Abstract
There has been increasing attention to quality of life for families supporting children with disabilities internationally; however, there is minimal research on family quality of life (FQOL) in low-income countries, and specifically in African contexts. This study explored how Ethiopian families of children with disabilities conceptualised FQOL and what they perceived their support needs related to FQOL were. Using a qualitative exploratory descriptive design, we interviewed Ethiopian family members of children with various disabilities. Audio-recorded interviews were transcribed verbatim and translated into English with professional translation assistance. We analysed translated transcripts inductively based on Braun and Clarke’s approach to thematic analysis. We found that spirituality was core to families and that they described FQOL in terms of their relationships within the immediate family and with the community. Additionally, families wanted to be self-sufficient and provide for themselves, but with the additional challenges of raising a child with a disability and pervasive poverty, they recognised their need for more support. Therefore, providing holistic, family-centred services to Ethiopian families of children with disabilities can contribute to enhancing FQOL.
1. Introduction
Families provide important social structures in societies across the world, and they are particularly crucial for supporting positive outcomes for children with disabilities [1,2]. Interest in family quality of life (FQOL) as an outcome for families of children with disabilities has increased since its more formal conception in 2000 at the World Congress of the International Association for the Scientific Study of Intellectual and Developmental Disability (IASSIDD) [1,3]. Emerging from the field of individual quality of life (QOL) [4,5], FQOL recognises the interconnection between family members and how individual needs and wellbeing affect the wellbeing of the whole family. Zuna and colleagues [6] developed a theory and model of FQOL, which was subsequently updated by Chiu and colleagues [7], to demonstrate the dynamic interplay between individual family members and the family unit within the context of programs, systems, policies, and societal values. Zuna et al. [6] define FQOL as “a dynamic sense of well-being of the family, collectively and subjectively defined and informed by its members, in which individual and family-level needs interact” (p. 262).
Research related to FQOL has predominantly focused on the perspectives of parents/caregivers, typically mothers, of children with disabilities, providing a preliminary understanding of factors that can either facilitate or impede FQOL [4,8]. Additionally, FQOL research originated in the field of Intellectual and Developmental Disability (IDD) [3,5,9] and whilst researchers are beginning to investigate FQOL with other disabilities [10,11], further exploration is needed with families of children with various and multiple disabilities and from the perspectives of various family members.
Although research related to FQOL is expanding from its origin in high-income, English-speaking countries to explore international perspectives [12,13,14,15,16], there is still limited research in low-and-middle-income countries (LMICs). The majority of children with disabilities live in LMICs [17,18], therefore it is important to understand perspectives in these contexts and to explore opportunities for supporting families to enhance FQOL. As culture and context significantly influence FQOL [4,19], it is also important that families of diverse backgrounds are engaged to develop a broader global understanding of FQOL and to direct the development of culturally relevant support services. We recently conducted a scoping review to explore the factors that contribute to FQOL for families of children with disabilities in African contexts [20]. We found that many factors align with the global FQOL literature, including family relationships, family income, and severity of disability; however, poverty, stigma, and spirituality were particularly significant and strongly affected FQOL in African countries.
As one of the mediating factors contributing to FQOL, it is important to consider the role of support for families of children with disabilities. Kyzar and colleagues [21] categorise support as emotional (improving psychosocial functioning), physical (related to health and daily living skills), material/instrumental (related to finances and helping families complete needed activities), and informational (improving knowledge). In a literature review of families of children with severe/multiple disabilities, they found that “family support provided an enhancing effect to family quality of life, family functioning, and family satisfaction and a buffering effect on family stress.” [21] (p. 41). In a more recent review of the relationship between family support and family outcomes among families of children with disabilities in LMICs, Nuri and colleagues [22] found that families received most support from informal sources—family, friends, peers—and support was connected to reduced parental stress and care-burden, improved parental knowledge and skills, and enhanced life satisfaction. In our scoping review, we also found that various types of support positively affected families in African contexts, but there was an overwhelming need for more support [20]. The connection between FQOL and the nature and level of support, particularly in LMICs, requires further research.
This study was conducted in Ethiopia, an East African country located in the Horn of Africa. It is the second-most populated country in Africa, after Nigeria, with an estimated 110–115 million people. Although reliable statistics on disability are difficult to ascertain, in 2011, the World Health Organisation (WHO) estimated that approximately 17.6% of Ethiopia’s total population had a disability [17]. Other studies have indicated that nearly half of those with disabilities in Ethiopia are children [23,24]. Minimal research has examined the subjective experiences and needs of children with disabilities and their families in Ethiopia [25,26,27,28]. The purpose of this study was to explore how Ethiopian families of children with disabilities in Gondar conceptualise FQOL and how support, or lack thereof, contributes to their FQOL. Understanding FQOL and families’ support needs in an Ethiopian context can help to direct appropriate support services for families of children with disabilities that are culturally relevant and family centred, as well as feasible within an Ethiopian context.
2. Materials and Methods
2.1. Study Design
We used a qualitative exploratory descriptive design to understand how Ethiopian families of children with disabilities in Gondar conceptualise FQOL and what they perceive are their support needs. An exploratory descriptive design allows flexibility to explore and describe participants’ experiences of a phenomenon where there has been limited previous research [29].
2.2. Participants
Ethiopia has signed the United Nations Convention on the Rights of Persons with Disabilities and has technically adopted their definition of disability [30,31] as stated in Article 1: “those who have long-term physical, mental, intellectual or sensory impairments which in interaction with various barriers may hinder their full and effective participation in society on an equal basis with others” [32]. However, like in other African contexts, children rarely have a formal diagnosis of disability in Ethiopia. In addition, similar to other African countries (e.g., Congo, Tanzania, South Africa), Ethiopian families often constitute a broader definition of family, more than simply blood relations [33,34,35]. Therefore, participants in this study included family members over the age of 18, based on the definition of family by Zuna and colleagues as the “collective number of individuals who consider themselves to be part of a family and who engage in some form of family activities together on a regular basis” (p. 263) [6]. Participants identified as having a child with a disability (age 0–18 [24]) regardless of diagnosis.
2.3. Data Collection
Participants were recruited with the assistance of the University of Gondar (UoG) Community-based rehabilitation (CBR) program who are familiar with local families of children with disabilities. We purposefully sampled to ensure a diverse representation of family members, types of disability, and levels of support. Aiming for approximately 20 family members, we used information power—considering the study aim, sample specificity, established theory, quality of dialogue, and analysis strategy—to determine sufficient data, as exploratory studies do not aim for a complete description of all aspects of the phenomenon (as targeted in theoretical data saturation), but rather seek abundant and varied accounts of a new phenomenon [36]. Once potential family members were identified, a CBR supervisor explained the study and if they provided verbal consent, a meeting was organised with a local research assistant (RA) who conducted all of the interviews in Amharic to ensure that participants were comfortable in their own language. The interviewer confirmed verbal consent again with each participant before starting the interview. Following recommendations from Ethiopian colleagues, interviews were conducted at the CBR centre, as it was a familiar central location. Participants received remuneration for transport/refreshment costs in line with local recommendations [37,38,39]. Following the interviews, a local faculty member of the UoG transcribed the audio recordings of interviews verbatim in Amharic. A skilled local translator then translated the interview transcript into English.
2.4. Data Analysis
Following translation, we used Braun and Clarke’s [40] approach to reflexive qualita-tive thematic analysis, first familiarising ourselves with the data before generating initial codes, searching for themes, reviewing and defining themes, and finally writing up the report. To improve rigour, 2 authors independently coded several transcripts, and all authors were involved in discussing the findings and potential themes. We also considered potential meanings of translations with Ethiopian colleagues [41,42,43,44,45].
2.5. Ethical Considerations
Cross-cultural research, as in the case of this study, introduces additional ethical dimensions that require sensitive consideration and reflexivity [43,46]. Firstly, we obtained ethical approval from Queen’s University, Canada (# 6028643), and the University of Gondar, Ethiopia. We were guided by Im et al.’s [47] criteria for cross-cultural rigour: Cultural relevance, contextuality, appropriateness, mutual respect, and flexibility. Our research purpose is relevant to the local community and seeks to practically contribute to improving FQOL. All of the authors have prior cross-cultural experience, and the first author had ongoing, extensive consultation with Ethiopian colleagues to ensure the research process was respectful and appropriate. Recognising inherent power imbalances between the researchers and participants, particularly with the majority of participants being women, we sought to minimise these differences as much as possible [48,49]. Specifically, none of the foreign researchers had direct contact with participants, whereby participants were identified via their local CBR worker (who has a longstanding relationship with families, completely separate from the study) and a local RA conducted all interviews. Voluntary consent was explained clearly to participants, and verbal consent was obtained to mitigate potential issues with literacy [50]. Non-English participants are sometimes overlooked in English-dominant academic work [51,52], therefore we ensured all interviews were in participants’ local language to allow them to express themselves fully. We endeavoured to model humility, respect, and flexibility throughout the research process.
3. Results
We interviewed 20 family members from 20 different families of children with disabilities in Gondar, Ethiopia. Our participants represented families of children with a range of disabilities between the ages of 2 and 17. Family members were predominantly mothers, but also included three fathers, three grandmothers, two aunts, and one sister. Whilst almost half had irregular income and could not provide an average monthly income, seven reported a monthly income of under 1500 Birr (approximately USD34). More detailed demographic information is evident in Table 1 whilst Table 2 provides contextual information for participant quotes.

Table 1.
Demographic characteristics of study participants.
Table 2.
Contextual information for participant quotes.
We drew out five major themes from interviews with family members: Spirituality, relationships (divided into subthemes: Relationships within immediate family and relationships with the community), self-sufficiency, parenting responsibilities, and the role of support. Figure 1 shows a visual representation of themes where spirituality is the central core with dotted lines depicting the inter-connections between spirituality, relationships, and self-sufficiency. Parenting responsibilities and support are on opposite ends of the spectrum as they represent competing constructs that must be balanced and work in tandem in order to achieve FQOL. They are also connected to and are affected by spirituality, relationships, and self-sufficiency. Table 3 delineates the overall themes with representative participant quotes.
