
The Potential Role of Fecal Microbiota Transplantation in Parkinson’s Disease: A Systematic Literature Review


Abstract
:1. Introduction
2. Materials and Methods
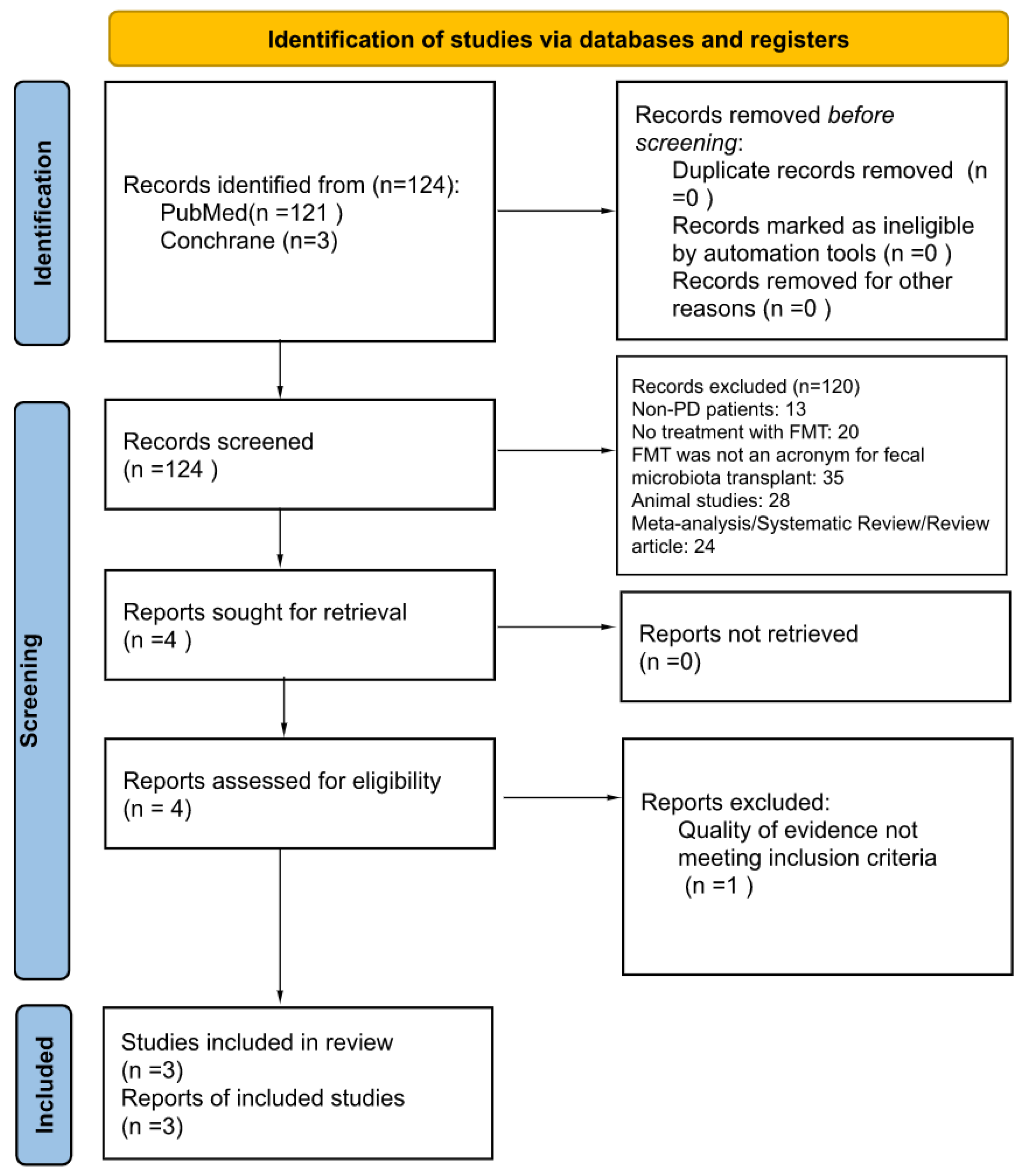
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Quality Assessment
2.4. Study Outcomes
2.5. Study Selection and Data Extraction
3. Results
4. Discussion
4.1. Neurologic Symptoms
4.2. Gastrointestinal Symptoms
4.3. Safety
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Armstrong, M.J.; Okun, M.S. Diagnosis and treatment of Parkinson disease: A review. Jama 2020, 323, 548–560. [Google Scholar] [CrossRef] [PubMed]
- Cryan, J.F.; O’Riordan, K.J.; Sandhu, K.; Peterson, V.; Dinan, T.G. The gut microbiome in neurological disorders. Lancet Neurol. 2020, 19, 179–194. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.-M.; Huang, H.-L.; Zhou, Y.-L.; Zhao, H.-L.; Xu, J.; Shou, D.-W.; Liu, Y.-D.; Zhou, Y.-J.; Nie, Y.-Q. Fecal Microbiota Transplantation: A New Therapeutic Attempt from the Gut to the Brain. Gastroenterol. Res. Pract. 2021, 2021, 6699268. [Google Scholar] [CrossRef] [PubMed]
- Yu, E.W.; Gao, L.; Stastka, P.; Cheney, M.C.; Mahabamunuge, J.; Soto, M.T.; Ford, C.B.; Bryant, J.A.; Henn, M.R.; Hohmann, E.L. Fecal microbiota transplantation for the improvement of metabolism in obesity: The FMT-TRIM double-blind placebo-controlled pilot trial. PLoS Med. 2020, 17, e1003051. [Google Scholar] [CrossRef] [PubMed]
- Scheperjans, F.; Aho, V.; Pereira, P.A.; Koskinen, K.; Paulin, L.; Pekkonen, E.; Haapaniemi, E.; Kaakkola, S.; Eerola-Rautio, J.; Pohja, M.; et al. Gut microbiota are related to Parkinson’s disease and clinical phenotype. Mov. Disord. 2015, 30, 350–358. [Google Scholar] [CrossRef]
