
Antimicrobial Coatings: Reviewing Options for Healthcare Applications




Abstract
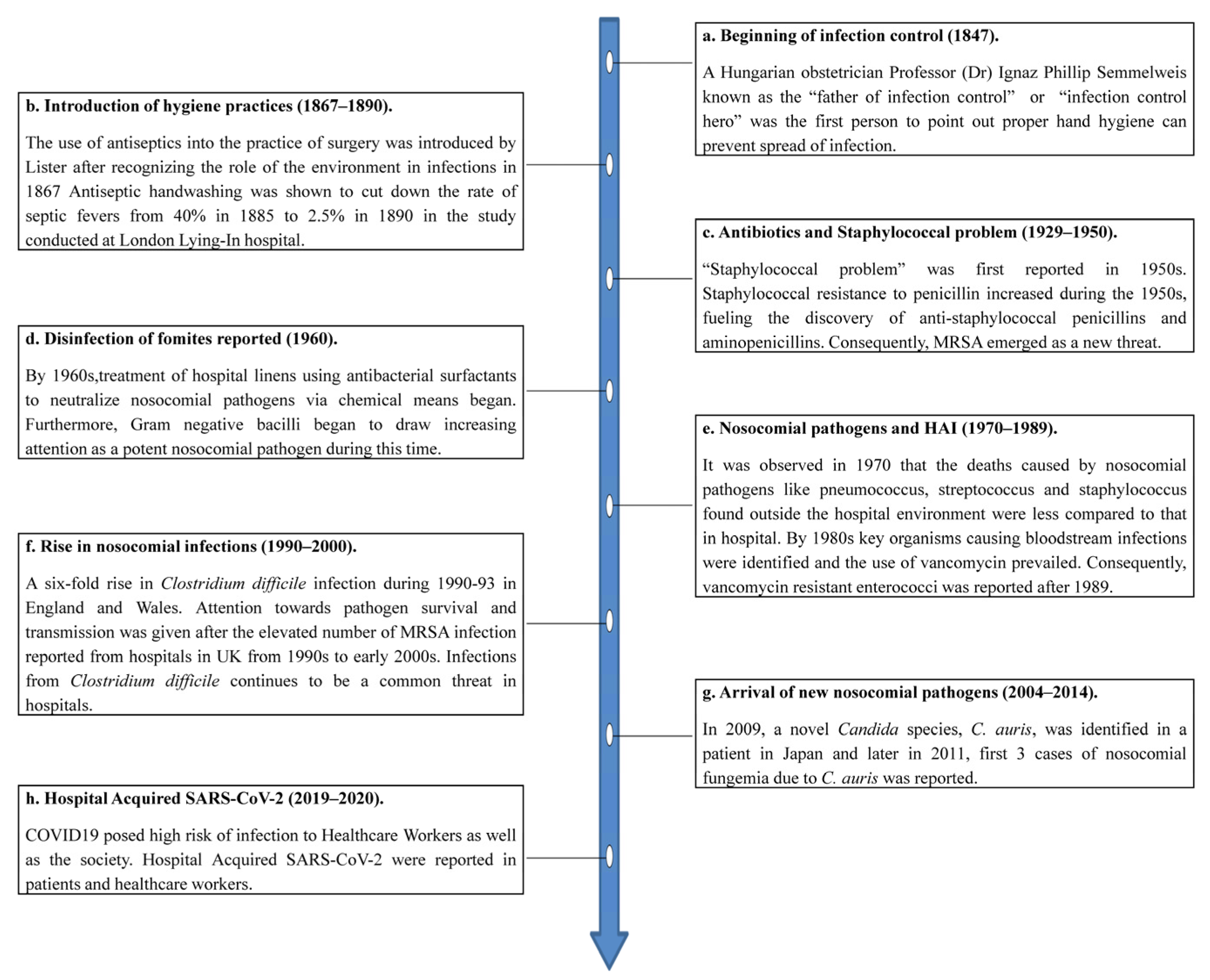
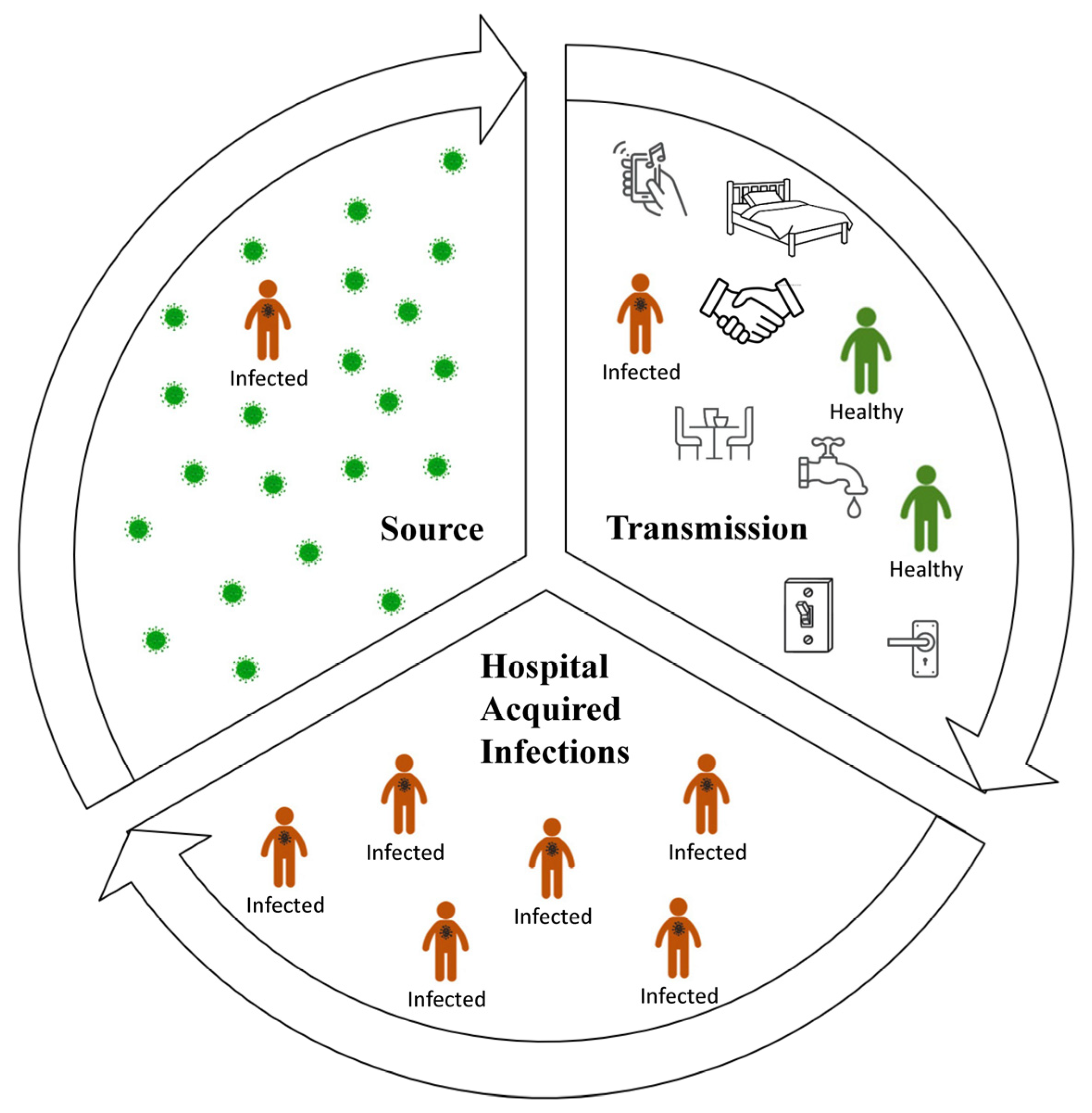
1. The Problem: HAIs and the Transmission of Pathogens by Fomites
2. The Evidence for Surface and Fomite-Mediated Transmission in Healthcare Facilities
3. How Can Fomite-Mediated Transmission Be Managed?
4. Can Special Surfaces/Coatings Help to Solve the Fomite Problem?
4.1. Antifouling Coatings
4.1.1. Nanostructured Surfaces
4.1.2. Chemically Modified Microbe Repelling Coatings
4.2. Antimicrobial Coatings
4.2.1. Contact-Active AMC
- (a)
- Contact-active AMC containing biomimetic polymers
- (b)
- Contact active AMC containing synthetic polymers
4.2.2. Biocide-Releasing AMC
- (a)
- Continuous release
- (b)
- Slow release
- (c)
