1. Introduction
Historically, large movements of people from place to place have led to outbreaks of epidemic infections that proved near catastrophic to continuing civilisation [
1,
2]. Consequently, increased travel for business and leisure is deemed to accelerate the global spread of infectious diseases, causing pandemics [
3]. The outbreak of COVID-19 in Wuhan, China, in January 2019 [
4] and its subsequent declaration as a global pandemic by the World Health Organization [
5] presented many challenges to the global community. The coronavirus pandemic can be considered the biggest challenge in scale and gravity faced by humanity this century. It has produced many unanticipated demands that governments, companies, and communities were ill-prepared to handle. As a result of improved travel, the virus quickly spread around the globe. This triggered a global response to contain the spread of the pandemic to curb human mortality. In recognition of the relationship between the spread of disease and human movement, most countries responded by imposing restrictions on local and long-distance travel immediately following the outbreak of the virus within their national boundaries, with various restrictions between countries [
6]. For example, Karim [
7] reported that in South Africa, after identifying 402 cases, a 35-day strict national lockdown was declared, which included the revocation of visas, instituting of travel bans, and closure of 35 of South Africa’s 53 land ports [
8]. Due to travel restrictions, every country experienced a massive demand for personal protective equipment (PPE), which could not be purchased anywhere else.
Similarly, Canada restricted international travel, and all Canadian provinces were mandated to close schools, universities, public playgrounds, and non-essential businesses. Further, the federal and provincial governments encouraged everyone except essential workers to stay at home [
9]. The Government of Botswana responded by declaring a State of Public Emergency (SoPE) and a 29-day national lockdown with extreme social distancing as the initial response. The nationwide lockdown confined every person to their place of residence except for those who needed to carry out essential services or access essential supplies [
10]. The national lockdown was followed by a lockdown of the Greater Gaborone Zone from 12 June to 13 August 2020, as it was identified as the epicentre of the pandemic in the country [
11]. Further, nationwide curfews of varying timeframes were implemented on 24 December 2020 [
11,
12].
It has, however, been widely recognised that the spread of the COVID-19 pandemic cannot be contained by the restriction of movement of people alone. For instance, other measures that have been widely used to prevent the spread of the virus are social distancing, face masks, and regular washing of hands with soap and/or using alcohol-based sanitisers. Since COVID-19 has been established as a respiratory disease [
13], in addition to measures intended to curb its spread, research and development initiatives went underway to develop breathing aid devices for caring for coronavirus-infected patients [
14]. This paper reports on the experiences of the University of Botswana in developing breathing aid devices in response to COVID-19. The paper is based on the first-hand account of those who participated in developing a ventilator, ventilation masks, ventilation hoods, and face shields.
The declaration of COVID-19 as a global pandemic by the World Health Organization on 11 March 2020 led the President of Botswana to declare a state of public emergency (SoPE) that commenced on 31 March 2020 to address the risks posed by the disease [
10]. Following the declaration of SoPE, emergency (COVID-19) regulations were developed to control the spread of the pandemic. Among these regulations was the declaration of a national lockdown from 2 April 2020 until 30 April 2020 [
15]. The lockdown confined people to their place of residences and prohibited gatherings. Only people deemed to be providing essential services were allowed outside their residence to obtain crucial supplies upon receiving a special permit. The University of Botswana’s COVID-19 response team was among those travelling to work on essential services permits. Further, during the SoPE, other statutory instruments were issued to control the pandemic’s spread as the disease burden in the country increased. These instruments, among others, prohibited international travel into Botswana from high-risk countries as defined by WHO, closed ports of entry, introduced curfews, restricted alcohol trading, and suspended some trading licenses.
At the onset of the pandemic in Botswana, four cases and one death were recorded on 30 March 2020. On 2 August 2021, the country recorded a peak of 15,884 cases and 269 deaths by 9 August 2021. On 17 February 2022, the cumulative COVID-19 positive cases were 260,491, with 2603 deaths also recorded [
5]. The Government of Botswana also engaged in a vaccine rollout programme. By 17 February 2022, 48.82 percent of the population was fully vaccinated [
16].
