
Dynamics of Variants of Concern (VOC) of SARS-CoV-2 during the Different Waves of COVID-19 in Senegal


 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
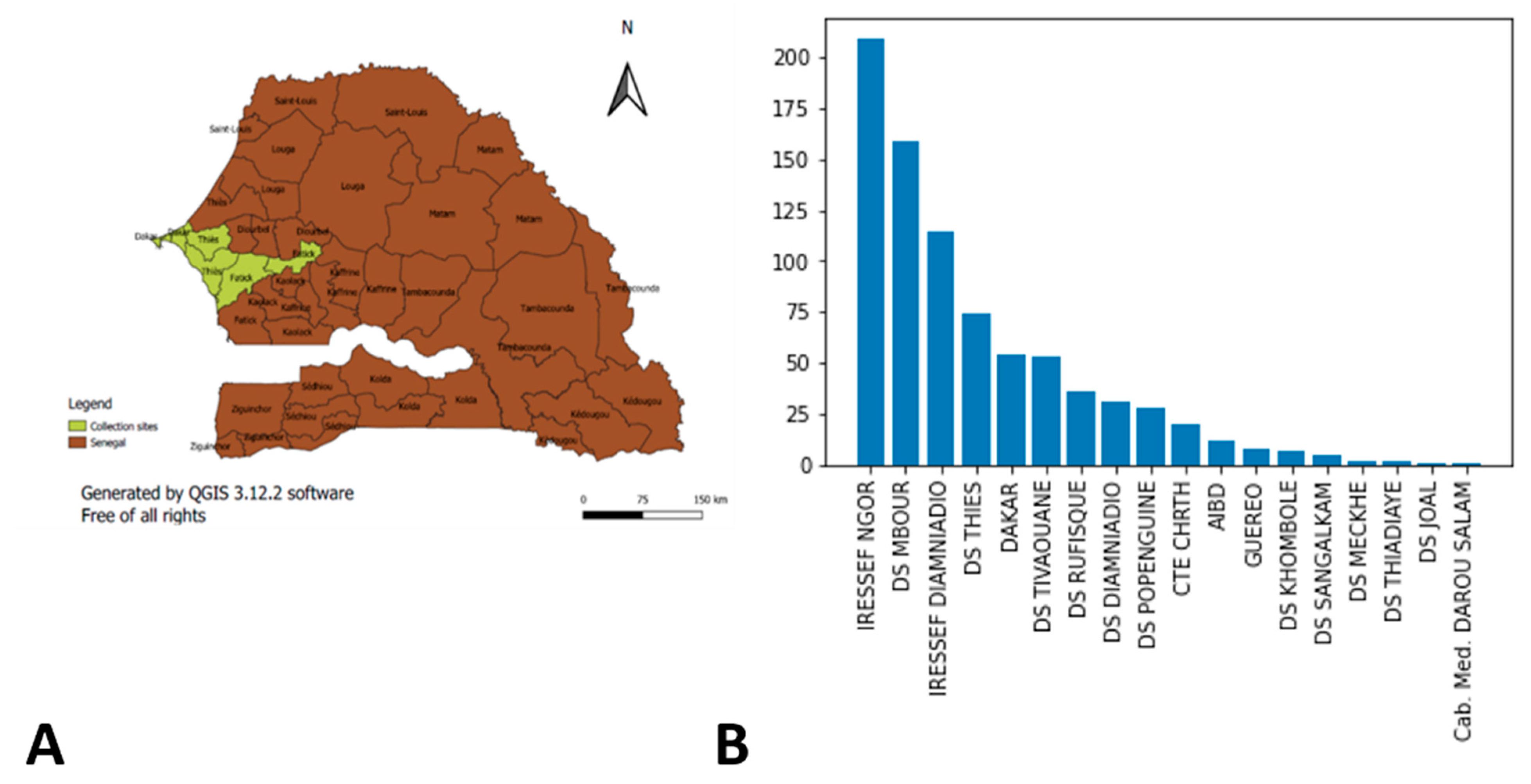
2.1. Study Settings and Design
2.2. Study Population and Sampling
2.3. RNA Extraction
2.4. Reverse Transcriptase-Polymerase Chain Reaction
2.5. Whole Genome Sequencing (WGS) of SARS-CoV-2 Using Oxford Nanopore Technology
2.5.1. Library Preparation and Sequencing
2.5.2. Data Analysis
3. Results
3.1. Waves and Variants
3.2. Distribution of Variants by Age and Sex
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- WHO. Novel Coronavirus—China. Available online: http://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/ (accessed on 16 January 2021).
