
Empowering Potential of the My Assistive Technology Guide: Exploring Experiences and User Perspectives


Abstract
1. Introduction
2. Materials and Methods
2.1. Karagianni’s Optimized Honeycomb Model
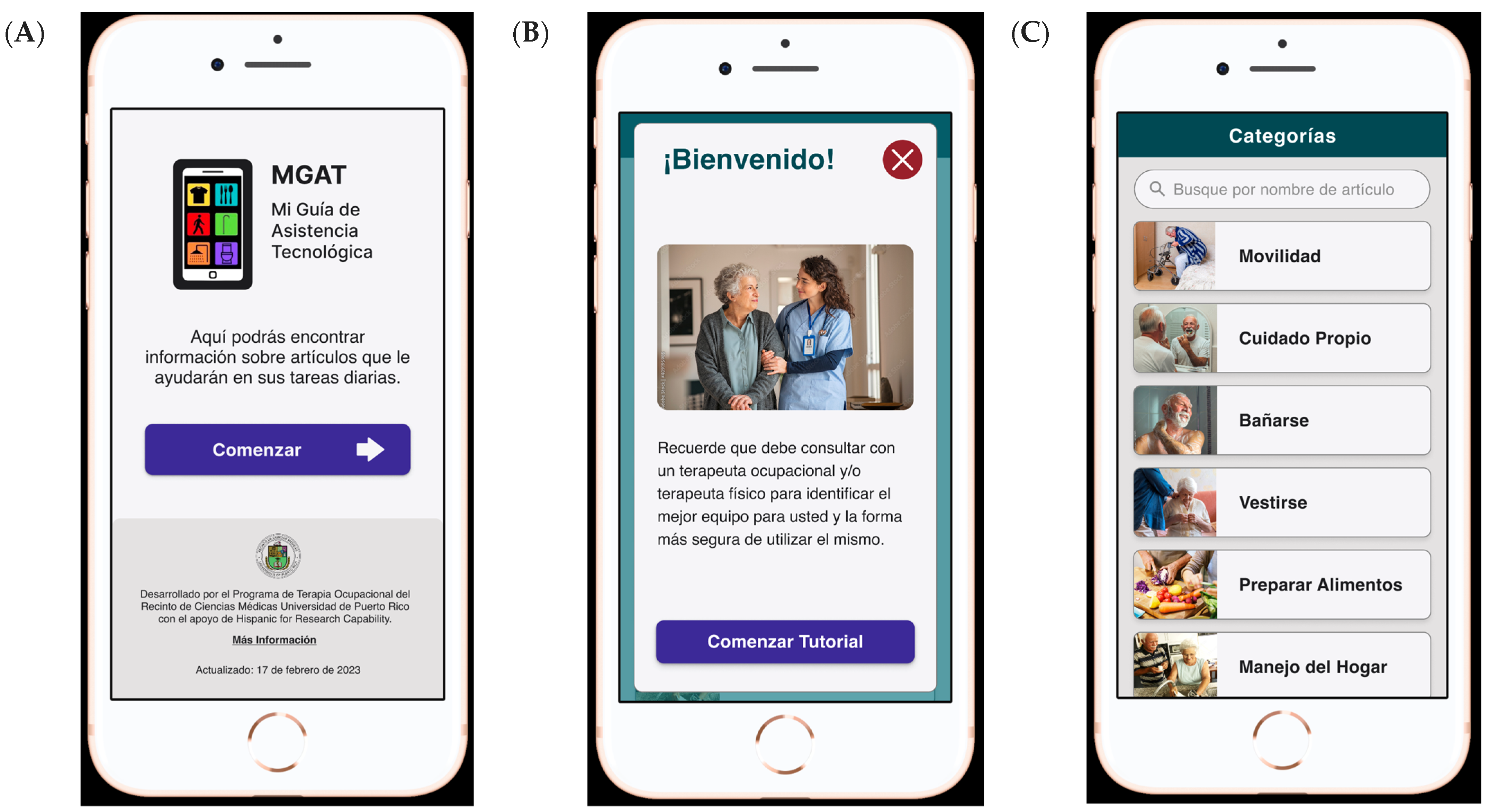
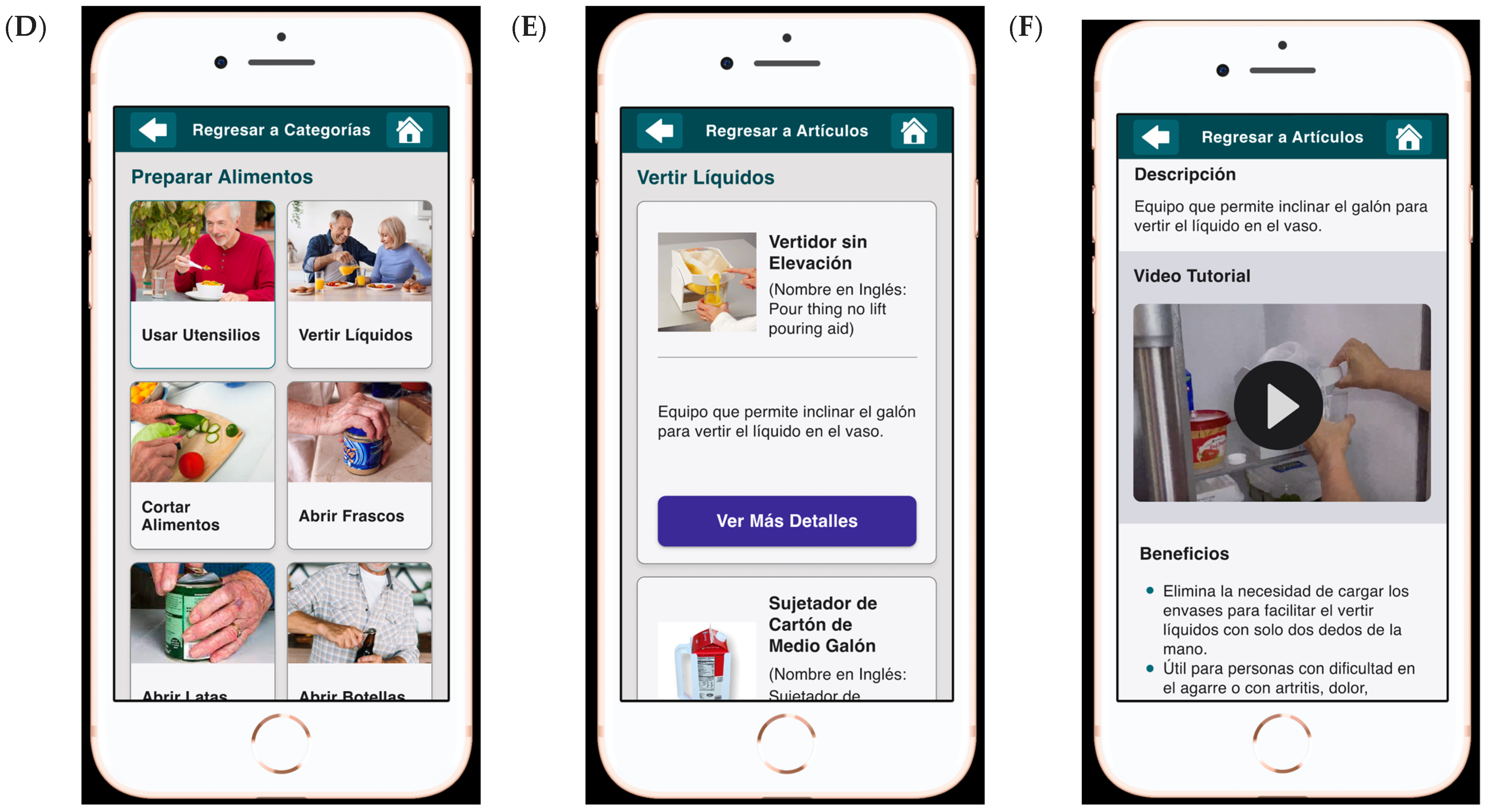
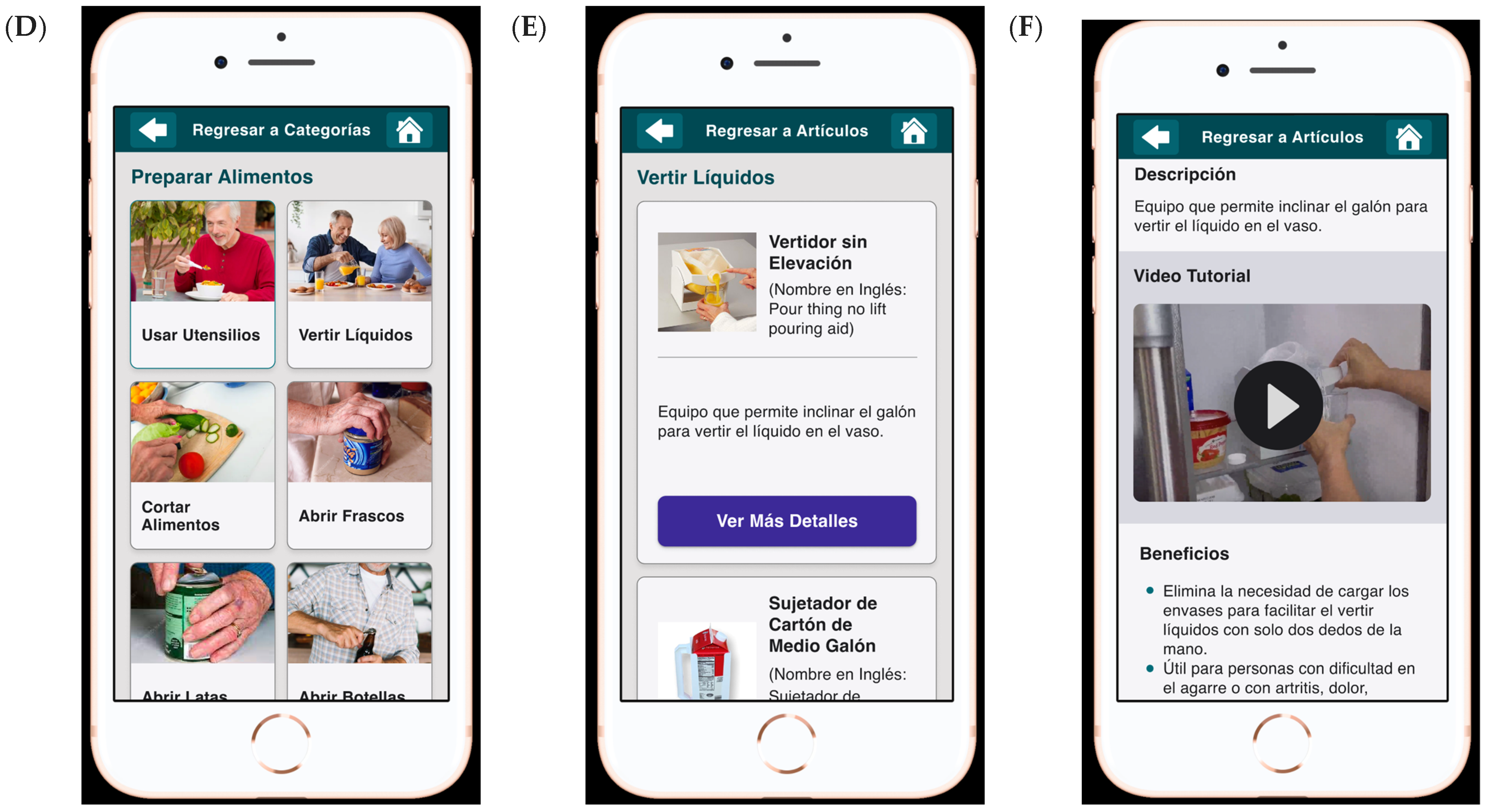
2.2. Intervention
2.3. Participants and Recruitment
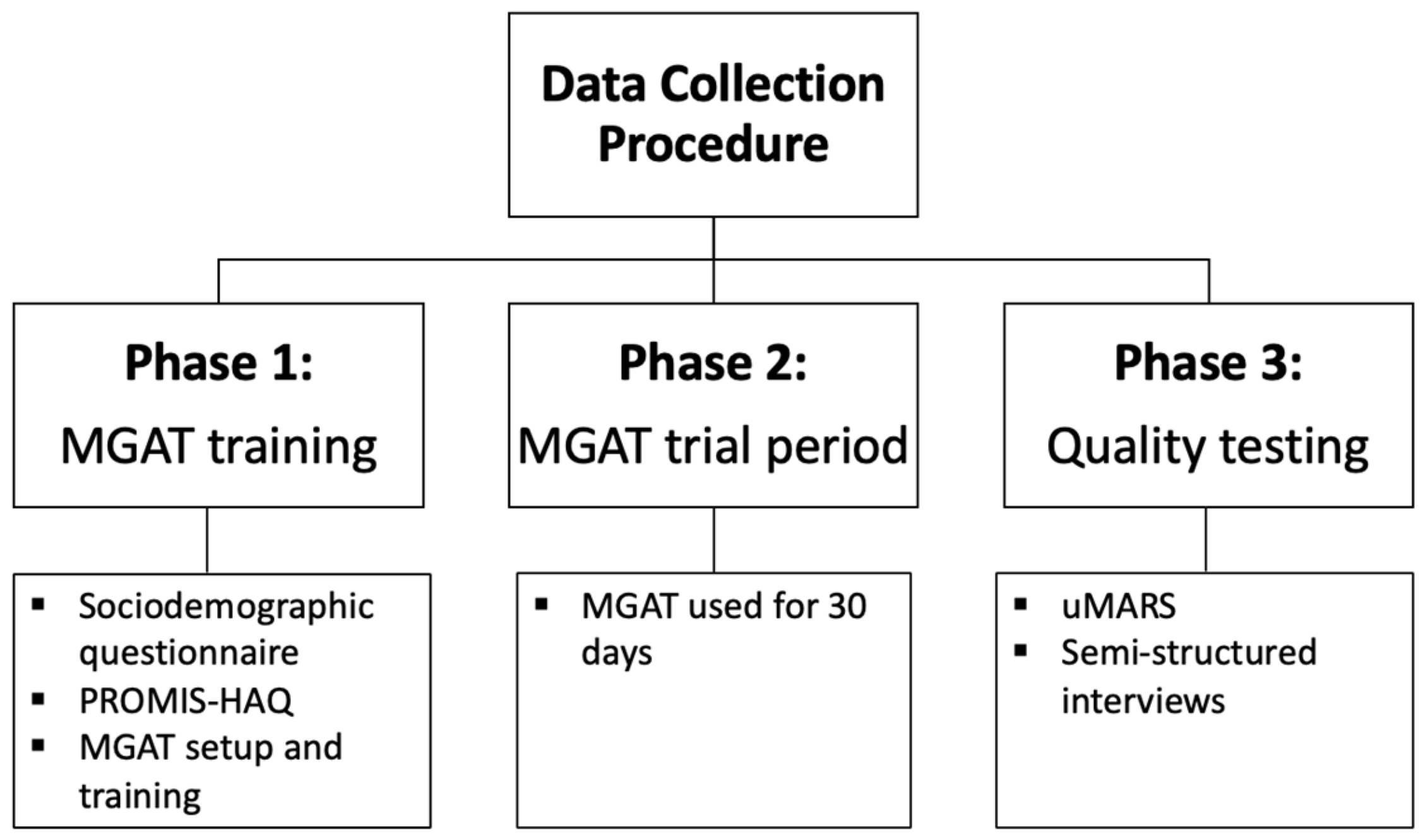
2.4. Data Collection Procedures
2.4.1. Phase 1: MGAT Training
2.4.2. Phase 2: MGAT Trial Period
2.4.3. Phase 3: Quality Testing
2.5. Study Measures
2.5.1. Sociodemographic Questionnaire
2.5.2. PROMIS Physical Function 24a (PROMIS-HAQ)
2.5.3. User Version of the Mobile Application Rating Scale (uMARS) Spanish Version
2.5.4. Semi-Structured Interview Guide
2.6. Data Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Quantitative Results
3.3. Quantitative uMARS Items Scores and Qualitative Reflections
3.3.1. Findable
3.3.2. Accessible
3.3.3. Usable
