Abstract
A thorough biomechanical understanding of human organs is of increasing importance for designing and improving a wide range of medical technologies from simulators to medical devices. Despite the crucial need for data, little procedure-specific biomechanical testing on human tissue has been published. Specifically, pancreatic duct anastomosis, which has high rates of complications related to pancreatic duct leakage and patency, could benefit from improved assistive technologies. This study aims to help characterize the biomechanics of this critical step of the procedure by measuring the suture pullout force (SPOF) of the pancreatic duct and capsule. 216 tests were performed on 33 fresh, unfixed donated human pancreases. A previously reported uniaxial testing frame, was used to measure the SPOF of the pancreases. The mean pancreatic duct SPOF was 2.62 ± 1.11 N and the mean pancreatic capsule SPOF was 1.99 ± 1.33 N. To our knowledge, this is the first reported human pancreatic duct and capsule suture pullout measurement. These data can be used to inform a wide variety of biomedical technologies with primary interest in high-fidelity training simulators.
1. Introduction
The pancreas is a soft, relatively flat retroperitoneal organ consisting of three main regions; the head, body, and tail, surrounded by a thin, mostly fibrous network of loose connective tissue called the pancreatic capsule. Within the head, body, and tail, the main pancreatic duct joins the common bile duct with the duodenum [1]. The primary function of the pancreas is to facilitate the storage of food by releasing insulin. Secondarily, it enables movement of food by releasing glucagon, a glucose controlling hormone, in response to lack of food [2].
The pancreaticoduodenectomy (Whipple) procedure is an exceedingly delicate and complex surgical procedure in which the head of the pancreas, gallbladder, duodenum, distal bile duct, and sometimes the distal portion of the stomach are removed. A Whipple procedure can be used to treat a variety of pancreatic, intestinal, and biliary disorders, most commonly to remove tumors in the head of the pancreas [3]. The Whipple procedure has a postoperative morbidity rate of up to 50%. Many of these postoperative issues arise from the pancreatic duct-to-jejunum anastomosis (pancreaticojejunostomy) [4]. These complications from the pancreaticojejunostomy might be life-threatening. For example, tearing of the sutures in the pancreas capsule or pancreatic duct can lead to capsule or duct disruption and the consequent pancreatic leak (up to 28% incidence [4]), fistula (12% incidence [5]), and biliary obstruction (<3% incidence [6]).
Considering these complications, one important biomechanical parameter of interest is the suture pullout force (SPOF) taken as the maximum safe force that can be applied to a suture before tearing the tissue. SPOF is also referred to as suture retention strength, suture holding capacity, and anastomotic strength [7,8]. SPOFs of the pancreatic duct and capsule are most relevant for the pancreaticojejunostomy step of the procedure, which is considered to be the “Achilles heel of pancreatic surgery” due to high rates of complications [9]. Low SPOFs are believed to be directly related to pancreatic leakage [7,9]. There has been some work analyzing the suture holding capacity in the pancreatic duct using a Newton dynamometer [7], however, much like most soft tissues, the pancreas is viscoelastic [10]. Therefore, tissue failure is rate-dependent and a suture pullout force is more accurately derived using a constant slow strain rate [10].
The aim of this study is to conduct a biomechanical characterization of the human pancreas through the analysis of pancreatic duct and pancreatic capsule SPOF. There are several potential applications of these data. One is to inform the development of a high-fidelity pancreas simulation for training and assessment of the psychomotor skills necessary to successfully and safely perform a pancreatic anastomosis. When combined with an analysis of demographic data, including the effects of age, sex, and BMI on the SPOF, these data could be invaluable for improving personalized and realistic simulations. Improvements in simulation fidelity and implementation will improve medical education for the goal of reducing patient morbidity and mortality caused by medical error. A potential clinical application is the development of smart surgical tools end-effectors that could gauge, inform and assist surgeons by calculating and interpreting intraoperative forces in real time.
2. Materials and Methods
2.1. Tissue Preparation
Pancreases were recovered from fresh, unfixed organ donors. Samples were tested within 72 h of death and were stored in University of Wisconsin (UW)® solution at 4 °C. Prior to testing, samples were removed from refrigeration and brought to room temperature. Samples were hydrated regularly with Wisconsin solution throughout experimentation. Thirty-three total unique donors were included in this study. Further breakdown of donor demographics is shown in Table 1.

