Abstract
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) spreads primarily through respiratory droplets, aerosols, and contaminated surfaces. While high-traffic locations like hospitals and airports have been studied extensively, detecting significant virus levels in aerosols and on environmental surfaces, campus settings remain underexplored. This study focused on two crowded buildings at the University of North Carolina at Charlotte (UNCC). From December 2021 to March 2022, we collected 16 indoor air samples and 201 samples from high-touch surfaces. During the sampling timeframe, 44.82% of surface samples from the Student Union and 28% from the University Recreational Center (UREC) tested positive for the presence of SARS-CoV-2 RNA. Median and average viral RNA copies per swab were higher in UREC (273 and 475) than in Student Union (92 and 269). However, all air samples tested negative. Surface positivity in these high-traffic campus locations was directly correlated with COVID-19 clinical cases in Mecklenburg County. The campus COVID-19 cases, driven by the Omicron wave, peaked a week before the peak detection of surface contamination. These findings underscore the importance of surface hygiene measures and highlight environmental conditions as potential contributors to COVID-19 spread on campuses.
1. Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), responsible for COVID-19 spreading globally since it emerged in late 2019, was first recorded in Wuhan, China [1]. The World Health Organization (WHO) declared it a pandemic in March 2020 [2], and as of February 2024, there were seven million reported deaths and 774 million confirmed COVID-19 cases worldwide [3].
Understanding the transmission mode of SARS-CoV-2 is essential for effective public health strategies to stop its spread. Significant amounts of SARS-CoV-2 RNA have previously been shown to be detectable in air and surface samples [4,5,6,7]. Aerosol inhalation is a major route of SARS-CoV-2 transmission [8,9,10], and indoor environments pose a consistently higher risk due to their enclosed spaces. According to the WHO, saliva or respiratory droplets are secreted in aerosols during activities such as coughing, sneezing, talking, and singing [11]. Viruses in aerosols with a size smaller than 100 μm can remain suspended in the air for three hours [12], increasing the risk of infecting others. Infectious viruses carried by aerosols can travel distances greater than 2 m, leading to their accumulation in indoor space and leading to super-spreading events [13]. For this reason, we wanted to examine the prevalence of detectable SARS-CoV-2 in spaces where students congregate, talk, and exercise in the time period after vaccination was widely available and constraints on the use of indoor spaces had largely been lifted.
Viral particles can be measured directly out of air, but settled material on surfaces can also be both an indicator of viral prevalence and a secondary transmission mode of COVID-19 [14]. Viral RNA has been found on various objects and surfaces, such as cell phones, door handles, chair handles, cupboards, and light switches [15,16]. In hospitals, SARS-CoV-2 RNA has been identified on surfaces including door handles, air vents, bed rails, bathroom areas, personal protective equipment, and hand sanitizer [17,18]. The persistence time varies on different porous and nonporous surfaces. It can last on dry surfaces from 8 to 72 h [6,12,19] and for longer periods on nonporous surfaces [20]. It can remain in an inactive phase on a surface for nine days at room temperature [1]. Individuals can become infected by touching surfaces where an infected person has recently coughed or sneezed [9,21]. Therefore, we included surface measurements in the study as a complementary approach to air sampling.
Studies of SARS-CoV-2 prevalence have been conducted in different indoor environments such as hospital wards, buses, and airport air and surfaces, with limited research conducted in residential areas [22]. However, there is a notable gap in research focusing on the detection of COVID-19 in aerosols and surfaces within indoor spaces at universities. In this study, we specifically investigate SARS-CoV-2 presence in two indoor university spaces, the Popp Martin Student Union (Student Union) and University Recreation Center (UREC), at three critical times in the second year of the pandemic: just before winter break, after winter break, and after spring break. At the end of December 2021, the Omicron viral variant became predominant over the Delta variant and spread rapidly [23]. The first detection of the Omicron variant in North Carolina, on the UNC Charlotte campus [24], coincided with the first week of the sampling period. In-person instruction in the spring semester was delayed until January 24 due to the Omicron wave, but by the end of our sampling period, most on-campus public health measures had again been lifted. The study spans periods of both mandatory and optional mask usage. These buildings experience high foot traffic, resulting in frequent contact with surfaces such as doors, elevators, stair handles, and electric push buttons. Air and surface testing in these areas is essential for identifying potential contamination hotspots and developing effective cleaning protocols.
2. Materials and Methods
2.1. Sampling Sites Description
The study involved two UNC Charlotte buildings: (1) Student Union and (2) University Recreational Center (UREC). Access to both buildings is restricted to UNC Charlotte members. Based on card-swipe access data, the Recreation Center has its highest occupancy in the mornings before 10 AM and evenings from 3 P.M. to 7 P.M. The Student Union has comparatively high occupancy during the daytime from around 12 noon to 04:00 P.M. The sample collection window in both buildings was between 11:30 A.M. and 3:00 P.M. Both the UREC and the Student Union have five floors, with entrances located on the 3rd floor of UREC and the first floor of the Student Union. In UREC, most of the gym equipment is located on the first floor, with additional equipment on the third and fourth floors. The first floor in the Student Union typically experiences the highest occupancy on regular days. Few individuals were observed on the second floor, and there were very few or no people present on the other floors. The estimated daily populations were 2000–3000 people in both buildings on normal days.
2.2. Sample Collection
Sixteen air samples and 201 surface samples were collected from two buildings on nine different days between 3 December 2021 and April 2022 from 11:30 A.M. to 3:00 P.M.
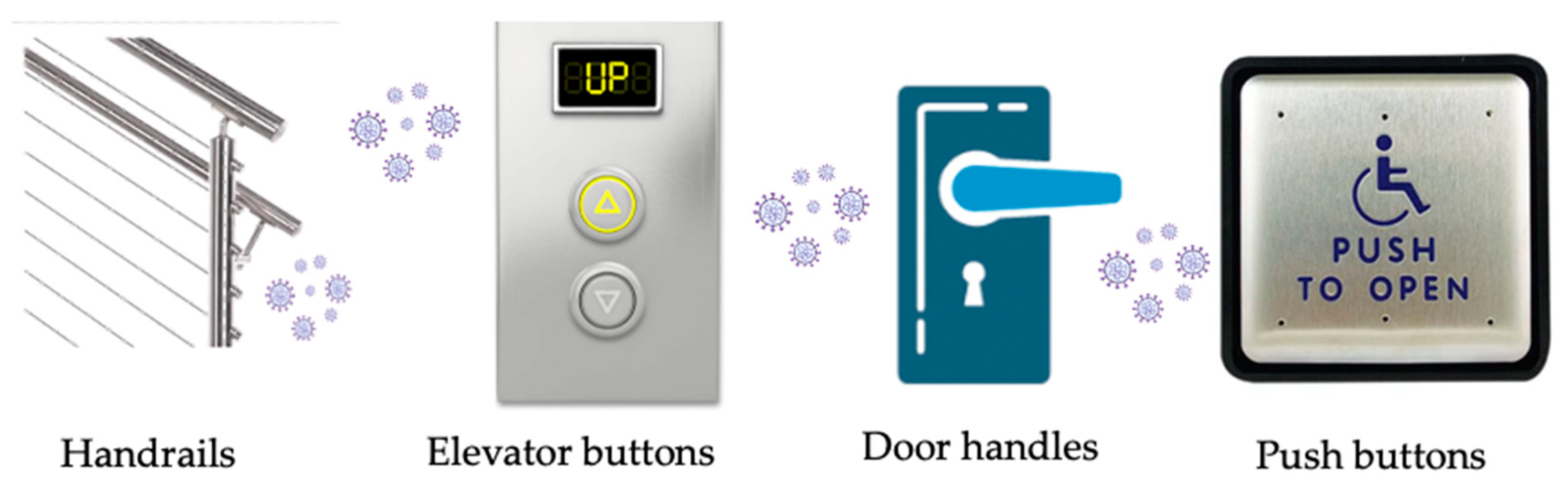
Air samplers were positioned inside the main entrances of both buildings to collect air samples. Surface samples were collected from locations including entrance and exit door handles, elevator buttons, stair handles, and electric push buttons (Figure 1). Seven to nine surface samples were collected from each surface area over 9 sampling days. As per university policy, all surface areas in both buildings undergo disinfection three times each day during the study period, once during each of the three housekeeping shifts.