I get lost (using the MGAT), because when I try to go back, it gets all messed up, and what I do is close the screen and enter again because it confuses me. So I give it a 2 (out of 5) because the truth is, you get lost. Oh dear, I don’t understand this device much, but at least it led me to read the information.
3.3.4. Desirable
(The graphics’ quality) is acceptable, but its neither complete nor concise because I understand that in some explanations, more information was needed for one to be aware of what it is about. Because the videos weren’t clear, and they also didn’t have audio.(L2)
3.3.5. Credible
(The MGAT) tells you everything summarized and where to buy the equipment, and I like that… it offers a lot of information, but it doesn’t have links to more information and resources… You should add that. That you click on the link and it takes you to Amazon or Ebay to buy the equipment.(B1)
I would give it a 4 (out of 5). Because there are things I would like to do without equipment, like putting on underwear that I sometimes can’t reach down there… adding techniques on how to do these things, maybe they could also include it in the video tutorial.(G2)
I think the app could have more information… The equipment seems like things that one is practically tired of seeing the same. I didn’t see new equipment that I know exists, better things. I could give you an example of what struck me the most due to my back condition that prevents me from using a mop. What I saw was a mop-type vacuum cleaner but with the same movement as a mop, which is not feasible for me to use. Currently, there are robots that, in my opinion, should have been included. Modern things in terms of new equipment that exists. Update in terms of equipment.(L1)
3.3.6. Useful
3.3.7. Valuable
This app has an immeasurable worth because it teaches you many things and devices that you were unaware of, and it gives you knowledge on how to help yourself in the future. Even though you might not need some of the devices at the moment, if you are on the path to needing them, you can, according to the application, select which device will be beneficial according to your problem.(A2)
For me (the MGAT) is worth a lot. Because many people who live alone don’t have someone to remind them, ‘Hey, Dad, did you take your pills?’ ‘Look, Dad, don’t walk like that, you’re going to fall’…because you see it as scolding. In the application, you see it as someone who is giving you advice. It’s not scolding…the application speaks to us with respect…that is a splendid for moving on. And that loneliness of feeling ‘I am alone’, there (MGAT) you have a companion to help with ‘how to go to the bathroom… how to go down the stairs.(N3)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carmona-Torres, M.; Rodríguez-Borrego, M.A.; Laredo-Aguilera, J.A.; López-Soto, P.J.; Santacruz-Salas, E.; Cobo-Cuenca, A.I. Disability for basic and instrumental activities of daily living in older individuals. PLoS ONE 2019, 14, e0220157. [Google Scholar] [CrossRef] [PubMed]
- Collins, D.M.; Downer, B.; Kumar, A.; Krishnan, S.; Li, C.Y.; Markides, K.S.; Karmarkar, A.M. Impact of Multiple Chronic Conditions on Activity Limitations Among Older Mexican-American Care Recipients. Prev. Chronic Dis. 2018, 15, E51. [Google Scholar] [CrossRef]
- Erickson, W.; Lee, C.; von Schrader, S. Disability Statistics from the American Community Survey (ACS). Cornell University. 2022. Available online: www.disabilitystatistics.org (accessed on 27 October 2023).