Table 1.
Donor demographics by test performed.
2.2. Suture Pullout Force Characterization
A previously reported modular laboratory-developed load frame known as DEXTER was used for all tests [11]. In short, DEXTER consists of a screw-driven load frame with various fixtures that can be attached to a load cell (REB7, Loadstar® Sensors, Fremont, CA, USA) to measure uniaxial compressive and tensile forces. The load cell is fixed to a stepping motor (E25 XSLIDE, Velmex, Bloomfield, NY, USA) that can be rotated. Before testing, the load cell was calibrated with 10–100 g weights to validate accuracy of force measurement in the appropriate range for our measurements.
The pancreas was divided at the neck in order to expose the pancreatic duct and provide access to the capsule for SPOF experiments. Two hundred sixteen pancreatic duct SPOF tests were performed on 33 pancreases. Cross sections of the pancreas were prepared using a No. 10 blade scalpel. 4-0 Covidien Sofsilk® (Minneapolis, MN, USA) sutures were chosen to be consistent with standard Whipple procedure protocol [9]. These sutures were looped through one side of the pancreatic duct wall (Figure 1a). The length of tissue between the loop (bite size) was measured with calipers. The suture strings were tied to the DEXTER attachment using a square knot, as it’s the gold standard for surgical procedures, as shown in Figure 1b [12]. The pancreas was placed on Siafast 80-grit sandpaper and firmly, manually held in place to prevent slippage. The suture was pulled in tension at 1.58 mm/s and the tensile force was measured continuously. The peak force before specimen failure was taken as the SPOF. Similarly, for the capsule, suture pullout, 4-0 Covidien Sofsilk® sutures were looped through the capsule and the capsule of the pancreas, attached to DEXTER, and pulled in tension until tissue failure occurred. Seventy-nine capsule SPOF tests were performed on 16 pancreases. After each test, the area of test was removed from the pancreas to expose a new, undeformed region.

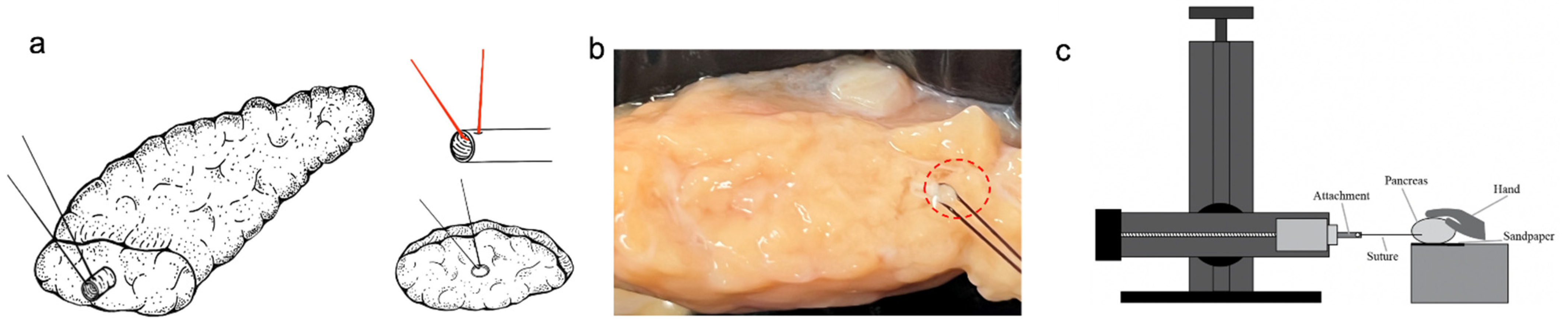
Figure 1.
Pancreas suture pullout test setup. (a) The schematic shows a suture placed through the pancreatic duct with bite size being between the end of the duct and the suture site. (b) The suture is placed through the pancreatic duct before being secured to the (c) rotatable DEXTER uniaxial force measurement load frame. Sandpaper, preload, and manual stabilization of SPOF tests are used to prevent slip.