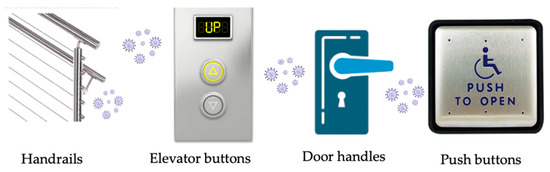
Figure 1.
Schematic representation of high-touch surfaces examined in the study.
- Air sampling
The ACD-200 BobCat Dry Filter Continuous Air Sampler (InnovaPrep, Drexel, MO, USA) was used for this study. The BobCat uses a 52 mm electret filter for collecting samples, eluted with ~7 mL elution fluid. The composition of the elution fluid was water, a low-concentration surfactant (0.075% Tween 20), and a pH buffer. All filter handling and elution were conducted aseptically as per manufacturer instructions [25]. The rechargeable battery was inserted into the ACD Bobcat, and its legs were adjusted upright. The top of the Bobcat was opened on its hinge, the filter cassette was positioned with the filter side down, and the lid was closed. The sampler ran for around 3 h. Afterward, the filter lid was opened, the sample cup was snapped into the cassette, and its lid was secured. The cup was then placed into a sterile Ziplock bag and transported to the laboratory, eluted with foam, and immediately concentrated. The sampler was disinfected with 10% bleach and 70% ethanol before and after each sampling event.
- Surface sampling
The typical method for surface sample collection involves using different cotton swabs due to their high adsorption capacity [4,26,27]. An isohelix buccal swab SK-4S (Boca Scientific, Dedham, MA, USA) was used for this study. A 500 μL solution of DNA/RNA shield buffer (Zymo Research, Irvine, CA, USA) was prepared and stored in 2 mL tubes before sample collection. The swab was then immersed in the solution. After removing the swab from the solution, the surface was rubbed in two different directions within a defined area, the size of which depended on the type of area chosen. The swab was then put back into the solution, with the top side discarded. Swabbing was conducted on 3.61 cm2 area on elevator buttons, >90 cm2 (15 cm × 5–6 cm) on stair handles, >240 cm2 (40 cm × 6 cm) on door handles, and 15.7 cm2 on the electric push button.
2.3. Virus Concentration and RNA Extraction
The Innova Prep CP Select was used to concentrate air samples into a volume of ~500 µL. RNA was extracted from 200 µL of the concentrated sample using the QIAamp Viral Mini Kit (Qiagen, Valencia, CA, USA), following the manufacturer’s protocol. Then, 60 µL of RNA was then eluted with AVE buffer and stored at −80 °C until quantification. Surface samples were extracted without concentration, as the initial volume of buffer solution was 500 µL. RNA extraction was performed using the Zymo Quick-RNA Viral Kit (Zymo Research #R1034), and the extracted RNA was stored at −80 °C until quantification. All sample processing was conducted in a Class II Biosafety Cabinet (BSC II).
2.4. Virus Quantification
N1 primers and a probe recommended by the United States Center for Disease Control (CDC) were used [28] to amplify the SARS-CoV-2 N1 target. RT-qPCR was carried out for 44 cycles in a 20 μL reaction mixture using the TaqMan universal reaction mixture. The one-step RT-qPCR reaction mixtures contained 10 μL of iTAQ universal reaction mix, 0.5 μL of iScript reverse transcriptase, 500 nM forward primer, 500 nM reverse primer, 250 nM probe, 5 μL template RNA, and nuclease-free water per reaction. The RT-qPCR thermal cycling conditions consisted of an initial step at 25 °C for 2 min, followed by a reverse transcription step at 50 °C for 15 min, an initial denaturation at 95 °C for 2 min, and then 44 cycles of denaturation at 95 °C for 3 s and annealing at 55 °C for 30 s [29].
Bovine coronavirus (BcoV) was used as a standard to determine the process recovery of viral detection [30]. A known concentration of BcoV was spiked into samples prior to running the RNA extraction. The one-step RT-qPCR reaction mixtures for BcoV contained 10 μL of iTAQ universal reaction mix, 0.5 μL of iScript reverse transcriptase, 600 nM forward and reverse primer, 250 nM probe, 0.2 μL template RNA, and nuclease-free water. The thermal conditions included incubation at 55 °C for 30 min, followed by an initial denaturation step at 95 °C for 2 min. Subsequently, there were 39 cycles of denaturation at 95 °C for 15 s and annealing at 55 °C for 1 min [31]. The initial concentrations of the SARS-CoV-2 stock solution and BcoV were 8.8 × 105 copies/μL and 1.04 × 105 copies/μL, respectively. All samples for the qPCR run were performed in triplicate.
2.5. Quality Control, Limit of Detection and Statistical Analysis
Nuclease-free water (NFW) was used as the negative extraction control during RNA extraction, and a no-template control (NTC) was included for the qPCR assay. A series of six standards with 10-fold dilutions, each in triplicate, was used to create the standard curves for the SARS-CoV-2 and the BcoV assays. The limit of detection (LOD) was determined through serial 10-fold dilutions of SARS-CoV-2 RNA up to the 6th standard. Starting from the 7th standard, five additional 3-fold dilutions were conducted, each replicated six times. The LOD was recorded if 60% or more of the replicates were quantified [32].
The calculation for BCoV recovery Is as follows
A Pearson correlation test was conducted to examine the correlation between surface samples and COVID-19 cases in Mecklenburg County.
