
Effectiveness of an Assistive Instrument for Physical Therapists with Visual Impairment to Conduct the Muscle Tightness Test


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Method of Muscle Tightness Test
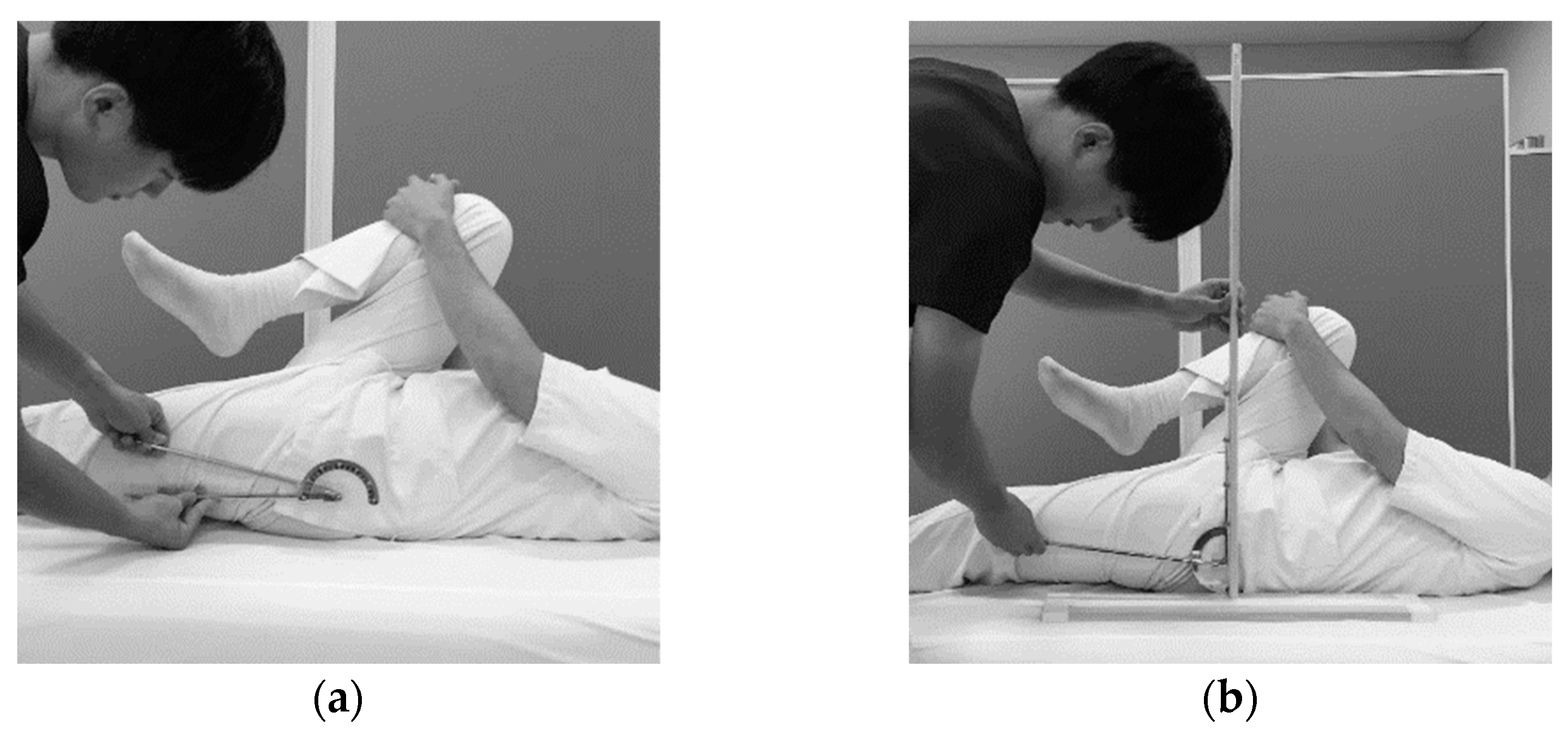
2.3.1. Hamstrings
2.3.2. Iliopsoas
2.3.3. Gastrocnemius
2.3.4. Quadriceps
2.4. Examining the Effectiveness of the Assistive Instrument
2.4.1. Ease
2.4.2. Accuracy
2.4.3. Measurement Time
2.5. Statistical Analysis
3. Results
3.1. Ease
3.2. Accuracy
3.3. Measurement Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blauwet, C.; Willick, S.E. The Paralympic Movement: Using sports to promote health, disability rights, and social inte-gration for athletes with disabilities. PM R J. Inj. Funct. Rehabil. 2012, 4, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Shimony, N.D.; Lidor, R.; Ziv, G. The effectiveness of bandwidth knowledge of results on a throwing task in goalball players with visual impairments. Eur. J. Adapt. Phys. Act. 2020, 13. [Google Scholar] [CrossRef]
- Dickson, T.J.; Darcy, S.; Johns, R.; Pentifallo, C. Inclusive by design: Transformative services and sport-event accessibility. Serv. Ind. J. 2016, 36, 532–555. [Google Scholar] [CrossRef]
- Duncan, K.M.; Wright, K.E. A National Survey of Athletic Trainer Roles and Responsibilities in the Allied Clinical Setting. J. Athl. Train. 1992, 27, 311–316. [Google Scholar]
- Japan Sport Association. The 1st Professional Survey of Trainers in Japan. 2018. Available online: https://www.japan-sports.or.jp/Portals/0/data/ikusei/doc/AT/Report/Japan_trainer_report.pdf (accessed on 17 January 2020).