- Triggered release
5. Antimicrobial Actions of Coatings with Both AMC and AFC
5.1. Contact-Killing and Repelling Coatings
5.2. Releasing and Repelling Coatings
5.3. Releasing and Contact-Killing Coatings
6. Replenishable Coatings: A Sustainable Option?
6.1. Photocatalytic Coatings
6.2. N-halamine Coatings
7. Selecting Suitable Coatings for Hospitals: A Major Challenge?
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Shittu, A.O.; Mellmann, A.; Schaumburg, F. Molecular characterization of Staphylococcus aureus complex from fomites in Nigeria. Infect. Genet. Evol. 2020, 85, 104504. [Google Scholar] [CrossRef] [PubMed]
- Stephens, B.; Azimi, P.; Thoemmes, M.S.; Heidarinejad, M.; Allen, J.G.; Gilbert, J.A. Microbial Exchange via Fomites and Implications for Human Health. Curr. Pollut. Rep. 2019, 5, 198–213. [Google Scholar] [CrossRef] [PubMed]
- Dancer, S.J. Controlling Hospital-Acquired Infection: Focus on the Role of the Environment and New Technologies for Decontamination. Clin. Microbiol. Rev. 2014, 27, 665–690. [Google Scholar] [CrossRef] [PubMed]
- Borkow, G. Use of Biocidal Surfaces for Reduction of Healthcare Acquired Infections, 1st ed.; Springer: Cham, Switzerland, 2014; p. 215. [Google Scholar]
- Kramer, A.; Schwebke, I.; Kampf, G. How long do nosocomial pathogens persist on inanimate surfaces? A systematic review. BMC Infect. Dis. 2006, 6, 130. [Google Scholar] [CrossRef] [PubMed]
- Donlan, R.M. Biofilms: Microbial life on surfaces. Emerg. Infect. Dis. 2002, 8, 881–890. [Google Scholar] [CrossRef]
- Dancer, S.J. Hospital cleaning in the 21st century. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 1473–1481. [Google Scholar] [CrossRef]
- Tang, J.W.; Tambyah, P.A.; Hui, D.S.C. Emergence of a novel coronavirus causing respiratory illness from Wuhan, China. J. Infect. 2020, 80, 350–371. [Google Scholar] [CrossRef] [PubMed]
- van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Dancer, S.J.; Li, Y.; Hart, A.; Tang, J.W.; Jones, D.L. What is the risk of acquiring SARS-CoV-2 from the use of public toilets? Sci. Total Environ. 2021, 792, 148341. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wang, Q.; Ding, P.; Cha, Y.e.; Mao, Y.; Ding, C.; Gu, W.; Wang, Y.; Ying, B.; Zhao, X.; et al. Risk factors and on-site simulation of environmental transmission of SARS-CoV-2 in the largest wholesale market of Beijing, China. Sci. Total Environ. 2021, 778, 146040. [Google Scholar] [CrossRef]
- Marsalek, J. Reframing the problem of the fomite transmission of COVID-19. J. Hosp. Infect. 2021, 115, 133–134. [Google Scholar] [CrossRef] [PubMed]
- Ong, S.W.X.; Tan, Y.K.; Chia, P.Y.; Lee, T.H.; Ng, O.T.; Wong, M.S.Y.; Marimuthu, K. Air, Surface Environmental, and Personal Protective Equipment Contamination by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) From a Symptomatic Patient. JAMA 2020, 323, 1610–1612. [Google Scholar] [CrossRef]
- Shirvanimoghaddam, K.; Akbari, M.K.; Yadav, R.; Al-Tamimi, A.K.; Naebe, M. Fight against COVID-19: The case of antiviral surfaces. APL Mater. 2021, 9, 031112. [Google Scholar] [CrossRef]
- Rakowska, P.D.; Tiddia, M.; Faruqui, N.; Bankier, C.; Pei, Y.; Pollard, A.J.; Zhang, J.; Gilmore, I.S. Antiviral surfaces and coatings and their mechanisms of action. Commun. Mater. 2021, 2, 53. [Google Scholar] [CrossRef]
- Powitz, R.W. The Rise of Antimicrobial Coatings Usage and Standards. Available online: https://www.food-safety.com/articles/7571-the-rise-of-antimicrobial-coatings-usage-and-standards (accessed on 12 July 2022).
- Rodríguez-Acelas, A.L.; de Abreu Almeida, M.; Engelman, B.; Cañon-Montañez, W. Risk factors for health care–associated infection in hospitalized adults: Systematic review and meta-analysis. Am. J. Infect. Control 2017, 45, 149–156. [Google Scholar] [CrossRef]
- Boev, C.; Kiss, E. Hospital-Acquired Infections: Current Trends and Prevention. Crit. Care Nurs. Clin. N. Am. 2017, 29, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, A.W. Control of hospital acquired infections and antimicrobial resistance in Europe: The way to go. Wien. Med. Wochenschr. 2019, 169, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Ducel, G.; Fabry, J.; Nicolle, L. Prevention of Hospital-Acquired Infections: A Practical Guide, 2nd ed.; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Gilmore, M.S.; Lebreton, F.; van Schaik, W. Genomic transition of enterococci from gut commensals to leading causes of multidrug-resistant hospital infection in the antibiotic era. Curr. Opin. Microbiol. 2013, 16, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.; Conceição, T.; Silva, I.S.; de Lencastre, H.; Aires-de-Sousa, M. Frequent MRSA nasal colonization among hospitalized children and their parents in Angola and São Tomé and Príncipe. J. Hosp. Infect. 2018, 100, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Best, M. Ignaz Semmelweis and the birth of infection control. Qual. Saf. Health Care 2004, 13, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Sydnor, E.R.M.; Perl, T.M. Hospital epidemiology and infection control in acute-care settings. Clin. Microbiol. Rev. 2011, 24, 141–173. [Google Scholar] [CrossRef] [PubMed]
- Neely, A.N. Persistence of microorganisms on common hospital surfaces: Strategies to control their dissemination. Infect. Control Resour. 2002, 4, 1–8. [Google Scholar]
- Larson, E. A Causal Link Between Handwashing and Risk of Infection? Examination of the Evidence. Infect. Control Hosp. Epidemiol. 1988, 9, 28–36. [Google Scholar] [CrossRef]
- Turner, N.A.; Sharma-Kuinkel, B.K.; Maskarinec, S.A.; Eichenberger, E.M.; Shah, P.P.; Carugati, M.; Holland, T.L.; Fowler, V.G. Methicillin-resistant Staphylococcus aureus: An overview of basic and clinical research. Nat. Rev. Microbiol. 2019, 17, 203–218. [Google Scholar] [CrossRef] [PubMed]
- Demain, A.L.; Elander, R.P. The beta-lactam antibiotics: Past, present, and future. Antonie Van Leeuwenhoek 1999, 75, 5–19. [Google Scholar] [CrossRef]
- Swartz, M.N. Hospital-acquired infections: Diseases with increasingly limited therapies. Proc. Natl. Acad. Sci. USA 1994, 91, 2420–2427. [Google Scholar] [CrossRef]
- Linfield, W.M.; Sherrill, J.C.; Casely, R.E.; Noel, D.R.; Davis, G.A. Studies in the development of antibacterial surfactants. I. institutional use of antibacterial fabric softeners. J. Am. Oil Chem. Soc. 1960, 37, 248–251. [Google Scholar] [CrossRef]
- Goldmann, D.A.; Huskins, W.C. Control of nosocomial antimicrobial-resistant bacteria: A strategic priority for hospitals worldwide. Clin. Infect. Dis. 1997, 24, 139–145. [Google Scholar] [CrossRef]
- Choi, K.B.; Suh, K.N.; Muldoon, K.A.; Roth, V.R.; Forster, A.J. Hospital-acquired Clostridium difficile infection: An institutional costing analysis. J. Hosp. Infect. 2019, 102, 141–147. [Google Scholar] [CrossRef]
- Wilcox, M.H.; Cunniffe, J.G.; Trundle, C.; Redpath, C. Financial burden of hospital-acquired Clostridium difficile infection. J. Hosp. Infect. 1996, 34, 23–30. [Google Scholar] [CrossRef]
- Fasugba, O.; Gardner, A.; Mitchell, B.G.; Mnatzaganian, G. Ciprofloxacin resistance in community- and hospital-acquired Escherichia coli urinary tract infections: A systematic review and meta-analysis of observational studies. BMC Infect. Dis. 2015, 15, 545. [Google Scholar] [CrossRef]
- Chowdhary, A.; Sharma, C.; Meis, J.F. Candida auris: A rapidly emerging cause of hospital-acquired multidrug-resistant fungal infections globally. PLoS Pathog. 2017, 13, e1006290. [Google Scholar] [CrossRef] [PubMed]
- Rickman, H.M.; Rampling, T.; Shaw, K.; Martinez-Garcia, G.; Hail, L.; Coen, P.; Shahmanesh, M.; Shin, G.Y.; Nastouli, E.; Houlihan, C.F. Nosocomial Transmission of Coronavirus Disease 2019: A Retrospective Study of 66 Hospital-acquired Cases in a London Teaching Hospital. Clin. Infect. Dis. 2020, 72, 690–693. [Google Scholar] [CrossRef] [PubMed]
- Richterman, A.; Meyerowitz, E.A.; Cevik, M. Hospital-acquired SARS-CoV-2 infection: Lessons for public health. JAMA 2021, 324, 2155–2156. [Google Scholar] [CrossRef] [PubMed]