- Keshavarzian, A.; Green, S.J.; Engen, P.A.; Voigt, R.M.; Naqib, A.; Forsyth, C.B.; Mutlu, E.; Shannon, K.M. Colonic bacterial composition in Parkinson’s disease. Mov. Disord. 2015, 30, 1351–1360. [Google Scholar] [CrossRef]
- American College of Cardiology. American Heart Association Task Force on Practice Guidelines, Obesity Expert Panel, 2013 Expert panel report: Guidelines (2013) for the management of overweight and obesity in adults. Obesity 2014, 22 (Suppl. S2), S41–S410. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Di Leo, G.; Sardanelli, F. Statistical significance: P value, 0.05 threshold, and applications to radiomics—Reasons for a conservative approach. Eur. Radiol. Exp. 2020, 4, 18. [Google Scholar] [CrossRef]
- Rodriguez-Blazquez, C.; Rojo-Abuin, J.M.; Alvarez-Sanchez, M.; Arakaki, T.; Bergareche-Yarza, A.; Chade, A.; Garretto, N.; Gershanik, O.; Kurtis, M.M.; Martinez-Castrillo, J.C.; et al. The MDS-UPDRS Part II (motor experiences of daily living) resulted useful for assessment of disability in Parkinson’s disease. Park. Relat. Disord. 2013, 19, 889–893. [Google Scholar] [CrossRef]
- Clarke, C.E.; Patel, S.; Ives, N.; Rick, C.E.; Woolley, R.; Wheatley, K.; Walker, M.F.; Zhu, S.; Kandiyali, R.; Yao, G.; et al. Clinical Effectiveness and Cost-Effectiveness of Physiotherapy and Occupational Therapy versus no Therapy in Mild to Moderate Parkinson’s Disease: A Large Pragmatic Randomised Controlled Trial (PD REHAB); NIHR Journals Library: Southampton, UK, 2016; Health Technology Assessment, No. 20.63. Appendix 8, Hoehn and Yahr Stages. Available online: https://www.ncbi.nlm.nih.gov/books/NBK379751/ (accessed on 1 April 2023).