As has been the trend with all previous pandemics, the COVID-19 pandemic was not without a swift response from institutions of higher learning through initiatives in R&D regionally and globally. Universities played a pivotal role in responding to the COVID-19 crisis through cutting-edge research and development. Higher education institutions worldwide reacted to the pandemic in various ways. Some worked in collaboration with government organs, others with the private sector, some acted independently, others forged partnerships with other higher education institutions, some freely shared their research findings, while others developed for-profit to ensure the sustainability of initiatives. Many universities have contributed to the pandemic response by producing vaccines, medical equipment, and supplies, such as the virus’s genome, vaccine development, personal protective equipment, and breathing assistive devices. With the global and regional responses to the COVID-19 pandemic by higher education institutions notwithstanding, universities in Botswana also responded swiftly to the pandemic through several R&D initiatives.
2. Research Method
The study adopted the qualitative research approach, which relies on the subjective expressions of meaning from the participants studied. The agile and co-creation methods were adopted because such a combination of design approach has been widely used in developing products and services [
17,
18,
19]. Although the agile methodology is a software development methodology, it offers many opportunities in product development because it is iterative and helped the design team to deliver value to users quickly in response to the COVID-19 crisis. The agile methodology involves continuous collaboration and working in iterations with users. This enabled the design team to continuously improve the products and respond to users’ feedback. Tessarolo [
20] argues that agile methodology is flexible, adaptable to change, and has a high user input level. Agile methodology improves development performance through numerous, efficient, and effective alterations of user requirements and subsequent changes [
19].
The co-creation process was used during the research and development phase to complement the agile methodology because it is an inclusive, innovative, collaborative, and participatory approach that produces new products and services with added value [
21,
22]. The value is created through close collaboration between the design team and stakeholders. Users and designers share knowledge, ideas, insights, and improve them together, thus creating collaborative innovation. A design approach based on incremental, iterative delivery and empirical feedback was considered more suited to the innovative character of the study because it reaches high user acceptability, usability, and satisfaction [
22]. Users/stakeholders were involved in each development phase (planning, design, development, laboratory testing, user testing, and evaluation) of the agile and co-creation approach. For example, the design team will engage users prior to and after each development phase to get user requirements and feedback to improve product development. This agile and iterative process enabled the design team to evaluate the design solutions’ efficiency and effectiveness and constantly improve them until the users’ needs were met.
The University of Botswana set up a multidisciplinary design team of 19 people made from medicine, biomedical engineering, mechanical engineering, electrical engineering, mechatronics, and industrial designers to design personal protective equipment and other specialised health-related products and services such as face masks, ventilators, and respiratory hood nebuliser (oxygen) mask. The design team worked with doctors (general practitioners, cardiologists, pulmonologists, nurses, and public members) at the University Teaching Hospital to develop the ventilator, face masks, ventilation hood, and nebulisers. The participants were purposively sampled because they were likely to give rich information about the phenomenon under study. They were readily available on the University campus since the country was on lockdown.
The COVID-19 design team started working on the products when almost all countries were in lockdown. This posed significant challenges for Botswana as a landlocked country, as it was impossible to import any materials and components needed for developing the products due to travel restrictions. At the same time, such equipment was required by hospitals in their countries of production, as the virus was spreading very fast. The design team had to rely on equipment and materials that could be sourced locally, even though there were some difficulties since the shops were closed due to lockdown and closed borders. This scenario required the design team to think creatively to contribute to saving lives. Despite all these challenges, the design team successfully delivered on some of their plans.
The feedback from participants on the performance of the designed products was collected through iterative semi-structured interviews. The interviews allowed probing for more detailed responses and clarified some issues with the users. The interview sessions were audio recorded and subsequently transcribed. Responses were coded into categories to find relevant patterns aligned with the product’s performance or lack thereof. All interview data were analysed by inductive thematic content analysis.