- Lai, X.; Wang, M.; Qin, C.; Tan, L.; Ran, L.; Chen, D.; Zhang, H.; Shang, K.; Xia, C.; Wang, S.; et al. Coronavirus Disease 2019 (COVID-2019) Infection Among Health Care Workers and Implications for Prevention Measures in a Tertiary Hospital in Wuhan, China. JAMA Netw. Open 2020, 3, e209666. [Google Scholar] [CrossRef] [PubMed]
- Suleyman, G.; Alangaden, G.; Bardossy, A.C. The Role of Environmental Contamination in the Transmission of Nosocomial Pathogens and Healthcare-Associated Infections. Curr. Infect. Dis. Rep. 2018, 20, 12. [Google Scholar] [CrossRef]
- Weber, D.J.; Rutala, W.A.; Miller, M.B.; Huslage, K.; Sickbert-Bennett, E. Role of hospital surfaces in the transmission of emerging health care-associated pathogens: Norovirus, Clostridium difficile, and Acinetobacter species. Am. J. Infect. Control 2010, 38, S25–S33. [Google Scholar] [CrossRef] [PubMed]
- Otter, J.A.; Yezli, S.; Salkeld, J.A.G.; French, G.L. Evidence that contaminated surfaces contribute to the transmission of hospital pathogens and an overview of strategies to address contaminated surfaces in hospital settings. Am. J. Infect. Control 2013, 41, S6. [Google Scholar] [CrossRef] [PubMed]
- Rampling, A.; Wiseman, S.; Davis, L.; Hyett, A.P.; Walbridge, A.N.; Payne, G.C.; Cornaby, A.J. Evidence that hospital hygiene is important in the control of methicillin-resistant Staphylococcus aureus. J. Hosp. Infect. 2001, 49, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Young, K.Y.; Hee, S.S.; Jeong, Y.K.; Dae, W.P.; Jang, W.S.; Kyung, H.R.; Seung, E.L.; Min, J.K. Epidemiology and control of an outbreak of vancomycin-resistant enterococci in the intensive care units. Yonsei Med. J. 2009, 50, 637–643. [Google Scholar] [CrossRef]
- Shams, A.M.; Rose, L.J.; Edwards, J.R.; Cali, S.; Harris, A.D.; Jacob, J.T.; Lafae, A.; Pineles, L.L.; Thom, K.A.; McDonald, L.C.; et al. Assessment of the Overall and Multidrug-Resistant Organism Bioburden on Environmental Surfaces in Healthcare Facilities. Infect. Control Hosp. Epidemiol. 2016, 37, 1426–1432. [Google Scholar] [CrossRef] [PubMed]
- Best, E.L.; Fawley, W.N.; Parnell, P.; Wilcox, M.H. The Potential for Airborne Dispersal of Clostridium difficile from Symptomatic Patients. Clin. Infect. Dis. 2010, 50, 1450–1457. [Google Scholar] [CrossRef]
- Ledwoch, K.; Maillard, J.Y. Candida auris dry surface biofilm (DSB) for disinfectant efficacy testing. Materials 2018, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Almatroudi, A.; Gosbell, I.B.; Hu, H.; Jensen, S.O.; Espedido, B.A.; Tahir, S.; Glasbey, T.O.; Legge, P.; Whiteley, G.; Deva, A.; et al. Staphylococcus aureus dry-surface biofilms are not killed by sodium hypochlorite: Implications for infection control. J. Hosp. Infect. 2016, 93, 263–270. [Google Scholar] [CrossRef]
- Vickery, K. Special Issue: Microbial biofilms in healthcare: Formation, prevention and treatment. Materials 2019, 12, 2001. [Google Scholar] [CrossRef]
- Almatroudi, A.; Tahir, S.; Hu, H.; Chowdhury, D.; Gosbell, I.B.; Jensen, S.O.; Whiteley, G.S.; Deva, A.K.; Glasbey, T.; Vickery, K. Staphylococcus aureus dry-surface biofilms are more resistant to heat treatment than traditional hydrated biofilms. J. Hosp. Infect. 2018, 98, 161–167. [Google Scholar] [CrossRef]
- Chowdhury, D.; Tahir, S.; Legge, M.; Hu, H.; Prvan, T.; Johani, K.; Whiteley, G.S.; Glasbey, T.O.; Deva, A.K.; Vickery, K. Transfer of dry surface biofilm in the healthcare environment: The role of healthcare workers’ hands as vehicles. J. Hosp. Infect. 2018, 100, 85–90. [Google Scholar] [CrossRef]
- Ledwoch, K.; Dancer, S.J.; Otter, J.A.; Kerr, K.; Roposte, D.; Rushton, L.; Weiser, R.; Mahenthiralingam, E.; Muir, D.D.; Maillard, J.Y. Beware biofilm! Dry biofilms containing bacterial pathogens on multiple healthcare surfaces; a multi-centre study. J. Hosp. Infect. 2018, 100, 47–56. [Google Scholar] [CrossRef]
- Muller, M.P.; MacDougall, C.; Lim, M.; Armstrong, I.; Bialachowski, A.; Callery, S.; Ciccotelli, W.; Cividino, M.; Dennis, J.; Hota, S.; et al. Antimicrobial surfaces to prevent healthcare-associated infections: A systematic review. J. Hosp. Infect. 2016, 92, 7–13. [Google Scholar] [CrossRef]
- Curtis, L.T. Prevention of hospital-acquired infections: Review of non-pharmacological interventions. J. Hosp. Infect. 2008, 69, 204–219. [Google Scholar] [CrossRef] [PubMed]
- Dougall, L.R.; Booth, M.G.; Khoo, E.; Hood, H.; Macgregor, S.J.; Anderson, J.G.; Timoshkin, I.V.; Maclean, M. Continuous monitoring of aerial bioburden within intensive care isolation rooms and identification of high-risk activities. J. Hosp. Infect. 2019, 103, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.W.; Li, Y.; Eames, I.; Chan, P.K.S.; Ridgway, G.L. Factors involved in the aerosol transmission of infection and control of ventilation in healthcare premises. J. Hosp. Infect. 2006, 64, 100–114. [Google Scholar] [CrossRef]
- Kotay, S.M.; Donlan, R.M.; Ganim, C.; Barry, K.; Christensen, B.E.; Mathers, A.J. Droplet- Rather than Aerosol-Mediated Dispersion Is the Primary Mechanism of Bacterial Transmission from Contaminated Hand-Washing Sink Traps. Appl. Environ. Microbiol. 2019, 85, 1–12. [Google Scholar] [CrossRef]
- Weinbren, M.J. The handwash station: Friend or fiend? J. Hosp. Infect. 2018, 100, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, R.; Fernandez, R.; Halcomb, E. Reservoirs of MRSA in the acute hospital setting: A systematic review. Contemp. Nurse 2002, 13, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Cavari, Y.; Kaplan, O.; Zander, A.; Hazan, G.; Shemer-Avni, Y.; Borer, A. Healthcare workers mobile phone usage: A potential risk for viral contamination. Surveillance pilot study. Infect. Dis. 2016, 48, 432–435. [Google Scholar] [CrossRef]
- Munoz-Gutierrez, K.M.; Canales, R.A.; Reynolds, K.A.; Verhougstraete, M.P. Floor and environmental contamination during glove disposal. J. Hosp. Infect. 2019, 101, 347–353. [Google Scholar] [CrossRef]
- Kotoda, M.; Hishiyama, S.; Mitsui, K.; Tanikawa, T.; Morikawa, S.; Takamino, A.; Matsukawa, T. Assessment of the potential for pathogen dispersal during high-flow nasal therapy. J. Hosp. Infect. 2020, 104, 534–537. [Google Scholar] [CrossRef]
- Mitchell, A.; Spencer, M.; Edmiston, C. Role of healthcare apparel and other healthcare textiles in the transmission of pathogens: A review of the literature. J. Hosp. Infect. 2015, 90, 285–292. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC); Infection Control Africa Network (ICAN). Best Practices for Environmental Cleaning in Healthcare Facilities in Resource-Limited Settings. 2019. Available online: https://www.cdc.gov/hai/prevent/resource-limited/index.html/ (accessed on 10 July 2022).
- NHS England. National Standards of Healthcare Cleanliness 2021. Available online: https://www.england.nhs.uk/publication/national-standards-of-healthcare-cleanliness-2021/ (accessed on 28 July 2022).
- French, G.L.; Otter, J.A.; Shannon, K.P.; Adams, N.M.T.; Watling, D.; Parks, M.J. Tackling contamination of the hospital environment by methicillin-resistant Staphylococcus aureus (MRSA): A comparison between conventional terminal cleaning and hydrogen peroxide vapour decontamination. J. Hosp. Infect. 2004, 57, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Manian, F.A.; Griesenauer, S.; Senkel, D.; Setzer, J.M.; Doll, S.A.; Perry, A.M.; Wiechens, M. Isolation of Acinetobacter baumannii Complex and Methicillin-Resistant Staphylococcus aureus from Hospital Rooms Following Terminal Cleaning and Disinfection: Can We Do Better? Infect. Control Hosp. Epidemiol. 2011, 32, 667–672. [Google Scholar] [CrossRef]
- Wilcox, M.H.; Fawley, W.N.; Wigglesworth, N.; Parnell, P.; Verity, P.; Freeman, J. Comparison of the effect of detergent versus hypochlorite cleaning on environmental contamination and incidence of Clostridium difficile infection. J. Hosp. Infect. 2003, 54, 109–114. [Google Scholar] [CrossRef]
- ASTM E2871−21; Standard Test Method for Determining Disinfectant Efficacy against Biofilm Grown in the CDC Biofilm Reactor Using the Single Tube Method. ASTM International: West Conshohocken, PA, USA, 2021.