3. Results
3.1. Standard Curve and Limit of Detection
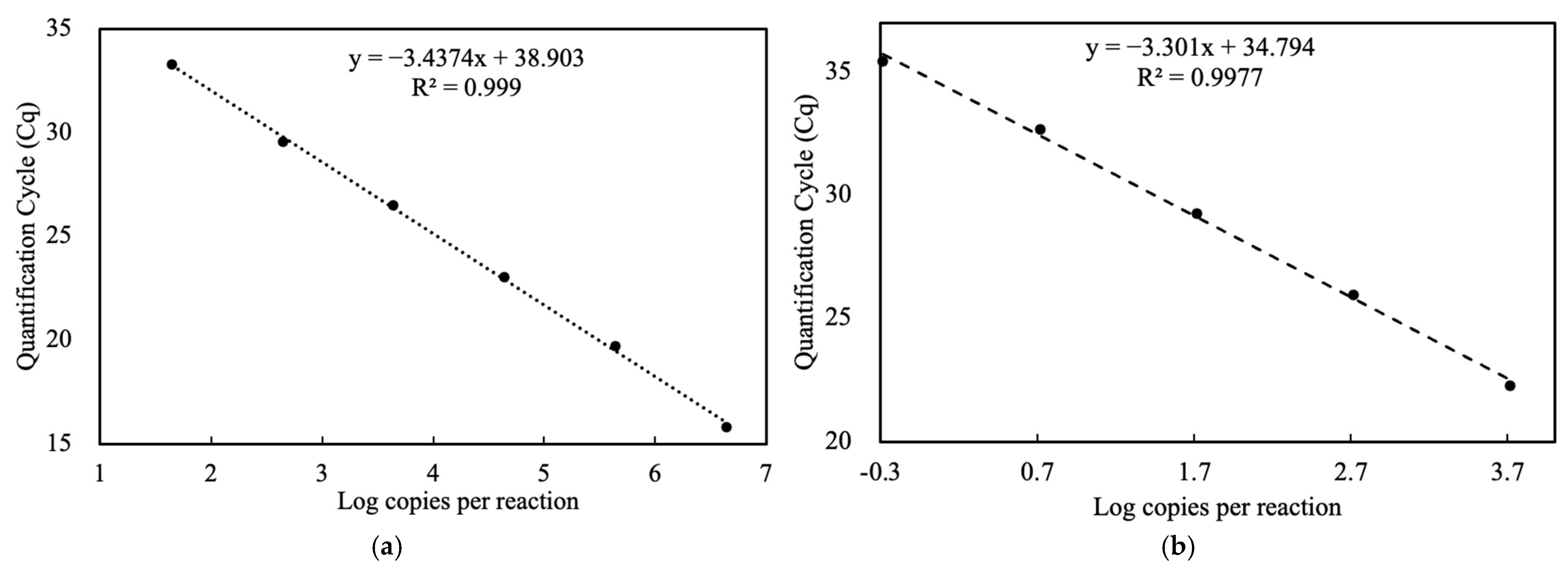
The standard run for SARS-CoV-2 was performed four times, and the average was calculated for all runs to plot a single standard curve (Figure 2a). The limit of detection (LOD) was determined to be 37.80 quantification cycle (Cq) and 2.3 copies/μL. The qPCR efficiency for SARS-CoV-2 was 95.39%, and for BcoV, it was 100.88%. The slope was −3.44 for SARS-CoV-2 and −3.3 for BcoV, with an R2 value of 0.99 (Figure 2b).
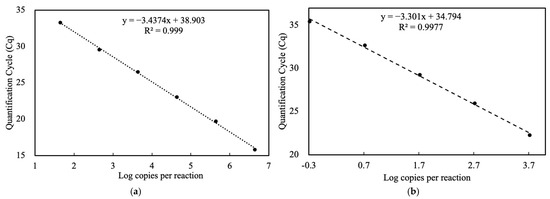
Figure 2.
Standard curve. (a) SARS-CoV-2; (b) BCoV.
3.2. SARS-CoV-2 Detection in Air and High-Touched Surfaces
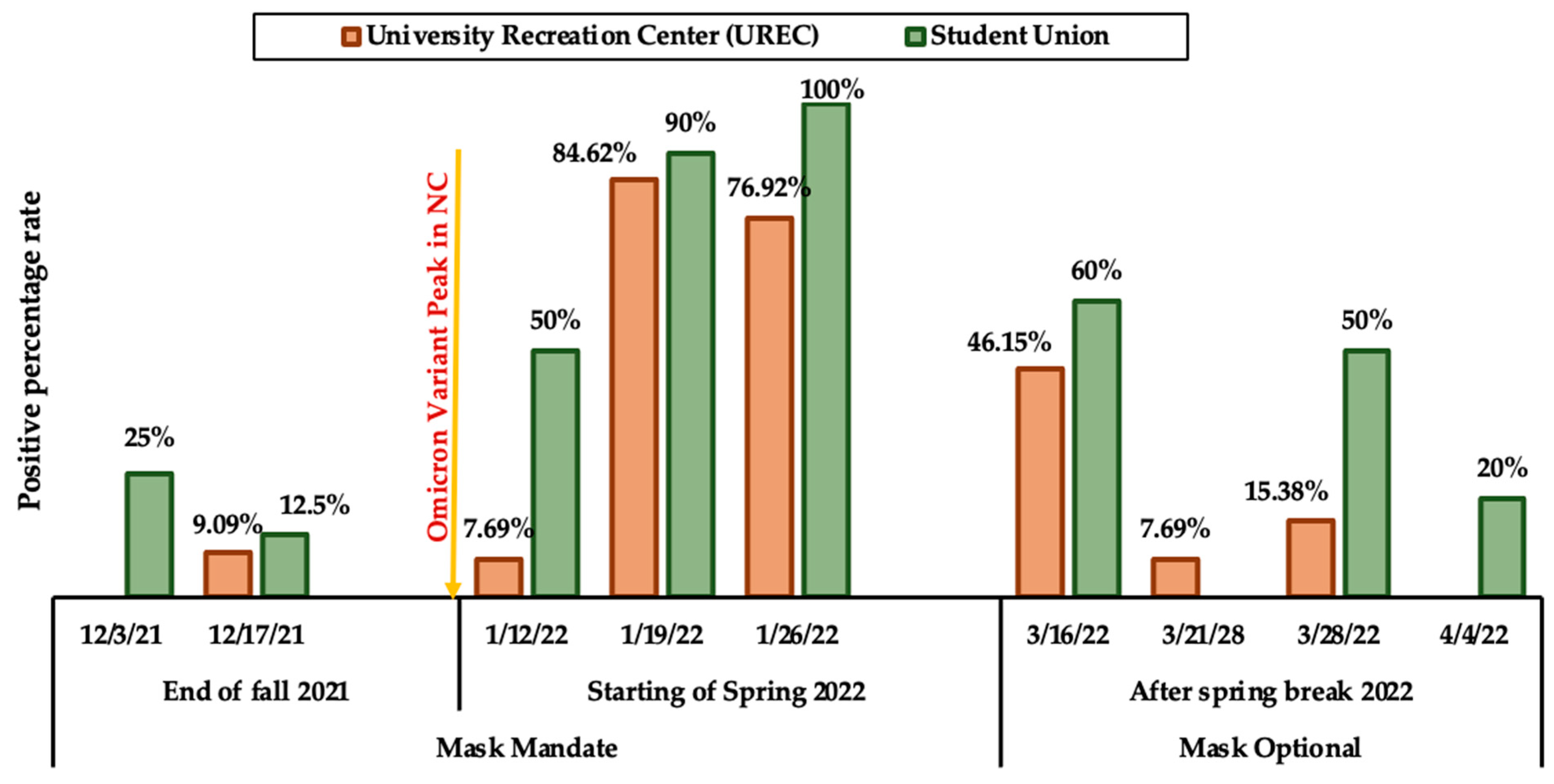
In our study, all 16 air samples tested negative, leading to no further analysis. Among the 201 surface samples, 113 were from UREC, and 88 were from the Student Union. Specifically, 32 (28.3%) samples from UREC and 40 (45.45%) samples from the Student Union tested positive. Notably, during the spring semester in January 2022, the highest positivity rates were observed: 77% to 85% in UREC and 90% to 100% in the Student Union just after the Omicron variant wave (Figure 3). Subsequently, positive rates gradually declined during the optional mask period.