3. Development and Testing of Prototypes
An abridged design process of quick research coupled with ideation and rapid and dirty prototyping was adopted. The prototypes were tested as early as in their crude form to get feedback from potential users and experts. A more significant advantage was that the team was multi-disciplinary, including co-creating solutions with the medical doctors at the University Teaching Hospital. It was also a designated COVID-19 hospital. Through this co-creation process with doctors, the team identified products that were a priority and, therefore, were given swift attention. Two products fell into this category of priorities (face shields and ventilators). Face shields were needed immediately, therefore, a more urgent effort was applied to ensure this need was met. The prototyping organisation was coupled with a production line for the face shields with a maximum capacity of 200 units per day.
3.1. Face Shields
Early face shield prototypes focused on the material, size, form, comfort, and usability experiments. The focus was on how an affordable face shield of good quality could be made quickly. Ease of use, cleaning, and optical quality were among the primary considerations. This triggered the search for ISO standards so that the team could identify the best possible material fit for the purpose. The standards particularly helped with the properties of materials. Some of the primary reference standards included ISO 4007:2012 (en)/ISO 4007:2018 (en) Personal protective equipment—Eye and face protection, ANSI/ISEA 287.1-2015—Droplet and Splash Hazard-Face shields (D3), and EN166:2001/BS EN166:2002—7.2.4 Protection against Droplets and Splashes of Liquids (3). In these standards, the visor was of interest to the team on properties concerning materials to produce the face protector/shield and the mounting that holds it to the head. The prescription was that of a single piece of transparent plastic material. With this guidance, the selected material for the shield/visor was PETG film with anti-fog or acrylic XT, with polypropylene or ABS browbands and straps that met the above standards.
Early prototyping relied on using waste pieces of 3 mm acrylic for the browbands and expanded polystyrene for comfort lining (
Figure 1). Although acrylic was found to be very brittle and uncomfortable to wear, it was a highly available material locally. The brittleness of acrylic led the team to explore using ABS for the same purpose (
Figure 1). The face protector was modelled with an A4 size PET used to model the face shields in
Figure 1. These models were tested and refined with feedback from staff at the University teaching hospital, leading to the production of a pre-production prototype.
The pre-production prototype was finalised with a PET face protector, ABS browbands, and an adjustable nylon strap. User feedback included accommodating different head sizes, users with their NK95 masks, and flipping the face protector for various purposes, such as eating and drinking a glass of water (2). One hundred units of this pre-production prototype were donated to the University Teaching Hospital. This was done through a well-organised presentation of handing the products over and demonstrating how to use the product. The purpose of the donation was to get more feedback from prolonged use by the COVID-response staff at the hospital. For example, some of the feedback obtained from participants included the following:
“The strip should be adjusted to accommodate people of different head sizes and those who have plaited their hair” (Participant 4).
“The shield should be designed to avoid a build-up of moisture from breathing, especially on the screen.” (Participant 6).
“The material used for the shield should resist scratches and allow easy cleaning. Otherwise, if the material scratches easily, visibility will be compromised” (Participant 7).
The feedback later informed whether the face protector PET could be retained for the manufactured product, considering its durability, ease of cleaning, and optical quality. The team was looking to produce a product that could be used and reused multiple times.
Feedback from the prolonged use of the pre-production prototype units informed the design team of the following:
The PET was of inferior quality in hardness (resistance to scratching and indentation).
Cleaning made the material almost opaque as it lost its optical quality.
ABS was comfortable to wear as a browband, but confirmation that it was a wearable version was required.