- Muhammad, T.; Maurya, P. Social support moderates the association of functional difficulty with major depression among community-dwelling older adults: Evidence from LASI, 2017–2018. BMC Psychiatry 2022, 22, 317. [Google Scholar] [CrossRef] [PubMed]
- Tetteh, J.; Kogi, R.; Yawson, A.O.; Mensah, G.; Biritwum, R.; Yawson, A.E. Effect of self-rated health status on functioning difficulties among older adults in Ghana: Coarsened exact matching method of analysis of the World Health Organization’s study on global AGEing and adult health, Wave 2. PLoS ONE 2019, 14, e0224327. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Disability Action Plan 2014–2021. Available online: https://www.who.int/publications/i/item/who-global-disability-action-plan-2014-2021 (accessed on 3 November 2023).
- Stamm, T.; Pieber, K.; Crevenna, R.; Dorner, T. Impairment in the activities of daily living in older adults with and without osteoporosis, osteoarthritis and chronic back pain: A secondary analysis of population-based health survey data. BMC Musculoskelet. Disord. 2016, 17, 139. [Google Scholar] [CrossRef]
- Waldron, D.; Layton, N. Hard and soft assistive technologies: Defining roles for clinicians. Aust. Occup. Ther. J. 2008, 55, 61–64. [Google Scholar] [CrossRef]
- CDC. Community Health and Program Services (CHAPS): Health Disparities Among Racial/Ethnic Populations; U.S. Department of Health and Human Services: Atlanta, GA, USA, 2008.
- Ben Mortenson, W.; Demers, L.; Fuhrer, M.J.; Jutai, J.W.; Bilkey, J.; Plante, M.; DeRuyter, F. Effects of a caregiver-inclusive assistive technology intervention: A randomized controlled trial. BMC Geriatr. 2018, 18, 97. [Google Scholar] [CrossRef]
- Gottlieb, A.S.; Caro, F.G. Providing low-tech assistive equipment through home care services: The Massachusetts Assistive Equipment Demonstration. Technol. Disabil. 2000, 13, 41–53. [Google Scholar] [CrossRef]
- Stanley, R. Technology supports for community-dwelling frail older adults. Arbutus Rev. 2015, 6, 46–49. [Google Scholar] [CrossRef]
- Yusif, S.; Soar, J.; Hafeez-Baig, A. Older people, assistive technologies, and the barriers to adoption: A systematic review. Int. J. Med. Inform. 2016, 94, 112–116. [Google Scholar] [CrossRef]
- Chong, N.; Akobirshoev, I.; Caldwell, J.; Kaye, H.S.; Mitra, M. The relationship between unmet need for home and community-based services and health and community living outcomes. Disabil. Health J. 2022, 15, 101222. [Google Scholar] [CrossRef]
- Kaye, H.S.; Yeager, P.; Reed, M. Disparities in usage of assistive technology among people with disabilities. Assist. Technol. 2008, 20, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Howard, J.; Fisher, Z.; Kemp, A.H.; Lindsay, S.; Tasker, L.H.; Tree, J.J. Exploring the barriers to using assistive technology for individuals with chronic conditions: A meta-synthesis review. Disabil. Rehabil. Assist. Technol. 2022, 17, 390–408. [Google Scholar] [CrossRef]
- Orellano-Colón, E.M.; Mann, W.C.; Rivero, M.; Torres, M.; Jutai, J.; Santiago, A.; Varas, N. Hispanic Older Adult’s Perceptions of Personal, Contextual and Technology-Related Barriers for Using Assistive Technology Devices. J. Racial. Ethn. Health Disparities 2016, 3, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Orellano-Colón, E.M.; Rivero-Méndez, M.; Ralat-Fonseca, B.N.; Varas-Díaz, N.; Lizama-Troncoso, M.; Jiménez-Velázquez, I.Z.; Jutai, J.W. Multilevel barriers to using assistive technology devices among older Hispanics from poor and disadvantaged communities: The relevance of a gender analysis. Disabil. Rehabil. Assist. Technol. 2022, 19, 682–698. [Google Scholar] [CrossRef] [PubMed]