- WHO. Director-General’s Remarks at the Media Briefing on 2019-nCoV on 11 February 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020 (accessed on 28 February 2021).
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Haider, N.; Yavlinsky, A.; Simons, D.; Osman, A.Y.; Ntoumi, F.; Zumla, A.; Kock, R. Passengers’ destinations from China: Low risk of Novel Coronavirus (2019-nCoV) transmission into Africa and South America. Epidemiol. Infect. 2020, 148, e41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert, M.; Pullano, G.; Pinotti, F.; Valdano, E.; Poletto, C.; Boëlle, P.-Y.; D’Ortenzio, E.; Yazdanpanah, Y.; Eholie, S.P.; Altmann, M.; et al. Preparedness and vulnerability of African countries against importations of COVID-19: A modelling study. Lancet 2020, 395, 871–877. [Google Scholar] [CrossRef] [Green Version]
- Khattab, N.M.; Vermund, S.H.; Hu, Y. How coronavirus disease 2019 entered Africa and the Middle East: A case study from Egypt. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 715–717. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus-West-Africa—Sahel and West Africa Club Secretariat. Available online: https://www.oecd.org/swac/coronavirus-west-africa/ (accessed on 16 September 2021).
- WHO|Regional Office for Africa. Senegal Reports First COVID-19 Case. Available online: https://www.afro.who.int/news/senegal-reports-first-covid-19-case (accessed on 16 January 2021).
- Volz, E.; Hill, V.; McCrone, J.T.; Price, A.; Jorgensen, D.; O’Toole, Á.; Southgate, J.; Johnson, R.; Jackson, B.; Nascimento, F.F.; et al. Evaluating the Effects of SARS-CoV-2 Spike Mutation D614G on Transmissibility and Pathogenicity. Cell 2021, 184, 64–75. [Google Scholar] [CrossRef] [PubMed]
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 and Novel Therapeutics Against Coronavirus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Padane, A.; Kanteh, A.; Leye, N.; Mboup, A.; Manneh, J.; Mbow, M.; Diaw, P.; Ndiaye, B.; Lo, G.; Lo, C.; et al. First detection of SARS-CoV-2 variant B.1.1.7 in Senegal. New Microbes New Infect. 2021, 41, 100877. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Deng, A.; Li, K.; Hu, Y.; Li, Z.; Xiong, Q.; Liu, Z.; Guo, Q.; Zou, L.; Zhang, H.; et al. Viral infection and transmission in a large well-traced outbreak caused by the Delta SARS-CoV-2 variant. medRxiv 2021. [CrossRef] [PubMed]
- Sahoo, J.P.; Samal, K.C. World on Alert: WHO Designated South African New COVID Strain (Omicron/B.1.1.529) as a Variant of Concern. Biot. Res. Today 2021, 3, 1086–1088. [Google Scholar]
- Freppel, W.; Merindol, N.; Rallu, F.; Bergevin, M. Efficient SARS-CoV-2 detection in unextracted oro-nasopharyngeal specimens by rRT-PCR with the Seegene Allplex™ 2019-nCoV assay. Virol. J. 2020, 17, 196. [Google Scholar] [CrossRef] [PubMed]
- Artic Network. Available online: https://artic.network/ncov-2019/ncov2019-bioinformatics-sop.html (accessed on 22 January 2022).
- Nextclade. Available online: https://clades.nextstrain.org (accessed on 22 January 2022).
- COG-UK. Available online: https://pangolin.cog-uk.io/ (accessed on 22 January 2022).
- GISAID—Initiative. Available online: https://www.gisaid.org/ (accessed on 22 January 2022).