With this feedback, the design team returned to the standards, conforming to the materials for the actual product. Acrylic XT was used for the face protector, and ABS was maintained for the browbands. The thicker Acrylic XT (1.1mm) required a forming technique since the PET film did not require any. Low-cost methods of heating the plastic in the polymer oven at 220 degrees Celsius for 25 s and forming it around a cylindrical surface of 100 mm diameter gave the design team a surface of excellent optical quality and the desired fit for various adult head sizes. The success of this experiment (
Figure 2) meant setting up the production line. It included marking and cutting out with a laser cutting machine, forming, branding (customised versions), joining, cleaning, quality assurance checks, packaging, and distribution. During the project’s tenure, 5512 face shields were manufactured and sold to various organisations and individual customers countrywide. The University donated one hundred and thirty-seven face shields to disadvantaged communities.
The face shield was successfully sold as a commercial product for US$12.00 for adults and US$9.10 for customised children’s sizes. While single-use disposable visors were sold for US$4.55, similar products meant to be used multiple times, which were equally washable and sanitisable, were selling in the range of US$12.14 to US$22.75 in online stores, exclusive of shipping costs. Some products were also produced from 3D printing, which would only sell at lower costs with high production volumes. Since the team’s production approach was upon request, a simple and low-cost production process was necessary, as outlined in this section.
3.2. Ventilation Hood
The ventilation hood was designed to assist COVID patients who can breathe independently but require assistance. The ventilation hood achieves this by creating a volume of pressurised air around the patient’s nose and mouth. This pressurised air then flows into the patient’s respiratory system when they breathe, thereby achieving positive airway pressure (PAP). The ventilator hood was constructed using locally available materials following designs adopted from lessons learned from areas that experienced the pandemic before Botswana [
23]. The main structure of the ventilation hood was made from polyvinyl chloride (PVC) at the base, which allowed closing and opening to fit over the patient’s head and had a provision for attachment of the aspiration and exhaled air. A translucent plastic was used to enable the patient to see through the hood, which was required for claustrophobic patients. A wireframe was used to support the plastic to prevent it from collapsing onto the patient in the event of pressure loss, thereby reducing the chances of suffocation.
Figure 3 shows the ventilation hood prototype undergoing testing at Sir Ketumile Masire Teaching Hospital by healthcare workers.
The tests for the ventilation hood by healthcare workers were positive. As shown in
Figure 3, the ventilation hood provided a continuous positive airway pressure and operated as envisioned. The aspirated air was supplied by a constant positive airway pressure (CPAP) device that maintained the required pressure inside the ventilation hood, regulated by a positive end-expiratory pressure (PEEP) valve, which is a standard off-the-shelf medical device used in respiration therapy.
As determined during testing, healthcare workers suggested improvements to the ventilation hood by using medical-grade materials and more transparent plastic for the hood material. Participants expressed the following:
“…use transparent medical grade plastics for the hood” (Participant 5).
“Simplify the way the hood is mounted on the head” (Participant 1).
“The hood works well, and it just needs minor modifications…” (Participant 2).
However, local efforts to source such materials proved difficult since there was virtually no medical equipment manufacturing industry in the country, and it was impossible to order materials from abroad.
The primary target market was local hospitals, intending them to use the device with the wall oxygen supply lines or with an oxygen concentrator at an estimated cost of US$151.75 per device. The cost estimate included the production of the oxygen treatment hood and off-the-shelve components to build the circuit, one oxygen tube, one PEEP valve, and three viral filters.
3.3. Nebulizer Mask
A nebulizer mask is used to change liquid medicine into fine droplets (in aerosol or mist form) that the patient inhales through a mouthpiece or mask. Nebulizers are used to distribute different types of medicines to patients. Since COVID-19 was associated with breathing problems, a nebulizer distributes medicine and moisture to help control breathing challenges such as wheezing and loosening lung secretions. The design team also produced nebulizers for COVID-19 patients. Therefore, the design team produced nebulizer masks in three sizes: small, medium, and large, for patients who needed such assistance. Design moulds for the small, medium, and large sizes were produced to allow the reproduction of more masks.