- Leas, B.F.; Sullivan, N.; Han, J.H.; Pegues, D.A.; Kaczmarek, J.L.; Umscheid, C.A. Environmental Cleaning for the Prevention of Healthcare-Associated Infections; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2015. [Google Scholar]
- Boyce, J.M.; Havill, N.L.; Otter, J.A.; McDonald, L.C.; Adams, N.M.T.; Cooper, T.; Thompson, A.; Wiggs, L.; Killgore, G.; Tauman, A.; et al. Impact of Hydrogen Peroxide Vapor Room Decontamination on Clostridium difficile Environmental Contamination and Transmission in a Healthcare Setting. Infect. Control Hosp. Epidemiol. 2008, 29, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Verity, P.; Wilcox, M.H.; Fawley, W.; Parnell, P. Prospective evaluation of environmental contamination by Clostridium difficile in isolation side rooms. J. Hosp. Infect. 2001, 49, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Fraise, A. Currently available sporicides for use in healthcare, and their limitations. J. Hosp. Infect. 2011, 77, 210–212. [Google Scholar] [CrossRef] [PubMed]
- Dettenkofer, M.; Block, C. Hospital disinfection: Efficacy and safety issues. Curr. Opin. Infect. Dis. 2005, 18, 320–325. [Google Scholar] [CrossRef]
- Kanamori, H.; Rutala, W.A.; Weber, D.J. The role of patient care items as a fomite in healthcare-associated outbreaks and infection prevention. Clin. Infect. Dis. 2017, 65, 1412–1419. [Google Scholar] [CrossRef]
- Otter, J.A.; Yezli, S.; Barbut, F.; Perl, T.M. An overview of automated room disinfection systems: When to use them and how to choose them. In Decontamination in Hospitals and Healthcare; Elsevier: Amsterdam, The Netherlands, 2020; pp. 323–369. [Google Scholar]
- Rutala, W.A.; Gergen, M.F.; Weber, D.J. Room Decontamination with UV Radiation. Infect. Control Hosp. Epidemiol. 2010, 31, 1025–1029. [Google Scholar] [CrossRef]
- Boyce, J.M.; Havill, N.L.; Moore, B.A. Terminal Decontamination of Patient Rooms Using an Automated Mobile UV Light Unit. Infect. Control Hosp. Epidemiol. 2011, 32, 737–742. [Google Scholar] [CrossRef]
- Ghantoji, S.S.; Stibich, M.; Stachowiak, J.; Cantu, S.; Adachi, J.A.; Raad, I.I.; Chemaly, R.F. Non-inferiority of pulsed xenon UV light versus bleach for reducing environmental Clostridium difficile contamination on high-touch surfaces in clostridium difficile infection isolation rooms. J. Med. Microbiol. 2015, 64, 191–194. [Google Scholar] [CrossRef]
- El Haddad, L.; Ghantoji, S.S.; Stibich, M.; Fleming, J.B.; Segal, C.; Ware, K.M.; Chemaly, R.F. Evaluation of a pulsed xenon ultraviolet disinfection system to decrease bacterial contamination in operating rooms. BMC Infect. Dis. 2017, 17, 672. [Google Scholar] [CrossRef] [PubMed]
- Maclean, M.; MacGregor, S.J.; Anderson, J.G.; Woolsey, G.A.; Coia, J.E.; Hamilton, K.; Taggart, I.; Watson, S.B.; Thakker, B.; Gettinby, G. Environmental decontamination of a hospital isolation room using high-intensity narrow-spectrum light. J. Hosp. Infect. 2010, 76, 247–251. [Google Scholar] [CrossRef]
- Yebra, D.M.; Kiil, S.; Dam-Johansen, K. Antifouling technology—Past, present and future steps towards efficient and environmentally friendly antifouling coatings. Prog. Org. Coat. 2004, 50, 75–104. [Google Scholar] [CrossRef]
- Page, K.; Wilson, M.; Parkin, I.P. Antimicrobial surfaces and their potential in reducing the role of the inanimate environment in the incidence of hospital-acquired infections. J. Mater. Chem. 2009, 19, 3819–3831. [Google Scholar] [CrossRef]
- Tiller, J.C. Antimicrobial Surfaces. Adv. Polym. Sci. 2011, 240, 193–217. [Google Scholar] [CrossRef]
- Greenhalgh, R.; Walker, J.T. Antimicrobial strategies for polymeric hygienic surfaces in healthcare. Int. Biodeterior. Biodegrad. 2017, 125, 214–227. [Google Scholar] [CrossRef]
- Adlhart, C.; Verran, J.; Azevedo, N.F.; Olmez, H.; Keinänen-Toivola, M.M.; Gouveia, I.; Melo, L.F.; Crijns, F. Surface modifications for antimicrobial effects in the healthcare setting: A critical overview. J. Hosp. Infect. 2018, 99, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Querido, M.M.; Aguiar, L.; Neves, P.; Pereira, C.C.; Teixeira, J.P. Self-disinfecting surfaces and infection control. Colloids Surf. B Biointerfaces 2019, 178, 8–21. [Google Scholar] [CrossRef]
- Gupta, S.; Puttaiahgowda, Y.M.; Nagaraja, A.; Jalageri, M.D. Antimicrobial polymeric paints: An up-to-date review. Polym. Adv. Technol. 2021, 32, 4642–4662. [Google Scholar] [CrossRef]
- Younis, A.B.; Haddad, Y.; Kosaristanova, L.; Smerkova, K. Titanium dioxide nanoparticles: Recent progress in antimicrobial applications. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Stowe, C. 5 Overlooked High-Touch Hospital Surfaces. Available online: https://www.infectioncontroltoday.com/view/five-overlooked-high-touch-hospital-surfaces (accessed on 12 July 2022).
- Kundrapu, S.; Sunkesula, V.; Jury, L.A.; Sitzlar, B.M.; Donskey, C.J. Daily disinfection of high-touch surfaces in isolation rooms to reduce contamination of healthcare workers' hands. Infect. Control Hosp. Epidemiol. 2012, 33, 1039–1042. [Google Scholar] [CrossRef] [PubMed]
- Cobrado, L.; Silva-Dias, A.; Azevedo, M.M.; Rodrigues, A.G. High-touch surfaces: Microbial neighbours at hand. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 2053–2062. [Google Scholar] [CrossRef]
- JIS Z 2801:2000; Antimicrobial Products-Test for Antimicrobial Activity and Efficacy. Japanese Standards Association: Tokyo, Japan, 2001.
- ISO 22196:2011; Measurement of Antibacterial Activity on Plastics and Other Non-Porous Surfaces. International Standard Organisation: Geneva, Switzerland, 2011.
- Perez-Gavilan, A.; de Castro, J.V.; Arana, A.; Merino, S.; Retolaza, A.; Alves, S.A.; Francone, A.; Kehagias, N.; Sotomayor-Torres, C.M.; Cocina, D.; et al. Antibacterial activity testing methods for hydrophobic patterned surfaces. Sci. Rep. 2021, 11, 6675. [Google Scholar] [CrossRef] [PubMed]
- Michels, H.T.; Noyce, J.O.; Keevil, C.W. Effects of temperature and humidity on the efficacy of methicillin-resistantStaphylococcus aureuschallenged antimicrobial materials containing silver and copper. Lett. Appl. Microbiol. 2009, 49, 191–195. [Google Scholar] [CrossRef] [PubMed]
- US Environmental Protection Agency Office of Pesticide Programs. Interim Method for the Evaluation of Bactericidal Activity of Hard, Non-Porous Copper-Containing Surface Products; US Environmental Protection Agency: Washington, DC, USA, 2020.
- ISO 27447:2019; Fine Ceramics (Advanced Ceramics, Advanced Technical Ceramics)—Test Method for Antibacterial Activity of Semiconducting Photocatalytic Materials. International Standard Organisation: Geneva, Switzerland, 2019.
- ISO 18071:2016; Fine Ceramics (Advanced Ceramics, Advanced Technical Ceramics)—Determination of Antiviral Activity of Semiconducting Photocatalytic Materials under Indoor Lighting Environment—Test Method Using Bacteriophage Q-Beta. International Standard Organisation: Geneva, Switzerland, 2016.
- ISO 18061:2014; Fine Ceramics (Advanced Ceramics, Advanced Technical Ceramics)—Determination of Antiviral Activity of Semiconducting Photocatalytic Materials—Test Method Using Bacteriophage Q-Beta. International Standard Organisation: Geneva, Switzerland, 2014.
- ISO 13125:2013; Fine Ceramics (Advanced Ceramics, Advanced Technical Ceramics)—Test Method for Antifungal Activity of Semiconducting Photocatalytic materials and Corrosion. International Standard Organisation: Geneva, Switzerland, 2013.
- ISO 20743:2021; Textiles—Determination of Antibacterial Activity of Textile Products. International Standard Organisation: Geneva, Switzerland, 2021.
- ASTM E2149-20; Standard Test Method for Determining the Antimicrobial Activity of Antimicrobial Agents under Dynamic Contact Conditions. ASTM International: West Conshohocken, PA, USA, 2020.
- Dundar Arisoy, F.; Kolewe, K.W.; Homyak, B.; Kurtz, I.S.; Schiffman, J.D.; Watkins, J.J. Bioinspired Photocatalytic Shark-Skin Surfaces with Antibacterial and Antifouling Activity via Nanoimprint Lithography. ACS Appl. Mater. Interfaces 2018, 10, 20055–20063. [Google Scholar] [CrossRef] [PubMed]
- Rieger, K.A.; Cho, H.J.; Yeung, H.F.; Fan, W.; Schiffman, J.D. Antimicrobial Activity of Silver Ions Released from Zeolites Immobilized on Cellulose Nanofiber Mats. ACS Appl. Mater. Interfaces 2016, 8, 3032–3040. [Google Scholar] [CrossRef]
- Kolewe, K.W.; Peyton, S.R.; Schiffman, J.D. Fewer Bacteria Adhere to Softer Hydrogels. ACS Appl. Mater. Interfaces 2015, 7, 19562–19569. [Google Scholar] [CrossRef]