- Wong, M.E. Higher education or vocational training inriryoka? Post-school choices of visually-impaired students. Part 2, Japan. Br. J. Vis. Impair. 2004, 22, 59–65. [Google Scholar] [CrossRef]
- Kondo, H.; Fujii, R. A survey of visually impaired anma-massage-shiatsu practitioners in Japanese hospitals. NTUT Educ. Disabil. 2014, 12, 24–27. [Google Scholar]
- Hansberger, B.L.; Loutsch, R.; Hancock, C.; Bonser, R.; Zeigel, A.; Baker, R.T. Evaluating the relationship between clinical assess-ments of apparent hamstring tightness: A correlational analysis. Int. J. Sports Phys. Ther. 2019, 14, 253–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahr, R.; Holme, I. Risk factors for sports injuries—a methodological approach. Br. J. Sports Med. 2003, 37, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Reis, F.J.J.; Macedo, A. Influence of Hamstring Tightness in Pelvic, Lumbar and Trunk Range of Motion in Low Back Pain and Asymptomatic Volunteers during Forward Bending. Asian Spine J. 2015, 9, 535–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Endo, Y.; Sakamoto, M. Correlation of shoulder and elbow injuries with muscle tightness, core stability, and balance by longitu-dinal measurements in junior high school baseball players. J. Phys. Ther. Sci. 2014, 26, 689–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huguenin, L.; Brukner, P.D.; McCrory, P.; Smith, P.; Wajswelner, H.; Bennell, K. Effect of dry needling of gluteal muscles on straight leg raise: A randomised, placebo controlled, double blind trial. Br. J. Sports Med. 2005, 39, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Zink, K.; Chini, B.; Cowens, J.; Kremer, L.; Lin, L. Improving Clinical Outcomes and Quality of Life with Massage Therapy in Youth and Young Adults with Cystic Fibrosis: A Pilot Study. Int. J. Ther. Massage Bodywork Res. Educ. Pract. 2019, 12, 4–15. [Google Scholar]
- Tamai, S.; Kuroda, S.; Numoto, N.; Yabe, T.; Wada, T. Examination of problems when the visually impaired measure the range of motion. Bull. Acupunct. Phys. Ther. Teach. Train. School Univ. Tsukuba 2019, 4, 5–12. [Google Scholar]
- Klavina, A.; Jekabsone, I. Static Balance of Persons with Intellectual Disabilities, Visual Impairment and without Disabilities. Eur. J. Adapt. Phys. Act. 2014, 7, 50–57. [Google Scholar] [CrossRef] [Green Version]
- Behnoush, B.; Tavakoli, N.; Bazmi, E.; Fard, F.N.; Shahi, M.H.P.; Okazi, A.; Mokhtari, T. Smartphone and Universal Goniometer for Measurement of Elbow Joint Motions: A Comparative Study. Asian J. Sports Med. 2016, 7, e30668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abe, H.; Watanabe, H.; Tojima, M.; Torii, S.; Shigeta, K.; Tsukimura, T.; Abe, H. Intrarater and interrater reliability of the muscle tightness test. J. Jpn. Soc. Clin. Sports Med. 2012, 20, 336–343. [Google Scholar]
- Lieberman, L.J.; Lepore, M.; Lepore-Stevens, M.; Ball, L. Physical Education for Children with Visual Impairment or Blindness. J. Phys. Educ. Recreat. Dance 2018, 90, 30–38. [Google Scholar] [CrossRef]
- Kimura, K.; Miyaji, H.; Hanaoka, Y.; Kadota, T.; Sato, T.; Wada, T.; Miyamoto, T. Examination of problems when the visually impaired conduct low frequency electroacupuncture. Bull. Acupunct. Phys. Ther. Teach. Train. School Univ. Tsukuba 2018, 3, 5–13. [Google Scholar]