Figure 4 shows the nebulizer mask being tested. The feedback from testing included the following:
The average cost of the nebulizer mask was calculated from the records of standard off-the-shelve components used, personnel, and overheads. Vacuum forming was used to manufacture the mask part. The process is cost-effective at low production volumes from 1 to 10,000 units, which was the estimate of the design team for the initial production output, resulting in a sale price of US$6.00 for large adult size, US$5.70 for medium size, and US$4.20 for pediatric sizes. The process also allowed fundamental shape complexity to reduce the cost and time to form the mould.
3.4. Ventilator
A ventilator is a medical device used in respiration therapy that aids a patient who cannot breathe independently. A ventilator is used by critically ill patients with breathing problems or patients that are sedated with an anaesthetic for surgery. Critical COVID-19 patients often require intensive care on a ventilator. As the number of critical patients exceeded intensive care units (ICUs) and commercial ventilators were placed on export embargos by manufacturing countries, developing countries had to find alternatives. To this end, the COVID-19 team undertook the development of a ventilator machine that could be used to assist patients that required breathing assistance.
An open-source ventilator design for a mechanical ventilator using repurposed material was used as a starting point for mechanised respirator bag compression. However, the COVID-19 team was guided by the United Kingdom specifications for rapidly manufactured ventilator systems (RMVS) for use in national health system (NHS) hospitals to assist with COVID-19 patients (MHRA 2020, Williams et al., 2010). The ventilator achieves volume-controlled ventilation by automating a bag valve mask’s mechanical compression and decompression (Ambu bag) using a repurposed motor. The motor speed is controlled in real-time by a microcontroller in a closed-loop control system using sensors. The ventilator allows medical practitioners to control and monitor critical parameters by the various inputs, such as respiration rate (RR), inspiratory-to-expiratory ratio (I:E ratio), and tidal volume (Vt), which are displayed on two displays. The displays are a fixed LCD and an optional Android tablet or mobile phone running the Vector Display application available on Google Play, which shows animated readings of pressure and airflow rate. Critical parameters such as peak inspiratory pressure (PIP), positive end-expiratory pressure (PEEP), tidal volume, and minute volume are displayed and graphed on the screens, allowing the medical practitioners to control and give detailed feedback. The entire breathing circuit comprises bio-compatible materials already used in patient respiration applications. Visual and audio signals were included in the system to alert healthcare workers in the event of a loss of pressure, which signals a breathing circuit malfunction or loss of power.