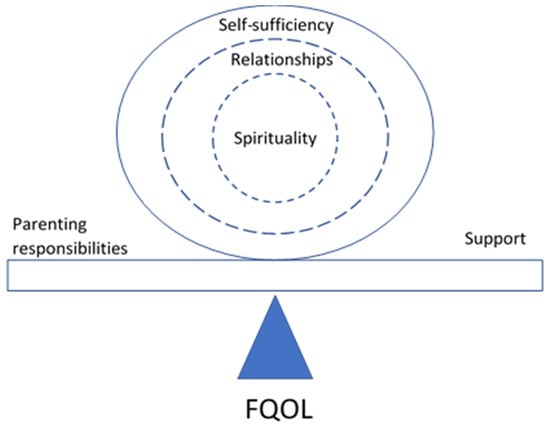
Figure 1.
Visual representation of themes related to family quality of life (FQOL).
Table 3.
Overall themes and representative quotes from participants.
3.1. “All I Have Is God”—The Foundational Role of Spirituality
Families of children with disabilities demonstrated how core their spiritual beliefs and values are to the way they live with disability and face their daily struggles. Participants adhered to traditional religious institutions, mostly some form of Orthodox Christianity, but several were Muslim. Spirituality influenced families’ behaviour (e.g., taking their child to holy water in the hope of a blessing or cure) as well as their beliefs, values, and hope for the future. For example, several participants accepted that it was God’s will that they were given a child with a disability and although they were initially disappointed and continued to struggle, they saw their child as a blessing and gift from God: “I always accept what God has given me. Whatever He has in store for me I just accept it and live with it.” (P11). In the face of discrimination and inadequate support, the participants turned to God as their source of comfort and support.
Their belief in God and acceptance of their ‘lot’ encouraged participants to persevere and have hope despite the challenges they faced raising children with disabilities: “Out of all the things, religion is important whether you have everything or not. You will benefit a lot when you become closer to God. He [God] always does what is good for us. Even if we have to face bad things, we should always be thankful for it. You will face many challenges in life but if you are able to pass them in patience, I think you can be successful” (P20). Perseverance was expressed in terms of working hard to change and improve the family’s life and enduring challenges without losing hope. Closely linked with perseverance, and again underscored by families’ spiritual beliefs, several participants described their commitment to raise their child with a disability and their willingness to sacrifice and accept their responsibility despite others telling them they should ‘give up’ their child. Participants described how they could set an example for others by demonstrating care for their child with disabilities, and by working hard and diligently to improve and change their lives for the better.
Although spirituality was crucial for families to cope with raising a child with disability, it also seemed connected to a more general morality, shaping family values, goals, and behaviours, regardless of the presence of disability. Participants described the need for families to model spiritual faith to children so that they grow up to be moral and responsible. One mother described how her husband was unsupportive because he did not take spiritual beliefs seriously: “We are Muslims and, in our religion, praying five times and reading the Qur’an is mandatory but he doesn’t do these things. I think this is why he couldn’t be good to his family. Because a religious person would fear his creator, and a person who fears his creator will be good to other people.” (P12).
Linked to morality, several participants spoke about wanting to ‘give back’ and help others less fortunate, despite struggling to make ends meet themselves. This was evident by a family member, other than parents, taking in the child with a disability (e.g., sister or aunt) because they felt that they were better able to care for the child and help in this way. Some recognised that they were not in a position to give much materially, but they still wanted to encourage and help others who had been through similar hardships. One woman described how she could never be truly happy when she knows that others suffer: “Even though I eat to the full, I would think of my poor relatives in the countryside. And if I see someone struggling, I would feel their pain. I don’t get satisfied with what I am giving and that creates a discomfort for me” (P5).
Going to church or other religious gatherings as a family and celebrating with others on holy days was also frequently described as important and a source of happiness even when life was an ongoing struggle. Other people were sometimes more generous in giving money, food, or clothes during these celebrations and these times offered families a break from work/routine and a chance to eat special food and enjoy time together. However, one grandmother described how poverty robbed this joy: “I am always heartbroken especially during holy days for I couldn’t be able to meet our needs. I spend most of my time in pain.” (P17). Attending church, praying, and taking the child to holy water (even if it was very physically demanding to carry their children and travel long distances) were all important activities for families and some lamented that they could not be more involved in spiritual practices because of the restriction of caring for their child. Engaging in spiritual activities was an important source of emotional support for families: “When I am bothered, I go to church. You meet the priests and other brothers who advise you and you would learn a lot from. That gives you a great relief. First of all, I get blessed when I go to church. And second, I get back home cheered up.” (P14). This same mother described how following religious traditions (i.e., at her wedding) also brought happiness.
3.2. Relationships
Relationships within the nuclear family and with others in the community were fundamental to FQOL for families of children with disabilities. However, these relationships could either facilitate or hinder FQOL.
3.2.1. “When They Are Happy, I Am Happy”—Relationships within the Immediate Family
Family members described their own happiness in terms of the happiness of other family members, and often the child with a disability. These close, mutually dependent ‘symbiotic’ relationships demonstrated the intense central core of the nuclear family in both positive and negative ways. Mothers particularly described how they were happy when their children were happy. Conversely, caregivers suffered when their children suffered. This symbiotic relationship was also evident between spouses, where one woman described how her wellbeing and happiness depended on whether her husband was satisfied. Several other participants described having unsupportive husbands either passively (i.e., their husbands had died, were ill and unable to work, or absent because of long work hours) or actively (i.e., husbands abandoning the family, rejecting the child with a disability, conflict, divorce, or blaming the mother): “After I gave birth, he doesn’t give his fatherly love to the new-born. He thinks the child will be disabled like his big brother. He would say to him ‘Be careful, she will make you like your brother; she will not handle you with care’” (P12). One mother claimed that her ex-husband actually caused her daughter’s disability by pushing the girl aggressively and claiming she was not his daughter when she confronted him to ask him to support the family. This wasn’t the case for every family though, where some fathers were caring, supportive, and actively involved in the family: “My husband supports what I do, he advises me. He is not only my husband, he is my father, my brother, my teacher and my everything. When I get angry, he calms me down.” (P5).
Participants described various ways that they interacted as a family, for example eating or drinking coffee together or celebrating holy days together. However, also relationally, they described the spectrum of emotional connection from love, care, and unity within the family, to conflict (particularly between parents and sometimes leading to divorce or rejection by the father). When asked to describe her family’s ‘good’ or ‘satisfactory’ life, a university-educated aunt with a supportive husband said: “With everything we got, we live in love, harmony, consulting and caring for each other” (P5). Unity and peace within the family came through as a desired attribute of FQOL, though many families recognised that this was not their reality. Other participants also affirmed the importance of love and care within the family. Communication between family members was another aspect of family interactions, although participants mainly described the challenges of communicating with their child with a disability. Many of them explained how they (or other close family members) were the only ones who understood their child and could respond to their needs. Interestingly, a couple of participants, both single mothers, described how their families had regular family ‘meetings’: “Every Friday is a family meeting. We evaluate everyone’s week and give constructive feedback regarding our behaviour, interactions with family members and others and performance of our duties in and outside the house. All of us take part in it. My oldest son leads the meeting and we all take note.” (P20).
Most family members mentioned how they prioritised their children, particularly their child with a disability, and sacrificed in order for their children to have a better life: “There are times when I only feed him and I fast for I couldn’t be able to provide.” (P17). Caregivers wanted to see all of their children become independent and successful. Many of them also tried to shield their children from the brunt of their harsh, impoverished lives. An aunt of an 11-year-old girl with a disability shared how she made a ‘pretend’ birthday celebration for the girl, making a cake and inviting friends even though she could not really afford it, because the girl was upset that she had been excluded from a neighbourhood celebration. This participant also spoke out against discrimination and advocated for her child’s right to education. Several other caregivers advocated for their children for health services, equipment, and housing.
3.2.2. “There Are some Who Understand and Others Will Take Offense”—Relationships with the Community
All of the participants described both positive and negative relationships with people outside of their immediate family, including relatives, neighbours/friends, as well as support providers. These external relationships either supported or detracted from the core family unit, affecting FQOL. All of the families received some support from others, although it was often inadequate to meet their needs. Some families received very little support from relatives/extended family and were dependent on the charity of strangers or organisations such as CBR. Relationships with the community were important for families’ practical survival, but also for their sense of belonging and connection within the community.
Families described contrasting experiences of people showing compassion and understanding for their situation versus discrimination and exclusion. Many of them were grateful for support from others and actually invoked blessings sporadically during the interviews. Several participants explained how they were better off in an urban environment such as Gondar, because people were generous and willing to support them. Support came from both friends and strangers. Some people supported families of children with disabilities by giving them money or food (especially on holy days) or providing emotional support through encouragement or respite. Spirituality also infused relationships with others, as one mother described how she was taking her daughter with a disability to a place with holy water (Tsebel): “Once we were on our way to the Tsebel place and this woman told me to not hate my child whatever situation I go through and I said, ‘How could I hate her when I am the one who brought her to this world’. And she said ‘Your child is God’s guest. He didn’t give her to you because you have sinned more than other people, but to test you with his creation’. And I was happy to hear her words and took a lesson to endure whatever challenges come my way” (P18).
Unfortunately, discrimination and stigma from others (both family and the community) were also a common experience. Stigma was often associated with spiritual beliefs around the cause of disability (i.e., sin, curse from God) and mothers were particularly blamed. The stigma surrounding disability meant that many people hide their children with disabilities. However, one mother described her relief on receiving support from the CBR program and realising that there are others in a similar situation: “I would be happy if people come out instead of hiding their children with a disability. At first, I thought I was the only one who has a child with a disability. But now I learn there are a lot of people hiding their child with a disability. They need to bring them out so that they can get the support they need. I realised I wasn’t the only one who has a child with a disability when I came to CBR” (P18). Several families described their social isolation both because of discrimination, but also because of the burden of caring for a child with a disability and being restricted in their ability to go out and interact with others. In contrast, one mother described how, instead of retreating socially, her family used discriminatory experiences to teach their son: “whenever he is outside playing with other kids and they do something bad, they mostly blame it on him knowing that he couldn’t speak up. So, when we receive complaints from the neighbours about him, we sit him down and tell him what is good and bad and how he should do or not do certain things” (P15).
Participants also described their lives in comparison to others and how they wanted to be like ‘everyone else’. Caregivers wanted to work like others and hoped their children with disabilities would be able to function independently, and access education and employment, like children without disabilities. They experienced disappointment and sadness when their child with a disability was unable to participate with other children or was treated differently. Parents also described feeling inadequate when their children would compare their family with other better-off families and want what they have. In contrast, one mother expressed gratitude when comparing herself to others who were worse off: “There are a lot of people with many problems in every household. When I see such people, I thank God for making mine easier” (P20).