- The Nippon Foundation Volunteer Support Center. Volunteer Participation Practice Report Meeting for the Visually Impaired Tokyo Olympic and Paralympic Games and beyond Has Been Held! 2021. Available online: https://www.volasapo.tokyo/column/report/3988/ (accessed on 5 October 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean (SD)/Number (%) |
|---|---|
| Sex (men:women) | 18:4 |
| Age (year) | 31.1 (7.5) |
| Age of diagnosis of VI (year) | 17.5 (10.5) |
| Duration of VI (year) | 13.9 (7.4) |
| Visual acuity | 0.24 (0.27) |
| Visual field constriction | 19 (86.3%) |
| Central scotoma | 5 (22.7%) |
| Duration of license of physical therapists (year) | 1.4 (1.4) |
| Items | UG | AsI | p-Value |
|---|---|---|---|
| (1) Operability of the goniometer | 3.0 (1.0) | 3.9 (0.8) | 0.001 |
| (2) Accurate placement of the angle meter with the basic axis | 2.8 (0.8) | 4.3 (0.6) | <0.001 |
| (3) Accurate placement of the angle meter with the moving axis | 2.7 (1.0) | 3.7 (0.8) | 0.001 |
| (4) Verification of the measurement position | 3.3 (1.0) | 3.6 (0.7) | 0.109 |
| (5) Maintenance of the measurement position | 2.9 (1.1) | 3.3 (1.0) | 0.058 |
| (6) Measurement of the joint angle as the position is maintained | 2.3 (1.1) | 3.8 (0.8) | <0.001 |
| (7) Readability of the scales of the angle meter | 2.5 (1.1) | 2.9 (1.1) | 0.046 |
| (8) Verification of muscle tightness | 3.3 (0.9) | 3.6 (0.6) | 0.083 |
| (9) Verification of trick motion | 2.7 (0.6) | 3.2 (0.6) | 0.013 |
| (10) Accurate verification of the basic (vertical) axis | 2.5 (1.0) | 4.1 (0.8) | <0.001 |
| (11) Comprehensive ease of the MTT | 2.8 (1.0) | 3.9 (0.8) | <0.001 |
| (12) Confidence in performing the MTT accurately | 2.1 (1.0) | 3.1 (0.8) | 0.001 |
| Items | UG | AsI |
|---|---|---|
| (a) Practice | 21 | 22 |
| (b) Gather advice | 19 | 17 |
| (c) Develop or improve the instrument | 7 | 6 |
| (d) No need for improvement | 0 | 0 |
| (e) Others * | 1 | 1 |
| Measurement Parts | UG | AsI | No Difference |
|---|---|---|---|
| (I) Hamstrings | 1 | 20 | 1 |
| (II) Iliopsoas | 7 | 7 | 8 |
| (III) Gastrocnemius | 4 | 14 | 4 |
| (IV) Quadriceps | 1 | 20 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamai, S.; Kuroda, S.; Yabe, T.; Wada, T. Effectiveness of an Assistive Instrument for Physical Therapists with Visual Impairment to Conduct the Muscle Tightness Test. Disabilities 2021, 1, 471-480. https://doi.org/10.3390/disabilities1040033
Tamai S, Kuroda S, Yabe T, Wada T. Effectiveness of an Assistive Instrument for Physical Therapists with Visual Impairment to Conduct the Muscle Tightness Test. Disabilities. 2021; 1(4):471-480. https://doi.org/10.3390/disabilities1040033
Chicago/Turabian StyleTamai, Shinsuke, Shusei Kuroda, Takayuki Yabe, and Tsunehiko Wada. 2021. "Effectiveness of an Assistive Instrument for Physical Therapists with Visual Impairment to Conduct the Muscle Tightness Test" Disabilities 1, no. 4: 471-480. https://doi.org/10.3390/disabilities1040033
APA StyleTamai, S., Kuroda, S., Yabe, T., & Wada, T. (2021). Effectiveness of an Assistive Instrument for Physical Therapists with Visual Impairment to Conduct the Muscle Tightness Test. Disabilities, 1(4), 471-480. https://doi.org/10.3390/disabilities1040033