- Mann, E.E.; Manna, D.; Mettetal, M.R.; May, R.M.; Dannemiller, E.M.; Chung, K.K.; Brennan, A.B.; Reddy, S.T. Surface micropattern limits bacterial contamination. Antimicrob. Resist. Infect. Control 2014, 3, 28. [Google Scholar] [CrossRef]
- Mukhopadhyay, R.D.; Vedhanarayanan, B.; Ajayaghosh, A. Creation of “Rose Petal” and “Lotus Leaf” Effects on Alumina by Surface Functionalization and Metal-Ion Coordination. Angew. Chem. 2017, 129, 16234–16238. [Google Scholar] [CrossRef]
- Meng, Q.; Wang, Z.; Chai, X.; Weng, Z.; Ding, R.; Dong, L. Fabrication of hematite (α-Fe2O3) nanoparticles using electrochemical deposition. Appl. Surf. Sci. 2016, 368, 303–308. [Google Scholar] [CrossRef]
- Kim, P.; Kreder, M.J.; Alvarenga, J.; Aizenberg, J. Hierarchical or not? Effect of the length scale and hierarchy of the surface roughness on omniphobicity of lubricant-infused substrates. Nano Lett. 2013, 13, 1793–1799. [Google Scholar] [CrossRef]
- Damodaran, V.B.; Murthy, N.S. Bio-inspired strategies for designing antifouling biomaterials. Biomater. Res. 2016, 20, 18. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Nanda, D. Methods and fabrication techniques of superhydrophobic surfaces. In Superhydrophobic Polymer Coatings; Elsevier: Amsterdam, The Netherlands, 2019; pp. 43–75. [Google Scholar]
- Chapman, R.G.; Ostuni, E.; Takayama, S.; Holmlin, R.E.; Yan, L.; Whitesides, G.M. Surveying for surfaces that resist the adsorption of proteins. J. Am. Chem. Soc. 2000, 122, 8303–8304. [Google Scholar] [CrossRef]
- Ostuni, E.; Chapman, R.G.; Holmlin, R.E.; Takayama, S.; Whitesides, G.M. A survey of structure-property relationships of surfaces that resist the adsorption of protein. Langmuir 2001, 17, 5605–5620. [Google Scholar] [CrossRef]
- Banerjee, I.; Pangule, R.C.; Kane, R.S. Antifouling coatings: Recent developments in the design of surfaces that prevent fouling by proteins, bacteria, and marine organisms. Adv. Mater. 2011, 23, 690–718. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.F.; Guan, Y.L.; Yang, D.Z.; Li, Z.; Yao, K.D. Antibacterial action of chitosan and carboxymethylated chitosan. J. Appl. Polym. Sci. 2001, 79, 1324–1335. [Google Scholar] [CrossRef]
- Francolini, I.; Vuotto, C.; Piozzi, A.; Donelli, G. Antifouling and antimicrobial biomaterials: An overview. APMIS 2017, 125, 392–417. [Google Scholar] [CrossRef]
- Gao, G.; Lange, D.; Hilpert, K.; Kindrachuk, J.; Zou, Y.; Cheng, J.T.J.; Kazemzadeh-Narbat, M.; Yu, K.; Wang, R.; Straus, S.K.; et al. The biocompatibility and biofilm resistance of implant coatings based on hydrophilic polymer brushes conjugated with antimicrobial peptides. Biomaterials 2011, 32, 3899–3909. [Google Scholar] [CrossRef]
- Siedenbiedel, F.; Tiller, J.C. Antimicrobial polymers in solution and on surfaces: Overview and functional principles. Polymers 2012, 4, 46–71. [Google Scholar] [CrossRef]
- Zasloff, M. Antimicrobial peptides of multicellular organisms. Nature 2002, 415, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Zander, Z.K.; Becker, M.L. Antimicrobial and Antifouling Strategies for Polymeric Medical Devices. ACS Macro Lett. 2018, 7, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Mathew, R.T. Greener Surface Anchoring Anti-Bacterials; University of Auckland: Auckland, New Zealand, 2019. [Google Scholar]
- Saseendran Nair, S.; Anand, V.; De Silva, K.; Wiles, S.; Swift, S. The antibacterial potency and antibacterial mechanism of a commercially available surface-anchoring quaternary ammonium salt (SAQAS)-based biocide in vitro. J. Appl. Microbiol. 2022, 133, 2583–2598. [Google Scholar] [CrossRef] [PubMed]
- Sambhy, V.; Peterson, B.R.; Sen, A. Multifunctional Silane Polymers for Persistent Surface Derivatization and Their Antimicrobial Properties. Langmuir 2008, 24, 7549–7558. [Google Scholar] [CrossRef]
- Legido-Quigley, C.; Marlin, N.D.; Melin, V.; Manz, A.; Smith, N.W. Advances in capillary electrochromatography and micro-high performance liquid chromatography monolithic columns for separation science. Electrophoresis 2003, 24, 917–944. [Google Scholar] [CrossRef] [PubMed]
- Robertson, J.; Dalton, J.; Wiles, S.; Gizdavic-Nikolaidis, M.; Swift, S. The tuberculocidal activity of polyaniline and functionalised polyanilines. PeerJ 2016, 4, e2795. [Google Scholar] [CrossRef] [PubMed]
- Robertson, J.; Gizdavic-Nikolaidis, M.; Swift, S. Investigation of Polyaniline and a Functionalised Derivative as Antimicrobial Additives to Create Contamination Resistant Surfaces. Materials 2018, 11, 436. [Google Scholar] [CrossRef] [PubMed]
- Robertson, J.; Gizdavic-Nikolaidis, M.; Nieuwoudt, M.K.; Swift, S. The antimicrobial action of polyaniline involves production of oxidative stress while functionalisation of polyaniline introduces additional mechanisms. PeerJ 2018, 6, e5135. [Google Scholar] [CrossRef] [PubMed]
- Marija Gizdavic-Nikolaidis, G.B.; Zujovic, Z. The Synthesis, Physical Properties, Bioactivity and Potential Applications of Polyanilines; Cambridge Scholars Publishing: Newcastle upon Tyne, UK, 2018; Volume 1. [Google Scholar]
- Gizdavic-Nikolaidis, M.R.; Bennett, J.R.; Swift, S.; Easteal, A.J.; Ambrose, M. Broad spectrum antimicrobial activity of functionalized polyanilines. Acta Biomater. 2011, 7, 4204–4209. [Google Scholar] [CrossRef]
- Rigo, S.; Cai, C.; Gunkel-Grabole, G.; Maurizi, L.; Zhang, X.; Xu, J.; Palivan, C.G. Nanoscience-Based Strategies to Engineer Antimicrobial Surfaces. Adv. Sci. 2018, 5, 1700892. [Google Scholar] [CrossRef]
- Li, Z.; Liu, L.; Zheng, H.; Meng, F.; Wang, F. Superhydrophobic, corrosion resistance, and antibacterial coating with delayed release of Ag ions. Compos. Commun. 2022, 31, 101134. [Google Scholar] [CrossRef]
- Bragg, P.D.; Rainnie, D.J. The effect of silver ions on the respiratory chain of Escherichia coli. Can. J. Microbiol. 1974, 20, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Durán, N.; Durán, M.; de Jesus, M.B.; Seabra, A.B.; Fávaro, W.J.; Nakazato, G. Silver nanoparticles: A new view on mechanistic aspects on antimicrobial activity. Nanomedicine 2016, 12, 789–799. [Google Scholar] [CrossRef] [PubMed]
- Warnes, S.L.; Highmore, C.J.; Keevil, C.W. Horizontal transfer of antibiotic resistance genes on abiotic touch surfaces: Implications for public health. mBio 2012, 3, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Panáček, A.; Kvítek, L.; Smékalová, M.; Večeřová, R.; Kolář, M.; Röderová, M.; Dyčka, F.; Šebela, M.; Prucek, R.; Tomanec, O.; et al. Bacterial resistance to silver nanoparticles and how to overcome it. Nat. Nanotechnol. 2017, 13, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Greene, N.P.; Koronakis, V. Bacterial Metal Resistance: Coping with Copper without Cooperativity? mBio 2021, 12, e00653-21. [Google Scholar] [CrossRef] [PubMed]
- Keevil, B. Copper Is Great at Killing Superbugs—So Why Don’t Hospitals Use It? Available online: https://theconversation.com/copper-is-great-at-killing-superbugs-so-why-dont-hospitals-use-it-73103 (accessed on 14 July 2022).
- Abraham, J.; Dowling, K.; Florentine, S. Can Copper Products and Surfaces Reduce the Spread of Infectious Microorganisms and Hospital-Acquired Infections? Materials 2021, 14, 3444. [Google Scholar] [CrossRef]
- Dauvergne, E.; Mullié, C. Brass Alloys: Copper-Bottomed Solutions against Hospital-Acquired Infections? Antibiotics 2021, 10, 286. [Google Scholar] [CrossRef]
- Montero, D.A.; Arellano, C.; Pardo, M.; Vera, R.; Gálvez, R.; Cifuentes, M.; Berasain, M.A.; Gómez, M.; Ramírez, C.; Vidal, R.M. Antimicrobial properties of a novel copper-based composite coating with potential for use in healthcare facilities. Antimicrob. Resist. Infect. Control 2019, 8, 3. [Google Scholar] [CrossRef] [PubMed]
- Mitra, D.; Kang, E.-T.; Neoh, K.G. Antimicrobial Copper-Based Materials and Coatings: Potential Multifaceted Biomedical Applications. ACS Appl. Mater. Interfaces 2019, 12, 21159–21182. [Google Scholar] [CrossRef]
- Schmidt, M.G.; Attaway, H.H.; Sharpe, P.A.; John, J.; Sepkowitz, K.A.; Morgan, A.; Fairey, S.E.; Singh, S.; Steed, L.L.; Cantey, J.R.; et al. Sustained Reduction of Microbial Burden on Common Hospital Surfaces through Introduction of Copper. J. Clin. Microbiol. 2012, 50, 2217–2223. [Google Scholar] [CrossRef] [PubMed]
- US Environmental Protection Agency. Protocol for the Evaluation of Bactericidal Activity of Hard, Non-Porous Copper Containing Surface Products; US Environmental Protection Agency: Washington, DC, USA, 2016.