3.3. “It’s Good to Stand by Yourself”—Wanting to Be Self-Sufficient
Although participants unquestionably appreciated support from others, there was a strong sense that families valued being able to provide for themselves and wanted to improve their family’s life through their efforts, particularly through work and education. This ethic seemed to generalise to families’ whole lives, although having a child with a disability added other dimensions and challenges to being self-sufficient. It was interesting to note that families did not want to have to ask for help explicitly, as this was associated with shame, whereas discretion was seen as a strength: “When our family struggles, we just keep that at home. We don’t appear to be struggling for other people. We will not talk about our problem to someone outside of our household, for I will think that I can work and make money as long as we are healthy. I will just think that I have even when I don’t” (P10).
Every participant mentioned employment as crucial for families to be self-sufficient and provide for themselves, and hence necessary for FQOL. The opportunity to work, regardless of the type, was seen as a source of independence, pride, and hope and a means for families to overcome challenges and rise out of poverty. However, many of them, particularly mothers, spoke of their inability or restrictions to work because of caring for their child with a disability. For those without a working husband or family member to support them, they resorted to begging and relying on support from strangers or organisations (such as CBR). However, they acknowledged that this is unsustainable, and they would prefer to work themselves and provide for their families through a reliable income. “I want to work and not expect from others. It’s a bit difficult for me not because I can’t work, but only because of my son’s problem.” (P4). A couple of participants also mentioned how COVID-19 had resulted in lost employment for themselves or another family member. Some participants had employment but still lamented that it was insufficient or barely covered basic necessities (i.e., particularly if they were daily labourers with no regular income) and several suggested that running their own business would be more profitable and sustainable. However, they recognised that starting a business requires initial capital so this was the kind of sustainable support they would prefer rather than just ongoing ‘handouts’. Some participants acknowledged the benefits of saving to prepare for a better future and facilitate change; however, this was a luxury once basic needs were met. Having income to buy land or build their own house was seen as important for a ‘good’ and stable life for their family as many were struggling with rent or living in government-subsidised housing.
Families spoke about how each family member should contribute, particularly by working, but in whatever capacity they can: “If we can work in collaboration, in respect, in understanding” (P1). Participants also hoped that their children (including their children with disabilities) would eventually be able to secure employment. In some circumstances, grown-up children were already working to support the family, even having dropped out of school to be able to financially contribute. Participants mentioned that physical health was more important than material wellbeing because as long as they were healthy and able, they could work and therefore provide for their family’s material needs: “Physical wellbeing is very important. Because when you are healthy, you can work and get money. But if you are not healthy, no one will have you work for them and you won’t have money.” (P8).
Similarly, education was frequently mentioned by participants as a means of improving life, not just for the individual child but for the whole family. Caregivers affirmed that education was important for all of their children, including children with disabilities, but many were unable to send their children to school because they could not afford it or because they were unable to provide the support to their child that schools demanded. Only a quarter of school-aged children were in school, and these included only children with physical disabilities or deaf, none with intellectual or multiple disabilities. Education was seen as an investment in that it increased their children’s employment prospects and, hence, ability to contribute and provide for the family, but it was also valued in and of itself for improving their child’s mental health, as a source of enjoyment, and for teaching morals and discipline. Parents hoped that their children could continue their education: “For the future, if the children learn, I have hope. […] I tell them to learn so that they will become someone” (P3).
It was striking to note how, in the midst of sometimes-desperate need, participants described that in order to have a ‘good’ life as a family, they needed basic necessities (e.g., food, shelter, clothing), and ‘extras’ were good so that they could give their children special food or treats; however, many of them clearly stated that they did not want excessive wealth, rather they wanted enough to be able to share and give to others: “I would be happy if I could have enough but not a lot.” (P4).
3.4. “Being a Parent Is a Big Responsibility and a Difficult One”—Challenges Raising Children with Disabilities
Hearing the stories of families of children with disabilities in Gondar clearly highlighted the immense daily burdens that many face because of poverty as well as the additional challenges of raising a child with a disability. Although some families were more financially stable, all of the participants described difficulty in providing for their family and some were barely scraping by, depending on the kindness of others. Caregivers expressed sorrow that they could not provide adequately for their children: “A child raised with every need fulfilled is not the same as a child whose needs aren’t met. On top of it, if the child is with a disability, it makes things worse” (P18). Rising costs of living put additional strains on families who could barely afford the basic necessities.
All of the participants described the additional challenges of raising a child with a disability that were exacerbated by poverty. Caregivers frequently mentioned how they were unable to work or were limited in their ability to do daily tasks and socialise because of the constant attention required for the child with a disability: “Raising a child with disability is really difficult […] How can I work when it takes me 3 hours to feed him?” (P7). Physical health was also affected because many caregivers had to carry their child on their backs due to children’s limited mobility, lack of mobility equipment, or inaccessible/unaffordable public transport. Caring became increasingly difficult as caregivers aged, particularly for grandmothers responsible for children. Children with disabilities needed medical treatment which added both financial and time/energy costs. Participants compared the difference between raising children with and without disabilities and one mother lamented that her life was snatched away because of the burdens of raising her child with a disability. For some families, the struggles of life seemed too great to bear: “There is nothing good about my life. My life is messed up. I can’t commit suicide for I fear heaven’s door being closed on me. And, I don’t have a comfortable life to live. When I find one thing, I miss another. Nothing ever gets fulfilled. I am hurt and I hate living.” (P17). Others continued to persevere and hope despite their challenges.
Families of children with behavioural challenges had significantly more difficulties raising their children and participating in their communities, negatively affecting FQOL: “I couldn’t have worked. Because my son’s behaviour is difficult. He yells and hits people. He can’t get along with the kids. There were many occasions where he hit kids and I was asked to cover for their treatment” (P13). Caregivers described how children with disabilities were more demanding, crying excessively or lashing out because they had limited ways to communicate. These behaviours restricted families’ socialisation and many caregivers were reluctant to leave their children under the care of others, allowing minimal respite. Some were concerned for the safety of their children if they left them with others, even resorting to locking them at home alone: “The biggest problem for me is I lock her at home when I go to work. I would just leave the key at the neighbour’s in case something happens. I can’t leave her at home without locking the doors. I am worried someone would do harm to her. I don’t want boys to be around her when I am not around; they might hurt her [sexually]. I wish she was a boy, the risk would be less” (P18). Families were also concerned about inaccessible physical environments that hindered their children’s ability to safely participate.
Despite the challenges of raising children, and children with disabilities particularly, one mother acknowledged: “But the love they have for me is priceless” (P19). Caregivers took their parenting responsibilities seriously, highlighting the importance of providing basic necessities for their children as well as love and care, even if they had to sacrifice: “Till the day I die, eating what we have together, I will raise them like a hen raises her chicks” (P2). Participants spoke about their role in raising responsible, independent children who can positively contribute to the community. As evidenced by most of the participants being mothers (or female caregivers), females took the brunt of parenting responsibilities. Some were also responsible for caring for ill husbands or other family members. However, having support from others, and particularly a supportive husband, was seen as necessary for successfully raising children.
3.5. “When I Get the Support, My Family Will Live a Better Life”—The Role of Support for FQOL
Even though families wanted to be self-sufficient and able to provide for themselves, many participants highlighted their need for material resources to be able to meet their family’s basic needs and have a ‘good’ life: “To me, support means money, things, clothes and in general doing good deeds. For example, if you feed me when I am starving, give me something to drink when I am thirsty, that means you have supported me. When you clothe me too” (P6). As mentioned previously, some families relied on others for their basic needs because they were unable to work and maintain a regular income (e.g., the three grandmothers). One mother expressed her hope for free education because she was currently unable to send her daughter with a disability to school: “If I had money, I would be able to spend it on my daughter so that she can attend her education. I always feel bad for not doing this to her because I didn’t have money. […] but if I get support for her with her education that would contribute a lot to the family. That would be the biggest support for me” (P16). Sometimes religious institutions (e.g., church, mosque) provided support, particularly during holy days or special seasons. The CBR program was a major source of material support for families, providing food, clothing, money, and soap. Several participants mentioned receiving extra money or food because of COVID-19 and they were grateful for this, but they recognised it as only temporary. Some families benefited from respite support from their neighbours, but more often than not, they struggled to manage their responsibilities whilst caring for their child with a disability.
Families reported receiving minimal support from health services apart from basic hospital treatment and some physiotherapy from the CBR program, although one participant mentioned that COVID-19 had disrupted CBR home visits. However, despite initially claiming no support, most participants had some interaction with support providers, currently or in the past. Although participants recognised the benefits of medical treatment, they were often unable to afford it. Children with disabilities also needed equipment (e.g., wheelchairs, hearing aids), but parents shared how even if they were given equipment, it was often broken or inappropriate. Some families were disillusioned with medical treatments and resorted to traditional methods instead, but even these options left them disappointed: “I brought him to Gondar hospital when the fever got worse. However, they [the doctors] didn’t know what it was. Then, I tried traditional medicine when the hospital treatment didn’t show any improvements. The traditional medicine wouldn’t give him relief as well. After that I was given some trainings to be able to help him with mobility” (P12). Overall, families had positive interactions with CBR workers and were grateful for the material, physical, and emotional support that they received.
Finally, many participants spoke about the importance of emotional support, even though they did not necessarily initially classify it as ‘support’. Emotional support came from immediate family, relatives/community, and CBR, and it was described in terms of providing “ideas” or being available to “listen”. Emotional support positively affected FQOL by decreasing worries and stress, offering comfort, increasing confidence and self-esteem, giving hope, and encouraging families despite their challenges. It was in direct contrast to the stigma and discrimination that some families faced. Interestingly, emotional support was also connected with self-sufficiency, as one father stated: “Support means collaboration. Collaborate so that I can be motivated, I can grow and I can stand on my own. It is something that could make my mind sane” (P9). Again, participants’ spiritual faith was a crucial source of emotional support, and some religious institutions provided emotional support as well as material support.