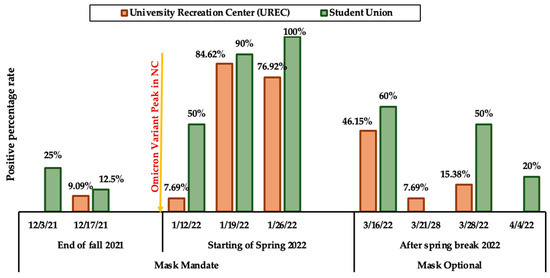
Figure 3.
Positive percentage rate based on the dates and mask options Student Union; n = 10 for all dates except n = 8 for 12-03-21; UREC; n = 13 for all dates except, n = 11 on 12-03-21, 12-17-21.
The high-touch surfaces selected for this research included handrails, elevator buttons, door handles, and push buttons in the Student Union and UREC (Figure 3). All the high-touch surfaces showed positive results at least 2 to 6 times, except for the 2nd-floor elevator buttons in UREC. In the Student Union, the maximum percentage of positive surface samples, with rates above 50%, were as follows: 55.56% for handrails, 66.67% for 1st-floor elevator buttons, 62.5% for exit push buttons, and 50% for entry push buttons. In UREC, the highest percentage of positive samples was 57% for exit push buttons, while the rates for the other surfaces were below 35% (Table 1).

Table 1.
Sampling frequency and positive percentage rate (%) for surface types.
3.3. Copies Per Swabbing Area
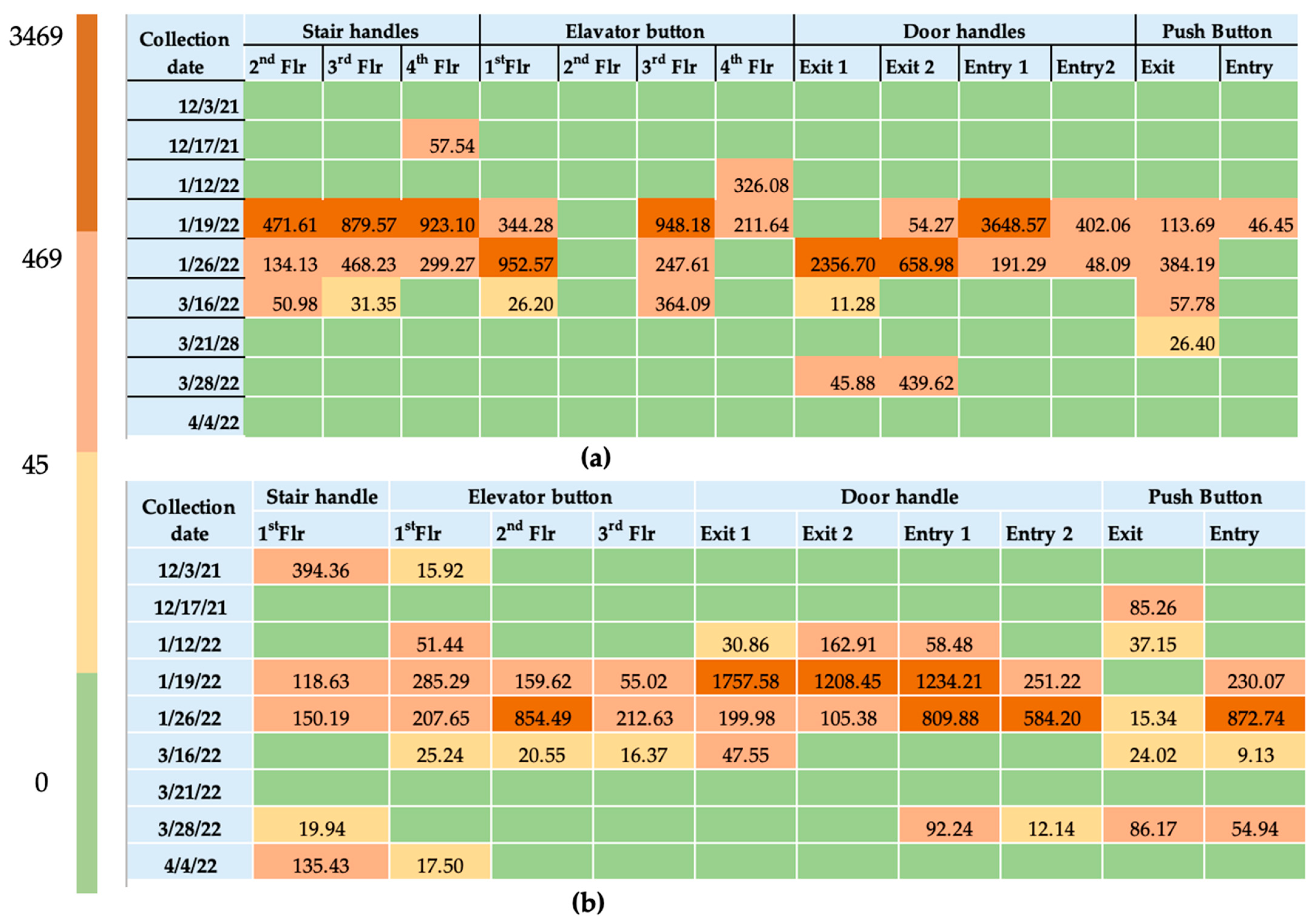
The copies per swabbing area were calculated from the Cq value using the given standard curve (Figure 1). Specifically, a Cq value less than 33 represents a concentration greater than 10.43 copies/μL, or 469.38 copies per swab. If the Cq value falls between 33 and 36.5, it indicates a concentration lower than 10.43 copies/μL and greater than 1 copy/μL, corresponding to 45 copies per swabbing area. A Cq value exceeding 36.5 indicates a concentration of less than 1 copy/μL, corresponding to 45 copies per swabbing area.
Cq values of SARS-CoV-2 ranged from 31.03 to 38.88 for the Student Union and from 29.94 to 42.91 for UREC. Some of the samples were detected below the limit of detection. Copies per swabbing area for both buildings are represented in the heat maps (Figure 4). The highest concentration was observed on 1/19/22 while the lowest to no concentrations were noted on 3/21/22 in both buildings. The concentration ranged from 9.13 copies per swab to 3648.57 copies per swab. On average, BCoV recovery was found to be 21.64% ± 11.88% across 15 surface samples, with a median of 19.80%. The highest recovery percentage observed was 49%, while the lowest was 9% (Equation (1)).
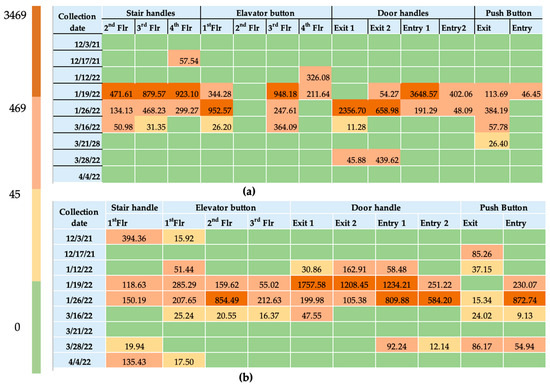
Figure 4.
Copies per swabbing area on four different surfaces (a) UREC; (b) Student Union (Flr = Floor).