- Tamilvanan, S.; Venkateshan, N.; Ludwig, A. The potential of lipid- and polymer-based drug delivery carriers for eradicating biofilm consortia on device-related nosocomial infections. J. Control. Release 2008, 128, 2–22. [Google Scholar] [CrossRef] [PubMed]
- Gollwitzer, H.; Ibrahim, K.; Meyer, H.; Mittelmeier, W.; Busch, R.; Stemberger, A. Antibacterial poly(D,L-lactic acid) coating of medical implants using a biodegradable drug delivery technology. J. Antimicrob. Chemother. 2003, 51, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Shukla, A.; Fleming, K.E.; Chuang, H.F.; Chau, T.M.; Loose, C.R.; Stephanopoulos, G.N.; Hammond, P.T. Controlling the release of peptide antimicrobial agents from surfaces. Biomaterials 2010, 31, 2348–2357. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.W.; Knowles, J.C.; Kim, H.E. Hydroxyapatite/poly(ε-caprolactone) composite coatings on hydroxyapatite porous bone scaffold for drug delivery. Biomaterials 2004, 25, 1279–1287. [Google Scholar] [CrossRef] [PubMed]
- Stigter, M.; Bezemer, J.; De Groot, K.; Layrolle, P. Incorporation of different antibiotics into carbonated hydroxyapatite coatings on titanium implants, release and antibiotic efficacy. J. Control. Release 2004, 99, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Aymonier, C.; Schlotterbeck, U.; Antonietti, L.; Zacharias, P.; Thomann, R.; Tiller, J.C.; Mecking, S. Hybrids of silver nanoparticles with amphiphilic hyperbranched macromolecules exhibiting antimicrobial properties. Chem. Commun. 2002, 24, 3018–3019. [Google Scholar] [CrossRef] [PubMed]
- Ramage, G.; Saville, S.P.; Wickes, B.L.; Lopez-Ribot, J.L. Inhibition of Candida albicans biofilm formation by farnesol, a quorum-sensing molecule. Appl. Environ. Microbiol. 2002, 68, 5459–5463. [Google Scholar] [CrossRef]
- Defoirdt, T.; Boon, N.; Bossier, P.; Verstraete, W. Disruption of bacterial quorum sensing: An unexplored strategy to fight infections in aquaculture. Aquaculture 2004, 240, 69–88. [Google Scholar] [CrossRef]
- Komnatnyy, V.V.; Chiang, W.C.; Tolker-Nielsen, T.; Givskov, M.; Nielsen, T.E. Bacteria-triggered release of antimicrobial agents. Angew. Chem. Int. Ed. 2014, 53, 439–441. [Google Scholar] [CrossRef] [PubMed]
- Lange, R.P.; Locher, H.H.; Wyss, P.C.; Then, R.L. The targets of currently used antibacterial agents: Lessons for drug discovery. Curr. Pharm. Des. 2007, 13, 3140–3154. [Google Scholar] [CrossRef]
- Tanihara, M.; Suzuki, Y.; Nishimura, Y.; Suzuki, K.; Kakimaru, Y. Thrombin-sensitive peptide linkers for biological signal-responsive drug release systems. Peptides 1998, 19, 421–425. [Google Scholar] [CrossRef]
- Yu, Q.; Johnson, L.M.; Lõpez, G.P. Nanopatterned polymer brushes for triggered detachment of anchorage-dependent cells. Adv. Funct. Mater. 2014, 24, 3751–3759. [Google Scholar] [CrossRef]
- Yu, Q.; Ista, L.K.; Gu, R.; Zauscher, S.; López, G.P. Nanopatterned polymer brushes: Conformation, fabrication and applications. Nanoscale 2016, 8, 680–700. [Google Scholar] [CrossRef] [PubMed]
- Wei, T.; Zhan, W.; Yu, Q.; Chen, H. Smart Biointerface with Photoswitched Functions between Bactericidal Activity and Bacteria-Releasing Ability. ACS Appl. Mater. Interfaces 2017, 9, 25767–25774. [Google Scholar] [CrossRef]
- Wei, T.; Tang, Z.; Yu, Q.; Chen, H. Smart Antibacterial Surfaces with Switchable Bacteria-Killing and Bacteria-Releasing Capabilities. ACS Appl. Mater. Interfaces 2017, 9, 37511–37523. [Google Scholar] [CrossRef] [PubMed]
- Akers, P.W.; Dingley, A.J.; Swift, S.; Nelson, A.R.J.; Martin, J.; McGillivray, D.J. Using Neutron Reflectometry to Characterize Antimicrobial Protein Surface Coatings. J. Phys. Chem. B 2017, 121, 5908–5916. [Google Scholar] [CrossRef] [PubMed]
- Karkhanechi, H.; Razi, F.; Sawada, I.; Takagi, R.; Ohmukai, Y.; Matsuyama, H. Improvement of antibiofouling performance of a reverse osmosis membrane through biocide release and adhesion resistance. Sep. Purif. Technol. 2013, 105, 106–113. [Google Scholar] [CrossRef]
- Qu, Z.; Xu, H.; Gu, H. Synthesis and biomedical applications of poly((meth)acrylic acid) brushes. ACS Appl. Mater. Interfaces 2015, 7, 14537–14551. [Google Scholar] [CrossRef]
- Kang, C.; Ahn, D.; Roh, C.; Kim, S.S.; Lee, J. Development of Synergistic Antimicrobial Coating of p-Aramid Fibers Using Ag Nanoparticles and Glycidyltrimethylammonium Chloride (GTAC) without the Aid of a Cross-Linking Agent. Polymers 2017, 9, 357. [Google Scholar] [CrossRef]
- Tadashi Matsunaga, R.; Nakajima, T.; Wake, H. Photoelectrochemical sterilization of microbial cells by semiconductor powders. FEMS Microbiol. Lett. 1985, 29, 211–214. [Google Scholar] [CrossRef]
- Byrne, J.; Dunlop, P.; Hamilton, J.; Fernández-Ibáñez, P.; Polo-López, I.; Sharma, P.; Vennard, A. A Review of Heterogeneous Photocatalysis for Water and Surface Disinfection. Molecules 2015, 20, 5574–5615. [Google Scholar] [CrossRef] [PubMed]
- Ramsden, J.J. Can bacteria develop resistance to photocatalytically generated reactive oxygen species? J. Biol. Phys. Chem. 2017, 17, 47–51. [Google Scholar] [CrossRef]
- Onodera, A.; Nishiumi, F.; Kakiguchi, K.; Tanaka, A.; Tanabe, N.; Honma, A.; Yayama, K.; Yoshioka, Y.; Nakahira, K.; Yonemura, S.; et al. Short-term changes in intracellular ROS localisation after the silver nanoparticles exposure depending on particle size. Toxicol. Rep. 2015, 2, 574–579. [Google Scholar] [CrossRef]
- Bogdan, J.; Zarzyńska, J.; Pławińska-Czarnak, J. Comparison of Infectious Agents Susceptibility to Photocatalytic Effects of Nanosized Titanium and Zinc Oxides: A Practical Approach. Nanoscale Res. Lett. 2015, 10, 309. [Google Scholar] [CrossRef]
- Wang, R.; Hashimoto, K.; Fujishima, A.; Chikuni, M.; Kojima, E.; Kitamura, A.; Shimohigoshi, M.; Watanabe, T.J.N. Light-induced amphiphilic surfaces. Nature 1997, 388, 431–432. [Google Scholar] [CrossRef]
- Zhou, Z.; Li, B.; Liu, X.; Li, Z.; Zhu, S.; Liang, Y.; Cui, Z.; Wu, S. Recent Progress in Photocatalytic Antibacterial. ACS Appl. Bio Mater. 2021, 4, 3909–3936. [Google Scholar] [CrossRef]
- Leyland, N.S.; Podporska-Carroll, J.; Browne, J.; Hinder, S.J.; Quilty, B.; Pillai, S.C. Highly Efficient F, Cu doped TiO2 anti-bacterial visible light active photocatalytic coatings to combat hospital-acquired infections. Sci. Rep. 2016, 6, 24770. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Shen, R.; Qin, L.; Kang, S.-Z.; Li, X. Metal organic frameworks mediated silver nanoparticles in the TiO2 coated copper sheet for synergetically enhanced surface enhanced Raman scattering and photocatalytic activities. Appl. Surf. Sci. 2022, 585, 152715. [Google Scholar] [CrossRef]
- Fujishima, A.; Zhang, X.; Tryk, D. Heterogeneous photocatalysis: From water photolysis to applications in environmental cleanup. Int. J. Hydrogen Energy 2007, 32, 2664–2672. [Google Scholar] [CrossRef]
- Chung, C.-J.; Lin, H.-I.; Tsou, H.-K.; Shi, Z.-Y.; He, J.-L. An antimicrobial TiO2 coating for reducing hospital-acquired infection. J. Biomed. Mater. Res. Part B Appl. Biomater. 2008, 85B, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Nanoksi’s Photocatalytic Nanocoating Provides Continuous Surface Disinfection. Available online: https://coatings.specialchem.com/news/industry-news/photocatalytic-nanocoating-surface-disinfection-000224391?li=20019065&lr=ipc21041650&utm_campaign=CI-Industry-NL&utm_medium=email&_hsmi=120264998&_hsenc=p2ANqtz-_y5Wx87gziVC1t1rNyc5IVlXosp3IdFoVdd_W-p-7uq27msxaXet0zj7-_km_6ZvIkdcnIU0gGJCt7ulwh5y2AFpt3Fij85k-_VNt7ch3imDlDWlk&utm_content=120264998&utm_source=hs_email (accessed on 10 September 2022).
- Nanoksi. Finnish Invisible Innovation Protects against the Bad. Available online: https://nanoksi.com/en/blog/finnish-invisible-innovation-protects-against-the-bad/ (accessed on 10 September 2022).