4. Discussion
This study explored how families of children with various disabilities in Gondar, Ethiopia, conceptualised FQOL and how support contributed to FQOL. Spiritual beliefs and values were core to FQOL for every family and were the lens through which families made sense of their lives, including disability and life struggles. Spirituality also informed relationships within the immediate family and with relatives and others in the community which subsequently shaped FQOL. Families described their need for support to live a ‘satisfying’ life, but many also expressed their desire to be self-sufficient (as a family) and not dependant on others long-term. In fact, they hoped to be able to provide for their families and then have enough to help others. Our findings showed the pervasive burden of poverty that exacerbated additional challenges that families experienced because they had a child with a disability. Support from others, both formally and informally, helped to counteract the burdens for some families, but participants expressed an overwhelming need for more support.
4.1. How Do Families Conceptualise FQOL?
When asked to imagine their family living the best possible life, many participants appeared to have difficulty articulating this abstract concept of FQOL. This could have resulted from a limitation in translation, but it also highlights the overall complexity of FQOL. Many family members instead shared how they would feel “happy” if they did have a ‘good’ life. However, less explicitly, participants did describe a ‘good’ or ‘satisfactory’ family life in terms of loving, peaceful, and caring relationships, where family members contributed to the wellbeing of each other and shared the burden of various challenges (particularly due to poverty). Conversely, research exploring folklore and traditions of parenting and socialisation of children in Ethiopia’s Amhara region highlights how parent-child attachment is traditionally discouraged, emotions are restrained and discipline is authoritarian (particularly from fathers) as children’s behaviour reflects on the parents [53]; however, children desire more love, care, respect and time from their parents [54]. Loving, close-knit, respectful and accepting family relationships as well as unity and solidarity within the family are affirmed in international literature as crucial for FQOL [1,4,14,34,55,56,57,58]. Our participants also highlighted that harmonious and caring relationships with others and participation in their community was important for FQOL. In exploring hierarchical relationships in Orthodox Ethiopia, Malara and Boylston [59] describe Ethiopians as having “a profoundly relational outlook on life” (p.53). However, they describe both positive and negative aspects, where relationships can paradoxically demonstrate love and care, as well as power and submission. As well as relational harmony, in terms of FQOL, families wanted all of their children to have the same opportunities as others and a better life than they themselves, especially related to education and the prospect of future employment [4,26,54].
Similar to many other studies of families of children with disabilities in African con-texts, we found that spirituality and religion strongly contributed to FQOL for Ethiopian families [14,28,34,60,61,62,63]. Spirituality encompasses broader, more personal beliefs values and meaning, whilst religion refers to institutionally established practices, disciplines and beliefs; however, for our participants, these were frequently intertwined and were both important for FQOL. Ethiopia is a religious country with ancient Christian roots as well as a significant Muslim minority, and religion permeates cultural identities and values in general, but also in regard to attitudes towards disability [64,65,66,67]. Some participants even seemed surprised to be asked about the influence of spirituality, assuming it to be a foundational, taken-for-granted aspect of life. We noted some negative aspects of spiritual beliefs where several participants described the stigma they experienced because people assumed their child’s disability was caused by sin or a curse (particularly blaming the mother); whilst stigma is experienced universally by families of children with disabilities, these overt expressions of stigma appear more common in LMICs and perhaps connect to stronger expressions of spirituality [62,68,69,70,71,72]. However, for our participants, the over-arching effect of spirituality was positive. Families’ spiritual values helped them to accept their children and was a major source of emotional support as well as religious institutions providing some practical support (i.e., food). Spirituality affected relationships between family members as well as with those outside of the family. Perhaps surprising for families who were often extremely poor, some of our participants shared how they wanted to be able to give back and help others because they understood the challenges of raising a child with a disability. These altruistic values appear to be rooted in their spiritual values. Other studies have demonstrated the universal link between altruism and wellbeing, highlighting how helping others can give people a sense of meaning and purpose, broaden their perspective from focusing on their own struggles, and strengthen social integration, even if they themselves have limited resources [73,74,75,76,77,78]. Considering the foundational role of spirituality to family life in Ethiopia, perhaps existing FQOL measures need adaptation to better capture the significance of spirituality.
4.2. Moderating Factors on Families’ Aspirations for Self-Sufficiency and FQOL
4.2.1. The Confining Demands of Basic Survival
Our findings indicated that many families still required basic support for survival (i.e., food, shelter, clothing), particularly those who were incapable of maintaining employment. Although giving basic social assistance (i.e., money) to families in poverty is controversial, Shepherd, Wadugodapitiya, and Evans [79] argue that social assistance is crucial for those who are vulnerable and chronically poor, and rather than creating dependency, it can in fact, promote saving, development, participation, and improve social networks as it “interrupts the intergenerational transmission of poverty” (p.1). Our findings demonstrated that families did indeed want to provide for themselves; however, they needed the initial capital to start a business or to buy educational resources for their children to attend school. Poverty has complex structural causes, therefore families of children with disabilities in Ethiopia cannot be responsible for overcoming poverty by their hard work alone [79]. Ethiopia has a productive safety net program to support chronically poor households and whilst this has been shown to improve household well-being [80], there may be other negative effects on families (e.g., reduced education of children if they are expected to contribute to labour) [81]. Additionally, Carruth and Freeman [82] warn that food-for-work aid programs in Ethiopia are exploitative and do not alleviate poverty or improve economic development because people are expected to work for inadequate recompense. Endris and colleagues [83] describe how social capital is an important influence on the provision of social assistance in Ethiopia – those with more social capital (i.e., larger networks and diverse relationships) receive more support because resources are often shared. This highlights the increased vulnerability of families who are stigmatised and excluded from typical social structures/networks. Perhaps targeting trustworthy support groups, rather than individual families, can better identify families who are genuinely vulnerable, minimise corruption, and more efficiently disperse resources [83]. With the complex, yet pervasive link between poverty and disability, disability-specific issues also need to be considered in development policies and programs [63,84].
4.2.2. Employment
As our findings demonstrated, employment and the opportunity to earn an income was important for families of children with disabilities and participants reported that employment affects FQOL. As well as financial benefits, work can give parents of children with disabilities a sense of purpose and identity outside of their caregiver role as well as respite from their home responsibilities [85,86]. However, across the world, having a child with a disability can often restrict caregivers’ ability to find and maintain work because of the additional burden of care, particularly for mothers [68,71,85,87,88,89,90,91]. In a literature review exploring work family balance for parents of children with disabilities, Brown and Clark [92] found that single mothers with more and younger children with increased behavioural challenges and unreliable childcare had lower employment rates and poorer work family balance. In a patriarchal society such as Ethiopia [93,94], families with unsupportive husbands/fathers may have less opportunities for employment and securing income, as well as other negative effects on FQOL. Traditional views of women can portray them as weak, dependent, and untrustworthy and they are discouraged from leadership roles [53]. Very few of our participants had a stable source of income, where many were daily labourers or involved in petty trade. This was reflected in the lowincome levels of all of our participants, where many did not even know what their monthly income was. Nonetheless, like other caregivers of children with disabilities in African contexts, our participants also demonstrated a strong desire to work and provide for their families rather than rely on donations from others [28,84,95]. Most families wanted to be self-sufficient and work hard to overcome their challenges. Perhaps this value of independence (not individualism) and hard work ties to the cultural pride that many Ethiopians hold due to their ancient culture and resistance to colonisation [96,97,98]. Families need support to engage in employment and earn an income. The literature describes various supportive factors that can facilitate employment for families of children with disabilities, including improving workplace policies to provide autonomy, flexibility, paid leave, supportive organisational cultures, and quality childcare [86,87,89,92]. In an African context, Clark et al. [99] describe the benefits of subsidised childcare (though not specifically for children with disabilities) to improve employment for poor urban mothers in Kenya, which could also help to close the gender gap in employment. Safe, quality childcare appears to be a critical need to support families of children with disabilities in African contexts and improve FQOL [28,91,100,101]. The link between higher education levels and improved employment outcomes [35,71,102,103] indicates that supporting parents to improve their educational qualifications could also be beneficial and improve FQOL.
4.2.3. Education
Education for children with disabilities was highlighted as another significant means for improving FQOL, with immediate and long-term benefits for both the child as well as the whole family, such as inclusion, and future prospects of better employment and self-sufficiency. Education can promote child development, skill acquisition, social inclusion, positive self-perception, stigma reduction, and empower children with disabilities to be more self-sufficient and contribute meaningfully to their community [26,104]. School attendance for the child with a disability also provides respite to caregivers and gives them opportunities to work [105,106]. Although Ethiopia is moving forward in improving education for children with disabilities, and public primary schools are required to accept all children unconditionally, in reality, this is not the case and very few children with disabilities attend schools [107,108,109]. Most of our participants seemed unaware of their child’s right to education or could not afford it and most of the children with disabilities were not going to school. Low expectations of children’s abilities, overprotection, as well as economic constraints can all create barriers for children with disabilities to participate [110]. Additionally, the explicit gender stereotypes in traditional Ethiopian culture can undermine the value of educating girls [53]. Tonegawa [107] explored both teachers’ and parents’ perceptions of inclusive education in Addis Ababa; they found that whilst teachers were positive about the philosophy and importance of inclusive education, they had limited resources, skills, time and support to implement it effectively. In contrast, most parents were not even aware of inclusive education and although they were grateful if their child was accepted into school and they noted benefits on their child’s social and communication skills, they also described a lack of understanding, support and expertise for their children with disabilities. Perhaps, instead of a ‘one track’ approach that focuses exclusively on inclusive education, schools in Ethiopia could consider complementary approaches, including disability awareness raising, teacher training, and provision of human and material resources for special schools, special needs education, and inclusive education [104,108,109].
4.3. How Does Support Contribute to FQOL?
Even families with a stable income expressed a need for more support and that having a child with a disability exacerbated existing needs. Similar to other studies of families of children with disabilities in African contexts [28,62], our families primarily identified material/instrumental needs such as money, educational resources, transport, and respite. Some families mentioned the need for more emotional support (i.e., someone to talk to, understanding from others) and those with stronger social networks clearly had better FQOL, affirming the link found in other African studies between emotional/social support, particularly from family, and FQOL [35,56,111,112,113]. Physical support (i.e., health services, medications) was also needed and most participants were dissatisfied with disability-related services similar to families across the world [4,14]. Very few participants directly spoke about the need for more information; however, inadvertently, their lack of awareness on their child’s specific disability and what supports were available or their rights to education demonstrated a need for more informational support. To contribute positively to FQOL, families need support that is family-centred and strengths-based, focusing on family assets, autonomy, and empowerment, with respectful, reciprocal partnerships between families and providers [4,55,114,115,116,117,118,119,120,121]. In a recent scoping review, Kokorelias and colleagues [122] identify key universal aspects for family-centred support, including collaboration between families and providers, considering the family’s context, ensuring flexible policies and procedures, and providing education to individuals, families and support providers.