- Staerk, C.; Wistuba, T.; Mayr, A. Estimating effective infection fatality rates during the course of the COVID-19 pandemic in Germany. BMC Public Health 2021, 21, 1073. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nextstrain (Clade) | Pango Lineages | WHO Label VOC Isolated at IRESSEF | Notification Date | |
|---|---|---|---|---|
| 19A | B, B.1, B.1.609 | Variants of Concern (VOC) | ||
| 19B | A, A.21, A.27 | |||
| 20A | B.1.1, B.1.160, B.1.214.2, B.1.221, B.1.258, B.1.416, B.1.469, B.1.541, B.1.610, B.1.620, B.1.596 | |||
| 20B | B.1.1.254, B.1.1.28, B.1.1.318, B.1.1.417, B.1.1.420, | |||
| 20C | B.1.2, B.1.429, B.1.469, B.1.626 | |||
| 20D | C.2, C.36 | |||
| 20E (EU1) | 20E (EU1), B.1.177 | |||
| 20G | B.1.2 | |||
| 20I (Alpha, V1) | B.1.1.7 | Alpha | 24 December 2020 | |
| 21D (Eta) | B.1.525 | Eta | ||
| 21J, 21A, 21I (Delta) | B.1.617.2, AY.10, AY.25, AY.26, AY.3, AY.34, AY.37, AY.39, AY.4, AY.43 | Delta | 28 May 2021 | |
| 21K (Omicron) | B.1.1.529 and BA.1 | Omicron | 25 November 2021 |
| Variants of Concern | Age Range | Male | Female | NF | p-Value |
|---|---|---|---|---|---|
| ALPHA | 0–15 | 1 | 0 | 2 | 0.47 |
| 16–30 | 0 | 2 | 2 | ||
| 31–45 | 3 | 1 | 4 | ||
| 46 and + | 3 | 3 | 13 | ||
| NF | 0 | 0 | 4 | ||
| DELTA | 0–15 | 3 | 2 | 0 | <0.001 |
| 16–30 | 11 | 23 | 1 | ||
| 31–45 | 30 | 32 | 2 | ||
| 46 and + | 32 | 21 | 2 | ||
| NF | 3 | 0 | 51 | ||
| OMICRON | 0–15 | 13 | 7 | 0 | 0.71 |
| 16–30 | 26 | 19 | 0 | ||
| 31–45 | 63 | 48 | 0 | ||
| 46 and + | 73 | 42 | 2 | ||
| NF | 1 | 2 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padane, A.; Diedhiou, C.K.; Gueye, K.; Ndiour, S.; Diagne, N.D.; Mboup, A.; Mbow, M.; Lo, C.I.; Leye, N.; Ndoye, A.S.; et al. Dynamics of Variants of Concern (VOC) of SARS-CoV-2 during the Different Waves of COVID-19 in Senegal. COVID 2022, 2, 691-702. https://doi.org/10.3390/covid2060052
Padane A, Diedhiou CK, Gueye K, Ndiour S, Diagne ND, Mboup A, Mbow M, Lo CI, Leye N, Ndoye AS, et al. Dynamics of Variants of Concern (VOC) of SARS-CoV-2 during the Different Waves of COVID-19 in Senegal. COVID. 2022; 2(6):691-702. https://doi.org/10.3390/covid2060052
Chicago/Turabian StylePadane, Abdou, Cyrille Kouligeul Diedhiou, Khadim Gueye, Samba Ndiour, Ndéye Diabou Diagne, Aminata Mboup, Moustapha Mbow, Cheikh Ibrahima Lo, Nafissatou Leye, Aissatou Sow Ndoye, and et al. 2022. "Dynamics of Variants of Concern (VOC) of SARS-CoV-2 during the Different Waves of COVID-19 in Senegal" COVID 2, no. 6: 691-702. https://doi.org/10.3390/covid2060052
APA StylePadane, A., Diedhiou, C. K., Gueye, K., Ndiour, S., Diagne, N. D., Mboup, A., Mbow, M., Lo, C. I., Leye, N., Ndoye, A. S., Ndiaye, A. J. S., Ndiaye, S., Dia, Y. A., Lo, G., Wade, D., Ahouidi, A., Diaw, P. A., Sarr, M., Beye, M., ... Mboup, S. (2022). Dynamics of Variants of Concern (VOC) of SARS-CoV-2 during the Different Waves of COVID-19 in Senegal. COVID, 2(6), 691-702. https://doi.org/10.3390/covid2060052