4. Discussion
SARS-CoV-2 was measured in indoor air and high-touch surfaces in two different buildings of the U.S. University. The study demonstrates that the university environment successfully identifies and isolates SARS-CoV-2 RNA. The standard curve for SARS-CoV-2 exhibited a high level of precision, reflected by a low limit of detection (LOD) of 37.80 Cq. Both SARS-CoV-2 and BCoV qPCR assays demonstrated efficient performance with high qPCR efficiencies of 95.39% and 100.88%. All parameters of the standard curve, including the limit of detection (LOD), qPCR efficiency, slope, and R2 value, fall within the specified range for qPCR, confirming the accuracy and reliability of the assay [33]. However, the concentration of some samples was below the LOD of the qPCR assay. Other studies also included data below the LOD in their analyses [34]. Based on a review of 51 studies using RT-qPCR on fomite transmission, cycle threshold values of SARS-CoV-2 on surfaces ranged from 20.8 to 44.1, and positive tests ranged from 0.5% to 75% [35].
BCoV was spiked for the processing control because it is a surrogate of human coronavirus. BCoV, like SARS-CoV-2, is an enveloped virus belonging to the Coronaviridae family [36]. It exhibits similar survival dynamics and trends on various surfaces as SARS-CoV-2 [37] and has been recommended by previous research for the process control [38]. In this study, the recovery efficiency of BCoV from surface samples was 21.64%, which is slightly higher than the 16% reported in previous studies on metal surfaces [39,40]. This may be because in previous research, BCoV was spiked onto surfaces before swabbing, whereas in our study, it was spiked after swabbing.
SARS-CoV-2 RNA was not detected in air samples, possibly due to the limited sampling period. Extending the sampling duration could enhance the effectiveness of capturing RNA in the air. The virus’s limited persistence could also influence this in the air compared to surface samples [12]. The absence of a standardized method for collecting air samples for virological investigation has also been noted [26]. When sneezing or coughing, the virus may be more dispersed and diluted in the larger volume of ambient air, reducing the probability of direct detection. Though indoor air may not show detectable COVID-19 contamination, surface analysis can reveal its presence because larger droplets settle on surfaces rather than remaining suspended in the air, leading to surface contamination [41].
In the present study, we found that SARS-CoV-2 RNA was abundantly detected on surfaces, despite a 3× daily sanitization regime. Surfaces may be a better proxy for the detection of increasing viral infection in shared environments than air sampling. This finding aligns with the outcomes of other comparative studies of surface and air sampling in hospital and public transit contexts. A study [42] of SARS-CoV-2 detection on surfaces and indoor air of subway trains and public buses revealed higher positivity (23 out of 58) compared to ambient air inside the vehicles (3 out of 12). Interestingly, two other studies found no SARS-CoV-2 RNA in the air, even when air samplers were placed near COVID-19 patients [26,43]. Meanwhile, a hospital study in Iran reported a 41% detection rate for COVID-19 in indoor air and 32% in surface samples. Samplers placed within two meters of the patient’s bed yielded positive results, while those placed 2 to 5 m away were negative [44]. Cheng et al. [26] swabbed frequently touched environmental surfaces near 21 patients, revealing that 19 (5.0%) of them tested positive by RT-PCR. Zhou et al. [27] found viral RNA on hospital surfaces at a rate of 52.3% (114 of 218 samples) and in air samples at 38.7% (14 of 31 samples) in COVID wards.
The detection rates of SARS-CoV-2 varied between the UREC and the Student Union buildings due to differences in sample timing, as discussed in the Section 2. The peak of surface detection in this study aligns with holiday gatherings and travel, highlighting the intermediate impact of social interactions on the prevalence of SARS-CoV-2 in campus environments. A significant factor affecting the surface contamination levels was the emergence of the Omicron variant.
While we did not plan the study to track Omicron infections specifically, the first detection of an Omicron variant in a COVID-19 case from UNC Charlotte’s student health center was reported on 10 December 2021, with the sample having been collected on 1 December, after students returned from Thanksgiving break [24]. In January 2022, the global daily average of COVID-19 cases reached an all-time high, including in the USA. However, SARS-CoV-2 detection rates on campus declined by March 2022, when face masks were optional in the United States [45]. This decrease may be attributed to several factors, such as increased vaccination rates, the development of natural immunity, and improved ventilation systems in public spaces.
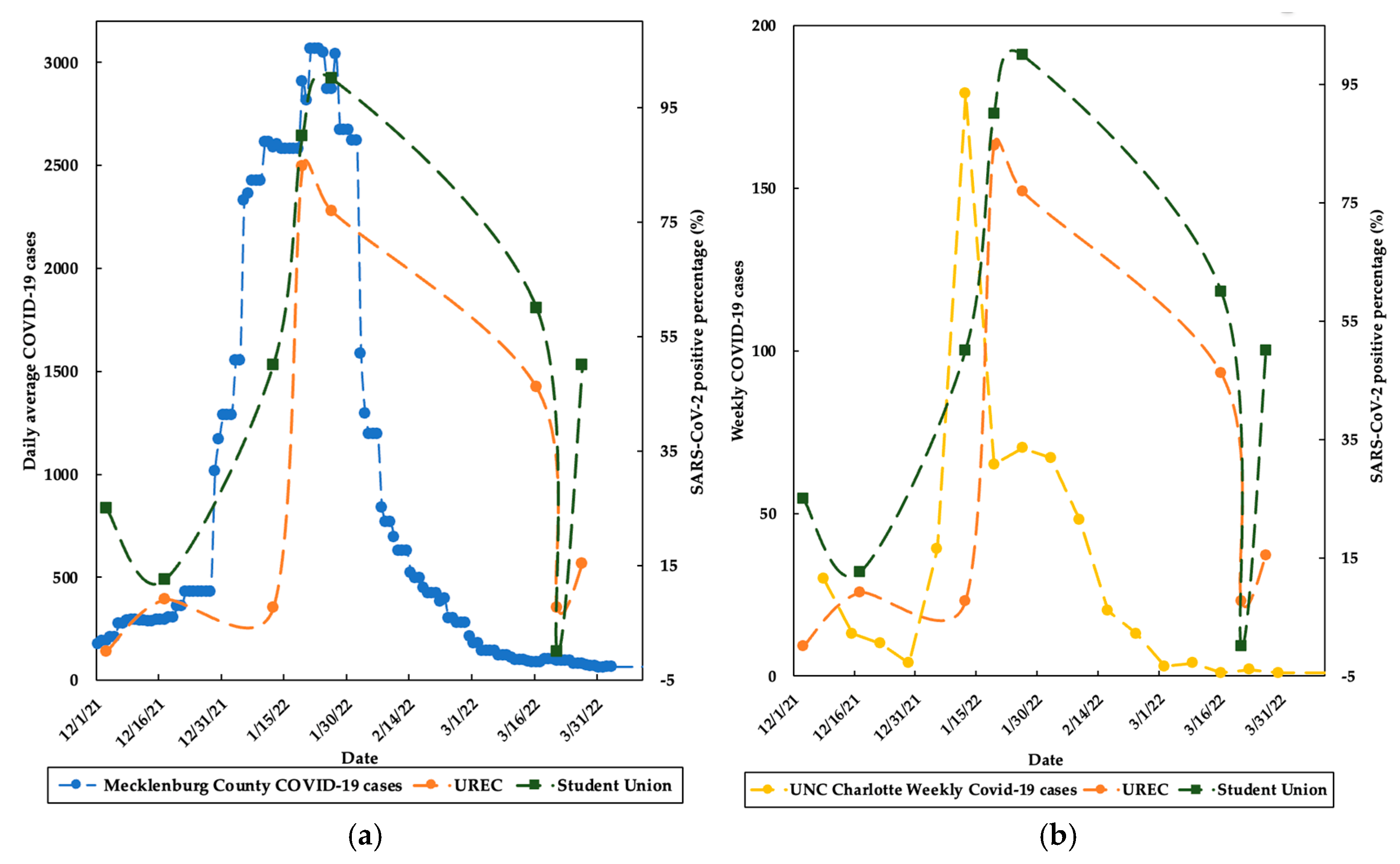
Furthermore, the data obtained from COVID-19 case numbers in Mecklenburg County correlated with the study data of the Student Union (r = 0.78) and UREC (r = 0.68). Surface positivity rates on campus declined more slowly than COVID-19 cases in Mecklenburg County (Figure 5a). The peak of campus COVID-19 cases, driven by the Omicron wave, occurred in January 2022, nearly a week before the peak detection of surface contamination data (Figure 5b).