4.3.1. Peer-Support Groups
Families would benefit from peer-support groups, as one of our mothers shared how important it was for her to realise that she was not alone and that there are other children with disabilities and families experiencing similar challenges. Several participants spoke about the importance of bringing disability into the light and raising awareness and acceptance in the community, even by just having their children with disabilities more visibly present. Peer-support groups can provide material and informational support, as well as emotional support, promoting inclusion and belonging, and helping families of children with disabilities to cope better with challenges and thrive [4,28,62,84,90,123,124,125,126]. Peer-support groups can also be a means of empowering women through facilitating income-generating activities and social support [123] as well as a platform for parent skills training [127].
4.3.2. Community-Based Rehabilitation
Community-Based Rehabilitation (CBR) is a strategy, initially developed by the World Health Organisation, to promote the rights of people with disabilities through equal access to support, empowerment and poverty reduction, particularly in LMICs [128]. Strengthening local CBR programs could benefit the appropriate distribution of resources to families of children with disabilities. CBR can be an important means for providing holistic support to families, including practical material support (e.g., food, money), rehabilitation (e.g., therapy, mobility aids), emotional support, information, and raising community awareness around disability [28,112,129,130,131,132,133,134]. All of our families were connected to the CBR project in Gondar, and many described how CBR had distributed money and hygiene supplies during COVID-19. The provision of appropriate equipment through CBR programs would benefit families as many participants spoke about having to carry their children, with serious consequences on parents’ health [105,135,136]. In terms of supporting emotional wellbeing, CBR could be involved in counselling, as many of our families spoke about the benefits of talking with others and sharing their burdens [84,137,138].
4.4. Limitations
We sought to comprehensively explore the perceptions of FQOL and support from family members of children with disabilities in Gondar, Ethiopia; however, there are some limitations that need to be considered when interpreting our results. Although we purposefully sampled to obtain a broad range of family members and disability types, our participants were still primarily mothers. Mothers are usually the primary caregivers of children with disabilities in Ethiopia and often have the most insight into family life, thus they are an important voice to be heard. Additionally, most Ethiopian children with disabilities do not have a formal medical diagnosis so we relied on the CBR program’s records to obtain a representation of different types of disability, different age levels, and a balance of male/female children. Families were recruited through contacts with the UoG CBR program, therefore were not necessarily representative of all families of children with disabilities in Ethiopia. Although some had very minimal support, families still had a connection with CBR, which may have influenced their perceptions of FQOL. In congruence with the exploratory nature of the current study, we chose to focus on experiences of families whose children represent a diverse range of disabilities. This may have influenced the depth of understanding of issues related to specific disabilities and FQOL. Further research is needed to explore FQOL for families of children with specific types of disabilities in an Ethiopian context.
Cross-cultural research has inherent limitations. Although we followed the advice of local Ethiopian colleagues for recruitment and data collection, language differences sometimes created a barrier. Analysing in the original language is preferable [43,45,139]; however, the primary researcher was unable to understand Amharic, hence was dependent on translations of transcripts into English to understand the findings. The research was slowed down by occasional miscommunications and waiting for each interview to be transcribed in Amharic and then translated into English. We experienced some discrepancies between the audio-recordings and transcriptions, hence another bilingual Ethiopian colleague, not connected to the research, listened to the interview audios independently and revised the English translations accordingly. Translation always introduces possible meaning loss; however, we attempted to accurately represent the voices of our participants through these additional checks. One of the authors, SD, is a local in Gondar, hence he provided invaluable information, advice, and assistance throughout the research. We also experienced difficulties where two initial interviews were not captured on the audio-recorder due to technical failures.
In addition, COVID-19 created challenges and some limitations to the research. The primary researcher had initially planned to spend extended time in the field in Gondar to better understand the context, but this was cut short due to the pandemic. Travel became more difficult for people within Gondar, and although we provided reimbursement for transport, some people may have been reluctant to travel for an interview during the uncertain times. We had to ensure COVID-19 protocols were followed, including providing masks, hand sanitiser, and ensuring social distancing during the interviews, which may have affected the quality of interviews and building rapport.
5. Conclusions
Families of children with disabilities in Ethiopia described FQOL in terms of relationships within the family and with others in the community where spiritual beliefs and values were foundational to their worldview. Having a child with a disability added significant challenges for families in terms of additional costs and care burden and limiting opportunities for education, employment, and social participation. These challenges were compounded by pervasive poverty. Although families wanted to work hard to be self-sufficient and provide for themselves, they recognised their need for support and highlighted the current lack of support. Culturally appropriate, family-centred support that considers families’ basic needs as well as employment, education, and social support would help families of children with disabilities to enhance FQOL.
Author Contributions
Conceptualisation, J.J.-v.V., R.L., B.B., and H.M.A.; methodology, J.J.-v.V., S.D., and H.M.A.; analysis, J.J.-v.V., R.L., B.B., and H.M.A.; resources, S.D.; writing—original draft preparation, J.J.-v.V.; writing—review and editing, J.J.-v.V., R.L., B.B., S.D., and H.M.A.; supervision, H.M.A. All authors have read and agreed to the published version of the manuscript.
Funding
The first author received funding for her PhD from the Queen Elizabeth II Diamond Jubilee Scholarship program from Universities Canada, Rideau Hall Foundations, and Community Foundations Canada (2018–2021). However, the funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Health Sciences Research Ethics Board of Queen’s University (protocol code #6028643, 20 February 2020) and the Institutional Ethical Review Board of the University of Gondar (10 March 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are not publicly available due to privacy reasons.
Acknowledgments
We would like to sincerely thank Molalign Belay for his ongoing support in the ‘field’ and throughout this research project. We would also like to thank Bilen Mekonnen for all of her time, insight, and support in reviewing the interview translations. Thank you also to Ansha Nega for supporting the data collection and providing invaluable advice about research in Ethiopia. We are thankful for various other colleagues who assisted with translation and advice regarding research in Ethiopia: Mulugeta Bayisa, Hiwot Temesgen, and Abey Abebe. A huge thank you to the CBR supervisors who assisted in recruitment for this study, but especially for all of their hard work in supporting families of children with disabilities. Finally, we would like to thank the family members who gave up their time and were willing to share some of their lives with us despite often very difficult circumstances (made more challenging during COVID-19!).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wang, M.; Brown, R. Family quality of life: A framework for policy and social service provisions to support families of children with disabilities. J. Fam. Soc. Work 2009, 12, 144–167. [Google Scholar] [CrossRef]
- Boelsma, F.; Caubo-Damen, I.; Schippers, A.; Dane, M.; Abma, T.A. Rethinking FQoL: The dynamic interplay between individual and family quality of life. J. Policy Pract. Intellect. Disabil. 2017, 14, 31–38. [Google Scholar] [CrossRef]
- Turnbull, A.P.; Brown, I.; Turnbull, R. (Eds.) Families and People with Mental Retardation: International Perspectives; American Association on Mental Retardation: Washington, DC, USA, 2004; ISBN 0-940898-87-X. [Google Scholar]
- Brown, R.I.; Kyrkou, M.R.; Samuel, P.S. Family quality of life. In Health Care for People with Intellectual and Developmental Disabilities across the Lifespan; Rubin, L.I., Merrick, J., Greydanus, D.E., Patel, D.R., Eds.; Springer International Publishing: Cham, Switzerland, 2016. [Google Scholar]
- Samuel, P.S.; Rillotta, F.; Brown, I. Review: The development of family quality of life concepts and measures. J. Intellect. Disabil. Res. 2012, 56, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Zuna, N.; Summers, J.A.; Turnbull, A.P.; Hu, X.; Xu, S. Theorizing about family quality of life. In Enhancing the Quality of Life of People with Intellectual Disabilities: From Theory to Practice; Kober, R., Ed.; Springer: Dordrecht, The Netherlands, 2010; pp. 241–278. [Google Scholar]
- Chiu, C.; Kyzar, K.; Zuna, N.; Turnbull, A.; Summers, J.A.; Gomez, V.A. Family quality of life. In The Oxford Handbook of Positive Psychology and Disability; Wehmeyer, M.W., Ed.; Oxford University Press: New York, NY, USA, 2013; pp. 365–392. [Google Scholar]
- International Association for the Scientific Study of Intellectual and Developmental Disabilities (IASSIDD). Families supporting a child with intellectual or developmental disabilities: The current state of knowledge. J. Appl. Res. Intellect. Disabil. 2014, 27, 420–430. [Google Scholar] [CrossRef]
- Brown, R.I.; Schippers, A. The background and development of quality of life and family quality of life: Applying research, policy, and practice to individual and family living. Int. J. Child Youth Family Stud. 2018, 9, 1–11. [Google Scholar] [CrossRef]
- Jackson, C.W.; Wegner, J.R.; Turnbull, A.P. Family quality of life following early identification of deafness. Lang. Speech Hear. Serv. Sch. 2010, 41, 194–205. [Google Scholar] [CrossRef]
- Kyzar, K.B.; Brady, S.E.; Summers, J.A.; Haines, S.J.; Turnbull, A.P. Services and supports, partnership, and family quality of life: Focus on deaf-blindness. Except. Child. 2016, 83, 77–91. [Google Scholar] [CrossRef]
- Hu, X.; Wang, M.; Fei, X. Family quality of life of Chinese families of children with intellectual disabilities. J. Intellect. Disabil. Res. 2012, 56, 30–44. [Google Scholar] [CrossRef]
- Isa, S.N.I.; Aziz, A.A.; Rahman, A.A.; Ibrahim, M.I.; Ibrahim, W.P.W.; Mohamad, N.; Othman, A.; Rahman, N.A.; Harith, S.; Van Rostenberghe, H. The impact of children with disabilities on parent health-related quality of life and family functioning in Kelantan and its associated factors. J. Dev. Behav. Pediatr. 2013, 34, 262–268. [Google Scholar] [CrossRef]
- Ajuwon, P.M.; Brown, I. Family quality of life in Nigeria. J. Intellect. Disabil. Res. 2012, 56, 61–70. [Google Scholar] [CrossRef]
- Richard, B.O. Families, well-being, and inclusion: Rethinking priorities for children with cognitive disabilities in Ladakh, India. Childhood 2014, 21, 308–323. [Google Scholar] [CrossRef]
- Bhopti, A.; Rangwala, S.; Sachdev, S. Family quality of life when there is a child with disability in India. J. Intellect. Disabil. Res. 2019, 63, 847. [Google Scholar] [CrossRef]
- World Health Organisation (WHO). World Report on Disability; World Health Organisation: Geneva, Switzerland, 2011; Available online: https://www.who.int/disabilities/world_report/2011/report.pdf (accessed on 28 June 2021).
