | 10.00% |
| C | 26.32% | 52.63% | 42.11% | 10.53% | 0.00% |
| D | 28.57% | 57.14% | 57.14% | 28.57% | 0.00% |
| E | 55.00% | 35.00% | 25.00% | 10.00% | 5.00% |
| Group | Food expenses | Breakfast intake | Frequency of self-catering | Number of foods | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Decrease | No change | Increase | Decrease | No change | Increase | Decrease | No change | Increase | Decrease | No change | Increase | |
| A | 26.7% | 51.1% | 22.2% | 24.4% | 66.7% | 8.9% | 13.3% | 53.3% | 33.3% | 8.9% | 80.0% | 11.1% |
| B | 40.0% | 30.0% | 30.0% | 20.0% | 70.0% | 10.0% | 20.0% | 50.0% | 30.0% | 10.0% | 60.0% | 30.0% |
| C | 31.6% | 47.4% | 21.1% | 21.1% | 68.4% | 10.5% | 10.5% | 63.2% | 26.3% | 21.1% | 78.9% | 0.0% |
| D | 0.0% | 57.1% | 42.9% | 28.6% | 57.1% | 14.3% | 28.6% | 42.9% | 28.6% | 28.6% | 57.1% | 14.3% |
| E | 15.0% | 45.0% | 40.0% | 20.0% | 75.0% | 5.0% | 15.0% | 60.0% | 25.0% | 5.0% | 75.0% | 20.0% |
| Average | 22.6% | 46.1% | 31.2% | 22.8% | 67.4% | 9,7% | 17.5% | 53.9% | 28.6% | 14.7% | 70.2% | 15.1% |
| Group | n | First grade | Male | UPITn | UPITe | UPIPn | UPIPe | UPIMn | UpiMe | UPICn | UPICe |
|---|---|---|---|---|---|---|---|---|---|---|---|
| A | 45 | 20.0% | 46.7% | 2.84 | 3.20 | 0.78 | 0.69 | 1.04 | 1.62 | 1.02 | 0.89 |
| B | 10 | 20.0% | 60.0% | 4.00 | 4.90 | 0.90 | 1.30 | 1.80 | 2.40 | 1.30 | 1.20 |
| C | 19 | 21.1% | 36.8% | 3.37 | 3.95 | 0.95 | 1.05 | 1.37 | 1.79 | 1.05 | 1.11 |
| D | 7 | 28.6% | 71.4% | 5.00 | 5.14 | 1.43 | 2.29 | 2.29 | 1.86 | 1.29 | 1.00 |
| E | 20 | 5.0% | 70.0% | 2.20 | 1.90 | 0.60 | 0.30 | 0.65 | 0.80 | 0.95 | 0.80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imoto, T.; Hoshino, Y.; Sato, Y.; Ohsaki, Y.; Shirakawa, H. Eating Habits and Mental Health of College Students in Japan during the COVID-19 Pandemic. COVID 2023, 3, 1721-1732. https://doi.org/10.3390/covid3120119
Imoto T, Hoshino Y, Sato Y, Ohsaki Y, Shirakawa H. Eating Habits and Mental Health of College Students in Japan during the COVID-19 Pandemic. COVID. 2023; 3(12):1721-1732. https://doi.org/10.3390/covid3120119
Chicago/Turabian StyleImoto, Tomoko, Yuichiro Hoshino, Yoshiyuki Sato, Yusuke Ohsaki, and Hitoshi Shirakawa. 2023. "Eating Habits and Mental Health of College Students in Japan during the COVID-19 Pandemic" COVID 3, no. 12: 1721-1732. https://doi.org/10.3390/covid3120119
APA StyleImoto, T., Hoshino, Y., Sato, Y., Ohsaki, Y., & Shirakawa, H. (2023). Eating Habits and Mental Health of College Students in Japan during the COVID-19 Pandemic. COVID, 3(12), 1721-1732. https://doi.org/10.3390/covid3120119