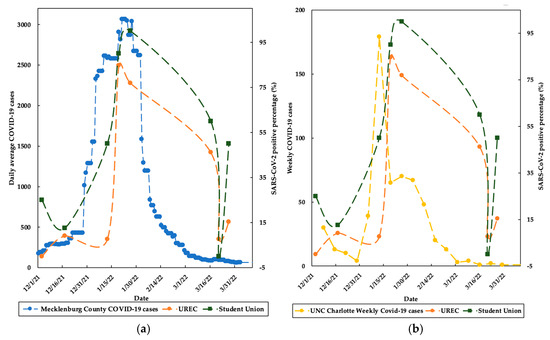
Figure 5.
Relationship between research data and (a) Mecklenburg County COVID-19 clinical cases [46]; (b) UNC Charlotte weekly COVID-19 clinical cases.
Consistent positive results on all selected high-touch surfaces indicate that every surface poses an equal risk of transmitting SARS-CoV-2. During the data collection period, surfaces were cleaned once per cleaner shift and three times per day, though the timing was inconsistent. Despite generally uninterrupted cleaning, we intentionally disrupted the process only twice to ensure the surfaces were swabbed before being wiped with disinfectant. Viral RNA was detected despite three rounds of cleaning in both buildings, suggesting that high-touch surfaces should be more focused while cleaning and should be cleaned based on the occupancy of the people. The SARS-CoV-2 concentrations on surfaces ranged from 9.13 copies/swab to 3.6 × 103 copies/swab, with some samples exceeding LOD. Research in a Scottish COVID ward revealed that most samples fell below assay detection limits, with maximum concentrations of 1.7 × 103 genomic copies/m3 in air and 1.9 × 10⁴ copies/swab on surfaces [34]. A similar study in Italy found 24.3% of 37 swab samples positive for viral RNA, with contamination particularly noted on medical equipment, shelves, door handles, and bed rails [17].
Although not all indoor surfaces are frequently touched, it is essential to care for and properly disinfect high-touch surfaces due to their higher risk of indirect COVID-19 transmission. SARS-CoV-2 contamination on surfaces within a university setting can be reduced by implementing several key measures. Increasing the frequency and thoroughness of cleaning high-touch surfaces, particularly during peak usage times, can be beneficial. Microbe levels could be reduced by 90 to 99% depending on the cleaning methods, the type of cleaner used, the cleaning procedure, and how well the cleaning is performed [47,48,49]. Therefore, a combination of proven disinfectants, such as ethanol (62% to 71%) and bleach, is effective at reducing viral loads [50]. Incorporating UV-C LED devices with specific wavelengths for surface disinfection can further aid in inactivating the virus without causing harm to humans [51]. Additionally, promoting good hygiene practices among students and staff, including regular handwashing, the use of hand sanitizers, and avoiding touching surfaces with the bare hand, is important. By considering these measures and adapting practices based on ongoing data and emerging variants, universities can effectively mitigate the risk of SARS-CoV-2 transmission from surfaces and enhance overall campus safety.
This study has several limitations that may have influenced the results. The air samplers were operated for only around 3 h, which may not have been sufficient to capture SARS-CoV-2 particles effectively. Extending the sampling duration in future studies could potentially increase detection rates. Additionally, the disinfection schedules of the buildings were inconsistent; disinfection occurred three times daily, once during each of the three housekeeping shifts, but the exact times were not fixed. While we ensured that disinfection did not occur immediately before or during the sampling periods, future studies could address this limitation by implementing controlled disinfection timing to reduce potential biases.
Resource constraints were a limiting factor in the study. Only two air samplers were available for the study, and they were positioned at the main entrances of each building where foot traffic was highest. Additional samplers on different floors could provide a more comprehensive understanding and potentially detect SARS-CoV-2 in other areas. Other potential influencing factors, such as population density, temperature, and ventilation conditions, were not considered in this analysis. The natural flow of people in the area was beyond our control, which could introduce variability and complexity into the results. Future research could incorporate these additional factors to provide a more detailed and comprehensive analysis.
5. Conclusions
The present research emphasizes the critical importance of SARS-CoV-2 surveillance within indoor campus environments, focusing on aerosol and high-touch surfaces, as campuses, often crowded, can potentially serve as hotspots for viral transmission. Despite negative detections in indoor air, the substantial positive findings on high-touch surfaces of UREC 28.3% and 45.45% from the Student Union were recorded. The research findings indicate an equal risk of transmission from all selected high-touched surfaces. The findings of this study contribute valuable insights for policymakers, healthcare professionals, and institutions aiming to mitigate the risk of COVID-19 transmission in high-traffic indoor environments.
Author Contributions
Conceptualization, investigation, methodology, formal analysis, data visualization, data curation, writing—original draft, N.K.; investigation, methodology; L.R.B. methodology, formal analysis; M.A.I.J. conceptualization, project administration, supervision, funding acquisition, writing—review and editing, C.G.; resources, conceptualization, project administration, writing—review and editing, J.S.; conceptualization, funding acquisition, project administration, supervision, writing—review and editing, M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Acknowledgments
We would like to thank the Division of Research, at UNC Charlotte, for supporting this project. We also express our sincere appreciation to Rachel Noble, Thomas Clerkin and Denene Blackwood, at UNC-IMS for their valuable support in developing the methodology whenever needed. We extend our gratitude to Morgan Meehan and Jim Walczyk for their excellent coordination and for facilitating sample collection at the Student Union and UREC during sampling days. We acknowledge Angelica Martins and the COVID-19 testing team at UNC Charlotte for providing the COVID-19 case data. We would also thank Reyhaneh Nouri for her assistance with initial sample collection and the wastewater monitoring team for their contributions.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report, 73. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200402-sitrep-73-covid-19.pdf (accessed on 12 August 2022).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://data.who.int/dashboards/covid19/cases?n=c (accessed on 25 February 2024).