- Martinez-Martin, P.; Chaudhuri, K.R.; Rojo-Abuin, J.M.; Rodriguez-Blazquez, C.; Alvarez-Sanchez, M.; Arakaki, T.; Bergareche-Yarza, A.; Chade, A.; Garretto, N.; Gershanik, O.; et al. Assessing the non-motor symptoms of Parkinson’s disease: MDS-UPDRS and NMS Scale. Eur. J. Neurol. 2015, 22, 37–43. [Google Scholar] [CrossRef]
- Nikjooy, A.; Jafari, H.; Saba, M.A.; Ebrahimi, N.; Mirzaei, R. Patient Assessment of Constipation Quality of Life Questionnaire: Translation, Cultural Adaptation, Reliability, and Validity of the Persian Version. Iran. J. Med. Sci. 2018, 43, 261–268. [Google Scholar]
- Frattini, J.C.; Nogueras, J.J. Slow Transit Constipation: A Review of a Colonic Functional Disorder. Clin. Colon Rectal Surg. 2008, 21, 146–152. [Google Scholar] [CrossRef]
- Chumpitazi, B.P.; Self, M.M.; Czyzewski, D.I.; Cejka, S.; Swank, P.R.; Shulman, R.J. Bristol Stool Form Scale Reliability and Agreement Decreases When Determining Rome III Stool Form Designations. Neurogastroenterol. Motil. 2016, 28, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Kuai, X.-Y.; Yao, X.-H.; Xu, L.-J.; Zhou, Y.-Q.; Zhang, L.-P.; Liu, Y.; Pei, S.-F.; Zhou, C.-L. Evaluation of fecal microbiota transplantation in Parkinson’s disease patients with constipation. Microb. Cell Factories 2021, 20, 98. [Google Scholar] [CrossRef] [PubMed]
- Segal, A.; Zlotnik, Y.; Moyal-Atias, K.; Abuhasira, R.; Ifergane, G. Fecal microbiota transplant as a potential treatment for Parkinson’s disease—A case series. Clin. Neurol. Neurosurg. 2021, 207, 106791. [Google Scholar] [CrossRef] [PubMed]
- Xue, L.-J.; Yang, X.-Z.; Tong, Q.; Shen, P.; Ma, S.-J.; Wu, S.-N.; Zheng, J.-L.; Wang, H.-G. Fecal microbiota transplantation therapy for Parkinson’s disease: A preliminary study. Medicine 2020, 99, e22035. [Google Scholar] [CrossRef]
- Touch, S.; Godefroy, E.; Rolhion, N.; Danne, C.; Oeuvray, C.; Straube, M.; Galbert, C.; Brot, L.; Salgueiro, I.A.; Chadi, S.; et al. Human CD4+CD8α+ Tregs induced by Faecalibacterium prausnitzii protect against intestinal inflammation. JCI Insight. 2022, 7, e154722. [Google Scholar] [CrossRef]
- DuPont, H.L.; Suescun, J.; Jiang, Z.-D.; Brown, E.L.; Essigmann, H.T.; Alexander, A.S.; DuPont, A.W.; Iqbal, T.; Utay, N.S.; Newmark, M.; et al. Fecal microbiota transplantation in Parkinson’s disease—A randomized repeat-dose, placebo-controlled clinical pilot study. Front. Neurol. 2023, 14, 1104759. [Google Scholar] [CrossRef]
- Warnecke, T.; Schäfer, K.-H.; Claus, I.; Del Tredici, K.; Jost, W.H. Gastrointestinal involvement in Parkinson’s disease: Pathophysiology, diagnosis, and management. npj Park. Dis. 2022, 8, 31. [Google Scholar] [CrossRef]
- Braak, H.; Del Tredici, K. Neuropathological Staging of Brain Pathology in Sporadic Parkinson’s disease: Separating the Wheat from the Chaff. J. Park. Dis. 2017, 7 (Suppl. S1), S71–S85. [Google Scholar] [CrossRef] [PubMed]