- Demir, B.; Cerkez, I.; Worley, S.D.; Broughton, R.M.; Huang, T.-S. N-Halamine-Modified Antimicrobial Polypropylene Nonwoven Fabrics for Use against Airborne Bacteria. ACS Appl. Mater. Interfaces 2015, 7, 1752–1757. [Google Scholar] [CrossRef] [PubMed]
- Dong, A.; Wang, Y.-J.; Gao, Y.; Gao, T.; Gao, G. Chemical Insights into Antibacterial N-Halamines. Chem. Rev. 2017, 117, 4806–4862. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Cao, Z.; Porteous, N.; Sun, Y. An N-halamine-based rechargeable antimicrobial and biofilm controlling polyurethane. Acta Biomater. 2012, 8, 1498–1506. [Google Scholar] [CrossRef]
- Jiang, Z.M.; Liu, Y.; Li, R.; Ren, X.H.; Huang, T.S. Preparation of antibacterial cellulose with a monochloro-s-triazine-based N-halamine biocide. Polym. Adv. Technol. 2016, 27, 460–465. [Google Scholar] [CrossRef]
- Kocer, H.B.; Cerkez, I.; Worley, S.D.; Broughton, R.M.; Huang, T.S. N-Halamine Copolymers for Use in Antimicrobial Paints. ACS Appl. Mater. Interfaces 2011, 3, 3189–3194. [Google Scholar] [CrossRef]
- Hui, F.; Debiemme-Chouvy, C. Antimicrobial N-Halamine Polymers and Coatings: A Review of Their Synthesis, Characterization, and Applications. Biomacromolecules 2013, 14, 585–601. [Google Scholar] [CrossRef]
- Timofeeva, L.; Kleshcheva, N. Antimicrobial polymers: Mechanism of action, factors of activity, and applications. Appl. Microbiol. Biotechnol. 2011, 89, 475–492. [Google Scholar] [CrossRef]
- Kocer, K.B.; Akdag, A.; Ren, X.; Broughton, R.M.; Worley, S.D.; Huang, T.S. Effect of alkyl derivatization on several properties of N-halamine antimicrobial siloxane coatings. Ind. Eng. Chem. Res. 2008, 47, 7558–7563. [Google Scholar] [CrossRef]
- Yao, J.R.; Sun, Y.Y. Preparation and characterization of polymerizable hindered amine-based antimicrobial fibrous materials. Ind. Eng. Chem. Res. 2008, 47, 5819–5824. [Google Scholar] [CrossRef]
- Cao, Z.B.; Sun, Y.Y. Polymeric N-Halamine Latex Emulsions for Use in Antimicrobial Paints. ACS Appl. Mater. Interfaces 2009, 1, 494–504. [Google Scholar] [CrossRef]
- Xuehong, R.; Changyun, Z.; Lei, K.; Worley, S.D.; Kocer, H.B.; Broughton, R.M.; Huang, T.S. Acyclic N-Halamine Polymeric Biocidal Films. J. Bioact. Compat. Polym. 2010, 25, 392–405. [Google Scholar] [CrossRef]
- Kocer, H.B.; Cerkez, I.; Worley, S.D.; Broughton, R.M.; Huang, T.S. Polymeric Antimicrobial N-Halamine Epoxides. ACS Appl. Mater. Interfaces 2011, 3, 2845–2850. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.H.; Kou, L.; Kocer, H.B.; Worley, S.D.; Broughton, R.M.; Tzou, Y.M.; Huang, T.S. Antimicrobial Modification of Polyester by Admicellar Polymerization. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 89b, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.M.; Ma, K.K.; Du, J.M.; Li, R.; Ren, X.H.; Huang, T.S. Synthesis of novel reactive N-halamine precursors and application in antimicrobial cellulose. Appl. Surf. Sci. 2014, 288, 518–523. [Google Scholar] [CrossRef]
- Cerkez, I.; Kocer, H.B.; Worley, S.D.; Broughton, R.M.; Huang, T.S. N-halamine copolymers for biocidal coatings. React. Funct. Polym. 2012, 72, 673–679. [Google Scholar] [CrossRef]
- Kocer, H.B. Residual disinfection with N-halamine based antimicrobial paints. Prog. Org. Coat. 2012, 74, 100–105. [Google Scholar] [CrossRef]
- Ren, X.H.; Akdag, A.; Zhu, C.; Kou, L.; Worley, S.D.; Huang, T.S. Electrospun polyacrylonitrile nanofibrous biomaterials. J. Biomed. Mater. Res. A 2009, 91a, 385–390. [Google Scholar] [CrossRef]
- Worley, S.D.; Williams, D.E.; Barnela, S.B. The Stabilities of New N-Halamine Water Disinfectants. Water Res. 1987, 21, 983–988. [Google Scholar] [CrossRef]
- Worley, S.D.; Burkett, H.D. The Stability in Water of a New Chloramine Disinfectant as a Function of Ph, Temperature, and Water-Quality. Water Resour. Bull. 1984, 20, 365–368. [Google Scholar] [CrossRef]
- Li, C.H.; Xue, L.Y.; Cai, Q.; Bao, S.; Zhao, T.Y.; Xiao, L.H.; Gao, G.; Harnoode, C.; Dong, A. Design, synthesis and biocidal effect of novel amine N-halamine microspheres based on 2,2,6,6-tetramethyl-4-piperidinol as promising antibacterial agents. RSC Adv. 2014, 4, 47853–47864. [Google Scholar] [CrossRef]
- Gutman, O.; Natan, M.; Banin, E.; Margel, S. Characterization and antibacterial properties of N-halamine-derivatized cross-linked polymethacrylamide nanoparticles. Biomaterials 2014, 35, 5079–5087. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Jiao, Y.C.; Kang, Z.Z.; Ma, K.K.; Ren, X.H.; Liang, J. Durable antimicrobial cotton fabrics containing stable quaternarized N-halamine groups. Cellulose 2013, 20, 3067–3077. [Google Scholar] [CrossRef]
- Zhao, N.; Logsetty, S.; Liu, S. Durability of Amide N-Chloramine Biocides to Ethylene Oxide Sterilization. J. Burn Care Res. 2012, 33, E201–E206. [Google Scholar] [CrossRef]
- Calvo, P.; Crugeiras, J.; Rios, A.; Rios, M.A. Nucleophilic substitution reactions of N-chloramines: Evidence for a change in mechanism with increasing nucleophile reactivity. J. Org. Chem. 2007, 72, 3171–3178. [Google Scholar] [CrossRef]
- MacCrehan, W.A.; Bedner, M.; Helz, G.R. Making chlorine greener: Performance of alternative dechlorination agents in wastewater. Chemosphere 2005, 60, 381–388. [Google Scholar] [CrossRef]
- Barnes, K.; Liang, J.; Wu, R.; Worley, S.D.; Lee, J.; Broughton, R.M.; Huang, T.S. Synthesis and antimicrobial applications of 5,5′-ethylenebis[5-methyl-3-(3-triethoxysilylpropyl)hydantoin]. Biomaterials 2006, 27, 4825–4830. [Google Scholar] [CrossRef]
- Ahmed, A.E.-S.I.; Hay, J.N.; Bushell, M.E.; Wardell, J.N.; Cavalli, G. Biocidal polymers (II): Determination of biological activity of novel N-halamine biocidal polymers and evaluation for use in water filters. React. Funct. Polym. 2008, 68, 1448–1458. [Google Scholar] [CrossRef]
- Ahmed, A.E.-S.I.; Hay, J.N.; Bushell, M.E.; Wardell, J.N.; Cavalli, G. Optimizing halogenation conditions of N-halamine polymers and investigating mode of bactericidal action. J. Appl. Polym. Sci. 2009, 113, 2404–2412. [Google Scholar] [CrossRef]
- Gerson, S.H.; Worley, S.D.; Bodor, N.; Kaminski, J.J. Electronic structures of some antimicrobial N-chloramines. Possible existence of intramolecular hydrogen bonding and its effect on germicidal efficiency. J. Med. Chem. 1978, 21, 686–688. [Google Scholar] [CrossRef]
- Liu, S.; Zheng, J.; Hao, L.; Yegin, Y.; Bae, M.; Ulugun, B.; Taylor, T.M.; Scholar, E.A.; Cisneros-Zevallos, L.; Oh, J.K.; et al. Dual-Functional, Superhydrophobic Coatings with Bacterial Anticontact and Antimicrobial Characteristics. ACS Appl. Mater. Interfaces 2020, 12, 21311–21321. [Google Scholar] [CrossRef] [PubMed]
- Bergeson & Campbell P.C. EPA Provides Expedited Pathway for Companies to Claim “LongLasting” Efficacy for Antiviral Products. Available online: https://www.lexology.com/library/detail.aspx?g=ae68716a-6a43-4485-91fc-4c7f0f24a324 (accessed on 28 July 2022).
- US Environmental Protection Agency Office of Pesticide Programs. Antimicrobial Testing Methods & Procedures: Interim Method for Evaluating the Efficacy of Antimicrobial Surface Coatings; US Environmental Protection Agency: Washington, DC, USA, 2020.
- EPA MLB SOP-MB-31; Procedure for the OECD Quantitative Method for Testing Antimicrobial Products again st Spores of Clostridium difficile (ATCC 43598) on Inanimate, Hard, Non-Porous Surfaces. US Environmental Protection Agency Office of Pesticide Programs: Washington, DC, USA, 2017.
- Hosseini, M.; Chin, A.W.H.; Behzadinasab, S.; Poon, L.L.M.; Ducker, W.A. Cupric Oxide Coating That Rapidly Reduces Infection by SARS-CoV-2 via Solids. ACS Appl. Mater. Interfaces 2021, 13, 5919–5928. [Google Scholar] [CrossRef]
- Jiang, R.; Hao, L.; Song, L.; Tian, L.; Fan, Y.; Zhao, J.; Liu, C.; Ming, W.; Ren, L. Lotus-leaf-inspired hierarchical structured surface with non-fouling and mechanical bactericidal performances. Chem. Eng. J. 2020, 398, 125609. [Google Scholar] [CrossRef]
- Buxadera-Palomero, J.; Albó, K.; Gil, F.J.; Mas-Moruno, C.; Rodríguez, D. Polyethylene glycol pulsed electrodeposition for the development of antifouling coatings on titanium. Coatings 2020, 10, 456. [Google Scholar] [CrossRef]
- Ramos, M.; Beltran, A.; Fortunati, E.; Peltzer, M.; Cristofaro, F.; Visai, L.; Valente, A.J.M.; Jiménez, A.; Kenny, J.M.; Garrigós, M.C. Controlled Release of Thymol from Poly(Lactic Acid)-Based Silver Nanocomposite Films with Antibacterial and Antioxidant Activity. Antioxidants 2020, 9, 395. [Google Scholar] [CrossRef]
- Chen, J.; Shi, X.; Zhu, Y.; Chen, Y.; Gao, M.; Gao, H.; Liu, L.; Wang, L.; Mao, C.; Wang, Y. On-demand storage and release of antimicrobial peptides using Pandora's box-like nanotubes gated with a bacterial infection-responsive polymer. Theranostics 2020, 10, 109–122. [Google Scholar] [CrossRef]
- Ikner, L.A.; Torrey, J.R.; Gundy, P.M.; Gerba, C.P. Efficacy of an antimicrobial surface coating against human coronavirus 229E and SARS-CoV-2. Am. J. Infect. Control 2021, 49, 1569–1571. [Google Scholar] [CrossRef]
- Zou, Y.; Lu, K.; Lin, Y.; Wu, Y.; Wang, Y.; Li, L.; Huang, C.; Zhang, Y.; Brash, J.L.; Chen, H.; et al. Dual-Functional Surfaces Based on an Antifouling Polymer and a Natural Antibiofilm Molecule: Prevention of Biofilm Formation without Using Biocides. ACS Appl. Mater. Interfaces 2021, 13, 45191–45200. [Google Scholar] [CrossRef]
- Vélez-Peña, E.; Pérez-Obando, J.; Pais-Ospina, D.; Marín-Silva, D.A.; Pinotti, A.; Cánneva, A.; Donadelli, J.A.; Damonte, L.; Pizzio, L.R.; Osorio-Vargas, P.; et al. Self-cleaning and antimicrobial photo-induced properties under indoor lighting irradiation of chitosan films containing Melon/TiO2 composites. Appl. Surf. Sci. 2020, 508, 144895. [Google Scholar] [CrossRef]
- Ma, Y.; Wisuthiphaet, N.; Bolt, H.; Nitin, N.; Zhao, Q.; Wang, D.; Pourdeyhimi, B.; Grondin, P.; Sun, G. N-Halamine Polypropylene Nonwoven Fabrics with Rechargeable Antibacterial and Antiviral Functions for Medical Applications. ACS Biomater. Sci. Eng. 2021, 7, 2329–2336. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Coating/Surface | Method | Summary | Advantages/Disadvantages |