- Dargahi, A.; Jeddi, F.; Vosoughi, M.; Karami, C.; Hadisi, A.; Mokhtari, S.A.; Ghobadi, H.; Alighadri, M.; Haghighi, S.B.; Sadeghi, H. Investigation of SARS CoV-2 virus in environmental surface. Environ. Res. 2021, 195, 110765. [Google Scholar] [CrossRef] [PubMed]
- Ziarani, F.R.; Tahamtan, A.; Safari, H.; Tabarraei, A.; Shahamat, Y.D. Detection of SARS-CoV-2 genome in the air, surfaces, and wastewater of the referral hospitals, Gorgan, north of Iran. Iran. J. Microbiol. 2022, 14, 617. [Google Scholar]
- Aytoğan, H.; Ayintap, E.; Yılmaz, N.Ö. Detection of coronavirus disease 2019 viral material on environmental surfaces of an ophthalmology examination room. JAMA Ophthalmol. 2020, 138, 990–993. [Google Scholar] [CrossRef]
- Tan, K.S.; Ang, A.X.Y.; Tay, D.J.W.; Somani, J.; Ng, A.J.Y.; Peng, L.L.; Chu, J.J.H.; Tambyah, P.A.; Allen, D.M. Detection of hospital environmental contamination during SARS-CoV-2 Omicron predominance using a highly sensitive air sampling device. Front. Public Health 2023, 10, 1067575. [Google Scholar] [CrossRef] [PubMed]
- Morawska, L.; Cao, J. Airborne transmission of SARS-CoV-2: The world should face the reality. Environ. Int. 2020, 139, 105730. [Google Scholar] [CrossRef]
- Morawska, L.; Tang, J.W.; Bahnfleth, W.; Bluyssen, P.M.; Boerstra, A.; Buonanno, G.; Cao, J.; Dancer, S.; Floto, A.; Franchimon, F. How can airborne transmission of COVID-19 indoors be minimised? Environ. Int. 2020, 142, 105832. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Li, Y.; Zhang, A.L.; Wang, Y.; Molina, M.J. Identifying airborne transmission as the dominant route for the spread of COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 14857–14863. [Google Scholar] [CrossRef]
- World Health Organization. Cleaning and Disinfection of Environmental Surfaces in the Context of COVID-19: Interim Guidance; WHO, Ed.; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Miller, S.L.; Nazaroff, W.W.; Jimenez, J.L.; Boerstra, A.; Buonanno, G.; Dancer, S.J.; Kurnitski, J.; Marr, L.C.; Morawska, L.; Noakes, C. Transmission of SARS-CoV-2 by inhalation of respiratory aerosol in the Skagit Valley Chorale superspreading event. Indoor Air 2021, 31, 314–323. [Google Scholar] [CrossRef]
- Karia, R.; Gupta, I.; Khandait, H.; Yadav, A.; Yadav, A. COVID-19 and its Modes of Transmission. SN Compr. Clin. Med. 2020, 2, 1798–1801. [Google Scholar] [CrossRef] [PubMed]
- Banik, R.K.; Ulrich, A. Evidence of short-range aerosol transmission of SARS-CoV-2 and call for universal airborne precautions for anesthesiologists during the COVID-19 pandemic. Anesth. Analg. 2020, 131, e102–e104. [Google Scholar] [CrossRef] [PubMed]
- Bloise, I.; Gómez-Arroyo, B.; García-Rodríguez, J. Detection of SARS-CoV-2 on high-touch surfaces in a clinical microbiology laboratory. J. Hosp. Infect. 2020, 105, 784–786. [Google Scholar] [CrossRef] [PubMed]
- Razzini, K.; Castrica, M.; Menchetti, L.; Maggi, L.; Negroni, L.; Orfeo, N.V.; Pizzoccheri, A.; Stocco, M.; Muttini, S.; Balzaretti, C.M. SARS-CoV-2 RNA detection in the air and on surfaces in the COVID-19 ward of a hospital in Milan, Italy. Sci. Total Environ. 2020, 742, 140540. [Google Scholar] [CrossRef]
- Chia, P.Y.; Coleman, K.K.; Tan, Y.K.; Ong, S.W.X.; Gum, M.; Lau, S.K.; Lim, X.F.; Lim, A.S.; Sutjipto, S.; Lee, P.H. Detection of air and surface contamination by SARS-CoV-2 in hospital rooms of infected patients. Nat. Commun. 2020, 11, 2800. [Google Scholar] [CrossRef]
- Carraturo, F.; Del Giudice, C.; Morelli, M.; Cerullo, V.; Libralato, G.; Galdiero, E.; Guida, M. Persistence of SARS-CoV-2 in the environment and COVID-19 transmission risk from environmental matrices and surfaces. Environ. Pollut. 2020, 265, 115010. [Google Scholar] [CrossRef]
- Chin, A.; Chu, J.; Perera, M.; Hui, K.; Yen, H.; Chan, M.; Peiris, M.; Poon, L. Stability of SARS-CoV-2 in different environmental conditions. Lancet Microbe 2020, 1, e10. [Google Scholar] [CrossRef]
- Ren, S.-Y.; Wang, W.-B.; Hao, Y.-G.; Zhang, H.-R.; Wang, Z.-C.; Chen, Y.-L.; Gao, R.-D. Stability and infectivity of coronaviruses in inanimate environments. World J. Clin. Cases 2020, 8, 1391. [Google Scholar] [CrossRef]
- Correia, G.; Rodrigues, L.; Afonso, M.; Mota, M.; Oliveira, J.; Soares, R.; Tomás, A.L.; Reichel, A.; Silva, P.M.; Costa, J.J. SARS-CoV-2 air and surface contamination in residential settings. Sci. Rep. 2022, 12, 18058. [Google Scholar] [CrossRef]
- DeWitt, M.E.; Tjaden, A.H.; Herrington, D.; Schieffelin, J.; Gibbs, M.; Weintraub, W.S.; Sanders, J.W.; Edelstein, S.L. COVID-19 symptoms by variant period in the North Carolina COVID-19 community research partnership, North Carolina, USA. Emerg. Infect. Dis. 2023, 29, 207. [Google Scholar] [CrossRef]
- Wright, W.; Sessoms, B. First Reported Positive Case of COVID Omicron Variant in NC Is Tied to College Student. Available online: https://www.charlotteobserver.com/news/coronavirus/article256492116.html (accessed on 12 December 2021).
- InnovaPrep LLC. ACD-200 Bobcat Dry Filter Air Sampler User’s Guide. 2012. Available online: https://photos.labwrench.com/equipmentManuals/19439-6723.pdf (accessed on 23 May 2022).