- United Nations Children Fund (UNICEF). Children and Young People with Disabilities Fact Sheet; UNICEF: New York, NY, USA, 2013; Available online: https://sites.unicef.org/disabilities/files/Factsheet_A5__Web_REVISED(1).pdf (accessed on 28 June 2021).
- Fong, V.C.; Gardiner, E.; Iarocci, G. Cross-cultural perspectives on the meaning of family quality of life: Comparing Korean immigrant families and Canadian families of children with autism spectrum disorder. Autism 2021, 25, 1335–1348. [Google Scholar] [CrossRef]
- Jansen-van Vuuren, J.; Nuri, R.P.; Nega, A.; Batorowicz, B.; Lysaght, R.; Aldersey, H.M. Family quality of life for families of children with disabilities in African contexts: A scoping review. Qual. Life Res. 2021. under review. [Google Scholar]
- Kyzar, K.B.; Turnbull, A.P.; Summers, J.A.; Gomez, V.A. The relationship of family support to family outcomes: A synthesis of key findings from research on severe disability. Res. Pract. Persons Severe. Disabil. 2012, 37, 31–44. [Google Scholar] [CrossRef]
- Nuri, R.P.; Batorowicz, B.; Aldersey, H.M. Family support and family and child-related outcomes among families impacted by disability in low- and middle-income countries: A scoping review. J. Child Health Care 2019, 24, 637–654. [Google Scholar] [CrossRef]
- Chala, M.B.; Mekonnen, S.; Andargie, G.; Kebede, Y.; Yitayal, M.; Alemu, K.; Awoke, T.; Wubeshet, M.; Azmeraw, T.; Birku, M.; et al. Prevalence of disability and associated factors in Dabat Health and Demographic Surveillance System site, northwest Ethiopia. BMC Public Health 2017, 17, 762. [Google Scholar] [CrossRef]
- United Nations Children Fund (UNICEF). Ethiopia Children: Factsheet 2018; UNICEF: New York, NY, USA, 2018; Available online: https://www.unicef.org/ethiopia/media/216/file/Ethiopia%20Children%20Fact%20Sheet%202018.pdf (accessed on 28 June 2021).
- Weldeab, C.T.; Opdal, L.R. Raising a Child with Intellectual Disabilities in Ethiopia: What Do Parents Say? In Proceedings of the Annual Meeting of the American Educational Research Association; Chicago, IL, USA, 8–13 April 2007. Available online: https://files.eric.ed.gov/fulltext/ED496076.pdf (accessed on 28 June 2021).
- Tefera, B.; Schippers, A.; van Engen, M.; van der Klink, J. The experiences of children with disabilities and primary caregivers on the social inclusion of children with disabilities in Ethiopia. Int. J. Child Youth Family Stud. 2018, 9, 146–167. [Google Scholar] [CrossRef]
- Wariyo, S.J. Growing up with Disability in Ethiopia: The Perspectives and Experiences of Physically Disabled Children. Master’s Thesis, Norwegian University of Sciences and Technology, Trondheim, Norway, 2016. Available online: https://ntnuopen.ntnu.no/ntnu-xmlui/handle/11250/2458385 (accessed on 28 June 2021).
- Aldersey, H.M.; Ahmed, A.N.; Tesfamichael, H.N.; Lotoski, N. Needs of families of children with intellectual and developmental disabilities in Addis Ababa. Afr. J. Disabil. 2020, 9, 1–11. [Google Scholar] [CrossRef]
- Hunter, D.J.; McCallum, J.; Howes, D. Defining exploratory-descriptive qualitative (EDQ) research and considering its application to healthcare. J. Nurs. Health Care 2019, 4, 1–7. [Google Scholar] [CrossRef]
- Swedish International Development Cooperation Agency (SIDA). Disability Rights in Ethiopia; SIDA: Stockholm, Sweden, 2014; Available online: https://sidase-wp-files-prod.s3.eu-north-1.amazonaws.com/app/uploads/2021/05/07125813/rights-of-persons-with-disabilities-ethiopia.pdf (accessed on 28 June 2021).
- Ministry of Labour and Social Affairs (MoLSA). National Plan of Action of Persons with Disabilities: 2012–2021; Ministry of Labour and Social Affairs (MoLSA): Addis Ababa, Ethiopia, 2012; Available online: https://www.ilo.org/dyn/natlex/natlex4.detail?p_isn=94528&p_lang=en (accessed on 5 July 2021).
- United Nations (UN). Convention on the Rights of Persons with Disabilities (CRPD). Available online: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities.html (accessed on 11 July 2021).
- Aldersey, H.M. Family perceptions of intellectual disability: Understanding and support in Dar es Salaam. Afr. J. Disabil 2012, 1, 32. [Google Scholar] [CrossRef]
- Aldersey, H.M.; Francis, G.L.; Haines, S.J.; Chiu, C.Y. Family quality of life in the Democratic Republic of the Congo. J. Policy Pract. Intellect. Disabil. 2017, 14, 78–86. [Google Scholar] [CrossRef]
- Schlebusch, L.; Dada, S.; Samuels, A. Family quality of life of South African families raising children with autism spectrum disorder. J. Autism Dev. Disord. 2017, 47, 1966–1977. [Google Scholar] [CrossRef] [PubMed]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample size in qualitative interview studies: Guided by information power. Qual. Health Res. 2015, 26, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Durham, J. Ethical challenges in cross-cultural research: A student researcher’s perspective. Aust. N. Z. J. Public Health 2014, 38, 509–512. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, C.; Whitley, R.; Wondimagegn, D.; Alem, A.; Prince, M. Postnatal mental distress in relation to the sociocultural practices of childbirth: An exploratory qualitative study from Ethiopia. Soc. Sci. Med. 2009, 69, 1211–1219. [Google Scholar] [CrossRef]
- Jakobsen, H. Focus groups and methodological rigour outside the minority world: Making the method work to its strengths in Tanzania. Qual. Res. 2012, 12, 111–130. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Al-Amer, R.; Ramjan, L.; Glew, P.; Darwish, M.; Salamonson, Y. Translation of interviews from a source language to a target language: Examining issues in cross-cultural health care research. J. Clin. Nurs. 2015, 24, 1151–1162. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Kushner, K.E.; Mill, J.; Lai, D.W.L. Understanding the language, the culture, and the experience: Translation in cross-cultural research. Int. J. Qual. Methods 2012, 11, 652–665. [Google Scholar] [CrossRef]
- Oxley, J.; Günhan, E.; Kaniamattam, M.; Damico, J. Multilingual issues in qualitative research. Clin. Linguist. Phon. 2017, 31, 612–630. [Google Scholar] [CrossRef]
- MacKenzie, C.A. Filtered meaning: Appreciating linguistic skill, social position and subjectivity of interpreters in cross-language research. Qual. Res. 2016, 16, 167–182. [Google Scholar] [CrossRef]
- Richardson, E.Z.L.; Allison, K.R.; Teleguario, H.; Chacach, W.; Tum, S.; Gesink, D.; Berry, A. “Taking Care” in intercultural research: Lessons from a Guatemalan family planning study. Int. J. Qual. Methods 2017, 16, 1–13. [Google Scholar] [CrossRef]
- Ilesanmi, O. What is cross-cultural research? Int. J. Psychol. Stud. 2009, 1, 82–96. [Google Scholar] [CrossRef]
- Im, E.-O.; Page, R.; Lin, L.-C.; Tsai, H.-M.; Cheng, C.-Y. Rigor in cross-cultural nursing research. Int. J. Nurs. Stud. 2004, 41, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Walter, L. Feminist anthropology? Gend. Soc. 1995, 9, 272–288. [Google Scholar] [CrossRef]
- Caretta, M.A. Situated knowledge in cross-cultural, cross-language research: A collaborative reflexive analysis of researcher, assistant and participant subjectivities. Qual. Res. 2015, 15, 489–505. [Google Scholar] [CrossRef]
- Liamputtong, P. Doing research in a cross-cultural context: Methodological and ethical challenges. In Doing Cross-Cultural Research: Ethical and Methodological Perspectives; Liamputtong, P., Ed.; Springer: Dordrecht, The Netherlands, 2008; pp. 3–20. [Google Scholar]
- Temple, B.; Young, A. Qualitative research and translation dilemmas. Qual. Res. 2004, 4, 161–178. [Google Scholar] [CrossRef]
- Esposito, N. From meaning to meaning: The influence of translation techniques on non-English focus group research. Qual. Health Res. 2001, 11, 568–579. [Google Scholar] [CrossRef]
- Belay, M. Part I: An inventory of folklore genres pertaining to parenting and children socialization among the Amhara the case of South Wollo and North Sehewa. In An Inventory of Folklore Genres Pertaining to Parenting and Children Socialization among the Ethiopian Communities; Chala, D.G., Ed.; Ethiopian Society of Sociologists, Social Workers and Anthropologists: Addis Ababa, Ethiopia, 2018; pp. 16–37. [Google Scholar]
- Mekuriaw, D.; Berhan, W.; Tarekegn, Y.; Basazinew, B. Part II: An inventory of folklore genres pertaining to parenting and children socialization among the Amhara the case of Debre Markos, Burie and Woreta towns and surrounding areas. In An Inventory of Folklore Genres Pertaining to Parenting and Children Socialization among the Ethiopian Communities; Chala, D.G., Ed.; Ethiopian Society of Sociologists, Social Workers and Anthropologists: Addis Ababa, Ethiopia, 2018; pp. 38–60. [Google Scholar]
- Bhopti, A.; Brown, T.; Lentin, P. Family quality of life. J. Early Interv. 2016, 38, 191–211. [Google Scholar] [CrossRef]