Figure 5a shows the ventilator under testing and the tablet user interface.
Figure 5b visualises the testing output/performance in a laboratory setting.
Figure 5c shows the test setup performed by the medical practitioners at the University Teaching Hospital.
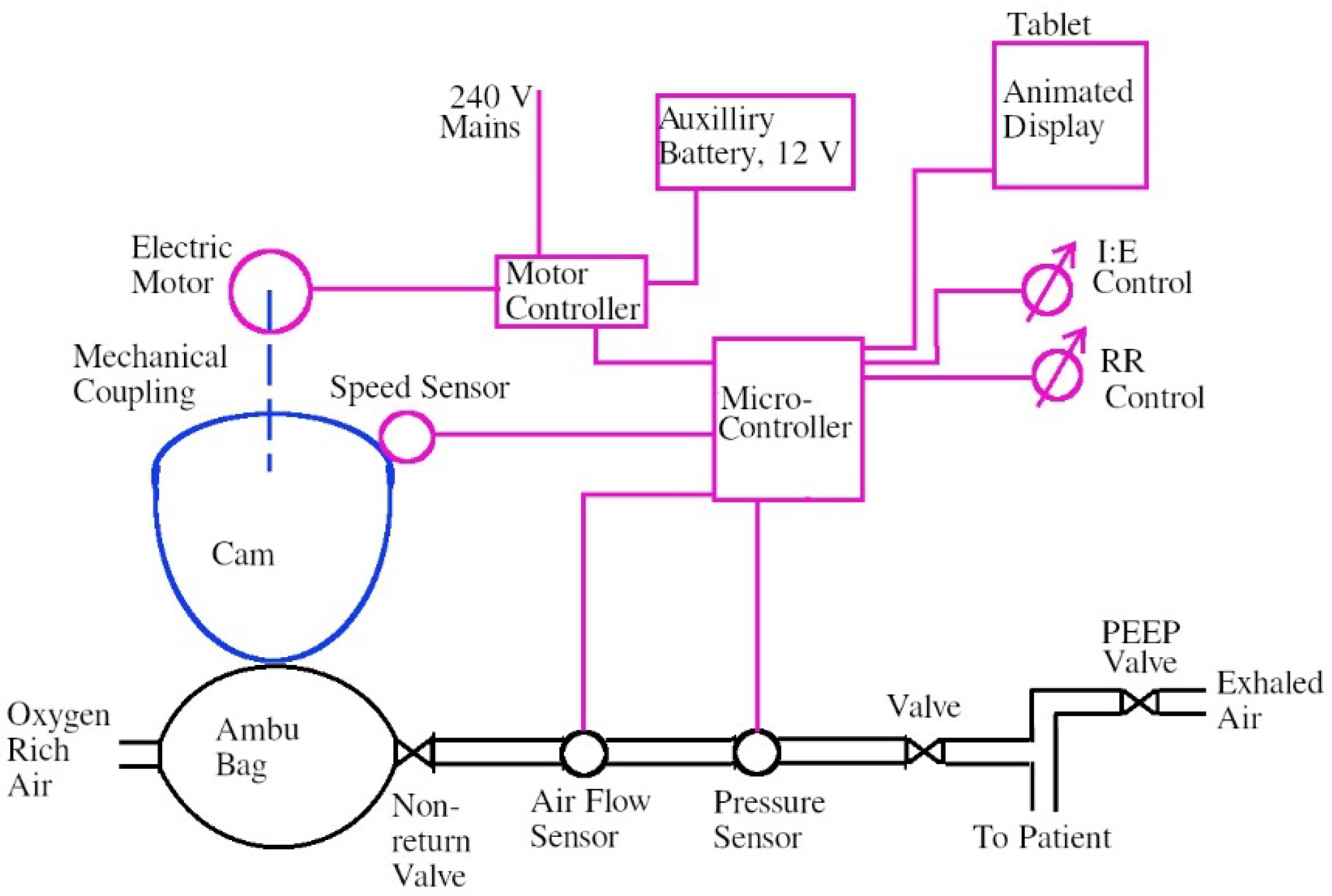
Figure 6 shows a schematic of the operation of the ventilator. An Ambu bag is compressed repeatedly via a cam driven by an electric motor whose rotation speed is controlled by a micro-controller in a closed-loop control system.
A healthcare professional sets the Ambu bag’s rate of compression via a respiration rate (RR control) input. The healthcare also set the inhale-to-exhale rate (I:E control) input. The oxygen-rich air flows to the patient via a series of valves and sensors which monitor the pressure and quantity of air supplied to the patient (minute volume). The pressure in the patient’s lungs is regulated by a standard post-end expiration pressure (PEEP) valve, which is also controlled by a healthcare professional. An animated graphic of the ventilation is displayed on a tablet (Android tablet) along with all critical parameters that the healthcare worker needs to provide assisted ventilation.
Healthcare workers then tested the ventilator at the University Teaching Hospital to determine its functionality. The healthcare workers used a Rigel VenTest 800 Gas Flow analyser (test unit) to test the ventilator prototype.
Table 1 compares the ventilator machine to the flow analyser with different oxygen flow rates of 5, 10, and 15 L/min at 25 breaths per minute.
As shown in the
Table 1 results, the ventilator prototype achieved a peak oxygen concentration of 54% with a 15 L/min supply of oxygen mixed with ambient air in the Ambu bag. The readings on the ventilator and the test equipment were closely matched. The difference in the breath rate can be attributed to calibration errors, as the ventilator was set up with a different load than the test lung. The peak inspiration pressures recorded by the ventilator machine and the test unit were very close, with the most significant difference being only 0.3 cm/H
2O. The tidal volume readings showed the most difference from the test unit due to the inaccurate/slow digital sensor used in the ventilator, which was insufficient for the application. An analog flow sensor would allow more accurate readings that would be close to the readings of the test unit. A second iteration of the ventilator prototype that incorporates the critical feedback produced by the medical practitioners is currently being worked on, with advanced modes and more functionality.