- Shahbazi, M.; Bagherian, H.; Sattari, M.; Saghaeiannejad-Isfahani, S. The opportunities and challenges of using mobile health in elderly self-care. J. Educ. Health Promot. 2021, 27, 80. [Google Scholar]
- Ha, S.K.; Lee, H.S.; Park, H.Y. Twelve smartphone applications for health management of older adults during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10235. [Google Scholar] [CrossRef] [PubMed]
- Orellano-Colón, E.M.; Ramos Marichal, A.I.; González-Crespo, V.R.; Zeballos Hernández, B.N.; Ruiz Márquez, K.N.; Roche Lima, A.; Adorno Mercado, J.; Berríos Llopart, J.G.; Cruz Ramos, A.M.; Montenegro, D.V.; et al. Design and development of Mi Guía de Asistencia Tecnológica WebAPP for older Hispanics with disabilities in daily activities [Poster Presentation]. P. R. Health Sci. J. 2023, 42 (Suppl. S1), 31. [Google Scholar]
- Knitza, J.; Tascilar, K.; Messner, E.M.; Meyer, M.; Vossen, D.; Pulla, A.; Bosch, P.; Kittler, J.; Kleyer, A.; Sewerin, P.; et al. German mobile apps in rheumatology: Review and analysis using the mobile application rating scale (MARS). JMIR Mhealth Uhealth 2019, 7, e14991. [Google Scholar] [CrossRef]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Wilson, H. Development and validation of the User Version of the Mobile Application Rating Scale (uMARS). JMIR Mhealth Uhealth 2016, 4, e72. [Google Scholar] [CrossRef]
- Villalobos, J.P.; Bull, S.S.; Portz, J.D. Usability and Acceptability of a Palliative Care Mobile Intervention for Older Adults With Heart Failure and Caregivers: Observational Study. JMIR Aging 2022, 5, e35592. [Google Scholar] [CrossRef] [PubMed]
- Argent, R.; Slevin, P.; Bevilacqua, A.; Neligan, M.; Daly, A.; Caulfield, B. Wearable Sensor-Based Exercise Biofeedback for Orthopaedic Rehabilitation: A Mixed Methods User Evaluation of a Prototype System. Sensors 2019, 19, 432. [Google Scholar] [CrossRef] [PubMed]
- Serlachius, A.; Schache, K.; Kieser, A.; Arroll, B.; Petrie, K.; Dalbeth, N. Association Between User Engagement of a Mobile Health App for Gout and Improvements in Self-Care Behaviors: Randomized Controlled Trial. JMIR Mhealth Uhealth 2019, 7, e15021. [Google Scholar] [CrossRef] [PubMed]
- Shakespeare-Finch, J.; Alichniewicz, K.K.; Strodl, E.; Brown, K.; Quinn, C.; Hides, L.; White, A.; Gossage, G.; Poerio, L.; Batras, D.; et al. Experiences of Serving and Ex-Serving Members With the PTSD Coach Australia App: Mixed Methods Study. J. Med. Internet Res. 2020, 22, e18447. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.; Plano Clark, V. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage Publications, Inc.: Singapore, 2018. [Google Scholar]
- Karaggiani, K. Optimizing the UX Honeycomb. 2018. Available online: https://uxdesign.cc/optimizing-the-ux-honeycomb-1d10cfb38097 (accessed on 20 January 2023).
- Morville, P. User Experience Design. Semantic Studios. 2004. Available online: https://semanticstudios.com/user_experience_design/ (accessed on 29 January 2023).