- Ntswane, A.M.; van Rhyn, L. The life-world of mothers who care for mentally retarded children: The Katutura township experience. Curationis 2007, 30, 85–96. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Barlindhaug, G.; Umar, E.; Wazakili, M.; Emaus, N. Living with disabled children in Malawi: Challenges and rewards. Afr. J. Disabil. 2016, 5, a254. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Greeff, A.P.; Nolting, C. Resilience in families of children with developmental disabilities. Fam. Syst. Health 2013, 31, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Malara, D.M.; Boylston, T. Vertical love: Forms of submission and top-down power in Orthodox Ethiopia. Soc Anal 2016, 60, 40–57. [Google Scholar] [CrossRef]
- Oti-Boadi, M. Exploring the lived experiences of mothers of children with intellectual disability in Ghana. SAGE Open 2017, 7, 1–12. [Google Scholar] [CrossRef]
- Muthukrishna, N.; Ebrahim, H. Motherhood and the disabled child in contexts of early education and care. Childhood 2014, 21, 369–384. [Google Scholar] [CrossRef]
- McNally, A.; Mannan, H. Perceptions of caring for children with disabilities: Experiences from Moshi, Tanzania. Afr. J. Disabil. 2013, 2, 1–10. [Google Scholar] [CrossRef]
- Van der Mark, E.J.; Conradie, I.; Dedding, C.W.M.; Broerse, J.E.W. How poverty shapes caring for a disabled child: A narrative literature review. J. Int. Dev. 2017, 29, 1187–1206. [Google Scholar] [CrossRef]
- Girma, M. Religion, politics and the dilemma of modernising Ethiopia. Hervormde Teologiese Studies 2018, 74, 1–9. [Google Scholar] [CrossRef]
- Baye, T.G. Muslims in Ethiopia: History and identity. Afr. Stud. 2018, 77, 412–427. [Google Scholar] [CrossRef]
- Schiemer, M. How to make sense of “developing a sense of belonging” through “feeling like a family” in the light of cultural and societal backgrounds. In Education for Children with Disabilities in Addis Ababa, Ethiopia: Developing a Sense of Belonging; Schiemer, M., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 7–42. [Google Scholar]
- Sonessa, W.L. Rethinking public theology in Ethiopia: Politics, religion, and ethnicity in a declining national harmony. Int. J. Public Theol. 2020, 14, 149–171. [Google Scholar] [CrossRef]
- Pretorius, C.; Steadman, J. Barriers and facilitators to caring for a child with cerebral palsy in rural communities of the Western Cape, South Africa. Child Care Pract. 2018, 24, 413–430. [Google Scholar] [CrossRef]
- Tilahun, D.; Hanlon, C.; Fekadu, A.; Tekola, B.; Baheretibeb, Y.; Hoekstra, R.A. Stigma, explanatory models and unmet needs of caregivers of children with developmental disorders in a low-income African country: A cross-sectional facility-based survey. BMC Health Serv. Res. 2016, 16, 152. [Google Scholar] [CrossRef]
- Cloete, L.G.; Obaigwa, E.O. Lived experiences of caregivers of children with autism spectrum disorder in Kenya. Afr. J. Disabil. 2019, 8, 1–9. [Google Scholar] [CrossRef]
- Marsh, V.M.; Kamuya, D.M.; Molyneux, S.S. ‘All her children are born that way’: Gendered experiences of stigma in families affected by sickle cell disorder in rural Kenya. Ethn. Health 2011, 16, 343–359. [Google Scholar] [CrossRef] [PubMed]
- Tekola, B.; Kinfe, M.; Girma, F.; Hanlon, C.; Hoekstra, R.A. Perceptions and experiences of stigma among parents of children with developmental disorders in Ethiopia: A qualitative study. Soc. Sci. Med. 2020, 256, 113034. [Google Scholar] [CrossRef]
- Post, S.G. Altruism, happiness, and health: It’s good to be good. Int. J. Behav. Med. 2005, 12, 66–77. [Google Scholar] [CrossRef]
- Smith, H.C. Finding purpose through altruism: The potential of ‘doing for others’ during asylum. J. Occup. Sci. 2018, 25, 87–99. [Google Scholar] [CrossRef]
- Hui, B.P.H.; Ng, J.C.K.; Berzaghi, E.; Cunningham-Amos, L.A.; Kogan, A. Rewards of kindness? A meta-analysis of the link between prosociality and well-being. Psychol. Bull. 2020, 146, 1084–1116. [Google Scholar] [CrossRef]
- Dunn, E.W.; Aknin, L.B.; Norton, M.I. Prosocial spending and happiness: Using money to benefit others pays off. Curr. Dir. Psychol. Sci. 2014, 23, 41–47. [Google Scholar] [CrossRef]
- Aknin, L.B.; Barrington-Leigh, C.P.; Dunn, E.W.; Helliwell, J.F.; Burns, J.; Biswas-Diener, R.; Kemeza, I.; Nyende, P.; Ashton-James, C.E.; Norton, M.I. Prosocial spending and well-being: Cross-cultural evidence for a psychological universal. J. Person. Soc. Psychol. 2013, 104, 635–652. [Google Scholar] [CrossRef]
- Chang, Y.-P.; Lin, Y.-C.; Chen, L.H. Pay it forward: Gratitude in social networks. J. Happiness Stud. 2012, 13, 761–781. [Google Scholar] [CrossRef]
- Shepherd, A.; Wadugodapitiya, D.; Evans, A. Social Assistance and the ‘Dependency Syndrome’; Chronic Poverty Research Centre: Manchester, UK, 2011; Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=1765933 (accessed on 28 June 2021).
- Mokomane, Z. Anti-Poverty Family-Focused Policies in Developing Countries; United Nations: New York, NY, USA, 2012; Available online: https://www.un.org/esa/socdev/family/docs/BP_POVERTY.pdf (accessed on 28 June 2021).
- Araya, M.; Hicks, J.H.; Baird, S.; Jones, N. Ethiopia’s productive safety net programme and adolescent well-being: Evidence from the gender and adolescence global evidence (GAGE) study. In What Works for Africa’s Poorest Children? Lawson, D., Angemi, D., Kasirye, I., Eds.; Practical Action Publishing: Rugby, UK, 2020; ISBN 9781780448572. Available online: https://practicalactionpublishing.com/book/2366/what-works-for-africas-poorest-children (accessed on 28 June 2021).
- Carruth, L.; Freeman, S. Aid or exploitation?: Food-for-work, cash-for-work, and the production of “beneficiary-workers” in Ethiopia and Haiti. World Dev. 2021, 140, 105283. [Google Scholar] [CrossRef]
- Endris, G.S.; Kibwika, P.; Obaa, B.B.; Hassan, J.Y. How social capital can inform targeting formal social safety net interventions in vulnerable communities in eastern Ethiopia: An ethnographic case study. J. Int. Humanit. Action 2020, 5, 10. [Google Scholar] [CrossRef]
- Paget, A.; Mallewa, M.; Chinguo, D.; Mahebere-Chirambo, C.; Gladstone, M. “It means you are grounded”—Caregivers’ perspectives on the rehabilitation of children with neurodisability in Malawi. Disabil. Rehabil. 2016, 38, 223–234. [Google Scholar] [CrossRef]
- Marta, S. Work-life (im)balance? An explorative qualitative study among mothers and fathers of persons with disabilities. Gender Disabil. Res. 2020, 16, 40–55. [Google Scholar] [CrossRef]
- Scott, E.K. Mother-Ready Jobs: Employment that works for mothers of children with disabilities. J. Fam. Issues 2018, 39, 2659–2684. [Google Scholar] [CrossRef]
- Lien, K.; Lashewicz, B.; Mitchell, J.; Boettcher, N. Blending traditional and nurturing fathering: Fathers of children with autism managing work and family. Fam. Relat. 2021, 70, 264–281. [Google Scholar] [CrossRef]
- Pinto, O.Y.; Raz, R. Employment outcomes after a birth of a child with a developmental disability: A national nested case-control study. J Autism Dev. Disord. 2021, 51, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Vinck, J.; Van Lancker, W. An intersectional approach towards parental employment in families with a child with a disability: The case of Belgium. Work Employ. Soc. 2020, 34, 228–261. [Google Scholar] [CrossRef]
- Van der Mark, E.J.; Conradie, I.; Dedding, C.W.M.; Broerse, J.E.W. ‘We create our own small world’: Daily realities of mothers of disabled children in a South African urban settlement. Disabil. Soc. 2019, 34, 95–120. [Google Scholar] [CrossRef]
- Gona, J.K.; Newton, C.R.; Rimba, K.K.; Mapenzi, R.; Kihara, M.; Vijver, F.V.; Abubakar, A. Challenges and coping strategies of parents of children with autism on the Kenyan coast. Rural Remote Health 2016, 16, 1–12. [Google Scholar]
- Brown, T.J.; Clark, C. Employed parents of children with disabilities and work family life balance: A literature review. Child Youth Care Forum 2017, 46, 857–876. [Google Scholar] [CrossRef]
- Liranso, B.E. A Critical Analysis of Women Employment. Int. J. Soc. Polit. Humanit. 2020, 7, 71–75. [Google Scholar]
- Ayele, M.G. Challenging the patriarchal national security. In The Gender Imperative; Routledge: New Delhi, India, 2018; pp. 85–107. [Google Scholar] [CrossRef]
- Nyante, G.G.; Carpenter, C. The experience of carers of children with cerebral palsy living in rural areas of Ghana who have received no rehabilitation services: A qualitative study. Child Care Health Dev. 2019, 45, 815–822. [Google Scholar] [CrossRef]
- Kebede, K. ‘Ethiopia is misunderstood’: Transnationalism among second-generation Ethiopian Americans. Afr. Black Diaspora 2019, 12, 243–266. [Google Scholar] [CrossRef]
- Tempelhoff, J. The Ethiopian example: Time for taking bold steps in our neck of the woods? J. Transdiscip. Res. South. Afr. 2019, 15, 2. [Google Scholar] [CrossRef]
- Steward, J.A. The Battle For The Battle of Adwa: Collective Identity and Nation-Building. Master’s Thesis, City College of New York, New York, NY, USA, 2020. Available online: https://academicworks.cuny.edu/cgi/viewcontent.cgi?article=1898&context=cc_etds_theses (accessed on 28 June 2021).