- Cheng, V.C.-C.; Wong, S.-C.; Chan, V.W.-M.; So, S.Y.-C.; Chen, J.H.-K.; Yip, C.C.-Y.; Chan, K.-H.; Chu, H.; Chung, T.W.-H.; Sridhar, S. Air and environmental sampling for SARS-CoV-2 around hospitalized patients with coronavirus disease 2019 (COVID-19). Infect. Control Hosp. Epidemiol. 2020, 41, 1258–1265. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Otter, J.A.; Price, J.R.; Cimpeanu, C.; Meno Garcia, D.; Kinross, J.; Boshier, P.R.; Mason, S.; Bolt, F.; Holmes, A.H. Investigating severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) surface and air contamination in an acute healthcare setting during the peak of the coronavirus disease 2019 (COVID-19) pandemic in London. Clin. Infect. Dis. 2021, 73, e1870–e1877. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed]
- CDC, C. Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel: CDC-006-00019, Revision: 05 [Internet]; CDC/DDID/NCIRD/Division of Viral Disease: Atlanta, GA, USA, 2020. [Google Scholar]
- Gibas, C.; Lambirth, K.; Mittal, N.; Juel, M.A.I.; Barua, V.B.; Brazell, L.R.; Hinton, K.; Lontai, J.; Stark, N.; Young, I. Implementing building-level SARS-CoV-2 wastewater surveillance on a university campus. Sci. Total Environ. 2021, 782, 146749. [Google Scholar] [CrossRef]
- Juel, M.A.I.; Stark, N.; Nicolosi, B.; Lontai, J.; Lambirth, K.; Schlueter, J.; Gibas, C.; Munir, M. Performance evaluation of virus concentration methods for implementing SARS-CoV-2 wastewater based epidemiology emphasizing quick data turnaround. Sci. Total Environ. 2021, 801, 149656. [Google Scholar] [CrossRef]
- Gonzalez, R.; Curtis, K.; Bivins, A.; Bibby, K.; Weir, M.H.; Yetka, K.; Thompson, H.; Keeling, D.; Mitchell, J.; Gonzalez, D. COVID-19 surveillance in Southeastern Virginia using wastewater-based epidemiology. Water Res. 2020, 186, 116296. [Google Scholar] [CrossRef]
- Bio-Rad. Real-Time PCR Applications Guide. Available online: https://www.bio-rad.com/webroot/web/pdf/lsr/literature/Bulletin_5279.pdf (accessed on 6 December 2022).
- Loh, M.; Yaxley, N.; Moore, G.; Holmes, D.; Todd, S.; Smith, A.; Macdonald, E.; Semple, S.; Cherrie, M.; Patel, M. Measurement of SARS-CoV-2 in air and on surfaces in Scottish hospitals. J. Hosp. Infect. 2023, 133, 1–7. [Google Scholar] [CrossRef]
- Onakpoya, I.J.; Heneghan, C.J.; Spencer, E.A.; Brassey, J.; Plüddemann, A.; Evans, D.H.; Conly, J.M.; Jefferson, T. SARS-CoV-2 and the role of fomite transmission: A systematic review. F1000Research 2021, 10, 233. [Google Scholar] [CrossRef] [PubMed]
- LaTurner, Z.W.; Zong, D.M.; Kalvapalle, P.; Gamas, K.R.; Terwilliger, A.; Crosby, T.; Ali, P.; Avadhanula, V.; Santos, H.H.; Weesner, K. Evaluating recovery, cost, and throughput of different concentration methods for SARS-CoV-2 wastewater-based epidemiology. Water Res. 2021, 197, 117043. [Google Scholar] [CrossRef]
- Watanabe, M.; Ohnishi, T.; Arai, S.; Kawakami, T.; Hayashi, K.; Ohya, K.; Hirose, S.; Yoshinari, T.; Taharaguchi, S.; Mekata, H. Survival of SARS-CoV-2 and bovine coronavirus on common surfaces of living environments. Sci. Rep. 2022, 12, 10624. [Google Scholar] [CrossRef] [PubMed]
- Pecson, B.M.; Darby, E.; Haas, C.N.; Amha, Y.M.; Bartolo, M.; Danielson, R.; Dearborn, Y.; Di Giovanni, G.; Ferguson, C.; Fevig, S. Reproducibility and sensitivity of 36 methods to quantify the SARS-CoV-2 genetic signal in raw wastewater: Findings from an interlaboratory methods evaluation in the US. Environ. Sci. Water Res. Technol. 2021, 7, 504–520. [Google Scholar] [CrossRef] [PubMed]
- Harvey, A.P.; Fuhrmeister, E.R.; Cantrell, M.E.; Pitol, A.K.; Swarthout, J.M.; Powers, J.E.; Nadimpalli, M.L.; Julian, T.R.; Pickering, A.J. Longitudinal monitoring of SARS-CoV-2 RNA on high-touch surfaces in a community setting. Environ. Sci. Technol. Lett. 2020, 8, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Castano, N.; Cordts, S.C.; Kurosu Jalil, M.; Zhang, K.S.; Koppaka, S.; Bick, A.D.; Paul, R.; Tang, S.K. Fomite transmission, physicochemical origin of virus–surface interactions, and disinfection strategies for enveloped viruses with applications to SARS-CoV-2. ACS Omega 2021, 6, 6509–6527. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.G.; Lin, T.; Wang, P. Mechanisms of SARS-CoV-2 transmission and pathogenesis. Trends Immunol. 2020, 41, 1100–1115. [Google Scholar] [CrossRef]
- Moreno, T.; Pintó, R.M.; Bosch, A.; Moreno, N.; Alastuey, A.; Minguillón, M.C.; Anfruns-Estrada, E.; Guix, S.; Fuentes, C.; Buonanno, G. Tracing surface and airborne SARS-CoV-2 RNA inside public buses and subway trains. Environ. Int. 2021, 147, 106326. [Google Scholar] [CrossRef] [PubMed]
- Ong, S.W.X.; Tan, Y.K.; Chia, P.Y.; Lee, T.H.; Ng, O.T.; Wong, M.S.Y.; Marimuthu, K. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA 2020, 323, 1610–1612. [Google Scholar] [CrossRef]
- Gharehchahi, E.; Dehghani, F.; Rafiee, A.; Jamalidoust, M.; Hoseini, M. Investigating the Presence of SARS-CoV-2 on the Surfaces, Fomites, and in Indoor Air of a Referral COVID-19 Hospital, Shiraz, Iran. J. Health Sci. Surveill. Syst. 2023, 11 (Suppl. S1), 241–251. [Google Scholar]
- AHA. CDC: Masks Are Now Optional for 90% of the Country. 2022. Available online: https://www.aha.org/news/news/2022-03-04-masks-are-now-optional-90-country (accessed on 17 July 2022).
- Times, T.N. Mecklenburg County, North Carolina COVID-19 Cases. Available online: https://www.nytimes.com/interactive/2021/us/mecklenburg-north-carolina-covid-cases.html (accessed on 12 December 2022).
- Bhattarai, T.; Ebong, A.; Raja, M.Y.A.; Munir, M. Advancements in 275 nm UV-LED Technology for Deactivation of Bacteriophages, Phi6 and MS2. In Proceedings of the 2023 IEEE 20th International Conference on Smart Communities: Improving Quality of Life Using AI, Robotics and IoT (HONET), Boca Raton, FL, USA, 4–6 December 2023; IEEE: New York, NY, USA, 2023. [Google Scholar]
- Delhalle, L.; Taminiau, B.; Fastrez, S.; Fall, A.; Ballesteros, M.; Burteau, S.; Daube, G. Evaluation of enzymatic cleaning on food processing installations and food products bacterial microflora. Front. Microbiol. 2020, 11, 1827. [Google Scholar] [CrossRef]
- Gibson, H.; Taylor, J.; Hall, K.; Holah, J. Effectiveness of cleaning techniques used in the food industry in terms of the removal of bacterial biofilms. J. Appl. Microbiol. 1999, 87, 41–48. [Google Scholar] [CrossRef]
- He, M.; Xiong, J.; Huang, S.; Bian, Y.; Yan, P.; Redding, S.R. Airborne precautions recommended in Wuhan, China for bedside fiberoptic bronchoscopy examination of patients with COVID-19. J. Infect. 2020, 81, e75. [Google Scholar] [CrossRef]
- Bhattarai, T.; Ebong, A.; Raja, M.Y.A. A Review of Light-Emitting Diodes and Ultraviolet Light-Emitting Diodes and Their Applications. Photonics 2024, 11, 491. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).