|---|---|---|---|
| Plastics and other non-porous surfaces | JIS Z 2801 or ISO 22196 [93,94] | Inoculate a known amount of bacteria on a surface. The inoculum is covered using a sterile plastic square piece to ensure uniform spreading and to avoid evaporation of the inoculum. After incubation, the system is transferred to a known volume of selected wash solution, and the surviving bacteria are enumerated by colony counts. The result is interpreted as a log reduction in colony count with respect to control obtained the next day after incubating the plates at 37 °C. | Widely accepted standard to test the antimicrobial potency of coatings. During the washing step, the active biocides may leach out and kill the microbes causing errors in the result. This can be prevented by using neutralizers for the biocide; however, it is dependent upon the concentration of neutralizer, concentration of leachates and specificity of the neutralizer. Some studies report that this method does not reflect real-world conditions of temperature and humidity [95]. It is limited to hard non-porous surfaces only. |
| Copper alloys and silver containing surfaces | Dry fomite assay [96] | A known amount of pathogen is inoculated on the sample surface, and this is incubated under 22 °C and 50% RH for different time intervals, with the surface drying with time. Viable cells removed from the surface by application of a wash solution allow effectiveness to be quantified in comparison to a control surface. | In this method, we test the antimicrobial efficacy under low levels of temperature and humidity to replicate indoor conditions. The RH value is >90% for JIS Z 2801 assay, which may be called as a wet fomite test, while this test ensures a more real-world humidity. |
| Hard, non-porous copper containing surfaces | EPA assay [97] | The Environmental Protection Agency (EPA), US proposed this interim protocol to study the continuous antimicrobial efficacy of a copper containing surface. The protocol is similar to JIS Z 2801; however, it specifies the periodic chemical exposure and mechanical abrasion of the surface. After six weeks of applied wear and tear, the antimicrobial activity of the Cu coating is tested for a period of 2 h. This protocol may be adopted to study the durability of coatings for indoor purposes. | Antibacterial activity monitored with regular cycles of physical abrasion and chemical treatment. Potentially applicable to other non-porous surfaces. |
| Photocatalytic coatings | ISO 27447 [98], ISO 18071 [99], ISO 18061 [100], ISO 13125 [101] | This standard applies to all photocatalytic coatings. The assay is similar to JIS Z 2801 but conducted under two illumination conditions. The sample is treated with the pathogen and allowed to incubate under dark and light conditions (ultraviolet or visible light of known intensity and wavelength) simultaneously. After the illumination period, viable cells are recovered from the surface and enumerated as described in JIS Z 2801 assay. | The standards provide a protocol for testing the efficacy of photocatalytic coatings against bacteria, viruses and fungi. A protocol to test activity under dry conditions is not given. |
| Textile products/surfaces | ISO 20743 [102] | This standard specifies three inoculation methods: absorption, transfer, and printing method. In the absorption method, the sterile sample is inoculated with a known amount of bacteria, and the system is treated immediately with 20 mL of wash solution, with shaking for 18–24 h at 37 °C. The final concentration of bacteria is determined using the colony count method. Activity compares cells recovered at time zero and after incubation. The transfer method inoculates the sample by touch transfer from an agar plate with recovery of viable cells at time zero and after incubation for 18–24 h at 37 °C. Activity compares cells recovered at time zero and after incubation. In the printing method, a known amount of bacteria is filtered onto a membrane. Bacteria are transferred to the sample by pressing the test piece on the filter using a weight and rotating 180°. The rest of the procedure follows as described in transfer method. | In some cases, this standard should be combined with other protocols depending on the material used. For example, a textile impregnated with photocatalytic material may need a modified protocol combining both ISO 20743 and ISO 27477 assay. |
| Surfaces, where substrates (fiber, fabric or other substrate) bonded with antimicrobial agents. | ASTM E2149 [103] | This method is used to determine the activity of a sample immersed and shaken in a concentrated bacterial suspension for 1 h. Surviving bacteria are enumerated by colony counting, with activity measured after comparison of viable colonies recovered at time zero and after 1 h. The experiment is simultaneously performed using an appropriate control. | This assay can be modified to assess the antibacterial activity of coatings and thin films [104,105]. |
| Antifouling surfaces | Immersion inoculation assay [95,104,106,107] | The sample is suspended or immersed in a known amount of bacteria. After the required incubation period, the growth media is carefully removed using a sterile pipette and the samples are rinsed to remove residual broth with phosphate buffered saline. The bacteria remaining on the surface are determined using a colony count method or microscopy. | This test can be used to identify the repelling or antifouling activity of a coating under wet conditions [95]. |
| Hydrophobic micropattern surfaces | Touch transfer and swab inoculation assay [95,107] | This is reported as the best method for determining anti-attachment and antibacterial activity of nano or micro patterned hydrophobic surfaces [95]. In the touch transfer assay, a sterile velveteen cloth is wrapped on top of a cylindrical weight and the tied cloth is immersed in a known amount of pathogen. The excess liquid is drained out using another piece of cloth and the tied cloth is pressed on to the surface of the sample. In order to get the colony count, after transferring the pathogen on to the sample, it is pressed to a fresh agar plate on the sample surface and incubated at 37 °C for 24 h. As an alternative method of inoculation, a cotton swab charged with a known amount of bacteria can be used. | This test can be used to identify both antifouling and anti-microbial activity of coating under dry conditions. The test better mimics real-life conditions [95]. |
| N-halamine Type | Structural Stability [178,202] | UV Light Stability [178,182] | Indoor Light Stability [178,192] | Water/Hydrolysis Stability [178,182,196,197] | Antimicrobial Activity [178,182,203,204,205] | |
|---|---|---|---|---|---|---|
| Chemical structure | Cyclic | * | High | High | High | * |
| Acyclic | * | Low | Low | Low | * | |
| Functional group | Amine | High | * | * | High | Low |
| Imide | Low | * | * | Low | High | |
| Amide | Moderate | * | * | Moderate | Moderate | |
| Multiple >N-Cl bonds | * | * | * | * | Highest | |
| >N-X | F | * | * | * | * | * |
| Cl | * | * | * | * | Low | |
| Br | * | * | * | * | Moderate | |
| I | * | * | * | * | High | |
| Type of Surface | Active Component | Conditions | Tested Pathogens | Activity (Microbe Repelled/Killed) | |
|---|---|---|---|---|---|
| Inoculum | RH, T and t | ||||
| Nanostructured AFC | Superhydrophobic surface integrated with micro-pillar arrays and packed nanoneedles [211] | 2 mL 108 cfu/mL | 37 °C 24 h | E. coli | >99%* |
| Chemically modified AFC | PEG [212] | 5 µL 108 cfu/mL | 37 °C 2 h | S. aureus E. coli | 90%* 90%* |
| Continuous releasing AMC | Cupric oxide [210] | 5 µL 107 TCID50/mL | 60−70%, 22−23 °C 30 min | SARS-CoV-2 | 99.8% |
| Slow releasing AMC | Silver and Thymol in poly(lactic acid) films [213] | 100 µL 104 cfu/mL | 24 °C, 3 h | S. aureus E. coli | 47.5% 40.6% |
| Triggered releasing AMC | pH responsive poly(methacrylic acid) with antimicrobial peptide [214] | 250 µL 107 cfu/mL | 1 h | S. aureus E. coli P. aeruginosa MRSA | 99.9% 99.9% 99.9% 99.9% |
| Contact active AMC | Quaternary ammonium polymer coating [215] | 50 µL | 30–50%, 22–23 °C, 2 h | SARS-CoV-2 Human coronavirus 229E | >3 log >5 log |
| Contact-killing and repelling coatings | Nano silica and fluorosilane with Lysozyme (muramidase) [206] | 1 mL/cm2 of 6.3 and 6.6 log cfu/mL | 150 rpm, 24 h | Listeria innocua Salmonella Typhimurium LT2 | 4 log# 6.5 log# |
| Releasing and repelling coatings | Copolymer brushes of 2-hydroxyethyl methacrylate and 3-(acrylamido)phenylboronic acid with Quercetin [216] | 500 µL 107 cfu/mL | 37 °C, 4 h | S. aureus P. aeruginosa | >80% >80% |
| Photocatalytic coatings | Melon/TiO2 [217] | 20 µL 106 cfu/mL | Actinic light 3 h | S. aureus | 99.9% |
| Rechargeable coatings | Polypropylene grafted methacrylamide [218] | 10 µL 107 cfu/mL 10 µL 107 pfu/mL | 15 min for bacteria and 5 min for virus | L. innocua E. coli T7 phage | >5 log >5 log 7 log |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jose, A.; Gizdavic-Nikolaidis, M.; Swift, S. Antimicrobial Coatings: Reviewing Options for Healthcare Applications. Appl. Microbiol. 2023, 3, 145-174. https://doi.org/10.3390/applmicrobiol3010012
Jose A, Gizdavic-Nikolaidis M, Swift S. Antimicrobial Coatings: Reviewing Options for Healthcare Applications. Applied Microbiology. 2023; 3(1):145-174. https://doi.org/10.3390/applmicrobiol3010012
Chicago/Turabian StyleJose, Ajay, Marija Gizdavic-Nikolaidis, and Simon Swift. 2023. "Antimicrobial Coatings: Reviewing Options for Healthcare Applications" Applied Microbiology 3, no. 1: 145-174. https://doi.org/10.3390/applmicrobiol3010012
APA StyleJose, A., Gizdavic-Nikolaidis, M., & Swift, S. (2023). Antimicrobial Coatings: Reviewing Options for Healthcare Applications. Applied Microbiology, 3(1), 145-174. https://doi.org/10.3390/applmicrobiol3010012