- Hwang, W.; Salvendy, G. Number of people required for usability evaluation: The 10 ± 2 rule. Commun. ACM 2010, 53, 130–133. [Google Scholar] [CrossRef]
- Fries, J.; Cella, D.; Rose, M.; Krishnan, E.; Bruce, B. Progress in assessing physical function in arthritis: PROMIS short forms and computerized adaptive testing. J. Rheumatol. 2009, 36, 2061–2066. [Google Scholar] [CrossRef] [PubMed]
- Bruce, B.; Fries, J. The health assessment questionnaire (HAQ). Clin. Exp. Rheumatol. 2005, 23, S14. [Google Scholar] [PubMed]
- Martin-Payo, R.; Carrasco-Santos, S.; Cuesta, M.; Stoyan, S.; Gonzalez-Mendez, X.; Fernandez-Alvarez, M.D.M. Spanish adaptation and validation of the User Version of the Mobile Application Rating Scale (uMARS). J. Am. Med. Inform. Assoc. 2021, 28, 2681–2686. [Google Scholar] [CrossRef]
- Kibiswa, N. Directed Qualitative Content Analysis (DQlCA): A Tool for Conflict Analysis. Qual. Rep. 2019, 24, 2059–2079. [Google Scholar] [CrossRef]
- Provalis Research. Year. Qualitative Data Analysis (QDA) Miner Lite (Version 3.0) [Computer Software]. 2023. Available online: https://provalisresearch.com/products/qualitative-data-analysis-software/freeware/ (accessed on 5 May 2023).
- Morse, J. Critical Analysis of Strategies for Determining Rigor in Qualitative Inquiry. Qual. Health Res. 2015, 25, 1212–1222. [Google Scholar] [CrossRef]
- Fetters, M.; Curry, L.A.; Creswell, J.W. Achieving integration in mixed methods designs-principles and practices. Health Serv. Res. 2013, 48, 2134–2156. [Google Scholar] [CrossRef]
- Scullin, M.K.; Jones, W.E.; Phenis, R.; Beevers, S.; Rosen, S.; Dinh, K.; Kiselica, A.; Keefe, F.J.; Benge, J.F. Using smartphone technology to improve prospective memory functioning: A randomized controlled trial. J. Am. Geriatr. Soc. 2022, 70, 459–469. [Google Scholar] [CrossRef]
- Øksnebjerg, L.; Woods, B.; Vilsen, C.R.; Ruth, K.; Gustafsson, M.; Ringkøbing, S.P.; Waldemar, G. Self-management and cognitive rehabilitation in early stage dementia—Merging methods to promote coping and adoption of assistive technology. A pilot study. Aging Ment. Health 2020, 24, 1894–1903. [Google Scholar] [CrossRef]
- Sureshkumar, K.; Murthy, G.V.; Natarajan, S.; Naveen, C.; Goenka, S.; Kuper, H. Evaluation of the feasibility and acceptability of the ‘Care for Stroke’ intervention in India, a smartphone-enabled, carer-supported, educational intervention for management of disability following stroke. BMJ Open 2016, 6, e009243. [Google Scholar] [CrossRef]
- Groussard, P.Y.; Pigot, H.; Giroux, S. From conception to evaluation of mobile services for people with head injury: A participatory design perspective. Neuropsychol. Rehabil. 2018, 28, 667–688. [Google Scholar] [CrossRef]
- Cross, T.; Bazron, B.; Dennis, K.; Isaacs, M.R. Towards a Culturally Competent System of Care; Georgetown University Child Development Center, CASSP Technical Assistance Center: Washington, DC, USA, 1989; Volume 1. [Google Scholar]
- López, L.; Tan-McGrory, A.; Horner, G.; Betancourt, J.R. Eliminating disparities among Latinos with type 2 diabetes: Effective eHealth strategies. J. Diabetes Complicat. 2016, 30, 554–560. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Active Aging: A Policy Framework. 2002. Available online: https://iris.who.int/handle/10665/67215 (accessed on 23 May 2009).