- Reichmann, H. Premotor Diagnosis of Parkinson’s Disease. Neurosci. Bull. 2017, 33, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Spillantini, M.G.; Schmidt, M.L.; Lee, V.M.; Trojanowski, J.Q.; Jakes, R.; Goedert, M. Alpha-synuclein in Lewy bodies. Nature 1997, 388, 839–840. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.K.; Wall, E.S.; Robinson, C.D.; Guillemin, K.; Eisen, J.S. Enteric nervous system modulation of luminal pH modifies the microbial environment to promote intestinal health. PLoS Pathog. 2022, 18, e1009989. [Google Scholar] [CrossRef] [PubMed]
- Kelly, C.R.; Ihunnah, C.; Fischer, M.; Khoruts, A.; Surawicz, C.; Afzali, A.; Aroniadis, O.; Barto, A.; Borody, T.; Giovanelli, A.; et al. Fecal Microbiota Transplant for Treatment of Clostridium difficile Infection in Immunocompromised Patients. Am. J. Gastroenterol. 2014, 109, 1065–1071. [Google Scholar] [CrossRef]
- Green, J.E.; Davis, J.A.; Berk, M.; Hair, C.; Loughman, A.; Castle, D.; Athan, E.; Nierenberg, A.A.; Cryan, J.F.; Jacka, F.; et al. Efficacy and safety of fecal microbiota transplantation for the treatment of diseases other than Clostridium difficile infection: A systematic review and meta-analysis. Gut Microbes 2020, 12, 1–25. [Google Scholar] [CrossRef]
- Miyasaki, J.M.; Martin, W.; Suchowersky, O.; Weiner, W.J.; Lang, A.E. Practice parameter: Initiation of treatment for Parkinson’s disease: An evidence-based review: Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2002, 58, 11–17. [Google Scholar] [CrossRef]
- Goetz, C.G.; Poewe, W.; Rascol, O.; Sampaio, C. Evidence-based medical review update: Pharmacological and surgical treatments of Parkinson’s disease: 2001 to 2004. Mov. Disord. 2005, 20, 523–539. [Google Scholar] [CrossRef]
- Ooijevaar, R.E.; Terveer, E.M.; Verspaget, H.W.; Kuijper, E.J.; Keller, J.J. Clinical Application and Potential of Fecal Microbiota Transplantation. Annu. Rev. Med. 2019, 70, 335–351. [Google Scholar] [CrossRef]

{kind=link}
| Author/Year | Study Design | Location (City, Country) | Pretreatment | Intervention |
|---|---|---|---|---|
| Kuai [16], 2021 | Case series | Jiangsu, China | High grain and vegetable diet, low meat | 40–50 mL of donor stool in 200 mL normal saline, one time, through nasoduodenal tube. |
| Segal [17], 2021 | Case series | Beersheba, Israel | NR | 65 g donor stool in 300 mL normal saline deposited through colonoscopy with 100 mL deposited in the terminal ileum, 100 mL in the cecum, and the last 100 mL throughout the remainder of the colon. |
| Xue [18], 2020 | Case series | Nanjing, China | NR | 10 patients had donor stool per colonoscopy into ascending colon, and 5 patients had delivery into the jejunum via nasal jejunal tube; unreported quantities. |
| Author/Year | Population Characteristics | Sample Size (n) | Age | Male (n) | Female (n) | Neurologic Scoring | GI Scoring |