- Clark, S.; Kabiru, C.W.; Laszlo, S.; Muthuri, S. The impact of childcare on poor urban women’s economic empowerment in Africa. Demography 2019, 56, 1247–1272. [Google Scholar] [CrossRef]
- Hemming, E.; Akhurst, J. Mothers’ life-worlds in a developing context when a child has special needs. Indo Pacific J. Phenomen. 2009, 9, 1–12. [Google Scholar] [CrossRef][Green Version]
- McKenzie, J.A.; Kahonde, C.; Mostert, K.; Aldersey, H.M. Community participation of families of children with profound intellectual and multiple disabilities in South Africa. J Appl. Res. Intellect. Disabil. 2021, 34, 525–536. [Google Scholar] [CrossRef]
- Awadalla, H.I.; Kamel, E.G.; Mahfouz, E.M.; Mohamed, A.A.; El-Sherbeeny, A.M. Determinants of maternal adaptation to mentally disabled children in El Minia, Egypt. East Mediterr. Health J 2010, 16, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, F.M.S.; Ali, S.M.; Mustafa, M.A.A. Quality of life of cerebral palsy patients and their caregivers: A cross sectional study in a rehabilitation center Khartoum-Sudan (2014–2015). J. Neurosci. Rural Pract. 2016, 7, 355. [Google Scholar] [CrossRef]
- Schiemer, M. (Ed.) Reality bites: Listening to children, parents, teachers and other experts. In Education for Children with Disabilities in Addis Ababa, Ethiopia: Developing a Sense of Belonging; Springer International Publishing: Cham, Switzerland, 2017; pp. 87–136. [Google Scholar]
- Geere, J.L.; Gona, J.; Omondi, F.O.; Kifalu, M.K.; Newton, C.R.; Hartley, S. Caring for children with physical disability in Kenya: Potential links between caregiving and carers’ physical health. Child Care Health Dev. 2013, 39, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Den Besten, J.; Cornielje, M.T.; Cornielje, H.; Botwey, D.N. Supporting parents in caring for children with disability in Ghana. DCID 2016, 27, 87–101. [Google Scholar] [CrossRef][Green Version]
- Tonegawa, Y. Policy and practice of “inclusive education” in Addis Ababa, Ethiopia: An analysis from the perspectives of teachers and parents of children with disabilities. Nilo Ethiop. Stud. 2019, 2019, 31–45. [Google Scholar] [CrossRef]
- Tefera, B.; Admas, F.; Mulatie, M. Education of children with special needs in Ethiopia: Analysis of the rhetoric of ‘education for all’ and the reality on the ground. Ethiop. J. Educ. 2015, 35, 45–97. [Google Scholar]
- Franck, B.; Joshi, D.K. Including students with disabilities in Education for All: Lessons from Ethiopia. Int. J. Incl. Educ. 2017, 21, 347–360. [Google Scholar] [CrossRef]
- Khan, G.; Isaacs, D.; Makoae, M.G.; Fluks, L.L.; Mokhele, T.; Mokomane, Z. Service providers’ perceptions of families caring for children with disabilities in resource-poor settings in South Africa. Child Fam. Soc. Work 2020, 25, 823–831. [Google Scholar] [CrossRef]
- Ahlert, I.A.; Greeff, A.P. Resilience factors associated with adaptation in families with deaf and hard of hearing children. Am. Ann. Deaf 2012, 157, 391–404. [Google Scholar] [CrossRef]
- Njelesani, J.; Couto, S.; Cameron, D. Disability and rehabilitation in Tanzania: A review of the literature. Disabil. Rehabil. 2011, 33, 2196–2207. [Google Scholar] [CrossRef]
- Bannink, F.; Stroeken, K.; Idro, R.; van Hove, G. Community knowledge, beliefs, attitudes, and practices towards children with spina bifida and hydrocephalus in Uganda. Int. J. Disabil. Dev. Educ. 2015, 62, 182–201. [Google Scholar] [CrossRef]
- Boehm, T.L.; Carter, E.W. Family quality of life and its correlates among parents of children and adults with intellectual disability. Am. J. Intellect. Dev. Disabil. 2019, 124, 99–115. [Google Scholar] [CrossRef]
- Boehm, T.L. Predictors of Family Quality of Life among Parents of Children and Adults with Intellectual Disability. Ph.D. Thesis, Vanderbilt University, Nashville, TN, USA, 2017. Available online: https://www-proquest-com.proxy.queensu.ca/docview/2178445671?pq-origsite=primo (accessed on 28 June 2021).
- Kuhaneck, H.M.; Madonna, S.; Novak, A.; Pearson, E. Effectiveness of interventions for children with autism spectrum disorder and their parents: A systematic review of family outcomes. Am. J. Occup. Ther. 2015, 69, 1–14. [Google Scholar] [CrossRef]
- Davis, K.; Gavidia-Payne, S. The impact of child, family, and professional support characteristics on the quality of life in families of young children with disabilities. J. Intellect. Dev. Disabil. 2009, 34, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Resch, J.A.; Mireles, G.; Benz, M.R.; Grenwelge, C.; Peterson, R.; Zhang, D. Giving parents a voice: A qualitative study of the challenges experienced by parents of children with disabilities. Rehabil. Psychol. 2010, 55, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Balcells-Balcells, A.; Giné, C.; Guàrdia-Olmos, J.; Summers, J.A.; Mas, J.M. Impact of supports and partnership on family quality of life. Res. Dev. Disabil. 2019, 85, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Hanna, S.; King, G.; Hurley, P.; King, S.; Kertoy, M.; Rosenbaum, P. Factors affecting family-centred service delivery for children with disabilities. Child Care Health Dev. 2003, 29, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Zuna, N.; Gracia, M.; Haring, S.H.; Aguilar, J.M. Parental perceptions and satisfaction with family services in families of children with autism spectrum disorder and other developmental disabilities. J. Intellect. Dev. Disabil. 2016, 41, 233–242. [Google Scholar] [CrossRef]
- Kokorelias, K.M.; Gignac, M.A.M.; Naglie, G.; Cameron, J.I. Towards a universal model of family centered care: A scoping review. BMC Health Serv. Res. 2019, 19, 564. [Google Scholar] [CrossRef]
- Aldersey, H.M.; Turnbull, A.P.; Turnbull, H.R. Family support in Kinshasa, Democratic Republic of the Congo. J. Policy Pract. Intellect. Disabil. 2016, 13, 23–32. [Google Scholar] [CrossRef]
- Halstead, E.J.; Griffith, G.M.; Hastings, R.P. Social support, coping, and positive perceptions as potential protective factors for the well-being of mothers of children with intellectual and developmental disabilities. Int. J. Dev. Disabil. 2018, 64, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Bray, L.; Carter, B.; Sanders, C.; Blake, L.; Keegan, K. Parent-to-parent peer support for parents of children with a disability: A mixed method study. Patient Educ. Couns. 2017, 100, 1537–1543. [Google Scholar] [CrossRef] [PubMed]
- Cole, L.; Kharwa, Y.; Khumalo, N.; Reinke, J.; Karrim, S. Caregivers of school-aged children with autism: Social media as a source of support. J. Child Fam. Stud. 2017, 26, 3464–3475. [Google Scholar] [CrossRef]
- Zuurmond, M.; O’Banion, D.; Gladstone, M.; Carsamar, S.; Kerac, M.; Baltussen, M.; Tann, C.J.; Gyamah Nyante, G.; Polack, S. Evaluating the impact of a community-based parent training programme for children with cerebral palsy in Ghana. PLoS ONE 2018, 13, 1–17. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation (WHO); International Labour Organisation (ILO); United Nations Educational, Scientific and Cultural Organization (UNESCO). CBR: A Strategy for Rehabilitation, Equalization of Opportunities, Poverty Reduction and Social Inclusion of People with Disabilities: Joint Position Paper; World Health Organisation: Geneva, Switzerland, 2004; Available online: https://apps.who.int/iris/bitstream/handle/10665/43060/9241592389_eng.pdf?sequence=1&isAllowed=y (accessed on 28 June 2021).
- McKenzie, J.A.; McConkey, R.; Adnams, C. Intellectual disability in Africa: Implications for research and service development. Disabil. Rehabil. 2013, 35, 1750–1755. [Google Scholar] [CrossRef]
- Hartley, S.; Ojwang, P.; Baguwemu, A.; Ddamulira, M.; Chavuta, A. How do carers of disabled children cope? The Ugandan perspective. Child Care Health Dev. 2005, 31, 167–180. [Google Scholar] [CrossRef]
- Shumba, T.W.; Moodley, I. Implementation of disability policy framework in Namibia: A qualitative study. S. Afr. J. Physiother. 2018, 74, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Cameron, D.L.; Nixon, S.; Parnes, P.; Pidsadny, M. Children with disabilities in low-income countries. Pediatr. Child Health 2005, 10, 269–272. [Google Scholar] [CrossRef]
- Boyce, W.; Cote, L. The influence of HIV/AIDS on community-based rehabilitation in Dar Es Salaam, Tanzania. Asia Pacific Disabil. Rehabil. J. 2009, 20, 52–72. [Google Scholar]
- Hansen, A.M.W.; Siame, M.; Van der Veen, J. A qualitative study: Barriers and support for participation for children with disabilities. Afr. J. Disabil. 2014, 3, 1–9. [Google Scholar] [CrossRef]
- Tigere, B.; Makhubele, J.C. The experiences of parents of children living with disabilities at Lehlaba protective workshop in Sekhukhune district of Limpopo province. Afr. J. Disabil. 2019, 8, 1–9. [Google Scholar] [CrossRef]
- Patel, P.; Baier, J.; Baranov, E.; Khurana, E.; Gambrah-Sampaney, C.; Johnson, A.; Monokwane, B.; Bearden, D.R. Health beliefs regarding pediatric cerebral palsy among caregivers in Botswana: A qualitative study. Child Care Health Dev. 2017, 43, 861–868. [Google Scholar] [CrossRef]
- Aldersey, H.M.; Turnbull, R.H.; Turnbull, A.P. Intellectual and developmental disabilities in Kinshasa, Democratic Republic of the Congo: Causality and implications for resilience and support. Intellect. Dev. Disabil. 2014, 52, 220–233. [Google Scholar] [CrossRef]
- Masulani-Mwale, C.; Mathanga, D.; Silungwe, D.; Kauye, F.; Gladstone, M. Parenting children with intellectual disabilities in Malawi: The impact that reaches beyond coping? Child Care Health Dev. 2016, 42, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Abalkhail, J.M. Challenges of translating qualitative management data. Gend. Manag. 2018, 33, 66–79. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).