2.3. Statistical Analysis
To examine the statistical relationship between various donor characteristics and SPOF values, we conducted a sequential multiple linear regression using IBM® SPSS® version 26.0 (IBM®, New York, NY, USA) [13]. The SPOF was used as the dependent variable. Age, body mass index (BMI), and sex were the independent variables. For the sequential multiple linear regression, the order of inputs were driven by previously reported data [7,14]. Sex was input first, followed by age, and finally BMI. Sex was coded as a binary variable with female being 0 and male being 1. The change in the correlation coefficient (R2) was reported for each variable in addition to the overall correlation with multiple factors. The slope coefficient calculated for these factors was also reported.
3. Results
3.1. Suture Pullout Force
One pancreatic duct donor was excluded from the results as it was determined to be an outlier with a mean SPOF greater than three standard deviations above the mean. The average SPOF for each donor was reported, with the bite sizes ranging from 0.73 to 5 mm for the capsule and 0.48 to 5 mm for the pancreatic duct. The average pancreatic duct SPOF was 2.62 ± 1.11 N from thirty-two donors. The average capsule SPOF was 1.99 ± 1.33 N from 16 donors. These results are summarized in Table 2, below.
Table 2.
Summary suture pullout force results.
3.2. The Effect of Age, Sex, and BMI on Suture Pullout Force
The suture pullout forces with respect to donor age, sex, and BMI of the pancreatic bile duct and capsule were analyzed using sequential multiple linear regression. For the pancreatic duct suture pullout forces, the R2 change for each variable was 0.351 for sex, 0.004 for age, and 0.026 for BMI. Overall, the R2 of the multiple linear regression was 0.381. This can be interpreted to mean that sex was predicted to be responsible for 35.1% of the variation in duct suture pullout force while age accounted for 0.4% and BMI accounted for 2.6%. All together, these three variables accounted for 38.1% of the variation in duct suture pullout force. Looking at the calculated slope coefficients when all variables were considered, males were predicted to have a 1.144 N higher duct suture pullout force on average than females. Someone who is obese with a BMI of 30 was predicted to have a 0.31 N lower suture pullout force than someone who is a healthy weight with a BMI of 20. Large changes in age were predicted to have negligible differences in SPOF. Of these predictive coefficients, only sex was statistically significant (sex: p = 0.004, age: p = 0.982, BMI: p = 0.289).