A typical ventilator costs approximately US
$20,488.25–US
$30,352.95 [
24,
25]. A low-cost, easy-to-build version costs US
$75.90–US
$303.50 when produced at higher volumes [
26,
27]. Low-cost ventilators utilising AMBU bags can perform all of the same functions as a conventional commercial ventilator, with a cost of US
$75.90 or less [
28]. The designed low-cost ventilator built with off the shelve components costs between US
$303.50 and US
$379.40. This cost could be relatively higher by 10% to 15% when raw materials and components are imported, yet still be available competitively compared to conventional commercial ventilators.
In summary, prototyping the ventilator was challenging due to the limited availability of components when many research institutions and commercial companies were developing the same product. Some of the critical components of the ventilator were unavailable locally and had to be sourced from abroad, mainly from China. Reduced global travel during the pandemic increased the lead times to procure critical components. Moreover, the costs of shipping were high during the same period. These challenges drastically slowed down the development process.
4. Discussion and Conclusions
The COVID-19 pandemic altered society’s way of life. The crisis also demonstrated research and development’s unique ability to adapt and respond to the most trying times. Most universities developed innovations aimed at lessening the spread of COVID-19, easing the social and economic burden, and safeguarding public health, safety, and remote learning. Universities’ research and development interventions to respond to the pandemic showed untapped, under-utilised human capital. The University of Botswana formed a multi-disciplinary team comprised of industrial designers and mechanical, electrical, electronic, and biomedical engineers to respond to the effects of the pandemic. The design interventions created by the University of Botswana contributed to saving lives, such as developing PPE and ventilators. The innovations made by the University of Botswana show great human creativity and resilience. The innovations were meant to keep Botswana’s front-line workers empowered and protected and give hope to COVID-19 patients. However, the innovations were made under challenging conditions during the lockdown, considering the closure of international borders and the difficulties sourcing the needed electronic components and materials. Universities used different approaches in developing COVID-19 products and services. Some used formal and informal bottom-up or top-down approaches. The University of Botswana team settled for the agile methodology and co-creation design approach, where the design team co-created medical products with medical staff at the University Teaching Hospital. The co-creation process was adopted because it produces impactful solutions that users readily accept, as they would have input in their development.
The COVID-19 pandemic opened a new avenue for the University of Botswana to continue researching and developing other areas affecting society. This makes the University more relevant to society because of its contributions to some of the community’s pressing challenges. The pandemic also showed that universities have adequate human resource capacity to resolve a crisis. Research and development are expensive exercises, and they need to be well resourced. The activity also opened collaborative opportunities with both local and international institutions.
Building on such a foundation from a university in an emerging economy context, it is essential to reflect and devise improved ways to respond to other future pressing scenarios facing Africa, such as energy, food crisis, poverty, climate change, pandemic diseases, increasing water scarcity, low resilience to natural disasters, etc. In developing economies, universities should be proactive and start to embrace more research and development activities to solve local and global challenges. African challenges need local solutions that are sensitive to people’s needs. The same approach used in the COVID-19 intervention could be used for post-pandemic initiatives to improve society’s quality of life. This paves the way for a transition toward a new and better sustainable livelihood. The University of Botswana’s multi-disciplinary team displayed collective capabilities and readiness to deal with present and future national or global emergencies. The lessons learned from the pandemic include the need for innovative, collaborative, cross-disciplinary, and multi-disciplinary approaches to future scenarios, as well as resilience. Universities must review their actions and decisions during the pandemic, focus on successes, and identify and learn from deficiencies [
23]. Such an approach will promote the re-building of a socially equitable, ethically responsible, and more sustainable response to future crises.


 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}