- Pryor, M.; McLaughlin, A.C. Developing Video or Multimedia Instructions for Older Adults. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2018, 62, 1739–1743. [Google Scholar] [CrossRef]
- Irrazabal, N.; Saux, G.; Burin, D. Procedural multimedia presentations: The effects of working memory and task complexity on instruction time and assembly accuracy. Appl. Cogn. Psychol. 2016, 30, 1052–1060. [Google Scholar] [CrossRef]
- Anderson, K.; Burford, O.; Emmerton, L. Mobile Health Apps to Facilitate Self-Care: A Qualitative Study of User Experiences. PLoS ONE 2016, 11, e0156164. [Google Scholar] [CrossRef]
- Zapata, B.C.; Fernández-Alemán, J.L.; Idri, A.; Toval, A. Empirical Studies on Usability of mHealth Apps: A Systematic Literature Review. J. Med. Syst. 2015, 39, 1. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categories | Facets | Descriptions and Definitions |
|---|---|---|
| Use | Findable | Navigable and easy to find information. |
| Accessible | Manageable for people with disabilities or reduced function. | |
| Usable | Ability to be used. | |
| Feel | Desirable | Features with an emotional engagement. |
| Credible | Influence of elements for users’ trust and belief in the product. | |
| Think | Useful | To make innovative solutions that are beneficial. |
| Valuable | Deliver value or advance the mission. |
| Participant’s Number | PROMIS HAQ (T-Score; Severity) a | Sex | Age | Health Conditions | Living Situation | Highest Level of Education | Annual Income |
|---|---|---|---|---|---|---|---|
| A2 | 37.6; moderate | M | 86 | Diabetes Hypertension Heart disease | Married | High school graduate | USD 1700 |
| A3 | 58.1; above average | F | 70 | Hypertension Visual | Divorced; separated | Bachelor’s degree | USD 1800 |
| B1 | 58.1; above average | M | 73 | Diabetes Hypertension | Widowed | Bachelor’s degree | USD 3000 |
| B2 | 58.1; above average | M | 74 | Other | Married | Bachelor’s degree | USD 6000 |
| B3 | 43.4; mild | F | 65 | Obesity Hypertension Gastrointestinal disease Respiratory disease Arthritis | Divorced; separated | High school graduate | USD 600 |
| G1 | 46.7; above average | M | 77 | Diabetes Hypertension Obesity Heart disease Gastrointestinal disease Arthritis Depression Other | Married | High school graduate | USD 2012 |
| G2 | 48.4; above average | F | 73 | Diabetes Hypertension Obesity Gastrointestinal disease Other | Married | More than high school | USD 860 |
| L1 | 43.4; mild | F | 66 | Other | Married | Bachelor’s degree | USD 2200 |
| L2 | 58.1; Above average | F | 77 | Osteoporosis Arthritis Other | Divorced; separated | High school graduate | USD 1000 |
| N1 | 58.1; above average | F | 75 | Hypertension Other | Married | More than high school | USD 2000 |
| N2 | 43.4; mild | F | 71 | Hypertension Auditory | Widowed | More than high school | USD 1887 |
| N3 | 58.1; above average | M | 81 | Diabetes Hypertension Gastrointestinal disease Arthritis | Divorced; separated | Bachelor’s degree | USD 1500 |
| uMARS Sections | uMARS Dimensions | Mean (SD) | Range a |
|---|---|---|---|
| Objective | Engagement | 2.97 (1.66) | 1–5 |
| Functionality | 4.40 (0.89) | 3–5 | |
| Aesthetics | 4.28 (1.61) | 3–5 | |
| Information | 4.31 (0.72) | 3–5 | |
| Overall mean | 3.99 (0.68) | 1–5 | |
| Subjective | Subjective quality | 3.56 (1.40) | 1–5 |
| Perceived impact | 4.70 (0.81) | 3–5 | |
| Overall mean | 4.13 (1.10) | 1–5 |
| Themes | Sub-Themes |
|---|---|
| Use | |
| Findable |
|
| Accessible |
|
| Usable |
|
| Feel | |
| Desirable |
|
| Credible |
|
| Think | |
| Useful |
|
| Valuable |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orellano-Colon, E.M.; Fernández-Torres, A.; Figueroa-Alvira, N.; Ortiz-Vélez, B.; Rivera-Rivera, N.L.; Torres-Ferrer, G.A.; Martín-Payo, R. Empowering Potential of the My Assistive Technology Guide: Exploring Experiences and User Perspectives. Disabilities 2024, 4, 303-320. https://doi.org/10.3390/disabilities4020020
Orellano-Colon EM, Fernández-Torres A, Figueroa-Alvira N, Ortiz-Vélez B, Rivera-Rivera NL, Torres-Ferrer GA, Martín-Payo R. Empowering Potential of the My Assistive Technology Guide: Exploring Experiences and User Perspectives. Disabilities. 2024; 4(2):303-320. https://doi.org/10.3390/disabilities4020020
Chicago/Turabian StyleOrellano-Colon, Elsa M., Angelis Fernández-Torres, Nixmarie Figueroa-Alvira, Bernice Ortiz-Vélez, Nina L. Rivera-Rivera, Gabriela A. Torres-Ferrer, and Rubén Martín-Payo. 2024. "Empowering Potential of the My Assistive Technology Guide: Exploring Experiences and User Perspectives" Disabilities 4, no. 2: 303-320. https://doi.org/10.3390/disabilities4020020
APA StyleOrellano-Colon, E. M., Fernández-Torres, A., Figueroa-Alvira, N., Ortiz-Vélez, B., Rivera-Rivera, N. L., Torres-Ferrer, G. A., & Martín-Payo, R. (2024). Empowering Potential of the My Assistive Technology Guide: Exploring Experiences and User Perspectives. Disabilities, 4(2), 303-320. https://doi.org/10.3390/disabilities4020020