Looking at graphical representations of these relationships, the linear regression for age vs. SPOF exhibited a slightly negative slope with respect to both males (R2 = 0.003) and females (R2 = 0.020) (Figure 2a). This behavior was similar when comparing BMI with SPOF, where female donors exhibited a slightly negative slope with an R2 = 0.00, but males resulted in a mildly negative slope with an R2 = 0.144 (Figure 2c). Male donor pancreatic ducts exhibited a higher median SPOF than female donors at 3.45 N vs. 1.84 N, respectively and this difference appears to be significant (Figure 2b).
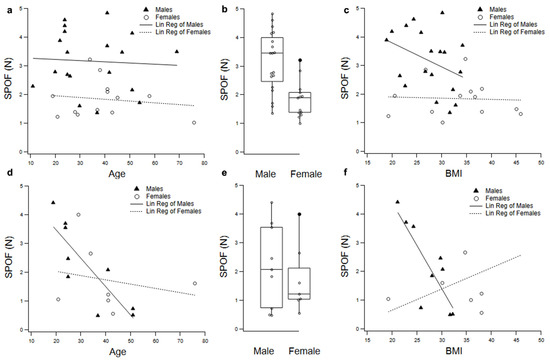
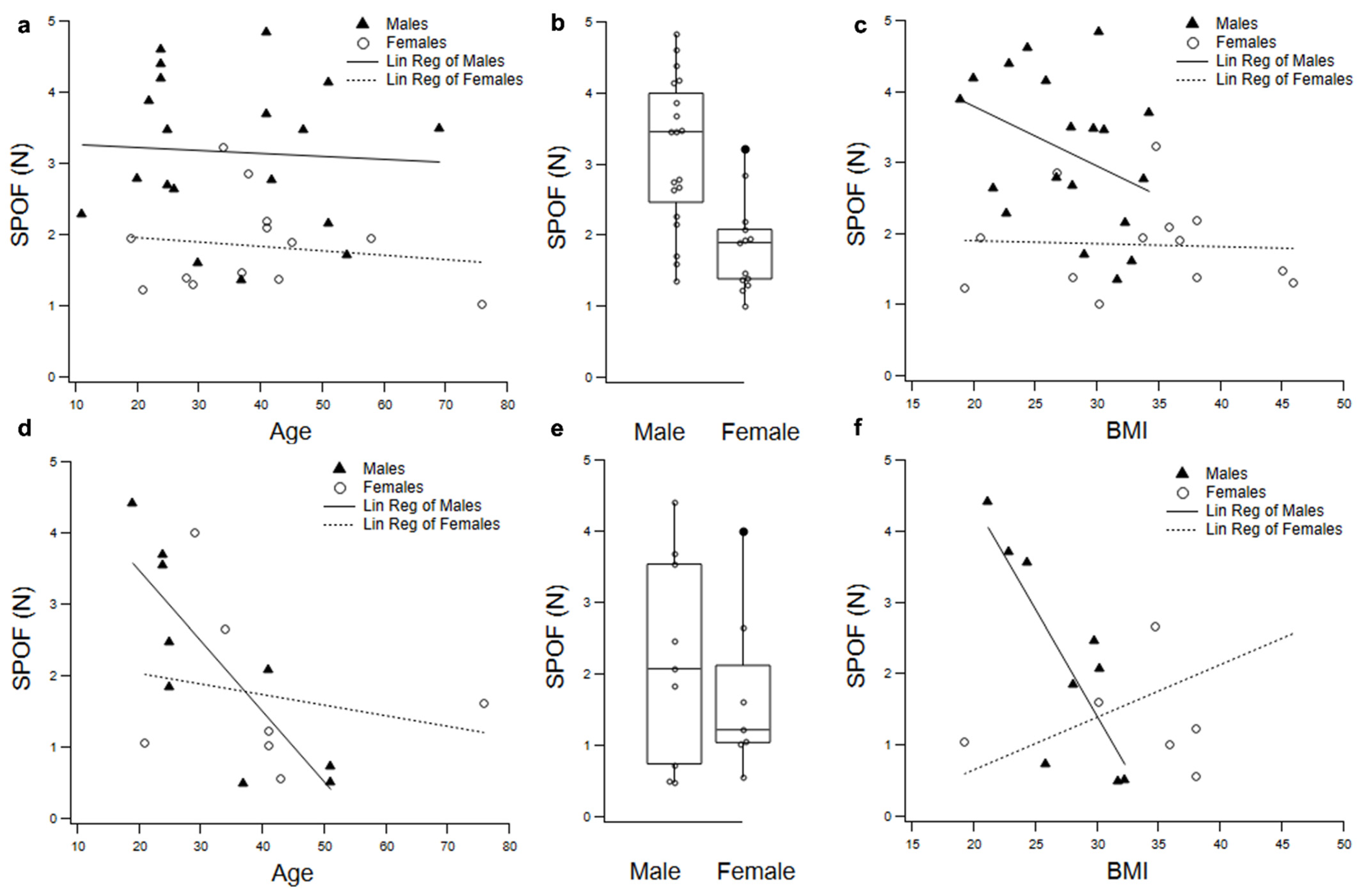
Figure 2.
Demographic analysis of the SPOF of the pancreatic duct and capsule. Each point represents one donor’s average SPOF. Multiple linear regression of the SPOF of the pancreatic duct with respect to (a) age, (b) sex, (c) BMI and the capsule with respect to (d) age, (e) sex, and (f) BMI.
For the multiple linear regression model for the capsule suture pullout forces, the R2 change for each variable was 0.032 for sex, 0.269 for age, and 0.001 for BMI. Overall, the R2 of the multiple linear regression was 0.302. This can be interpreted to mean that sex was predicted to be responsible for 3.2% of the variation in capsule suture pullout force while age accounted for 26.9% and BMI accounted for 0.1%. All together, these three variables accounted for 30.2% of the variation in capsule suture pullout force. Looking at the calculated slope coefficients when all variables were considered, someone who is 60 years old was predicted to have a 1.47 N lower capsule suture pullout force on average than someone who is 30 years old and males were predicted to have a 0.14 N higher capsule suture pullout force than females. The predicted difference in SPOF due to BMI was negligible. None of these predictive coefficients were statistically significant, although age is quite close (sex: p = 0.850, age: p = 0.054, BMI: p = 0.884).