|---|---|---|---|---|---|---|---|
| Kuai [16], 2021 | Adult PD with constipation | 11 | 62.45 years | 7 | 5 | H-Y 2.27 (.75), UPDRS II 11.36 (4.7), NMSS 22.36 (7.05) | PAC-QOL 102.55 (12.21), WCSS 11.63 (3.22) |
| Segal [17], 2021 | Adult PD meeting criteria for colonoscopy screening also complaining of constipation | 6 | 63.5 years | 3 | 3 | UPDRS III rated mild to moderate range 5–41 | BSFS 1–2, WCSS 13.5(10.75–15.25) |
| Xue [18], 2020 | Adult PD with constipation not relieved by previous management | 15 | 61 years | 11 | 4 | Baseline NMSS and UPDRS III scores NR | NR |
| Study | Results | p-Value |
|---|---|---|
| Kuai [16], 2021 | H-Y: initial—2.27, 6 wks—1.45, 12 wks 1.09. | 0.0023 |
| UPDRS II: initial—11.36, 6 wks 6.18, 12 wks 4.9 | 0.0036 | |
| NMSS: initial-22.36, 6 wks—12.55, 12 wks—0.003 | 0.003 | |
| Segal [17], 2021 | UPDRS III: Initial—25, 24 wks—20.16 | NR |
| NMSS: Initial—59.85, 24 wks—38.83 | NR | |
| Xue [18], 2020 | NMSS: 4 wks—11.06, 12 wks—9.83 | 4 wks—0.001, 12 wks—<0.001 |
| UPDRS: 4 wks 33.8, 12 wks—24 | 4 wks—0.001, 12 wks—<0.001 |
| Study | Results | p-Value |
|---|---|---|
| Kuai [16], 2021 | PAC-QOL: initial—102.55, 6 wks—51.27, 12 wks 43.45 | <0.0002 |
| WCSS: initial—11.63, 6 wks—8.16, 12 wks—6.22 | 0.0231 | |
| Segal [17], 2021 | BSFS: initial—1.5, 24 wks—4 | NR |
| WCSS: initial—13.5, 24 wks—9 | NR |
| Author/Year | AE | Serious AE | Death |
|---|---|---|---|
| Kuai [16], 2021 | 1 diarrhea, 5 abdominal pain, 3 venting, 7 flatus, 3 nausea, 2 throat irritation | None | None |
| Segal [17], 2021 | None | One patient had recurrent episodic vasovagal syncope requiring hospital observation, which was self-resolving. | None |
| Xue [18], 2020 | 2 diarrhea, 2 abdominal pain, 1 flatulence | None | None |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vongsavath, T.; Laeeq, T.; Tun, K.M.; Hong, A.S. The Potential Role of Fecal Microbiota Transplantation in Parkinson’s Disease: A Systematic Literature Review. Appl. Microbiol. 2023, 3, 993-1002. https://doi.org/10.3390/applmicrobiol3030067
Vongsavath T, Laeeq T, Tun KM, Hong AS. The Potential Role of Fecal Microbiota Transplantation in Parkinson’s Disease: A Systematic Literature Review. Applied Microbiology. 2023; 3(3):993-1002. https://doi.org/10.3390/applmicrobiol3030067
Chicago/Turabian StyleVongsavath, Tahne, Tooba Laeeq, Kyaw Min Tun, and Annie S. Hong. 2023. "The Potential Role of Fecal Microbiota Transplantation in Parkinson’s Disease: A Systematic Literature Review" Applied Microbiology 3, no. 3: 993-1002. https://doi.org/10.3390/applmicrobiol3030067
APA StyleVongsavath, T., Laeeq, T., Tun, K. M., & Hong, A. S. (2023). The Potential Role of Fecal Microbiota Transplantation in Parkinson’s Disease: A Systematic Literature Review. Applied Microbiology, 3(3), 993-1002. https://doi.org/10.3390/applmicrobiol3030067