The linear regression for age vs. capsule SPOF exhibited a negative slope for both males (R2 = 0.698) and females (R2 = 0.046) (Figure 2d). The linear regression for BMI vs. SPOF exhibited a steep negative slope for males (R2 = 0.664) and mildly positive slope for females (R2 = 0.255) (Figure 2f). When comparing sex and SPOF (Figure 2e), the median is slightly higher between males and females at 2.07 N and 1.22 N, respectively, but this is not a significant difference.
4. Discussion
Medical error is estimated to be a leading cause of death in the United States [15]. This alarming fact of modern medicine calls for improved medical education. Simulation technologies are a burgeoning surgical education tool. Simulation based medical education has been shown to improve practitioner training [16,17,18]. The most effective anatomical simulators for surgical training are high-fidelity, meaning they look and feel like real human tissue [19]. In order to inform optimized design and manufacturing of high-fidelity medical simulations, thorough biomechanical characterization is necessary.
To optimize surgical simulators, a primary surgically relevant biomechanical parameter of interest is SPOF. When analyzing SPOF experimentally, an important consideration is the depth of suture placement known as bite size. Clinically, if the suture’s bite size is too small, the suture will easily tear which can lead to myriad surgical complications such as anastomosis leakage [7]. If the bite size is too large, the tension on the involved and surrounding tissue may cause necrosis or stenosis [20]. Experimentally, there is no standard bite size for characterizing the suture pullout force of tissues resulting in ranges from 1–5 mm [7,21,22,23,24]; however, Pensalfini et al. evaluated the role of suture bite size on breaking starting strength (BSS) and suture retention strength (reported here as SPOF). It was reported that the BSS and SPOF influence by the bite size was bounded; with clear independence on bite size and thickness of the samples ≥ 2,10 mm, respectively. Our results are similar to previously reported values of the pancreas itself. Belyaev et. al. reported the suture holding capacity of the pancreas of 4.4 ± 1.7 N for patients at risk for postoperative pancreatic fistula and 2.8 ± 0.4 for patients who developed a grade B or C fistula using a 5-0 PDS II suture and a bite size of 5 mm.
The results from this analysis provide an understanding of the suture pullout force of the pancreatic duct and capsule. The order of sequential multiple linear regression was decided based on previously reported results. BMI was entered last as Belyaev et. al. reported a patient with high BMI would exhibit a fatty soft pancreas resulting in decreased SPOF [7]. Age was input second as Chantarojanasiri et al. reported increased hardness of the pancreas with age, specifically at ages > 40 [14]. This increase in hardness is expected to increase the SPOF as reported by Belyaev. Sex was input first as Belyaev et. al. reported SPOF of the pancreas exhibited no significant relationship. With the present data, we found sex to be the only significant demographic effect, with the predictive coefficient having a p-value of 0.004 and accounting for 35% of the variation in pancreatic duct SPOF. For the capsule, age was close to having a significant effect with it accounting for 27% of the variation. More donors over the age of 50 could provide more data into the effects of age on SPOF of the pancreatic duct and capsule; however, the present study utilized a sample of convenience due to donor availability. Few published studies discuss demographic effects on the SPOF of the pancreas. Belyaev et al. reported BMI, and not age or sex, influences the SPOF of the pancreas; however, they targeted the pancreas itself and the pancreatic duct with the pancreas. The presented approach targeted specifically the suture-tissue interactions during the anastomosis which may have resulted in the lower influence.
As is expected in human tissue research, there is substantial variability in the results. Future work will include more donors with health conditions, such as diabetes and fatty infiltration of the pancreas to understand the effect on pancreas biomechanics. This knowledge could be used for individualized, patient specific predictive biomechanical modeling.
Experimental parameters are another likely cause of variation in the results. The reported suture pullout forces were based on peak forces, although more work needs to be done to understand the precise compounding relationships between bite size, exposed surface area/geometry, securement to the test apparatus, and pullout force for the pancreatic duct and capsule. The motivation behind not using a standardized geometry is two-fold. Firstly, to mimic the in-vivo boundary conditions of the pancreatic duct and capsule as much as possible, the surrounding tissue was left intact. Secondly, the pancreas varies in size widely between available donors, making a consistent size difficult. This is a limitation to our findings due to the inability to control for a consistent shape, area, and exposed region of the pancreatic duct and capsule. Due to the large variation in size, the samples were secured with a hand. Future work should utilize a standard geometry with a tighter inclusion criteria and custom designed clamps to control for size and area exposed for testing. The rate of the experiment may also affect the SPOF. The velocity was chosen to be 1.58 mm/s or 94.8 mm/min for two reasons. The primary reason was to reduce the duration the pancreas was exposed to room conditions. Although the sample hydration was maintained by periodically applying solution between experiments, a longer duration test would cause reduced hydration, potentially deteriorating the organ. Additionally, previous work reported on suture retention tests of scaffolds in ophthalmology found a pull rate between 10–100 mm/min leads to negligible difference [21].
These additional data would be essential prior to applying the data towards the future development of smart tools to augment safe performance of this delicate operation. For example, a robot assisted Whipple procedure could employ a device that measures tension in sutures and ensure the expected suture pullout force is never exceeded. Similarly, without haptic sensation, measurement of forces associated with laparoscopic surgical techniques could be a primary source of feedback. The data could also be used to inform computational models of the pancreas that may be integrated with augmented reality assisted simulation training.
In the present study, suture pullout force is reported as the peak force prior to tearing through the pancreatic duct and capsule. Pensalfini et al. reported the observation of mode I crack formation/propagation prior to the peak force on silicone elastomer and porcine pericardium using optical tracking, noting the breaking starting strength (BSS) vs. the suture retention strength (suture pullout force) [8]. Mine et al. reported breakage pattern will depend on material and thereby advocated the use of peak strength and a standard wire guide [25]. The existence of optical tracking to identify crack formation prior to ultimate failure in conjunction with the suture pullout force are both invaluable to understanding the mechanics of the pancreatic duct and capsule, but further studies will have to explore which is more relevant to surgical and simulation needs, as the amount of failure recorded at the BBS may not be enough to cause complications for the patients whereas catastrophic failure of the suture as measured by suture pullout force is surely enough.
As it relates to informing materials development for educational simulators, however, the data has immediate utility. High-fidelity synthetic models of organs and tissues are an increasingly utilized surgical training tool [19]. These simulators have been shown to be an effective mode of education while offering an ethical alternative to practicing on animals or human patients [16,17,18]. Therefore, the first step in developing a useful simulator is to record surgically relevant biomechanical forces, such as suture pullout force. From this, materials can be chosen or developed to match real tissue data. These data provide a range of properties, for which synthetic or virtual training materials/models can be produced. Such data and subsequently, training models other than cadaveric or animal specimens previously did not exist.
5. Conclusions
This paper reports a biomechanical analysis of the fresh, unfixed human pancreas. The mean pancreatic duct SPOF was 2.62 ± 1.11 N and the mean pancreatic capsule SPOF was 1.99 ± 1.33 N. More data and multi-factorial analyses will elucidate demographic, lifestyle, and health factors influencing variability in these measurements which could expand applications of the data into robotic and laparoscopic surgery tool development and computational modeling.
Author Contributions
Conceptualization, A.T.G., J.E.N., M.E.P. and R.M.S.; formal analysis, A.T.G., S.L.B., A.M.D. and J.E.B.; funding acquisition, A.T.G. and R.M.S.; investigation, A.T.G., S.L.B., A.M.D., J.E.B., A.Y.S., A.L.S. and E.Y.W.; methodology, A.T.G., S.L.B., M.E.P. and R.M.S.; supervision, R.M.S.; writing—original draft, A.T.G., S.L.B., J.E.N., M.E.P. and R.M.S.; writing—review and editing, A.T.G., S.L.B., A.M.D., J.E.B., A.Y.S., A.L.S., E.Y.W., J.E.N., M.E.P. and R.M.S. All authors have read and agreed to the published version of the manuscript.
Funding
A.T.G., S.L.B., J.E.B., A.Y.S., A.M.D., A.L.S., E.Y.W., J.E.N. and R.M.S. funded through Department of Defense (DoD) grants #W911NF-16-2-0147 and #W912CG-20-2-0004. M.E.P. was funded through the ACS-AEI Pellegrini/Oelschlager Endowed Fellowship. Research was sponsored by the CCDC-SC and was accomplished under Cooperative Agreement Number W912CG-20-2-0004. The views and conclusions contained in this document are those of the authors and should not be interpreted as representing the official policies, either expressed or implied, of the CCDC-SC or the U.S. Government. The U.S. Government is authorized to reproduce and distribute reprints for Government purposes notwithstanding any copyright notation herein.
Institutional Review Board Statement
Cadaveric pancreases was deemed institutional review board (IRB) exempt by the University of Washington’s Human Subject Division (HSD 52692).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to acknowledge LifeCenter Northwest for providing the pancreases. We would also like to acknowledge Victoria Roach for statistical consulting and Shi-Wen Olivia Yau for creating (Figure 1a).
Conflicts of Interest
At this time the authors declare they have no conflict of interest. S.L.B., J.E.B., A.Y.S., A.L.S. and E.Y.W. performed the research prior to joining their current affiliations.
References
- Mahadevan, V. Anatomy of the pancreas and spleen. Surgery 2019, 37, 297–301. [Google Scholar]
- Krahl, M.E. Endocrine function of the pancreas. Annu. Rev. Physiol. 1974, 36, 331–360. [Google Scholar] [CrossRef] [PubMed]
- Whipple Procedure—Mayo Clinic. Available online: https://www.mayoclinic.org/tests-procedures/whipple-procedure/about/pac-20385054 (accessed on 20 June 2020).
- Katsaragakis, S.; Larentzakis, A.; Panousopoulos, S.-G.; Toutouzas, K.G.; Theodorou, D.; Stergiopoulos, S.; Androulakis, G. A new pancreaticojejunostomy technique: A battle against postoperative pancreatic fistula. World J. Gastroenterol. WJG 2013, 19, 4351–4355. [Google Scholar] [CrossRef] [PubMed]
- Smits, F.J.; Santvoort, H.C.V.; Besselink, M.G.; Batenburg, M.C.T.; Slooff, R.A.E.; Boerma, D.; Busch, O.R.; Coene, P.P.L.O.; van Dam, R.M.; Van Dijk, D.P.J.; et al. Management of Severe Pancreatic Fistula After Pancreatoduodenectomy. JAMA Surg. 2017, 152, 540–548. [Google Scholar] [CrossRef] [PubMed]
- House, M.G.; Cameron, J.L.; Schulick, R.D.; Campbell, K.A.; Sauter, P.K.; Coleman, J.; Lillemoe, K.D.; Yeo, C.J. Incidence and Outcome of Biliary Strictures After Pancreaticoduodenectomy. Ann. Surg. 2006, 243, 571–578. [Google Scholar] [CrossRef]
- Belyaev, O.; Rosenkranz, S.; Munding, J.; Herzog, T.; Chromik, A.M.; Tannapfel, A.; Uhl, W. Quantitative assessment and determinants of suture-holding capacity of human pancreas. J. Surg. Res. 2013, 184, 807–812. [Google Scholar] [CrossRef]
- Pensalfini, M.; Meneghello, S.; Lintas, V.; Bircher, K.; Ehret, A.E.; Mazza, E. The suture retention test, revisited and revised. J. Mech. Behav. Biomed. Mater. 2018, 77, 711–717. [Google Scholar] [CrossRef]
- Azumi, Y.; Isaji, S.; Kato, H.; Nobuoka, Y.; Kuriyama, N.; Kishiwada, M.; Hamada, T.; Mizuno, S.; Usui, M.; Sakurai, H.; et al. A standardized technique for safe pancreaticojejunostomy: Pair-Watch suturing technique. World J. Gastrointest. Surg. 2010, 2, 260–264. [Google Scholar] [CrossRef]
- Wex, C.; Fröhlich, M.; Brandstädter, K.; Bruns, C.; Stoll, A. Experimental analysis of the mechanical behavior of the viscoelastic porcine pancreas and preliminary case study on the human pancreas. J. Mech. Behav. Biomed. Mater. 2015, 41, 199–207. [Google Scholar] [CrossRef]
- Poniatowski, L.H.; Somani, S.S.; Veneziano, D.; McAdams, S.; Sweet, R.M. Characterizing and Simulating Needle Insertion Forces for Percutaneous Renal Access. J. Endourol. 2016, 30, 1049–1055. [Google Scholar] [CrossRef]
- Muffly, T.M.; Boyce, J.; Kieweg, S.L.; Bonham, A.J. Tensile strength of a surgeon’s or a square knot. J. Surg. Educ. 2010, 67, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Corp, I. IBM SPSS Statistics for Windows, Version 26.0.; IBM Co.: Armonk, NY, USA, 2019. [Google Scholar]
- Chantarojanasiri, T.; Hirooka, Y.; Kawashima, H.; Ohno, E.; Sugimoto, H.; Hayashi, D.; Kuwahara, T.; Yamamura, T.; Funasaka, K.; Nakamura, M. Age-related changes in pancreatic elasticity: When should we be concerned about their effect on strain elastography? Ultrasonics 2016, 69, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Makary, M.A.; Daniel, M. Medical error—The third leading cause of death in the US. BMJ 2016, 353, i2139. [Google Scholar] [CrossRef]
- Cook, D.A.; Hamstra, S.J.; Brydges, R.; Zendejas, B.; Szostek, J.H.; Wang, A.T.; Erwin, P.J.; Hatala, R. Comparative effectiveness of instructional design features in simulation-based education: Systematic review and meta-analysis. Med. Teach. 2013, 35, e867–e898. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.B.; Williams, B.A.; Fang, J.B.; Ye, Q.H. A systematic review of selected evidence on improving knowledge and skills through high-fidelity simulation. Nurse Educ. Today 2012, 32, 294–298. [Google Scholar] [CrossRef] [PubMed]
- McGaghie, W.C.; Issenberg, S.B.; Petrusa, E.R.; Scalese, R.J. A critical review of simulation-based medical education research: 2003–2009. Med. Educ. 2010, 44, 50–63. [Google Scholar] [CrossRef]
- Beal, M.D.; Kinnear, J.; Anderson, C.R.; Martin, T.D.; Wamboldt, R.; Hooper, L. The Effectiveness of Medical Simulation in Teaching Medical Students Critical Care Medicine: A Systematic Review and Meta-Analysis. Simul. Healthc. 2017, 12, 104–116. [Google Scholar] [CrossRef] [Green Version]
- Bartlett, L.C. Pressure necrosis is the primary cause of wound dehiscence. Can. J. Surgery. J. Can. De Chir. 1985, 28, 27–30. [Google Scholar]
- Küng, F.; Schubert, D.W.; Stafiej, P.; Kruse, F.E.; Fuchsluger, T.A. Influence of operating parameters on the suture retention test for scaffolds in ophthalmology. Mater. Sci. Eng. C 2017, 77, 212–218. [Google Scholar] [CrossRef]
- Trowbridge, E.; Lawford, P.; Crofts, C. Pericardial heterografts: A comparative study of suture pull-out and tissue strength. J. Biomed. Eng. 1989, 11, 311–314. [Google Scholar] [CrossRef]
- Kocabey, Y.; Taser, O.; Nyland, J.; Doral, M.N.; Demirhan, M.; Caborn, D.N.; Sarban, S. Pullout strength of meniscal repair after cyclic loading: Comparison of vertical, horizontal, and oblique suture techniques. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.A.; Temple, W.J.; Frank, C.B.; Huchcroft, S.A. A biomechanical study of suture pullout in linea alba. Surgery 1989, 106, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Mine, Y.; Mitsui, H.; Oshima, Y.; Noishiki, Y.; Nakai, M.; Sano, S. Suture retention strength of expanded polytetrafluoroethylene (ePTFE) graft. Acta Med. Okayama 2010, 64, 121–128. [Google Scholar] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).